
Patient Characteristics Associated with Repeat Antibiotic Prescribing Pre- and during the COVID-19 Pandemic: A Retrospective Nationwide Cohort Study of >19 Million Primary Care Records Using the OpenSAFELY Platform

Abstract
:1. Introduction
2. Results
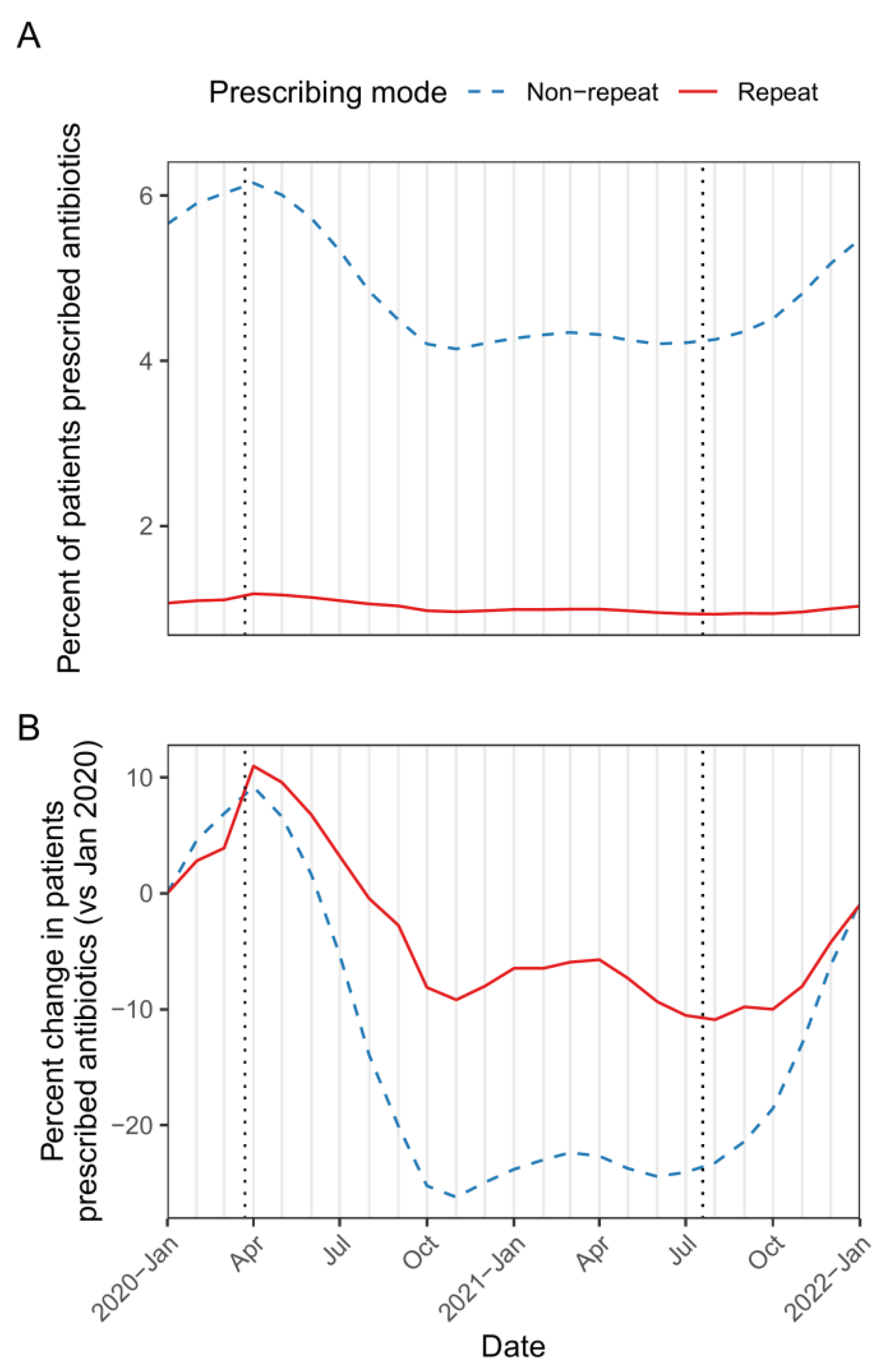
2.1. Frequency of Antibiotic Prescribing (Repeat and Non-Repeat) through the COVID-19 Pandemic
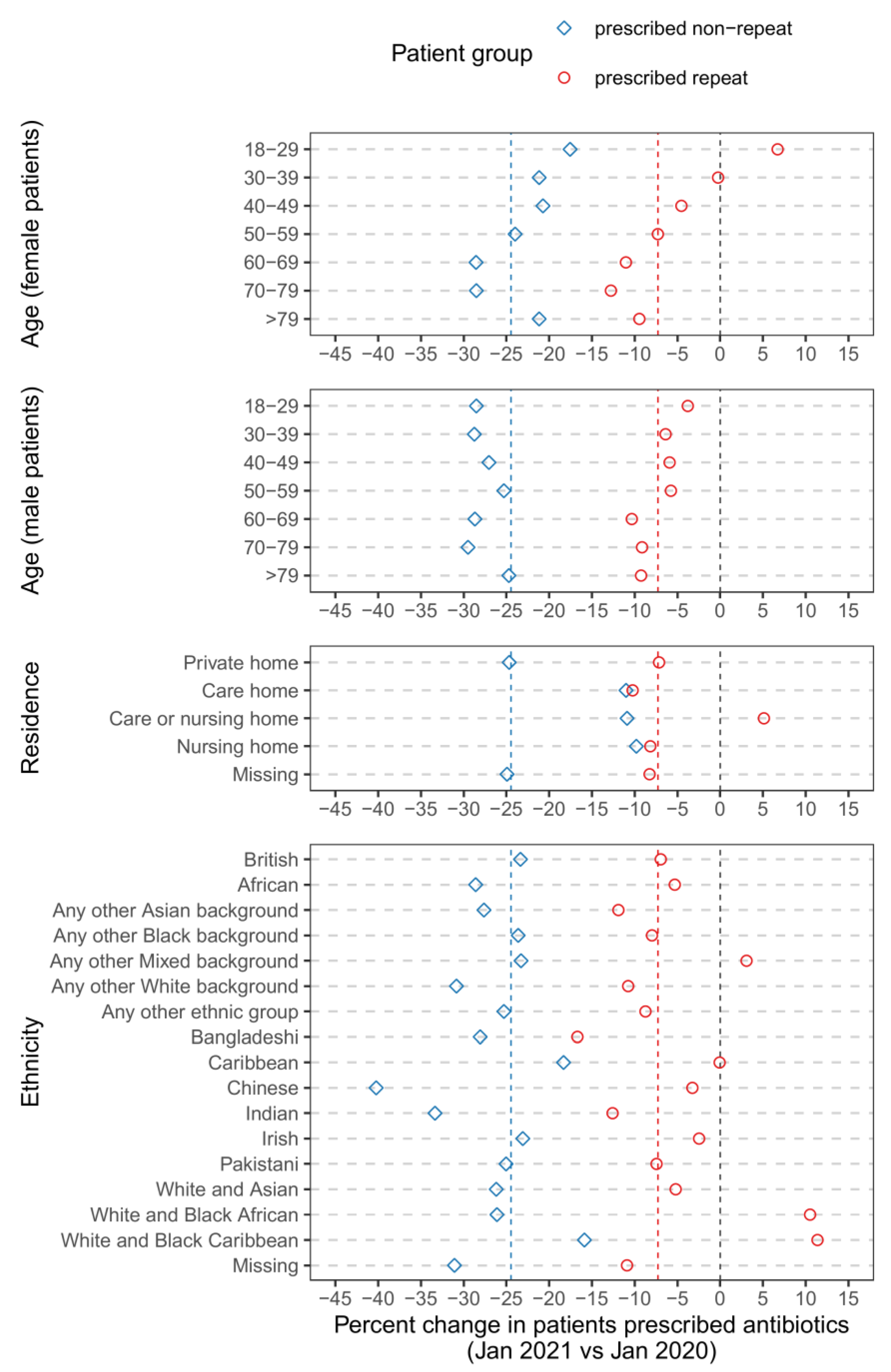
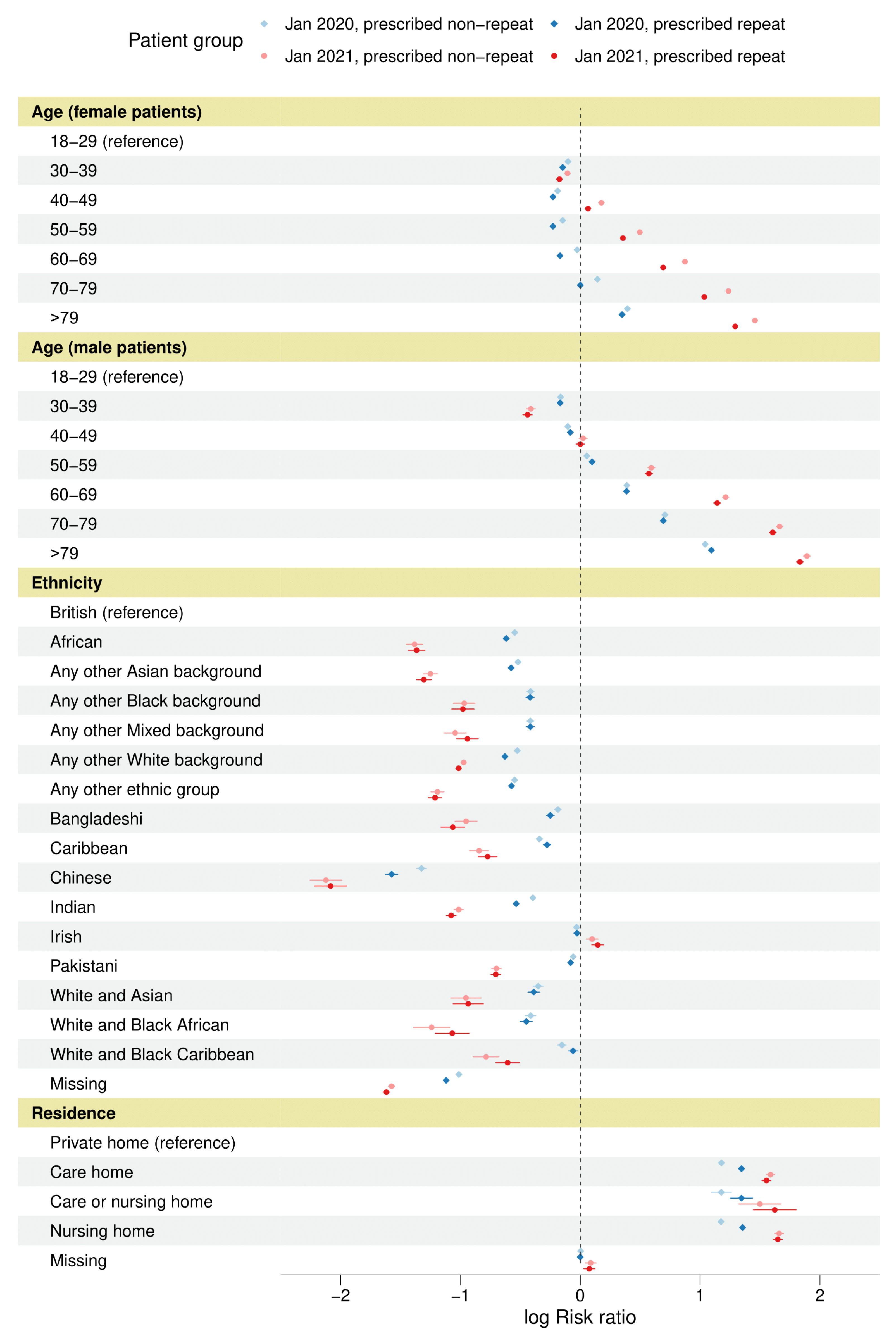
2.2. Demographics of Antibiotic Prescribing (Repeat and Non-Repeat) in Pre-Pandemic and Pandemic Cohorts

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | January 2020 (Pre-Pandemic) Cohort | January 2021 (Pandemic) Cohort | |||||
|---|---|---|---|---|---|---|---|
| Population (n = 19,375,208 n Female = 9,756,346 n Male = 9,618,862) | Prescribed Repeat Antibiotics (n = 206,865 n Female = 129,717 n Male = 77,148) | Prescribing per 1000 | Population (n = 19,545,285 n Female = 9,835,177 n Male = 9,710,108) | Prescribed Repeat Antibiotics (n = 193,517 n Female = 121,616 n Male = 71,901) | Prescribing per 1000 | Percent Change vs. January 2020 | |
| Age (female patients) | |||||||
| 18–29 | 1,789,887 (9.24) (18.35) | 13,038 (6.30) (10.05) | 7.28 | 1,768,295 (9.05) (17.98) | 13,746 (7.10) (11.30) | 7.77 | 6.72 |
