
A Straightforward Approach to Analyze Skeletal Muscle MRI in Limb-Girdle Muscular Dystrophy for Differential Diagnosis: A Systematic Review

Abstract
:1. Introduction
2. Results
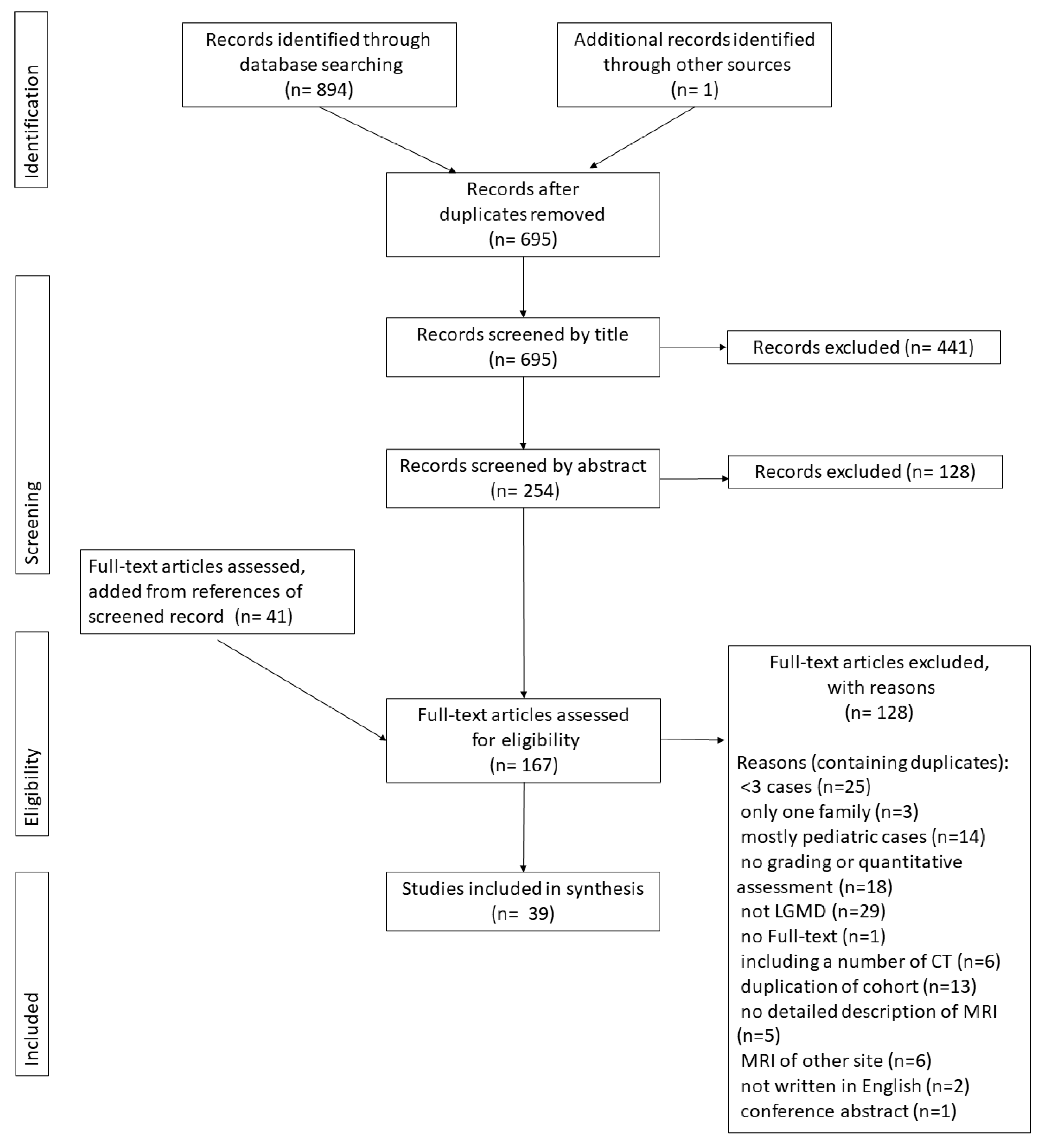
2.1. Study Selection
2.2. Demographic Data
2.3. MRI Sequence
2.4. Grading System
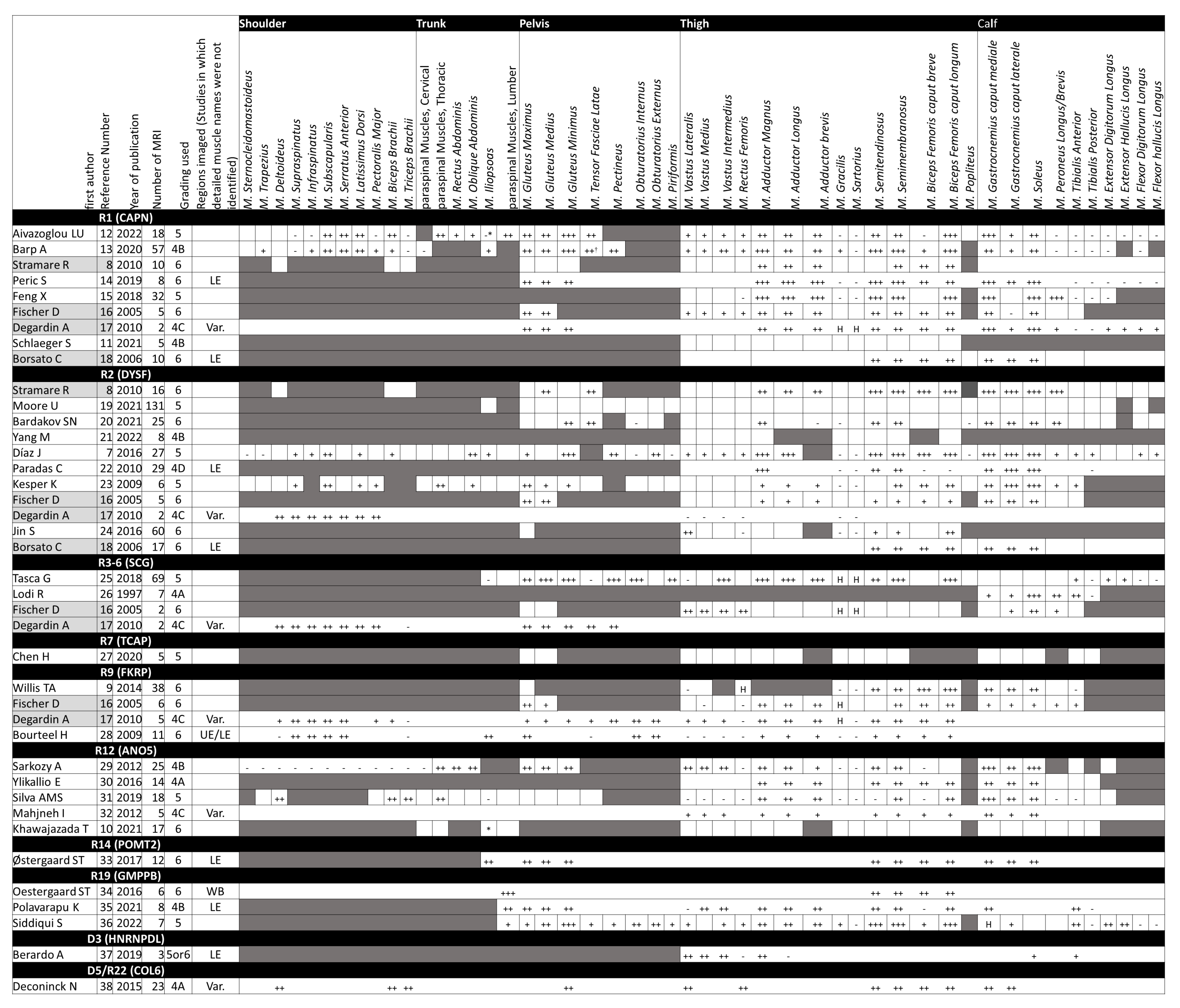
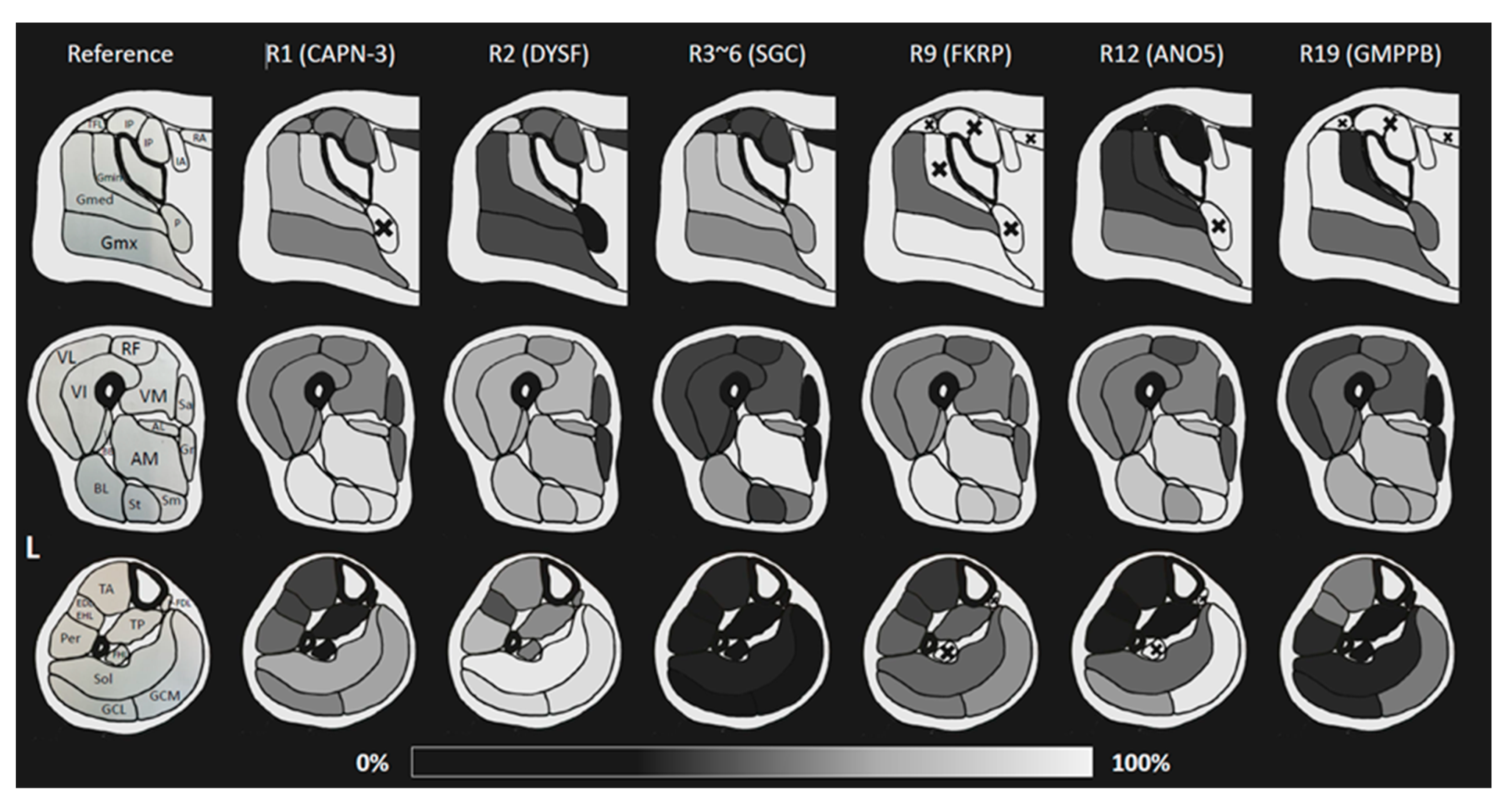
2.5. Synthesis and Summary of Results in Each Anatomical Region
2.6. Pelvis
2.7. Thigh
2.8. Calf
2.9. Upper Limb and Upper Girdle
2.10. Body Trunk
2.11. Pattern of Intramuscular Fatty Infiltration
2.12. Myoedema
3. Method
3.1. Database Search
- (1)
- Studies not involving human subjects;
- (2)
- Clinical trials;
- (3)
- Studies that excluded clinical information;
- (4)
- Studies not involving conditions classified as LGMD in the ENMC2017 workshop [1];
- (5)
- Studies not dealing with skeletal muscle MRI;
- (6)
- Studies written in languages other than English;
