
Neuromuscular Rehabilitation of the Brachioradialis Muscle after Distal Radius Fracture in Two Professional Soccer Players Using Electromyographic Biofeedback

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
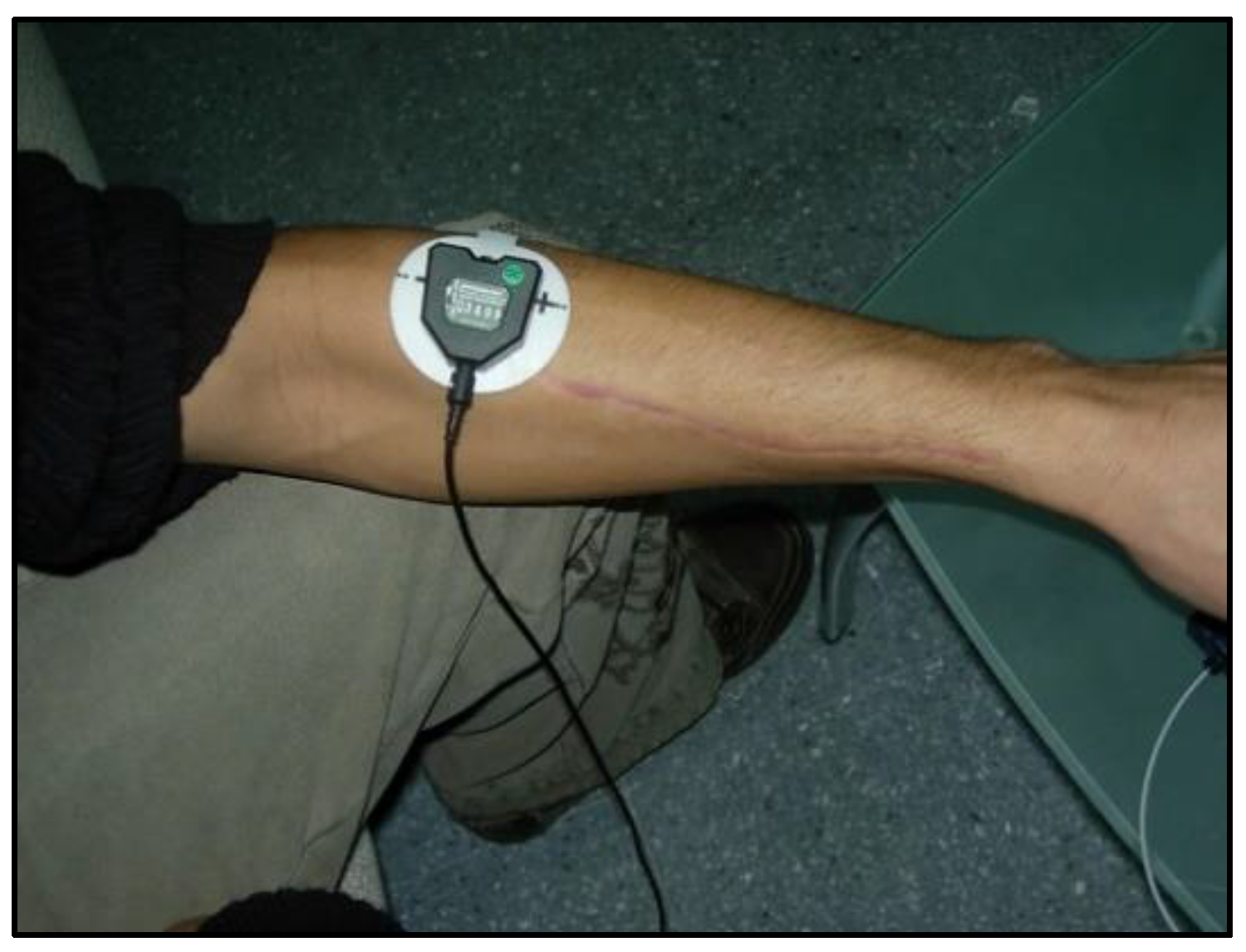
Measurements and Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Analysis of Variance Components
Generalizability Analysis
3.2. Differences in Maximum and Mean Values between Trials with BF and Trials without BF
3.3. Differences in Electromyographic Activity between Session 1 and Session 8
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liparoti, M.; Lopez, E.T. Biofeedback in sport and education. J. Hum. Sport Exerc. 2021, 16, S922–S929. [Google Scholar] [CrossRef]
- Giggins, O.M.; Persson, U.; Caulfield, B. Biofeedback in rehabilitation. J. Neuroeng. Rehabil. 2013, 10, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Pizzoli, S.F.; Marzorati, C.; Gatti, D.; Monzani, D.; Mazzocco, K.; Pravettoni, G. A meta-analysis on heart rate variability biofeedback and depressive symptoms. Sci. Rep. 2021, 11, 6650. [Google Scholar] [CrossRef]
- Lehrer, P.; Kaur, K.; Sharma, A.; Shah, K.; Huseby, R.; Bhavsar, J.; Sgobba, P.; Zhang, Y. Heart rate variability biofeedback improves emotional and physical health and performance: A systematic review and meta analysis. Appl. Psychophys. Biofeedback 2020, 45, 109–129. [Google Scholar] [CrossRef] [PubMed]
- Ardizone, I.; Sánchez, T.; Celemín, A.; Rivero, A. Biofeedback electromiográfico. Una alternativa terapéutica útil para la relajación muscular en pacientes con disfunción craneomandibular. Revista Internacional Prótesis Estomatológica 2009, 11, 85–88. [Google Scholar]
- Bowman, T.; Gervasoni, E.; Arienti, C.; Lazzerini, S.G.; Negrini, S.; Crea, S.; Cattaneo, D.; Carrozza, M.C. Wearable devices for biofeedback rehabilitation: A systematic review and meta-analysis to design application rules and estimate the effectiveness on balance and gait outcomes in neurological diseases. Sensors 2021, 21, 3444. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zheng, X.; Yi, X.; Lai, P.; Lan, Y. Electromyographic biofeedback for stress urinary incontinence or pelvic floor dysfunction in women: A systematic review and meta-analysis. Adv. Ther. 2021, 38, 4163–4177. [Google Scholar] [CrossRef]
- Kamonseki, D.H.; Calixtre, L.B.; Barreto, R.P.G.; Camargo, P.R. Effects of electromyographic biofeedback interventions for shoulder pain and function: Systematic review and meta-analysis. Clin. Rehabil. 2021, 35, 952–963. [Google Scholar] [CrossRef]
