
Treatment-Related Late Adverse Events in Childhood Cancer Survivors of Mexico: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design and Setting and Context
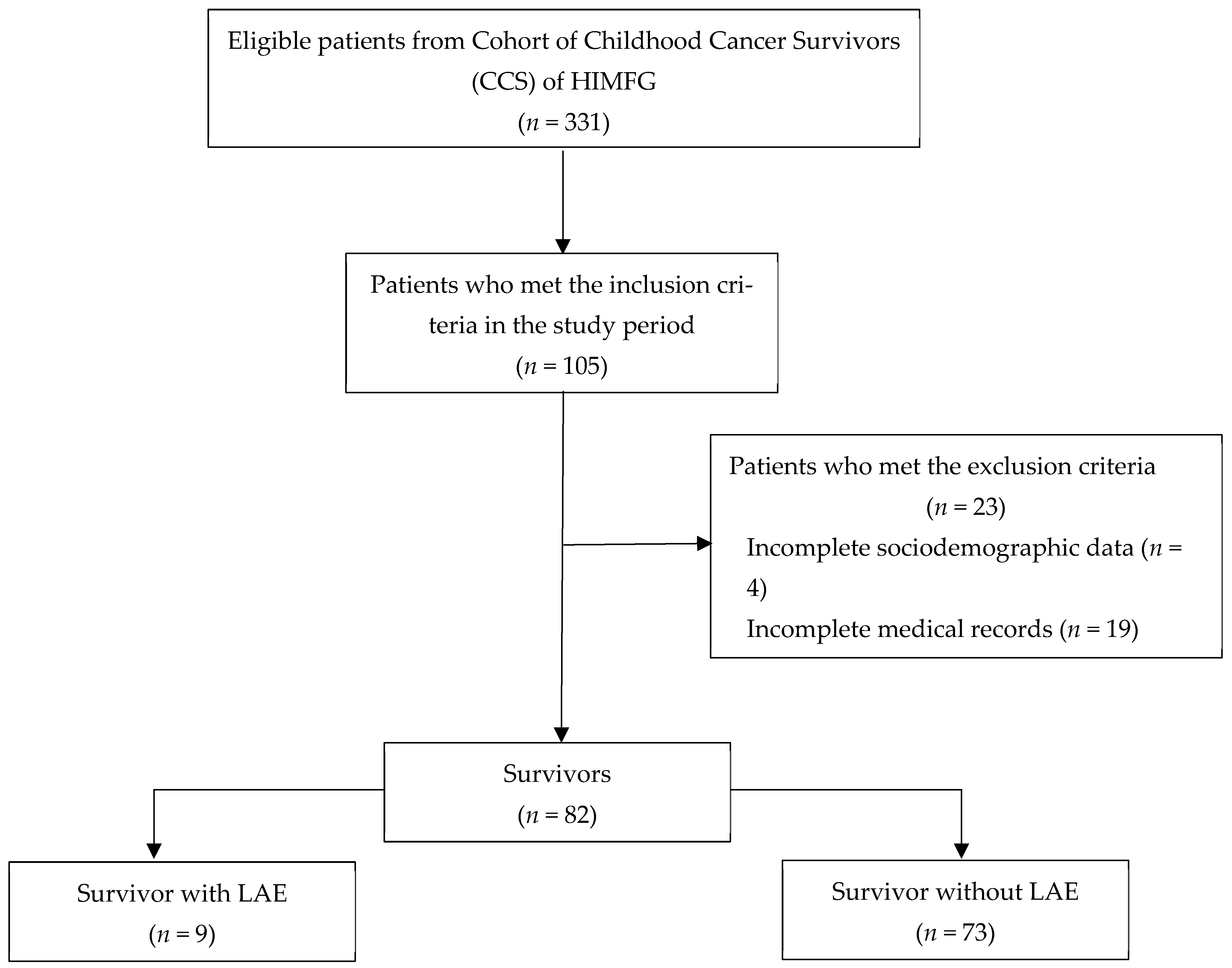
4.2. Participants
4.3. Variables and Data Sources
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Phillips, S.M.; Padgett, L.S.; Leisenring, W.M.; Stratton, K.K.; Bishop, K.; Krull, K.R.; Alfano, C.M.; Gibson, T.M.; de Moor, J.S.; Hartigan, D.B.; et al. Survivors of Childhood Cancer in the United States: Prevalence and Burden of Morbidity. Cancer Epidemiol. Biomark. Prev. 2015, 24, 653–663. [Google Scholar] [CrossRef] [Green Version]
- Cancer Facts & Figures 2013|American Cancer Society [Internet]. Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2013.html (accessed on 6 October 2022).