- (7)
- Reviews, Editorials, and Response letters;
- (8)
- Fewer than 3 patients or only 1 family being scanned;
- (9)
- No definitive genetic or histochemical diagnosis.
- (1)
- More than half of the patients are adults (18 years or older);
- (2)
- If the condition in (1) is unknown or most patients are under 18, the study must be limited to patients at least 10 years of age.
3.2. Data Extraction
3.3. Data Synthesis and Analysis
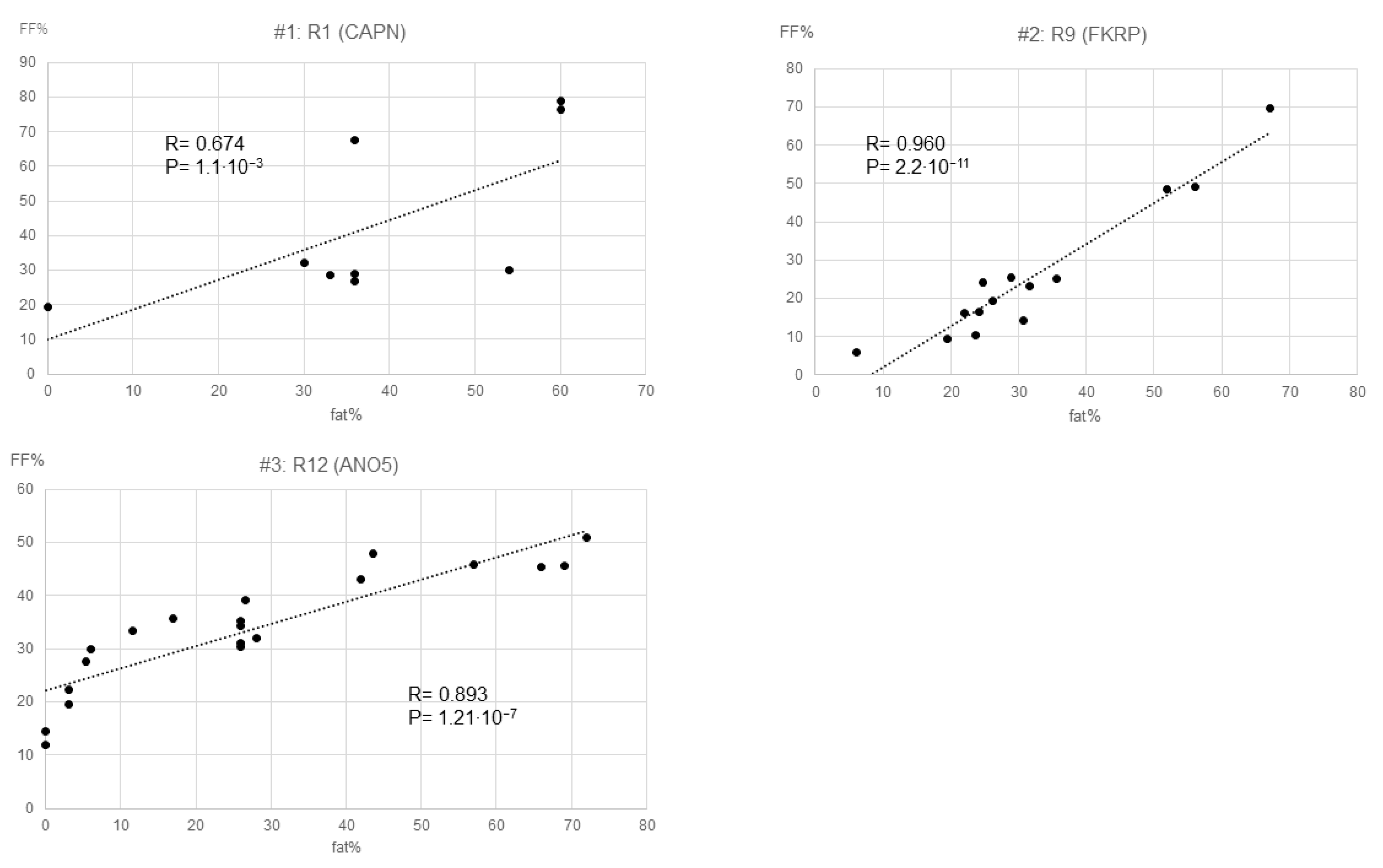
3.3.1. Fat Infiltration
3.3.2. Myoedema
3.3.3. Additional Analytic Points
4. Discussion
- (1).
- Newly noted in our study, which has not been reported in previous MRI studies:
- #1.
- Gmed is more likely to be affected in R19 and Gmx in R12;
- #2.
- TFL is impaired in R2;
- #3.
- RF is relatively preserved in R12;
- #4.
- VL is preserved in R19;
- #5.
- Hypertrophy of Gr/Sar is likely to be observed in R1 and R3–6;
- #6.
- BFLH impairment is prominent in R9;
- #7.