- Sturma, A.; Hruby, L.A.; Prahm, C.; Mayer, J.A.; Aszmann, O.C. Rehabilitation of upper extremity nerve injuries using surface EMG biofeedback: Protocols for clinical application. Front. Neurosci. 2018, 12, 906. [Google Scholar] [CrossRef]
- Gámez, A.B.; Hernandez Morante, J.J.; Martínez Gil, J.L.; Esparza, F.; Martínez, C.M. The effect of surface electromyography biofeedback on the activity of extensor and dorsiflexor muscles in elderly adults: A randomized trial. Sci. Rep. 2019, 9, 13153. [Google Scholar] [CrossRef]
- Kotov-Smolenskiy, A.M.; Khizhnikova, A.E.; Klochkov, A.S.; Suponeva, N.A.; Piradov, M.A. Surface EMG: Applicability in the motion analysis and opportunities for practical rehabilitation. Hum. Physiol. 2021, 47, 237–247. [Google Scholar] [CrossRef]
- Lirio-Romero, C.; Torres-Lacomba, M.; Gómez-Blanco, A.; Acero-Cortés, A.; Retana-Garrido, A.; de la Villa-Polo, P.; Sánchez-Sánchez, B. Electromyographic biofeedback improves upper extremity function: A randomized, single-blinded, controlled trial. Physiotherapy 2021, 110, 54–62. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.J. Electromyography. In Encyclopaedia of Medical Devices and Instrumentation; Webster, J.G., Ed.; Wiley: New York, NY, USA, 1988; pp. 1111–1120. [Google Scholar]
- Simon, M.A. Biofeedback y Rehabilitación; Promolibro: Valencia, Spain, 1989. [Google Scholar]
- Raeissadat, S.A.; Rayegani, S.M.; Sedighipour, L.; Bossaghzade, Z.; Abdollahzadeh, M.H.; Nikray, R.; Mollayi, F. The efficacy of electromyographic biofeedback on pain, function, and maximal thickness of vastus medialis oblique muscle in patients with knee osteoarthritis: A randomized clinical trial. J. Pain Res. 2018, 11, 2781–2789. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.J.; Wang, S.; Gong, Q.J.; Wang, J.X.; Sun, F.H.; Miyamoto, A.; Ocu, X.; Wang, L.; Wang, S.Q.; Zhang, C. Effects of electromyography biofeedback for patients after knee surgery: A systematic review and meta-analysis. J. Biomech. 2021, 120, 110386. [Google Scholar] [CrossRef]
- Wasielewski, N.J.; Parker, T.M.; Kotsko, K.M. Evaluation of electromyographic biofeedback for the quadriceps femoris: A systematic review. J. Athl. Train. 2011, 46, 543–554. [Google Scholar] [CrossRef]
- Oravitan, M.; Avram, C. The effectiveness of electromyographic biofeedback as part of a meniscal repair rehabilitation programme. J. Sports Sci. Med. 2013, 12, 526–532. [Google Scholar]
- Okamura, K.; Egawa, K.; Okii, A.; Oki, S.; Kanai, S. Intrinsic foot muscle strengthening exercises with electromyographic biofeedback achieve increased toe flexor strength in older adults: A pilot randomized controlled trial. Clin. Biomech. 2020, 80, 105187. [Google Scholar] [CrossRef]