- El Cáncer Infantil [Internet]. Available online: https://www.who.int/es/news-room/fact-sheets/detail/cancer-in-children (accessed on 14 November 2022).
- Programa de Cáncer en la Infancia y la Adolescencia|Centro Nacional para la Salud de la Infancia y Adolescencia|Gobierno|gob.mx [Internet]. Available online: https://www.gob.mx/salud/censia/acciones-y-programas/programa-cancer-en-la-infancia-y-la-adolescencia (accessed on 14 November 2022).
- Gómez-Mercado, C.A.; Segura-Cardona, A.M.; Pájaro-Cantillo, D.E.; Mesa-Largo, M. Incidencia y determinantes demográficos de la leucemia linfoide aguda en pacientes con cáncer pediátrico. Antioq. Univ. Salud. 2020, 22, 112–119. [Google Scholar] [CrossRef]
- Managing Chemotherapy-Related Cardiotoxicity in Survivors of Childhood Cancers—PubMed [Internet]. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/25134924/ (accessed on 14 November 2022).
- Landier, W.; Skinner, R.; Wallace, W.H.; Hjorth, L.; Mulder, R.L.; Wong, F.L.; Yasui, Y.; Bhakta, N.; Constine, L.S.; Bhatia, S.; et al. Surveillance for Late Effects in Childhood Cancer Survivors. J. Clin. Oncol. 2018, 36, 2216–2222. [Google Scholar] [CrossRef]
- Ross, C.J.D.; Visscher, H.; Rassekh, S.R.; Castro-Pastrana, L.I.; Shereck, E.; Carleton, B.; Hayden, M.R. Pharmacogenomics of serious adverse drug reactions in pediatric oncology. J. Popul. Ther. Clin. Pharmacol. 2011, 18, e134–e151. [Google Scholar] [PubMed]
- Blaauwbroek, R.; Stant, A.; Groenier, K.; Kamps, W.; Meyboom, B.; Postma, A. Health-related quality of life and adverse late effects in adult (very) long-term childhood cancer survivors. Eur. J. Cancer 2007, 43, 122–130. [Google Scholar] [CrossRef] [Green Version]
- Hudson, M.M.; Ness, K.K.; Gurney, J.G.; Mulrooney, D.A.; Chemaitilly, W.; Krull, K.R.; Green, D.M.; Armstrong, G.T.; Nottage, K.A.; Jones, K.E.; et al. Clinical Ascertainment of Health Outcomes Among Adults Treated for Childhood Cancer. JAMA 2013, 309, 2371–2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livinalli, A.; Silva, M.T.; Lopes, L.C. Late adverse effects related to treatment in a cohort of survivors of childhood and adolescent cancer. Medicine 2019, 98, e14921. [Google Scholar] [CrossRef]
- Kremer, L.C.M.; van der Pal, H.J.H.; Offringa, M.; van Dalen, E.C.; Voûte, P.A. Frequency and risk factors of subclinical cardiotoxicity after anthracycline therapy in children: A systematic review. Ann. Oncol. 2002, 13, 819–829. [Google Scholar] [CrossRef]
- Lipshultz, S.E.; Lipsitz, S.R.; Sallan, S.E.; Dalton, V.M.; Mone, S.M.; Gelber, R.D.; Colan, S.D. Chronic Progressive Cardiac Dysfunction Years After Doxorubicin Therapy for Childhood Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2005, 23, 2629–2636. [Google Scholar] [CrossRef]
- Kenney, L.B.; Melvin, P.; Fishman, L.N.; O'Sullivan-Oliveira, J.; Sawicki, G.S.; Ziniel, S.; Diller, L.; Fernandes, S.M. Transition and transfer of childhood cancer survivors to adult care: A national survey of pediatric oncologists. Pediatr. Blood Cancer 2017, 64, 346–352. [Google Scholar] [CrossRef]
- Zheng, D.J.; Sint, K.; Mitchell, H.-R.; Kadan-Lottick, N.S. Patterns and predictors of survivorship clinic attendance in a population-based sample of pediatric and young adult childhood cancer survivors. J. Cancer Surviv. 2016, 10, 505–513. [Google Scholar] [CrossRef]
- Aging and Risk of Severe, Disabling, Life-Threatening, and Fatal Events in the Childhood Cancer Survivor Study—PubMed [Internet]. Available online: https://pubmed-ncbi-nlm-nih-gov.pbidi.unam.mx:2443/24638000/ (accessed on 14 November 2022).