- In R2 and R12, lower leg involvement is evident;
- #8.
- The impairment of Sol in R2 and GCM in R1/R9/R12/R19 is notable, especially in R12;
- #9.
- R2/R19 is also apt to involve the TA/Per/EDL;
- #10.
- In R1, SA is impaired, and ISP is preserved, but in R2, the pattern is reversed;
- #11.
- A specific finding may be the later-medial, cauda-cranial gradient of the paraspinal muscles in R1.
- (2).
- Comparison with results of the previous 2023 Systematic ReviewsThe previously described patterns, confirmed in our study:
- #1.
- Muscle selectivity in the involvement of the gluteus maximus muscle group is very useful for differentiation. Gmin is most likely affected by R1/R2, whereas Gmx is most likely affected by R9;
- #2.
- It is generally expected to have less involvement of the Sa and Gr muscles (with a few exceptions);
- #3.
- In R3–6, the lower leg is spared even in the later stages. If impaired, TA is typical;
- #4.
- In R1/R9, TA is preserved even in the late stage;
- #5.
- The Gastrocnemius caput laterale (GCL) is relatively preserved in R1.
- (3).
- Findings mentioned in the previous 2023 studies and not pursued in our study:
- #1.
- If there is no accentuation of degeneration of the gluteus muscle group, R12/R19 if the gluteus muscle group is less degenerative than other parts of the body, otherwise R9 is the differential [4];
- #2.
- R12 has a patchy rather than homogeneous distribution of fatty infiltration in the thighs [4];
- #3.
- Biceps femoris short head (BFSH) will likely be spared in R12 [4];
- #4.
- TA and tibialis posterior (TP) are key muscles of differentiation in the lower leg; TP is impaired in R19 [4];
- #5.
- R3–6 shows a concentric fatty infiltration pattern (VL, RF, and Vastus medialis (VM) outer areas are spared, while others have degenerated) [2];
- #6.
- Concentric fatty infiltration is seen in the distal femur, even in R9 [2].