- Junge, A.; Dvorak, J. Soccer injuries. Sports Med. 2004, 34, 929–938. [Google Scholar] [CrossRef]
- Karaborklu-Argut, S.; Celik, D.; Yasacı, Z. Effectiveness of therapeutic electromyographic biofeedback after orthopedic knee surgeries: A systematic review. Disabil. Rehabil. 2021, 44, 3364–3372. [Google Scholar] [CrossRef]
- Nilstad, A.; Andersen, T.E.; Bahr, R.; Holme, I.; Steffen, K. Risk factors for lower extremity injuries in elite female soccer players. Am. J. Sport Med. 2014, 42, 940–948. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gómez, A.; Vera-Garcia, F.J.; Croix, M.D.S.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Br. J. Sport Med. 2020, 54, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, J.; Junge, A. Football injuries and physical symptoms. Am. J. Sport Med. 2000, 28, 3–9. [Google Scholar] [CrossRef]
- Robertson, G.A.; Ang, K.K.; Jamal, B. Fractures in soccer: The current evidence, and how this can guide practice. J. Orthop. 2022, 33, 25–30. [Google Scholar] [CrossRef]
- Hart, D.; Funk, L. Serious shoulder injuries in professional soccer: Return to participation after surgery. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 2123–2129. [Google Scholar] [CrossRef] [PubMed]
- Matthias, R.C. Forearm, Wrist and Hand Injuries in Football. In Football Injuries; Farmer, K.W., Ed.; Springer: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Beleckas, C.; Calfee, R. Distal radius fractures in the athlete. Curr. Rev. Musculoskelet. Med. 2017, 10, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Bogart, R.; Vidlock, K. Ruptured extensor pollicis longus tendon after a nondisplaced distal radius fracture in a young adult soccer player. Clin. J. Sport Med. 2020, 30, e23–e24. [Google Scholar] [CrossRef] [PubMed]
- Adickes, M.S.; Stuart, M.J. Youth football injuries. Sports Med. 2004, 34, 201–207. [Google Scholar] [CrossRef]
- Johnson, N.; Leighton, P.; Distal Radius Fracture Delphi Study Group; Pailthorpe, C.; Dias, J. Defining displacement thresholds for surgical intervention for distal radius fractures—A Delphi study. PLoS ONE 2019, 14, e0210462. [Google Scholar] [CrossRef]
- Leixnering, M.; Rosenauer, R.; Pezzei, C.; Jurkowitsch, J.; Beer, T.; Keuchel, T.; Simon, D.; Hausner, T.; Quadlbauer, S. Indications, surgical approach, reduction, and stabilization techniques of distal radius fractures. Arch. Orthop. Trauma Surg. 2020, 140, 611–621. [Google Scholar] [CrossRef]
- Gradl, G.; Mielsch, N.; Wendt, M.; Falk, S.; Mittlmeier, T.; Gierer, P.; Gradl, G. Intramedullary nail versus volar plate fixation of extra-articular distal radius fractures. Two-year results of a prospective randomized trial. Injury 2014, 45, S3–S8. [Google Scholar] [CrossRef]