| 30–39 | 1,683,962 (8.69) (17.26) | 11,029 (5.33) (8.50) | 6.55 | 1,707,559 (8.74) (17.36) | 11,156 (5.76) (9.17) | 6.53 | −0.25 |
| 40–49 | 1,526,149 (7.88) (15.64) | 13,261 (6.41) (10.22) | 8.69 | 1,530,997 (7.83) (15.57) | 12,700 (6.56) (10.44) | 8.3 | −4.53 |
| 50–59 | 1,635,345 (8.44) (16.76) | 19,576 (9.46) (15.09) | 11.97 | 1,654,637 (8.47) (16.82) | 18,363 (9.49) (15.10) | 11.1 | −7.29 |
| 60–69 | 1,305,184 (6.74) (13.38) | 22,772 (11.01) (17.56) | 17.45 | 1,331,364 (6.81) (13.54) | 20,668 (10.68) (16.99) | 15.52 | −11.02 |
| 70–79 | 1,090,670 (5.63) (11.18) | 27,359 (13.23) (21.09) | 25.08 | 1,116,918 (5.71) (11.36) | 24,437 (12.63) (20.09) | 21.88 | −12.78 |
| >79 | 725,149 (3.74) (7.43) | 22,682 (10.96) (17.49) | 31.28 | 725,407 (3.71) (7.38) | 20,546 (10.62) (16.89) | 28.32 | −9.45 |
| Age (male patients) | |||||||
| 18–29 | 1,801,657 (9.30) (18.73) | 6764 (3.27) (8.77) | 3.75 | 1,787,078 (9.14) (18.40) | 6455 (3.34) (8.98) | 3.61 | −3.79 |
| 30–39 | 1,732,184 (8.94) (18.01) | 4305 (2.08) (5.58) | 2.49 | 1,756,215 (8.99) (18.09) | 4086 (2.11) (5.68) | 2.33 | −6.39 |
| 40–49 | 1,620,217 (8.36) (16.84) | 6224 (3.01) (8.07) | 3.84 | 1,629,425 (8.34) (16.78) | 5889 (3.04) (8.19) | 3.61 | −5.92 |