4.1. For Genotypes Not Addressed in This Study
4.2. Advantages of Our Systematic Review and Future Recommendations
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Straub, V.; Murphy, A.; Udd, B.; LGMD Workshop Study Group. 229th ENMC international workshop: Limb girdle muscular dystrophies—Nomenclature and reformed classification Naarden, the Netherlands, 17–19 March 2017. Neuromuscul. Disord. 2018, 28, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Dahlqvist, J.R.; Widholm, P.; Leinhard, O.D.; Vissing, J. MRI in Neuromuscular Diseases: An Emerging Diagnostic Tool and Biomarker for Prognosis and Efficacy. Ann. Neurol. 2020, 88, 669–681. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.G. Magnetic resonance imaging patterns of muscle involvement in genetic muscle diseases: A systematic review. J. Neurol. 2017, 264, 1320–1333. [Google Scholar] [CrossRef] [PubMed]
- Alawneh, I.; Stosic, A.; Gonorazky, H. Muscle MRI patterns for limb girdle muscle dystrophies: Systematic review. J. Neurol. 2023, 270, 3946–3957. [Google Scholar] [CrossRef] [PubMed]
- Stramare, R.; Beltrame, V.; Dal Borgo, R.; Gallimberti, L.; Frigo, A.C.; Pegoraro, E.; Angelini, C.; Rubaltelli, L.; Feltrin, G.P. MRI in the assessment of muscular pathology: A comparison between limb-girdle muscular dystrophies, hyaline body myopathies and myotonic dystrophies. Radiol. Medica 2010, 115, 585–599. [Google Scholar] [CrossRef]
- Schlaeger, S.; Sollmann, N.; Zoffl, A.; Becherucci, E.A.; Weidlich, D.; Kottmaier, E.; Riederer, I.; Greve, T.; Montagnese, F.; Deschauer, M.; et al. Quantitative Muscle MRI in Patients with Neuromuscular Diseases-Association of Muscle Proton Density Fat Fraction with Semi-Quantitative Grading of Fatty Infiltration and Muscle Strength at the Thigh Region. Diagnostics 2021, 11, 1056. [Google Scholar] [CrossRef]
- Aivazoglou, L.U.; Guimarães, J.B.; Costa, M.A.F.; Aihara, A.Y.; Cardoso, F.N.; Pinto, W.; de Souza, P.V.S.; de Silva, A.M.S.; Zanoteli, E.; Olivieira, A.S.B.; et al. Whole-Body MRI in Limb Girdle Muscular Dystrophy Type R1/2A: Correlation with Clinical Scores. Muscle Nerve 2022, 66, 471–478. [Google Scholar] [CrossRef]
- Barp, A.; Laforet, P.; Bello, L.; Tasca, G.; Vissing, J.; Monforte, M.; Ricci, E.; Choumert, A.; Stojkovic, T.; Malfatti, E.; et al. European muscle MRI study in limb girdle muscular dystrophy type R1/2A (LGMDR1/LGMD2A). J. Neurol. 2020, 267, 45–56. [Google Scholar] [CrossRef]
- Peric, S.; Stevanovic, J.; Johnson, K.; Kosac, A.; Peric, M.; Brankovic, M.; Marjanovic, A.; Jankovic, M.; Banko, B.; Milenkovic, S.; et al. Phenotypic and genetic spectrum of patients with limb-girdle muscular dystrophy type 2A from Serbia. Acta Myol. 2019, 38, 163–171. [Google Scholar]
- Feng, X.; Luo, S.; Li, J.; Yue, D.; Xi, J.; Zhu, W.; Gao, X.; Guan, X.; Lu, J.; Liang, Z.; et al. Fatty infiltration evaluation and selective pattern characterization of lower limbs in limb-girdle muscular dystrophy type 2A by muscle magnetic resonance imaging. Muscle Nerve 2018, 58, 536–541. [Google Scholar] [CrossRef]
- Fischer, D.; Walter, M.C.; Kesper, K.; Petersen, J.A.; Aurino, S.; Nigro, V.; Kubisch, C.; Meindl, T.; Lochmüller, H.; Wilhelm, K.; et al. Diagnostic value of muscle MRI in differentiating LGMD2I from other LGMDs. J. Neurol. 2005, 252, 538–547. [Google Scholar] [CrossRef]
- Degardin, A.; Morillon, D.; Lacour, A.; Cotten, A.; Vermersch, P.; Stojkovic, T. Morphologic imaging in muscular dystrophies and inflammatory myopathies. Skelet. Radiol. 2010, 39, 1219–1227. [Google Scholar] [CrossRef] [PubMed]
- Borsato, C.; Padoan, R.; Stramare, R.; Fanin, M.; Angelini, C. Limb-Girdle muscular distrophies type 2A and 2B: Clinical and radiological aspects. Basic Appl. Myol. 2006, 16, 17–25. [Google Scholar]