- Nho, J.H.; Gong, H.S.; Song, C.H.; Wi, S.M.; Lee, Y.H.; Baek, G.H. Examination of the pronator quadratus muscle during hardware removal procedures after volar plating for distal radius fractures. Clin. Orthop. Surg. 2014, 6, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, L.A.; de Oliveira, D.L.; Romano, R.G.; Correa, S.C. Leg preference and interlateral asymmetry of balance stability in soccer players. Res. Q. Exerc. Sport 2011, 82, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.K.; Park, J.S.; Shin, S.J.; Bae, H.; Kim, S.Y. The effect of brachioradialis release during distal radius fracture fixation on elbow flexion strength and wrist function. J. Hand Surg. 2014, 39, 2246–2250. [Google Scholar] [CrossRef] [PubMed]
- Hohendorff, B.; Unglaub, F.; Spies, C.K.; Mueller, L.P.; Ries, C. Repair of the pronator quadratus muscle with a part of the brachioradialis muscle insertion in volar plate fixation of a distal radius fracture. Oper. Orthop. Traumatol. 2019, 32, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Christanell, F.; Hoser, C.; Huber, R.; Fink, C.; Luomajoki, H. The influence of electromyographic biofeedback therapy on knee extension following anterior cruciate ligament reconstruction: A randomized controlled trial. Sports Med. Arthrosc. Rehab. Ther. Tech. 2012, 4, 41. [Google Scholar] [CrossRef] [PubMed]
- Chambless, D.L.; Hollon, S.D. Defining empirically supported therapies. J. Consult. Clin. Psych. 1998, 66, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Criado, L.; de La Fuente, A.; Heredia, M.; Montero, J.; Albaladejo, A.; Criado, J.-M. Electromyographic biofeedback training for reducing muscle pain and tension on masseter and temporal muscles: A pilot study. J. Clin. Exp. Dent. 2016, 8, e571–e576. [Google Scholar] [CrossRef]
- World Medical Association. World medical association declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Solé, V.; Moliner, L. Metodología para el estudio de la fatiga y la contracción muscular. Rehabilitación 1988, 22, 37–50. [Google Scholar]
- Hojat, M.; Xu, G. A visitor’s guide to effect sizes: Statistical significance versus practical (clinical) importance of research findings. Adv. Health Sci. Educ. Theory Pract. 2004, 9, 241–249. [Google Scholar] [CrossRef]
- SAS Institute. User’s Guide, 8th ed.; SAS/STAT SAS Institute: Cary, NC, USA, 1999. [Google Scholar]
- Schlotzhauer, S.D.; Littell, R. SAS System for Elementary Statistical Analysis; SAS Institute Inc.: Cary, NC, USA, 1997. [Google Scholar]