| 50–59 | 1,686,327 (8.70) (17.53) | 11,459 (5.54) (14.85) | 6.8 | 1,705,162 (8.72) (17.56) | 10,919 (5.64) (15.19) | 6.4 | −5.76 |
| 60–69 | 1,281,804 (6.62) (13.33) | 16,188 (7.83) (20.98) | 12.63 | 1,310,721 (6.71) (13.50) | 14,842 (7.67) (20.64) | 11.32 | −10.34 |
| 70–79 | 992,394 (5.12) (10.32) | 19,662 (9.50) (25.49) | 19.81 | 1,014,499 (5.19) (10.45) | 18,263 (9.44) (25.40) | 18 | −9.14 |
| >79 | 504,279 (2.60) (5.24) | 12,546 (6.06) (16.26) | 24.88 | 507,008 (2.59) (5.22) | 11,447 (5.92) (15.92) | 22.58 | −9.25 |
| England region | |||||||
| London | 1,370,757 (7.07) | 5582 (2.70) | 4.07 | 1,401,485 (7.17) | 5340 (2.76) | 3.81 | −6.43 |
| East | 4,473,416 (23.09) | 50,364 (24.35) | 11.26 | 4,524,344 (23.15) | 46,804 (24.19) | 10.34 | −8.11 |
| East Midlands | 3,346,011 (17.27) | 37,326 (18.04) | 11.16 | 3,368,011 (17.23) | 35,476 (18.33) | 10.53 | −5.58 |
| North East | 924,774 (4.77) | 11,482 (5.55) | 12.42 | 928,030 (4.75) | 10,503 (5.43) | 11.32 | −8.85 |
| North West | 1,695,187 (8.75) | 23,100 (11.17) | 13.63 | 1,706,464 (8.73) | 22,020 (11.38) | 12.9 | −5.31 |
| South East | 1,316,373 (6.79) | 13,095 (6.33) | 9.95 | 1,323,206 (6.77) | 11,985 (6.19) | 9.06 | −8.95 |
| South West | 2,701,539 (13.94) | 29,560 (14.29) | 10.94 | 2,726,547 (13.95) | 27,402 (14.16) | 10.05 | −8.15 |