- Díaz, J.; Woudt, L.; Suazo, L.; Garrido, C.; Caviedes, P.; CÁrdenas, A.M.; Castiglioni, C.; Bevilacqua, J.A. Broadening the imaging phenotype of dysferlinopathy at different disease stages. Muscle Nerve 2016, 54, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Moore, U.; Gordish, H.; Diaz-Manera, J.; James, M.K.; Mayhew, A.G.; Guglieri, M.; Fernandez-Torron, R.; Rufibach, L.E.; Feng, J.; Blamire, A.M.; et al. Miyoshi myopathy and limb girdle muscular dystrophy R2 are the same disease. Neuromuscul. Disord. 2021, 31, 265–280. [Google Scholar] [CrossRef]
- Bardakov, S.N.; Tsargush, V.A.; Carlier, P.G.; Nikitin, S.S.; Kurbatov, S.A.; Titova, A.A.; Umakhanova, Z.R.; Akhmedova, P.G.; Magomedova, R.M.; Zheleznyak, I.S.; et al. Magnetic resonance imaging pattern variability in dysferlinopathy. Acta Myol. Myopathies Cardiomyopathies Off. J. Mediterr. Soc. Myol. 2021, 40, 158–171. [Google Scholar] [CrossRef]
- Yang, M.; Ji, S.; Xu, L.; Zhang, Q.; Li, Y.; Gao, H.; Bu, B. The Clinicopathological Distinction between Immune-Mediated Necrotizing Myopathy and Limb-Girdle Muscular Dystrophy R2: Key Points to Prevent Misdiagnosis. J. Clin. Med. 2022, 11, 6566. [Google Scholar] [CrossRef]
- Paradas, C.; Llauger, J.; Diaz-Manera, J.; Rojas-Garcia, R.; De Luna, N.; Iturriaga, C.; Márquez, C.; Usón, M.; Hankiewicz, K.; Gallardo, E.; et al. Redefining dysferlinopathy phenotypes based on clinical findings and muscle imaging studies. Neurology 2010, 75, 316–323. [Google Scholar] [CrossRef]
- Kesper, K.; Kornblum, C.; Reimann, J.; Lutterbey, G.; Schroder, R.; Wattjes, M.P. Pattern of skeletal muscle involvement in primary dysferlinopathies: A whole-body 3.0-T magnetic resonance imaging study. Acta Neurol. Scand. 2009, 120, 111–118. [Google Scholar] [CrossRef]
- Jin, S.; Du, J.; Wang, Z.; Zhang, W.; Lv, H.; Meng, L.; Xiao, J.; Yuan, Y. Heterogeneous characteristics of MRI changes of thigh muscles in patients with dysferlinopathy. Muscle Nerve 2016, 54, 1072–1079. [Google Scholar] [CrossRef]
- Tasca, G.; Monforte, M.; Diaz-Manera, J.; Brisca, G.; Semplicini, C.; D’Amico, A.; Fattori, F.; Pichiecchio, A.; Berardinelli, A.; Maggi, L.; et al. MRI in sarcoglycanopathies: A large international cohort study. J. Neurol. Neurosurg. Psychiatry 2018, 89, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Lodi, R.; Muntoni, F.; Taylor, J.; Kumar, S.; Sewry, C.A.; Blamire, A.; Styles, P.; Taylor, D.J. Correlative MR imaging and 31P-MR spectroscopy study in sarcoglycan deficient limb girdle muscular dystrophy. Neuromuscul. Disord. 1997, 7, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Xu, G.; Lin, F.; Jin, M.; Cai, N.; Qiu, L.; Ye, Z.; Wang, L.; Lin, M.; Wang, N. Clinical and genetic characterization of limb girdle muscular dystrophy R7 telethonin-related patients from three unrelated Chinese families. Neuromuscul. Disord. 2020, 30, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Willis, T.A.; Hollingsworth, K.G.; Coombs, A.; Sveen, M.L.; Andersen, S.; Stojkovic, T.; Eagle, M.; Mayhew, A.; de Sousa, P.L.; Dewar, L.; et al. Quantitative magnetic resonance imaging in limb-girdle muscular dystrophy 2I: A multinational cross-sectional study. PLoS ONE 2014, 9, e90377. [Google Scholar] [CrossRef]
- Bourteel, H.; Vermersch, P.; Cuisset, J.M.; Maurage, C.A.; Laforet, P.; Richard, P.; Stojkovic, T. Clinical and mutational spectrum of limb-girdle muscular dystrophy type 2I in 11 French patients. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1405–1408. [Google Scholar] [CrossRef]
- Khawajazada, T.; Kass, K.; Rudolf, K.; de Stricker Borch, J.; Sheikh, A.M.; Witting, N.; Vissing, J. Muscle involvement assessed by quantitative magnetic resonance imaging in patients with anoctamin 5 deficiency. Eur. J. Neurol. 2021, 28, 3121–3132. [Google Scholar] [CrossRef]
- Sarkozy, A.; Deschauer, M.; Carlier, R.Y.; Schrank, B.; Seeger, J.; Walter, M.C.; Schoser, B.; Reilich, P.; Leturq, F.; Radunovic, A.; et al. Muscle MRI findings in limb girdle muscular dystrophy type 2L. Neuromuscul. Disord. 2012, 22 (Suppl. S2), S122–S129. [Google Scholar] [CrossRef]