- Lipshultz, S.E.; Alvarez, J.A.; Scully, R. Anthracycline associated cardiotoxicity in survivors of childhood cancer. Heart 2008, 94, 525–533. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Health. Common Terminology Criteria for Adverse Events (CTCAE). V5.0 [Internet]. Handydex; 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf. (accessed on 14 November 2022).
- Chow, E.J.; Chen, Y.; Krem er, L.C.; Breslow, N.E.; Hudson, M.M.; Armstrong, G.T.; Border, W.L.; Feijen, E.A.M.; Green, D.M.; Meacham, L.R.; et al. Individual Prediction of Heart Failure Among Childhood Cancer Survivors. J. Clin. Oncol. 2015, 33, 394–402. [Google Scholar] [CrossRef] [PubMed]
- El Superviviente de Cáncer Pediátrico, Retos y Perspectivas [Internet]. Available online: https://www.scielo.org.mx/scielo.php?pid=S2565-005X2020000300077&script=sci_arttext&tlng=es (accessed on 14 November 2022).
- Pellegrino, P.; Carnovale, C.; Cattaneo, D.; Perrone, V.; Antoniazzi, S.; Pozzi, M.; Napoleone, E.; Filograna, M.R.; Clementi, E.; Radice, S. Pharmacovigilance knowledge in family paediatricians. A survey study in Italy. Health Policy 2013, 113, 216–220. [Google Scholar] [CrossRef]
- Sammons, H.M.; Choonara, I. Learning Lessons from Adverse Drug Reactions in Children. Children 2016, 3, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kearns, G.L.; Abdel-Rahman, S.M.; Alander, S.W.; Blowey, D.L.; Leeder, J.S.; Kauffman, R.E. Developmental pharmacology--drug disposition, action, and therapy in infants and children. N. Engl. J. Med. 2003, 349, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Geenen, M.M.; Cardous-Ubbink, M.C.; Kremer, L.C.M.; van den Bos, C.; van der Pal, H.J.H.; Heinen, R.C.; Jaspers, M.W.M.; Koning, C.C.E.; Oldenburger, F.; Langeveld, N.E.; et al. Medical Assessment of Adverse Health Outcomes in Long-term Survivors of Childhood Cancer. JAMA 2007, 297, 2705–2715. [Google Scholar] [CrossRef] [Green Version]
- Suh, E.; Stratton, K.L.; Leisenring, W.M.; Nathan, P.C.; Ford, J.S.; Freyer, D.R.; McNeer, J.L.; Stock, W.; Stovall, M.; Krull, K.R.; et al. Late mortality and chronic health conditions in long-term survivors of early-adolescent and young adult cancers: A retrospective cohort analysis from the Childhood Cancer Survivor Study. Lancet Oncol. 2020, 21, 421–435. [Google Scholar] [CrossRef]
- Mulrooney, D.A.; Soliman, E.Z.; Ehrhardt, M.J.; Lu, L.; Duprez, D.A.; Luepker, R.V.; Armstrong, G.T.; Joshi, V.M.; Green, D.M.; Srivastava, D.; et al. Electrocardiographic abnormalities and mortality in aging survivors of childhood cancer: A report from the St Jude Lifetime Cohort Study. Am. Heart J. 2017, 189, 19–27. [Google Scholar] [CrossRef]
- Wilson, C.L.; Liu, W.; Yang, J.J.; Kang, G.; Ojha, R.P.; Neale, G.A.; Srivastava, D.K.; Gurney, J.G.; Hudson, M.M.; Robison, L.L.; et al. Genetic and clinical factors associated with obesity among adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort. Cancer 2015, 121, 2262–2270. [Google Scholar] [CrossRef] [Green Version]
- Efectos Adversos de la Terapia con Glucocorticoides|Iatreia [Internet]. Available online: https://revistas.udea.edu.co/index.php/iatreia/article/view/342711 (accessed on 5 December 2022).