| West Midlands | 777,478 (4.01) | 7135 (3.45) | 9.18 | 778,032 (3.98) | 6633 (3.43) | 8.53 | −7.1 |
| Yorkshire and The Humber | 2,760,064 (14.25) | 29,119 (14.08) | 10.55 | 2,778,667 (14.22) | 27,246 (14.08) | 9.81 | −7.06 |
| Missing | 9609 (0.05) | 102 (0.05) | 10.62 | 10,499 (0.05) | 108 (0.06) | 10.29 | −3.09 |
| Ethnicity | |||||||
| British | 13,336,088 (68.83) | 180,353 (87.18) | 13.52 | 13,424,038 (68.68) | 168,923 (87.29) | 12.58 | −6.95 |
| African | 237,664 (1.23) | 806 (0.39) | 3.39 | 248,818 (1.27) | 799 (0.41) | 3.21 | −5.31 |
| Any other Asian background | 280,197 (1.45) | 1085 (0.52) | 3.87 | 290,504 (1.49) | 991 (0.51) | 3.41 | −11.9 |
| Any other Black background | 88,421 (0.46) | 454 (0.22) | 5.13 | 93,335 (0.48) | 441 (0.23) | 4.72 | −7.98 |
| Any other Mixed background | 90,785 (0.47) | 432 (0.21) | 4.76 | 94,187 (0.48) | 462 (0.24) | 4.91 | 3.08 |
| Any other White background | 1,671,589 (8.63) | 8543 (4.13) | 5.11 | 1,718,196 (8.79) | 7836 (4.05) | 4.56 | −10.76 |
| Any other ethnic group | 304,982 (1.57) | 1252 (0.61) | 4.11 | 320,839 (1.64) | 1202 (0.62) | 3.75 | −8.74 |
| Bangladeshi | 85,337 (0.44) | 445 (0.22) | 5.21 | 89,091 (0.46) | 387 (0.20) | 4.34 | −16.7 |
| Caribbean | 105,798 (0.55) | 615 (0.30) | 5.81 | 106,382 (0.54) | 618 (0.32) | 5.81 | −0.06 |