- Hernández-Mendo, A.; Blanco-Villaseñor, A.; Pastrana, J.L.; Morales-Sánchez, V.; Ramos-Pérez, F.J. SAGT: New software for generalizability analysis. Rev. Iberoam. Psicol. Ejerc. Deporte 2016, 11, 77–89. [Google Scholar]
- Hemmerle, W.; Hartley, H. Computing maximum likelihood estimates for the mixed AOV Model using the w-transformation. Technometrics 1973, 15, 819–831. [Google Scholar]
- Searle, S.; Casella, G.; McCulloch, C. Variance Components; John Wiley & Sons: New York, NY, USA, 1992. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Session | (T) | (R) | (T) | (R) | (T) | (R) | (T) | (R) | (T) | (R) | (T) | (R) | (T) | (R) | (T) |
| 10 | 12 | 12 | 12 | 12 | 12 | 12 | 10 | ||||||||
| trials | trials | trials | trials | trials | trials | trials | final trials | ||||||||
| baseline | a/b/c | a/b/c | a/b/c | a/b/c | a/b/c | a/b/c |
| Model z = Means-EMG | Sources of Variation | Sum of Squares | Degrees of Freedom | Mean Square | F | Pr < F | % |
| (p) | 99,005.04 | 1 | 99,005.04 | 157.26 | <0.0001 | 19.62 | |
| (f) | 192,112.50 | 2 | 96,056.25 | 152.57 | <0.0001 | 31.91 | |
| (p)(f) | 27,258.95 | 2 | 13,629.47 | 21.65 | <0.0001 | 10.48 | |
| (s) | 118,500.80 | 5 | 23,700.16 | 37.64 | <0.0001 | 11.14 | |
| (p)(s) | 46,684.39 | 4 | 11,671.10 | 18.54 | <0.0001 | 14.34 | |
| (f)(s) | 0 | 0 | 0 | 0 | 0 | 0 | |
| (p)(f)(s) | 0 | 0 | 0 | 0 | 0 | 0 | |
| (e) | 50,256.65 | 9 | 5584.07 | 8.87 | <0.0001 | 5.54 | |
| (p)(e) | 6982.46 | 9 | 775.83 | 1.23 | 0.2828 | 1.21 | |
| (f)(e) | 11,859.62 | 10 | 1185.96 | 1.88 | 0.0549 | 1.88 | |
| (p)(f)(e) | 3159.98 | 10 | 315.99 | 0.50 | 0.8855 | 1.36 | |
| (s)(e) | 8340.64 | 5 | 1668.12 | 2.65 | 0.0266 | 0.41 | |
| (p)(s)(e) | 5965.22 | 4 | 1491.30 | 2.37 | 0.0570 | 2.06 | |
| (f)(s)(e) | 0 | 0 | 0 | 0 | 0 | 0 | |
| (p)(f)(s)(s)(e) | 0 | 0 | 0 | 0 | 0 | 0 | |
| Model y = Maximums-EMG | (p) | 206,481.35 | 1 | 206,481.35 | 208.35 | <0.0001 | 26.83 |
| (f) | 234,004.41 | 2 | 117,002.20 | 118.06 | <0.0001 | 24.17 | |
| (p)(f) | 15,756.65 | 2 | 7878.33 | 7.95 | 0.0006 | 3.35 | |
| (s) | 201,490.42 | 5 | 40,298.08 | 40.66 | <0.0001 | 10.34 | |
| (p)(s) | 84,059.18 | 4 | 21,014.79 | 21.21 | <0.0001 | 14.94 | |
| (f)(s) | 0 | 0 | 0 | 0 | 0 | 0. | |
| (p)(f)(s) | 0 | 0 | 0 | 0 | 0 | 0 | |
| (e) | 164,282.93 | 9 | 18,253.65 | 18.42 | <0.0001 | 10.74 | |
| (p)(e) | 21,378.09 | 9 | 2375.34 | 2.40 | 0.0161 | 2.82 | |
| (f)(e) | 26,392.10 | 10 | 2639.21 | 2.66 | 0.0060 | 2.44 | |
| (p)(f)(e) | 6745.96 | 10 | 674.59 | 0.68 | 0.7403 | 1.67 | |
| (s)(e) | 21,928.59 | 5 | 4385.72 | 4.43 | 0.0010 | 1.69 | |
| (p)(s)(e) | 4913.24 | 4 | 1228.31 | 1.24 | 0.2985 | 0.97 | |
| (f)(s)(e) | 0 | 0 | 0 | 0 | 0 | 0 | |