- Ylikallio, E.; Auranen, M.; Mahjneh, I.; Lamminen, A.; Kousi, M.; Träskelin, A.L.; Muurinen, T.; Löfberg, M.; Salmi, T.; Paetau, A.; et al. Decreased Aerobic Capacity in ANO5-Muscular Dystrophy. J. Neuromuscul. Dis. 2016, 3, 475–485. [Google Scholar] [CrossRef]
- Silva, A.M.S.; Coimbra-Neto, A.R.; Souza, P.V.S.; Winckler, P.B.; Gonçalves, M.V.M.; Cavalcanti, E.B.U.; Carvalho, A.; Sobreira, C.; Camelo, C.G.; Mendonça, R.D.H.; et al. Clinical and molecular findings in a cohort of ANO5-related myopathy. Ann. Clin. Transl. Neurol. 2019, 6, 1225–1238. [Google Scholar] [CrossRef]
- Mahjneh, I.; Bashir, R.; Kiuru-Enari, S.; Linssen, W.; Lamminen, A.; Visser, M. Selective pattern of muscle involvement seen in distal muscular dystrophy associated with anoctamin 5 mutations: A follow-up muscle MRI study. Neuromuscul. Disord. 2012, 22 (Suppl. S2), S130–S136. [Google Scholar] [CrossRef]
- Østergaard, S.T.; Johnson, K.; Stojkovic, T.; Krag, T.; De Ridder, W.; De Jonghe, P.; Baets, J.; Claeys, K.G.; Fernández-Torrón, R.; Phillips, L.; et al. Limb girdle muscular dystrophy due to mutations in POMT2. J. Neurol. Neurosurg. Psychiatry 2018, 89, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Oestergaard, S.T.; Stojkovic, T.; Dahlqvist, J.R.; Bouchet-Seraphin, C.; Nectoux, J.; Leturcq, F.; Cossée, M.; Solé, G.; Thomsen, C.; Krag, T.O.; et al. Muscle involvement in limb-girdle muscular dystrophy with GMPPB deficiency (LGMD2T). Neurol. Genet. 2016, 2, e112. [Google Scholar] [CrossRef] [PubMed]
- Polavarapu, K.; Mathur, A.; Joshi, A.; Nashi, S.; Preethish-Kumar, V.; Bardhan, M.; Sharma, P.; Parveen, S.; Seth, M.; Vengalil, S.; et al. A founder mutation in the GMPPB gene [c.1000G > A (p.Asp334Asn)] causes a mild form of limb-girdle muscular dystrophy/congenital myasthenic syndrome (LGMD/CMS) in South Indian patients. Neurogenetics 2021, 22, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, S.; Polavarapu, K.; Bardhan, M.; Preethish-Kumar, V.; Joshi, A.; Nashi, S.; Vengalil, S.; Raju, S.; Chawla, T.; Leena, S.; et al. Distinct and Recognisable Muscle MRI Pattern in a Series of Adults Harbouring an Identical GMPPB Gene Mutation. J. Neuromuscul. Dis. 2022, 9, 95–109. [Google Scholar] [CrossRef]
- Berardo, A.; Lornage, X.; Johari, M.; Evangelista, T.; Cejas, C.; Barroso, F.; Dubrovsky, A.; Bui, M.T.; Brochier, G.; Saccoliti, M.; et al. HNRNPDL-related muscular dystrophy: Expanding the clinical, morphological and MRI phenotypes. J. Neurol. 2019, 266, 2524–2534. [Google Scholar] [CrossRef]
- Deconinck, N.; Richard, P.; Allamand, V.; Behin, A.; Lafôret, P.; Ferreiro, A.; de Becdelievre, A.; Ledeuil, C.; Gartioux, C.; Nelson, I.; et al. Bethlem myopathy: Long-term follow-up identifies COL6 mutations predicting severe clinical evolution. J. Neurol. Neurosurg. Psychiatry 2015, 86, 1337–1346. [Google Scholar] [CrossRef]
- Arrigoni, F.; De Luca, A.; Velardo, D.; Magri, F.; Gandossini, S.; Russo, A.; Froeling, M.; Bertoldo, A.; Leemans, A.; Bresolin, N.; et al. Multiparametric quantitative MRI assessment of thigh muscles in limb-girdle muscular dystrophy 2A and 2B. Muscle Nerve 2018, 58, 550–558. [Google Scholar] [CrossRef]
- Forsting, J.; Rohm, M.; Froeling, M.; Güttsches, A.K.; Südkamp, N.; Roos, A.; Vorgerd, M.; Schlaffke, L.; Rehmann, R. Quantitative muscle MRI captures early muscle degeneration in calpainopathy. Sci. Rep. 2022, 12, 19676. [Google Scholar] [CrossRef]
- Reyngoudt, H.; Marty, B.; Boisserie, J.M.; Le Louer, J.; Koumako, C.; Baudin, P.Y.; Wong, B.; Stojkovic, T.; Béhin, A.; Gidaro, T.; et al. Global versus individual muscle segmentation to assess quantitative MRI-based fat fraction changes in neuromuscular diseases. Eur. Radiol. 2021, 31, 4264–4276. [Google Scholar] [CrossRef]