| Chinese | 133,388 (0.69) | 216 (0.10) | 1.62 | 134,678 (0.69) | 211 (0.11) | 1.57 | −3.25 |
| Indian | 528,449 (2.73) | 2591 (1.25) | 4.9 | 547,831 (2.80) | 2348 (1.21) | 4.29 | −12.58 |
| Irish | 102,020 (0.53) | 1523 (0.74) | 14.93 | 102,812 (0.53) | 1497 (0.77) | 14.56 | −2.46 |
| Pakistani | 372,857 (1.92) | 2505 (1.21) | 6.72 | 385,318 (1.97) | 2396 (1.24) | 6.22 | −7.44 |
| White and Asian | 45,869 (0.24) | 239 (0.12) | 5.21 | 48,185 (0.25) | 238 (0.12) | 4.94 | −5.2 |
| White and Black African | 42,435 (0.22) | 166 (0.08) | 3.91 | 44,412 (0.23) | 192 (0.10) | 4.32 | 10.51 |
| White and Black Caribbean | 53,562 (0.28) | 330 (0.16) | 6.16 | 55,520 (0.28) | 381 (0.20) | 6.86 | 11.38 |
| Missing | 1,895,767 (9.78) | 5310 (2.57) | 2.8 | 1,841,139 (9.42) | 4595 (2.37) | 2.5 | −10.9 |
| IMD quintile | |||||||
| 1 | 3,688,616 (19.04) | 41,591 (20.11) | 11.28 | 3,708,065 (18.97) | 39,089 (20.20) | 10.54 | −6.51 |
| 2 | 3,806,589 (19.65) | 40,311 (19.49) | 10.59 | 3,827,052 (19.58) | 37,623 (19.44) | 9.83 | −7.17 |
| 3 | 4,113,190 (21.23) | 44,300 (21.41) | 10.77 | 4,133,488 (21.15) | 41,411 (21.40) | 10.02 | −6.98 |
| 4 | 3,861,551 (19.93) | 40,581 (19.62) | 10.51 | 3,883,672 (19.87) | 37,744 (19.50) | 9.72 | −7.52 |
| 5 | 3,529,411 (18.22) | 36,074 (17.44) | 10.22 | 3,548,646 (18.16) | 33,424 (17.27) | 9.42 | −7.85 |