- Encuesta Nacional de Salud y Nutrición 2018–19. Resultados Nacionales [Internet]. Available online: https://www.insp.mx/produccion-editorial/novedades-editoriales/ensanut-2018-nacionales (accessed on 5 December 2022).
- Vargas-Neri, J.L.; Carleton, B.; Ross, C.J.; Medeiros, M.; Castañeda-Hernández, G.; Clark, P. Pharmacogenomic study of anthracycline-induced cardiotoxicity in Mexican pediatric patients. Pharmacogenomics 2022, 23, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Lipshultz, S.; Scully, R.E.; Lipsitz, S.R.; Sallan, S.E.; Silverman, L.B.; Miller, T.L.; Barry, E.V.; Asselin, B.L.; Athale, U.; Clavell, L.A.; et al. Assessment of dexrazoxane as a cardioprotectant in doxorubicin-treated children with high-risk acute lymphoblastic leukaemia: Long-term follow-up of a prospective, randomised, multicentre trial. Lancet Oncol. 2010, 11, 950–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robison, L.L.; Hudson, M.M. Survivors of childhood and adolescent cancer: Life-long risks and responsibilities. Nat. Rev. Cancer 2014, 14, 61–70. [Google Scholar] [CrossRef]
- Landier, W.; Armenian, S.H.; Lee, J.; Thomas, O.; Wong, F.L.; Francisco, L.; Herrera, C.; Kasper, C.; Wilson, K.D.; Zomorodi, M.; et al. Yield of Screening for Long-Term Complications Using the Children’s Oncology Group Long-Term Follow-Up Guidelines. J. Clin. Oncol. 2012, 30, 4401–4408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Study Population n = 82 | Patients with LAEs n = 9 | Patients without LAEs n = 73 | p-Value |
|---|---|---|---|---|
| Age at diagnosis (years) [median and IQR] | 6.0 (3.0–13.0) | 5.0 (2.5–12.5) | 6.0 (3.0–13.0) | 0.666 |
| Sex Male (n, %) | 45 (54.9) | 3 (33.3) | 42 (57.5) | 0.287 |
| Weight (kg) [median and IQR] | 25.0 (13.9–49.6) | 27.0 (14.5–66.0) | 24.0 (13.8–47.3) | 0.369 |