| (p)(f)(s)(s)(e) | 0 | 0 | 0 | 0 | 0 | 0 |
| Face | Levels | Size Universe | Description | Variance | Model Generalizability | G Relative | G Absolute |
|---|---|---|---|---|---|---|---|
| (p) | 2 | INF | participants | 26.832 | (f) (s) (e)/(p) | 0.806 | 0.661 |
| (f) | 3 | INF | phases | 24.170 | (s) (e) (p)/(f) | 0.965 | 0.866 |
| (s) | 6 | INF | session | 10.340 | (p) (f) (e)/(s) | 0.961 | 0.939 |
| (e) | 10 | INF | test | 10.745 | (p) (f) (s)/(e) | 0.988 | 0.975 |
| Face | Levels | Size Universe | Description | Variance | Model Generalizability | G Relative | G Absolute |
|---|---|---|---|---|---|---|---|
| (p) | 2 | INF | participants | 19.624 | (f) (s) (e)/(p) | 0.776 | 0.675 |
| (f) | 3 | INF | phases | 31.918 | (s) (e) (p)/(f) | 0.922 | 0.781 |
| (s) | 6 | INF | session | 11.148 | (p) (f) (e)/(s) | 0.963 | 0.939 |
| (e) | 10 | INF | test | 5.547 | (p) (f) (s)/(e) | 0.992 | 0.986 |
| Electromyographic Activity (µV) | ||||||
|---|---|---|---|---|---|---|
| Values | Testing | M | SD | S | K | S-W |
| Maximums | Without biofeedback | 158.53 | 48.97 | 1.61 | 2.98 | 0.85 *** |
| With biofeedback | 227.80 | 82.86 | 1.44 | 2.01 | 0.86 *** | |
| Mean | Without biofeedback | 103.67 | 38.69 | 0.72 | 1.14 | 0.93 ** |
| With biofeedback | 144.58 | 59.36 | 2.57 | 2.21 | 0.70 *** | |
| Electromyographic Activity (µV) | ||||||
|---|---|---|---|---|---|---|
| Values | Session | M | SD | S | K | S-W |
| Maximums | 1 | 99.62 | 21.18 | −0.48 | −0.97 | 0.92 |
| 8 | 247.24 | 71.66 | 0.55 | −1.10 | 0.93 | |
| Mean | 1 | 48.85 | 10.27 | 0.12 | −1.04 | 0.95 |
| 8 | 186.63 | 58.35 | 0.24 | −1.51 | 0.91 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales-Sánchez, V.; Reigal, R.E.; García-Morales, V.; Hernández-Mendo, A.; Falcó, C. Neuromuscular Rehabilitation of the Brachioradialis Muscle after Distal Radius Fracture in Two Professional Soccer Players Using Electromyographic Biofeedback. Muscles 2024, 3, 16-27. https://doi.org/10.3390/muscles3010003
Morales-Sánchez V, Reigal RE, García-Morales V, Hernández-Mendo A, Falcó C. Neuromuscular Rehabilitation of the Brachioradialis Muscle after Distal Radius Fracture in Two Professional Soccer Players Using Electromyographic Biofeedback. Muscles. 2024; 3(1):16-27. https://doi.org/10.3390/muscles3010003
Chicago/Turabian StyleMorales-Sánchez, Verónica, Rafael E. Reigal, Verónica García-Morales, Antonio Hernández-Mendo, and Coral Falcó. 2024. "Neuromuscular Rehabilitation of the Brachioradialis Muscle after Distal Radius Fracture in Two Professional Soccer Players Using Electromyographic Biofeedback" Muscles 3, no. 1: 16-27. https://doi.org/10.3390/muscles3010003