| Missing | 375,851 (1.94) | 4008 (1.94) | 10.66 | 444,362 (2.27) | 4226 (2.18) | 9.51 | −10.82 |
| Residence | |||||||
| Private home | 19,102,126 (98.59) | 199,286 (96.34) | 10.43 | 19,276,300 (98.62) | 186,730 (96.49) | 9.69 | −7.15 |
| Care home | 56,979 (0.29) | 2908 (1.41) | 51.04 | 56,385 (0.29) | 2583 (1.33) | 45.81 | −10.24 |
| Care or nursing home | 2505 (0.01) | 117 (0.06) | 46.71 | 2322 (0.01) | 114 (0.06) | 49.1 | 5.11 |
| Nursing home | 48,843 (0.25) | 2678 (1.29) | 54.83 | 47,447 (0.24) | 2389 (1.23) | 50.35 | −8.17 |
| Missing | 164,755 (0.85) | 1876 (0.91) | 11.39 | 162,831 (0.83) | 1701 (0.88) | 10.45 | −8.26 |
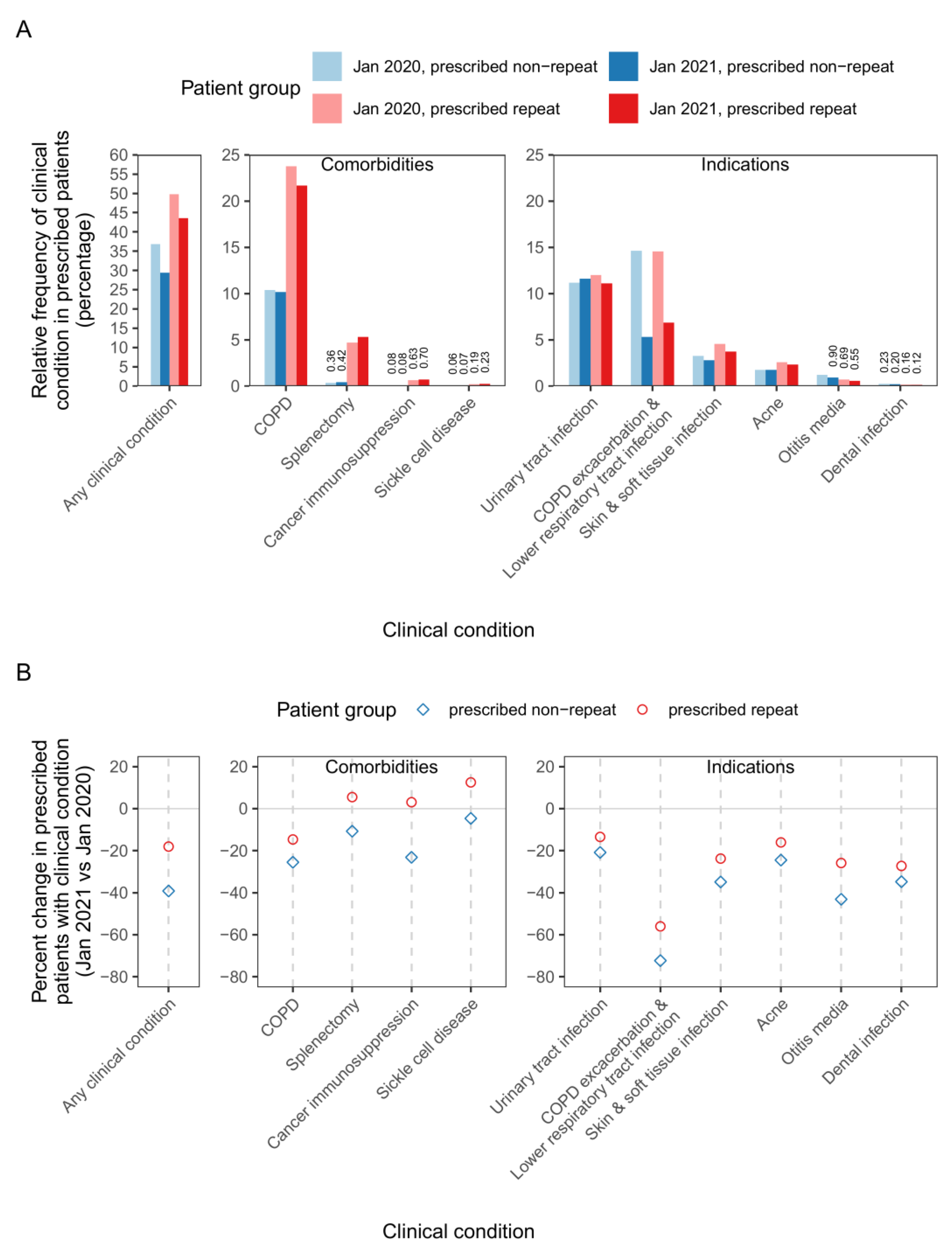
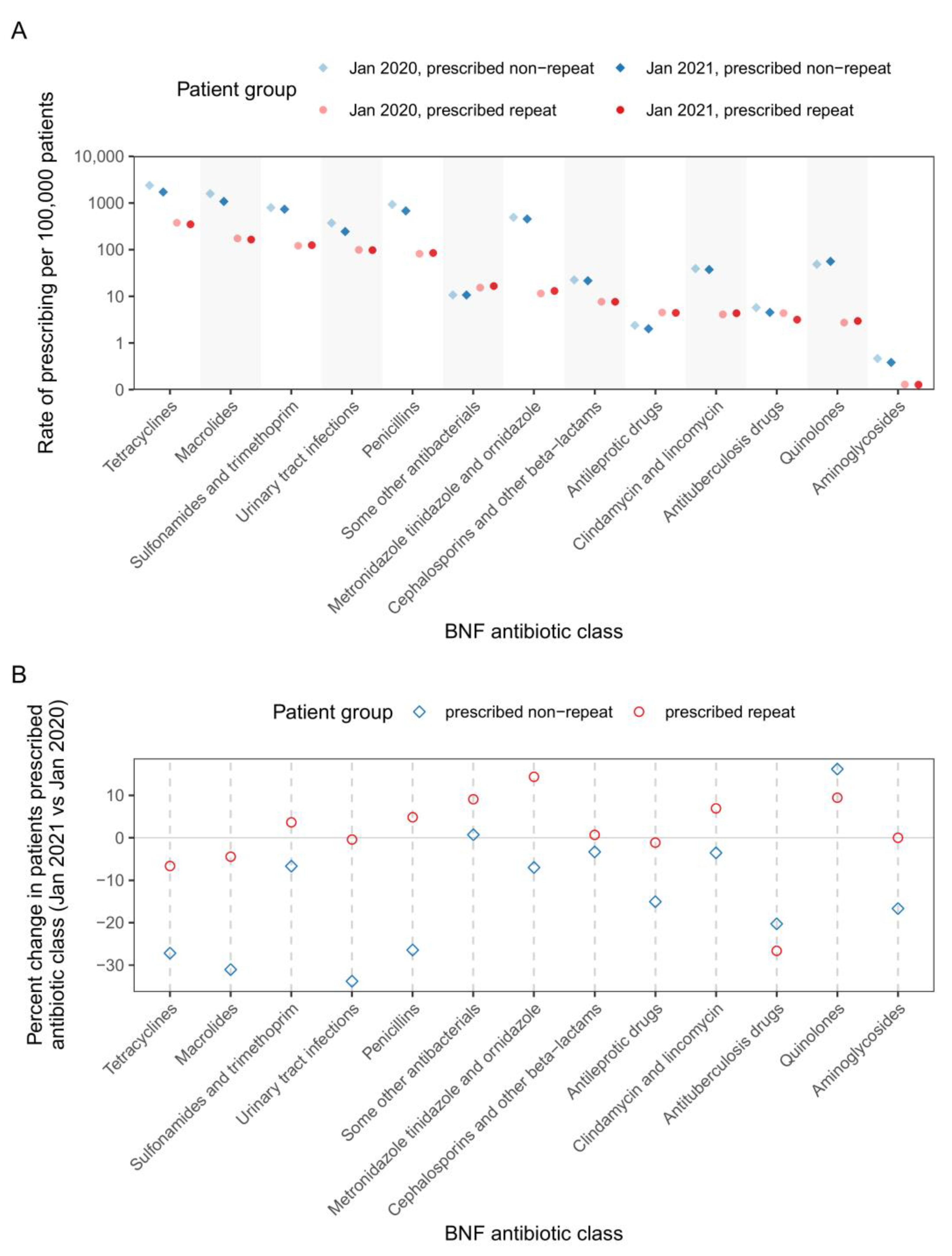
2.3. Patterns of Antibiotic Prescribing (Repeat and Non-Repeat) across Patient Clinical Conditions and Antibiotic Classes in Pre-Pandemic and Pandemic Cohorts
3. Discussion
4. Materials and Methods
4.1. OpenSAFELY-TPP Data Source and Study Design
4.2. Statistics and Reproducibility
4.3. Data Security and Disclosure Control
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UK Health Security Agency. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR): Report 2020 to 2021; UK Health Security Agency: London, UK, 2021.