| Height (cm) [median and IQR] | 113.3 (88.0–152.3) | 100.0 (75.5–143.6) | 114.0 (89.0–152.5) | 0.509 |
| Diagnosis | ||||
| Leukemia (n, %) | 37 (45.1) | 3 (33.3) | 34 (46.6) | 0.349 |
| Lymphoma (n, %) | 12 (14.6) | 2 (22.2) | 10 (13.7) | 0.392 |
| Germ cell tumors (n, %) | 12 (14.6) | 1 (11.1) | 11 (15.1) | 0.608 |
| Central nervous system tumor (n, %) | 5 (6.1) | 1 (11.1) | 4 (5.5) | 0.450 |
| Rhabdomyosarcoma (n, %) | 3 (3.7) | 0 (0.0) | 3 (4.1) | 1.00 |
| Retinoblastoma (n, %) | 3 (3.7) | 0 (0.0) | 3 (4.1) | 1.00 |
| Wilms tumor (n, %) | 3 (3.7) | 1 (11.1) | 2 (2.7) | 0.298 |
| Neuroblastoma (n, %) | 2 (2.4) | 1 (11.1) | 1 (1.4) | 0.209 |
| Ewing’s sarcoma (n, %) | 2 (2.4) | 0 (0.0) | 2 (2.7) | 1.00 |
| Osteosarcoma (n, %) | 1 (1.2) | 0 (0.0) | 1 (1.4) | 1.00 |
| Hepatoblastoma (n, %) | 1 (1.2) | 0 (0.0) | 1 (1.4) | 1.00 |
| Langerhans cell histiocytosis (n, %) | 1 (1.2) | 0 (0.0) | 1 (1.4) | 1.00 |
| Treatment | ||||
| Chemotherapy only (n, %) | 37 (45.1) | 1 (11.1) | 36 (49.3) | 0.030 * |
| Chemotherapy + radiation (n, %) | 16 (19.5) | 4 (44.4) | 12 (16.4) | 0.068 |
| Chemotherapy + surgery (n, %) | 17 (20.7) | 2 (22.2) | 15 (20.5) | 0.598 |
| Chemotherapy + surgery + radiation (n, %) | 12 (14.6) | 2 (22.2) | 10 (13.7) | 0.392 |
| Follow-up (years) [median and IQR] | 6.5 (3.0–12.0) | 7.0 (3.0–13.0) | 6.0 (3.0–12.0) | 0.778 |
| Patient outcome | 0.378 | |||
| Survivors (n, %) | 78 (95.1) | 8 (88.9) | 70 (95.9) | |
| Death (n, %) | 4 (4.9) | 1 (11.1) | 3 (4.1) |
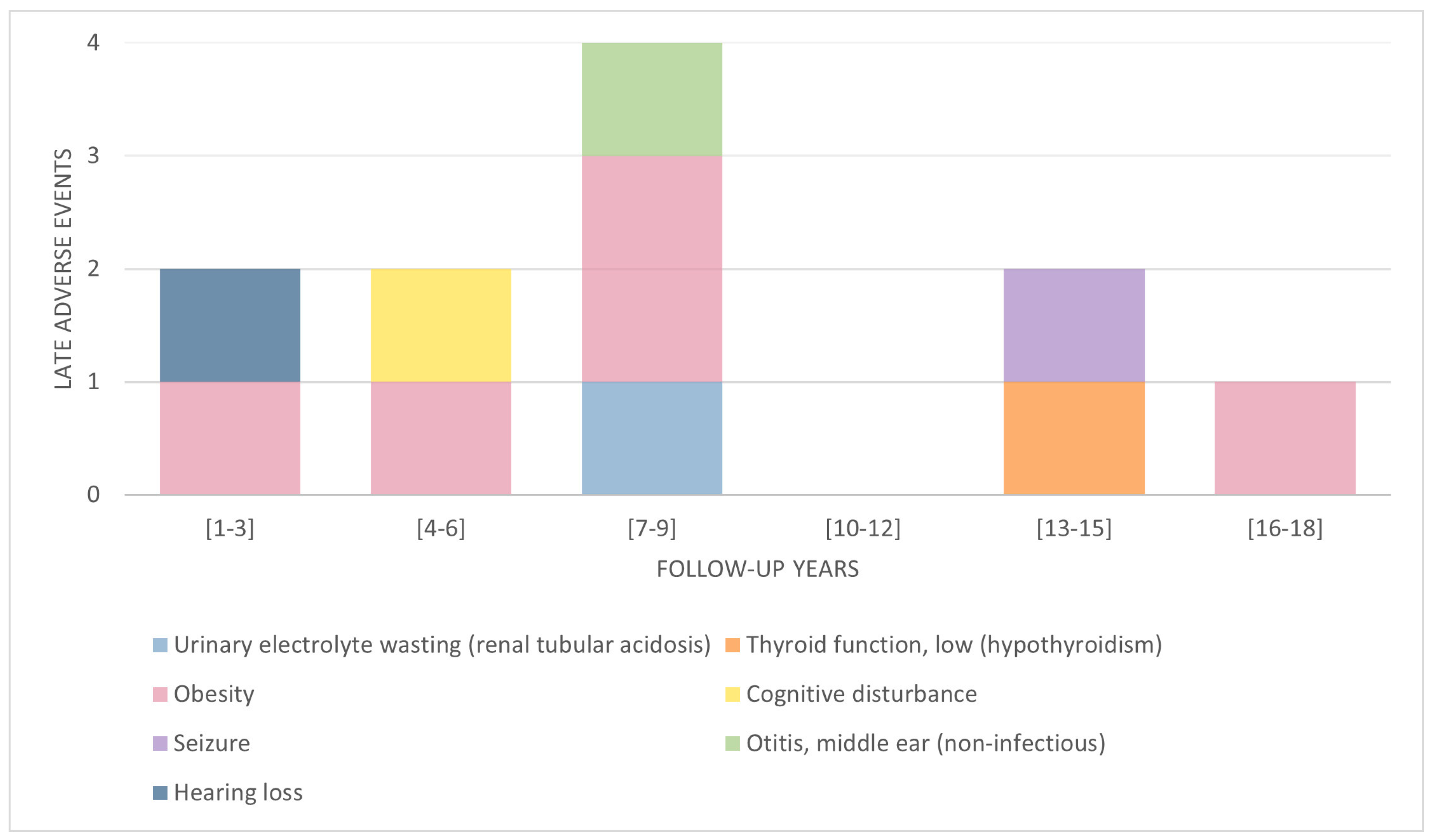
| Body System | LAEs (n, %) | Patients (n, %) |
|---|---|---|
| Endocrine | 6 (54.5) | 5 (55.6) |
| Obesity | 5 (45.4) | |
| BMI 25–29.9 kg/m2 | 3 (27.2) | |
| BMI 30–39.9 kg/m2 | 2 (18.2) | |
| Thyroid function, low (hypothyroidism) | 1 (9.1) | |
| Neurological | 2 (18.2) | 2 (22.2) |