- Collignon, P.; Beggs, J.J. CON: COVID-19 will not result in increased antimicrobial resistance prevalence. JAC Antimicrob Resist. 2020, 2, dlaa051. [Google Scholar] [CrossRef] [PubMed]
- Majeed, A.; Maile, E.J.; Bindman, A.B. The primary care response to COVID-19 in England’s National Health Service. J. R. Soc. Med. 2020, 113, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Borek, A.J.; Maitland, K.; McLeod, M.; Campbell, A.; Hayhoe, B.; Butler, C.C.; Morrell, L.; Roope, L.S.J.; Holmes, A.; Walker, A.S.; et al. Impact of the COVID-19 Pandemic on Community Antibiotic Prescribing and Stewardship: A Qualitative Interview Study with General Practitioners in England. Antibiotics 2021, 10, 1531. [Google Scholar] [CrossRef] [PubMed]
- Ashiru-Oredope, D.; Kerr, F.; Hughes, S.; Urch, J.; Lanzman, M.; Yau, T.; Cockburn, A.; Patel, R.; Sheikh, A.; Gormley, C.; et al. Assessing the Impact of COVID-19 on Antimicrobial Stewardship Activities/Programs in the United Kingdom. Antibiotics 2021, 10, 110. [Google Scholar] [CrossRef] [PubMed]
- Mahida, N.; Winzor, G.; Wilkinson, M.; Jumaa, P.; Gray, J. Antimicrobial stewardship in the post COVID-19 pandemic era: An opportunity for renewed focus on controlling the threat of antimicrobial resistance. J. Hosp. Infect. 2022, 129, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Social Care. UK 5-Year Action Plan for Antimicrobial Resistance 2019 to 2024; Department of Health and Social Care: London, UK, 2019.
- NHS England. Expanding Our Workforce. Available online: https://www.england.nhs.uk/gp/expanding-our-workforce (accessed on 11 October 2021).
- Krockow, E.M.; Harvey, E.J.; Ashiru-Oredope, D. Addressing long-term and repeat antibiotic prescriptions in primary care: Considerations for a behavioural approach. BMJ Qual. Saf. 2022, 31, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Andrews, A.; Bou-Antoun, S.; Guy, R.; Brown, C.S.; Hopkins, S.; Gerver, S. Respiratory antibacterial prescribing in primary care and the COVID-19 pandemic in England, winter season 2020–21. J. Antimicrob. Chemother. 2022, 77, 799–802. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.Z.; Paudyal, V.; Hadi, M.A. Impact of the COVID-19 Pandemic on the Prescribing Patterns of First-Line Antibiotics in English Primary Care: A Longitudinal Analysis of National Prescribing Dataset. Antibiotics 2021, 10, 591. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Institute for Government. Timeline of UK Government Coronavirus Lockdowns and Restrictions; Institute for Government: London, UK, 2022.
- Brown, B.; Kirk-Wade, E.; Baker, C.; Barber, S. Coronavirus: A History of English Lockdown Laws; UK Parliament: London, UK, 2021. [Google Scholar]
- Zhu, N.; Aylin, P.; Rawson, T.; Gilchrist, M.; Majeed, A.; Holmes, A. Investigating the impact of COVID-19 on primary care antibiotic prescribing in North West London across two epidemic waves. Clin. Microbiol. Infect. 2021, 27, 762–768. [Google Scholar] [CrossRef]
- Rezel-Potts, E.; L’Esperance, V.; Gulliford, M.C. Antimicrobial stewardship in the UK during the COVID-19 pandemic: A population-based cohort study and interrupted time-series analysis. Br. J. Gen. Pract. 2021, 71, e331–e338. [Google Scholar] [CrossRef]
- Malcolm, W.; Seaton, R.A.; Haddock, G.; Baxter, L.; Thirlwell, S.; Russell, P.; Cooper, L.; Thomson, A.; Sneddon, J. Impact of the COVID-19 pandemic on community antibiotic prescribing in Scotland. JAC Antimicrob Resist. 2020, 2, dlaa105. [Google Scholar] [CrossRef] [PubMed]
- The Office for National Statistics. Coronavirus (COVID-19) Case Rates by Socio-Demographic Characteristics, England: 1 September 2020 to 10 December 2021; The Office for National Statistics: Newport, UK, 2022.
- Department of Health & Social Care. Technical Report on the COVID-19 Pandemic in the UK: Chapter 8.2: Care Homes; Department of Health and Social Care: London, UK, 2022.
- Department of Health & Social Care. Technical Report on the COVID-19 Pandemic in the UK: Chapter 6: Testing; Department of Health and Social Care: London, UK, 2022.
- The Office for National Statistics. Ethnicity Facts and Figures: UK Population by Ethnicity; The Office for National Statistics: Newport, UK, 2023.
- NICE. BNF Treatment Summaries: Antibacterials, Use for Prophylaxis. Available online: https://bnf.nice.org.uk/treatment-summaries/antibacterials-use-for-prophylaxis (accessed on 3 May 2023).
- NICE. Sickle Cell Disease: Scenario: Prevention of Complications. Available online: https://cks.nice.org.uk/topics/sickle-cell-disease/management/prevention-of-complications/ (accessed on 19 May 2023).
- Ahmed, H.; Davies, F.; Francis, N.; Farewell, D.; Butler, C.; Paranjothy, S. Long-term antibiotics for prevention of recurrent urinary tract infection in older adults: Systematic review and meta-analysis of randomised trials. BMJ Open 2017, 7, e015233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lown, M.; McKeown, S.; Stuart, B.; Francis, N.; Santer, M.; Lewith, G.; Su, F.; Moore, M.; Little, P. Prescribing of long-term antibiotics to adolescents in primary care: A retrospective cohort study. Br. J. Gen. Pract. 2021, 71, e887–e894. [Google Scholar] [CrossRef] [PubMed]
- RCGP. Antibiotic Stewardship Tools, Audits and Other Resources: How to..? Resources. Available online: https://elearning.rcgp.org.uk/mod/book/view.php?id=12649&chapterid=793 (accessed on 2 May 2023).
- RCGP. TARGET Antibiotics Toolkit Hub. Royal College of General Practitioners: Learning. Available online: https://elearning.rcgp.org.uk/course/view.php?id=553 (accessed on 23 August 2022).
- OpenSAFELY. Overview: What Is a Study Definition? Available online: https://docs.opensafely.org/study-def/ (accessed on 8 May 2023).
- Mathur, R.; Bhaskaran, K.; Chaturvedi, N.; Leon, D.A.; vanStaa, T.; Grundy, E.; Smeeth, L. Completeness and usability of ethnicity data in UK-based primary care and hospital databases. J. Public Health 2013, 36, 684–692. [Google Scholar] [CrossRef]
- Schultze, A.; Bates, C.; Cockburn, J.; Mackenna, B.; Nightingale, E.; Curtis, H.J.; Hulme, W.J.; Morton, C.E.; Croker, R.; Bacon, S.; et al. Identifying Care Home Residents in Electronic Health Records—An OpenSAFELY Short Data Report. Wellcome Open Res. 2021, 6, 90. [Google Scholar] [CrossRef] [PubMed]
- Lenti, M.V.; Luu, S.; Carsetti, R.; Osier, F.; Ogwang, R.; Nnodu, O.E.; Wiedermann, U.; Spencer, J.; Locatelli, F.; Corazza, G.R.; et al. Asplenia and spleen hypofunction. Nat. Rev. Dis. Prim. 2022, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- OpenSAFELY. Study Definitions: Working with Dates: Dynamic Dates. Available online: https://docs.opensafely.org/study-def-dates/#dynamic-dates (accessed on 19 May 2023).
- Aragon, T.J.; Fay, M.P.; Wollschlaeger, D.; Omidpanah, A.; Omidpanah, M.A. Package ‘epitools’. Available online: https://cran.r-project.org/web/packages/epitools/index.html (accessed on 4 June 2023).
- OpenSAFELY. “Safe Outputs” and Requesting Release of Files from the Level 4 Server. Available online: https://docs.opensafely.org/releasing-files/#safe-outputs-and-requesting-release-of-files-from-the-level-4-server (accessed on 8 May 2023).
- NHS Digital. BETA—Clinical Information Standards. Available online: https://digital.nhs.uk/about-nhs-digital/our-work/nhs-digital-data-and-technology-standards/clinical-information-standards (accessed on 24 November 2022).
- NHS Digital. Data Security and Protection Toolkit. Available online: https://digital.nhs.uk/data-and-information/looking-after-information/data-security-and-information-governance/data-security-and-protection-toolkit (accessed on 24 November 2022).
- NHS Digital. ISB1523: Anonymisation Standard for Publishing Health and Social Care Data. Available online: https://digital.nhs.uk/data-and-information/information-standards/information-standards-and-data-collections-including-extractions/publications-and-notifications/standards-and-collections/isb1523-anonymisation-standard-for-publishing-health-and-social-care-data (accessed on 24 November 2022).
- DHSC. Coronavirus (COVID-19): Notification to Organisations to Share Information. Available online: https://web.archive.org/web/20200421171727/https://www.gov.uk/government/publications/coronavirus-covid-19-notification-of-data-controllers-to-share-information (accessed on 8 May 2023).
- NHS Health Research Authority. Is My Study Research? Available online: http://www.hra-decisiontools.org.uk/research/index.html (accessed on 24 November 2022).





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orlek, A.; Harvey, E.; Fisher, L.; Mehrkar, A.; Bacon, S.; Goldacre, B.; MacKenna, B.; Ashiru-Oredope, D. Patient Characteristics Associated with Repeat Antibiotic Prescribing Pre- and during the COVID-19 Pandemic: A Retrospective Nationwide Cohort Study of >19 Million Primary Care Records Using the OpenSAFELY Platform. Pharmacoepidemiology 2023, 2, 168-187. https://doi.org/10.3390/pharma2020016
Orlek A, Harvey E, Fisher L, Mehrkar A, Bacon S, Goldacre B, MacKenna B, Ashiru-Oredope D. Patient Characteristics Associated with Repeat Antibiotic Prescribing Pre- and during the COVID-19 Pandemic: A Retrospective Nationwide Cohort Study of >19 Million Primary Care Records Using the OpenSAFELY Platform. Pharmacoepidemiology. 2023; 2(2):168-187. https://doi.org/10.3390/pharma2020016
Chicago/Turabian StyleOrlek, Alex, Eleanor Harvey, Louis Fisher, Amir Mehrkar, Seb Bacon, Ben Goldacre, Brian MacKenna, and Diane Ashiru-Oredope. 2023. "Patient Characteristics Associated with Repeat Antibiotic Prescribing Pre- and during the COVID-19 Pandemic: A Retrospective Nationwide Cohort Study of >19 Million Primary Care Records Using the OpenSAFELY Platform" Pharmacoepidemiology 2, no. 2: 168-187. https://doi.org/10.3390/pharma2020016