| Cognitive disturbance | 1 (9.1) | |
| Seizure | 1 (9.1) | |
| Auditory | 2 (18.2) | 1 (11.1) |
| Hearing loss | 1 (9.1) | |
| Otitis, middle ear (non-infectious) | 1 (9.1) | |
| Renal | 1 (9.1) | 1 (11.1) |
| Urinary electrolyte wasting (renal tubular acidosis) | 1 (9.1) | |
| Total | 11 (100.0) | 9 (100.0) |
| Diagnosis | Severity Grade | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| Leukemia (n, %) | 1 (50.0) | 1 (16.7) | 1 (50.0) | 1 (100.0) | 0 (0.0) |
| Lymphoma (n, %) | 0 (0.0) | 2 (33.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Other types of cancer (n, %) | 0 (0.0) | 0 (0.0) | |||
| Central nervous system tumor (n, %) | 1 (50.0) | ||||
| Germ cell tumors (n, %) | 1 (16.7) | ||||
| Rhabdomyosarcoma (n, %) | 1 (16.7) | ||||
| Wilms tumor (n, %) | 1 (16.7) | ||||
| Neuroblastoma (n, %) | 1 (50.0) | ||||
| Total n = 11 | 2 (18.2) | 6 (54.5) | 2 (18.2) | 1 (9.1) | 0 (0.0) |
| Variable | Patients with LAEs n = 9 | Patients without LAEs n = 73 | Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Age at diagnosis | ----- | ----- | ----- | ----- | 0.71 (0.51–0.99) | 0.046 * |
| Weight | ----- | ----- | ----- | ----- | 1.09 (0.98–1.21) | 0.096 |
| Height | ----- | ----- | ----- | ----- | 1.00 (0.93–1.06) | 0.962 |
| Sex Female | 6 | 31 | 2.71 (0.63–11.69) | 0.169 | 4.54 (0.83–24.81) | 0.081 |
| Diagnosis | ----- | ----- | ||||
| Leukemia | 3 | 34 | 0.57 (0.13–2.47) | 0.451 | ||
| Lymphoma | 2 | 10 | 1.80 (0.33–9.92) | 0.495 | ||
| Germ cell tumor | 1 | 11 | 0.705 (0.08–6.20) | 0.751 | ||
| Central nervous system tumor | 1 | 4 | 2.16 (0.21–21.73) | 0.505 | ||
| Rhabdomyosarcoma | 0 | 3 | 0.89 (0.82–0.96) | 0.536 | ||
| Retinoblastoma | 0 | 3 | 0.89 (0.82–0.96) | 0.536 | ||
| Wilms Tumor | 1 | 2 | 4.44 (0.36–54.56) | 0.207 | ||
| Neuroblastoma | 1 | 1 | 9.00 (0.51–158.17) | 0.074 | ||
| Ewing’s sarcoma | 0 | 2 | 0.89 (0.82–0.96) | 0.615 | ||
| Osteosarcoma | 0 | 1 | 0.89 (0.82–0.96) | 0.724 | ||
| Hepatoblastoma | 0 | 1 | 0.89 (0.82–0.96) | 0.724 | ||
| Langerhans cell histiocytosis | 0 | 1 | 0.89 (0.82–0.96) | 0.724 | ||
| Treatment | ||||||
| Chemotherapy only | 1 | 36 | 0.13 (0.01–1.08) | 0.030 * | 0.03 (0.00–0.86) | 0.040 * |
| Chemotherapy + radiation | 4 | 12 | 4.07 (0.95–17.40) | 0.045 * | 1.73 (1.20–15.30) | 0.621 |
| Chemotherapy + surgery | 2 | 15 | 1.10 (0.21–5.87) | 0.907 | 0.26 (0.02–3.24) | 0.293 |
| Chemotherapy + surgery + radiation | 2 | 10 | 1.80 (0.33–9.92) | 0.495 | Reference | |
| Patient outcome | ||||||
| Survivors | 8 | 70 | ----- | ----- | 0.15 (0.01–2.93) | 0.211 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Franco, J.F.; Hernández-Pliego, G.; Jacobo-Mendoza, J.; Martínez-Lara, V.K.; Juárez-Villegas, L.E.; Clark, P.; Vargas-Neri, J.L. Treatment-Related Late Adverse Events in Childhood Cancer Survivors of Mexico: A Cross-Sectional Study. Pharmacoepidemiology 2023, 2, 157-167. https://doi.org/10.3390/pharma2020015
Pérez-Franco JF, Hernández-Pliego G, Jacobo-Mendoza J, Martínez-Lara VK, Juárez-Villegas LE, Clark P, Vargas-Neri JL. Treatment-Related Late Adverse Events in Childhood Cancer Survivors of Mexico: A Cross-Sectional Study. Pharmacoepidemiology. 2023; 2(2):157-167. https://doi.org/10.3390/pharma2020015
Chicago/Turabian StylePérez-Franco, José Fernando, Gabriela Hernández-Pliego, Jocelyn Jacobo-Mendoza, Vanessa Karina Martínez-Lara, Luis Enrique Juárez-Villegas, Patricia Clark, and Jessica Liliana Vargas-Neri. 2023. "Treatment-Related Late Adverse Events in Childhood Cancer Survivors of Mexico: A Cross-Sectional Study" Pharmacoepidemiology 2, no. 2: 157-167. https://doi.org/10.3390/pharma2020015