- Revsbech, K.L.; Rudolf, K.; Sheikh, A.M.; Khawajazada, T.; de Stricker Borch, J.; Dahlqvist, J.R.; Løkken, N.; Witting, N.; Vissing, J. Axial muscle involvement in patients with Limb girdle muscular dystrophy type R9. Muscle Nerve 2022, 65, 405–414. [Google Scholar] [CrossRef]
- Løkken, N.; Hedermann, G.; Thomsen, C.; Vissing, J. Contractile properties are disrupted in Becker muscular dystrophy, but not in limb girdle type 2I. Ann. Neurol. 2016, 80, 466–471. [Google Scholar] [CrossRef] [PubMed]
- De Wel, B.; Huysmans, L.; Peeters, R.; Goosens, V.; Ghysels, S.; Byloos, K.; Putzeys, G.; D’Hondt, A.; De Bleecker, J.L.; Dupont, P.; et al. Two-Years Prospective Natural History Study in 24 Adult LGMDR12 Patients: Clinical and Radiological Outcome Measures. J. Neuromuscul. Dis. 2022, 9 (Suppl. S1), S170. [Google Scholar] [CrossRef]
- Salim, R.; Dahlqvist, J.R.; Khawajazada, T.; Kass, K.; Revsbech, K.L.; de Stricker Borch, J.; Munawar Sheikh, A.; Vissing, J. Characteristic muscle signatures assessed by quantitative MRI in patients with Bethlem myopathy. J. Neurol. 2020, 267, 2432–2442. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Wattjes, M.P.; Kley, R.A.; Fischer, D. Neuromuscular imaging in inherited muscle diseases. Eur. Radiol. 2010, 20, 2447–2460. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, E.; Cini, C.; Counsell, S.; Allsop, J.; Zolkipli, Z.; Jungbluth, H.; Sewry, C.; Brown, S.C.; Pepe, G.; Muntoni, F. Muscle MRI findings in a three-generation family affected by Bethlem myopathy. Eur. J. Paediatr. Neurol. 2002, 6, 309–314. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Qualitative Study (with Grading System) | Quantitative Study (Fat Fraction, FF%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall | Fat% Calculation | ||||||||
| N of Study | N of Case | Synthetic Mean | N of Study | N of Case | Synthetic Mean | N of Study | N of Case | Synthetic Mean | |
| R1 (CAPN) | 9 | 159 | 7 | 128 | 3 | 35 | |||
| Mean age | 9 | 159 | 33.8 | 7 | 128 | 35.1 | 3 | 35 | 40.9 |
| Mean duration | 6 | 60 | 14.0 | 4 | 38 | 15.9 | 3 | 35 | 18.9 |
| Male% | 8 | 156 | 47.7 | 7 | 128 | 48.8 | 3 | 35 | 41.6 |
| R2 (DYSF) | 11 | 364 | 9 | 2 | 21 | ||||
| Mean age | 11 | 364 | 34.2 | 9 | 333 | 34.4 | 1 | 9 | 49.4 |
| Mean duration | 9 | 321 | 12.8 | 7 | 292 | 13.2 | 1 | 9 | 25.7 |
| Male% | 9 | 333 | 51.3 | 9 | 333 | 51.3 | 2 | 21 | 40.2 |
| R3–6 (SCG) | 4 | 81 | 3 | 78 | |||||
| Mean age | 4 | 81 | 22.8 | 3 | 78 | 22.5 | |||
| Mean duration | 4 | 81 | 13.2 | 3 | 78 | 12.8 | |||
| Male% | 3 | 78 | 50.0 | 3 | 78 | 50.0 | |||
| R9 (FKRP) | 4 | 62 | 2 | 44 | 4 | 70 | |||
| Mean age | 4 | 62 | 38.4 | 2 | 44 | 40.6 | 3 | 63 | 39.4 |
| Mean duration | 4 | 62 | 20.0 | 2 | 44 | 19.3 | 3 | 63 | 19.5 |
| Male% | 3 | 55 | 49.1 | 2 | 44 | 43.3 | 4 | 70 | 50.0 |
| R12 (ANO5) | 5 | 98 | 5 | 98 | 2 | 41 | |||
| Mean age | 5 | 98 | 48.0 | 5 | 98 | 48.0 | 2 | 41 | 47.1 |
| Mean duration | 5 | 98 | 13.4 | 5 | 98 | 13.4 | 2 | 41 | 15.7 |
| Male% | 5 | 98 | 71.4 | 5 | 98 | 71.4 | 2 | 41 | 73.1 |
| R19 (GMPPB) | 3 | 25 | |||||||
| Mean age | 3 | 25 | 42.4 | ||||||
| Mean duration | 3 | 25 | 20.0 | ||||||
| Male% | 3 | 25 | 52.0 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morishima, R.; Schoser, B. A Straightforward Approach to Analyze Skeletal Muscle MRI in Limb-Girdle Muscular Dystrophy for Differential Diagnosis: A Systematic Review. Muscles 2023, 2, 374-388. https://doi.org/10.3390/muscles2040029
Morishima R, Schoser B. A Straightforward Approach to Analyze Skeletal Muscle MRI in Limb-Girdle Muscular Dystrophy for Differential Diagnosis: A Systematic Review. Muscles. 2023; 2(4):374-388. https://doi.org/10.3390/muscles2040029
Chicago/Turabian StyleMorishima, Ryo, and Benedikt Schoser. 2023. "A Straightforward Approach to Analyze Skeletal Muscle MRI in Limb-Girdle Muscular Dystrophy for Differential Diagnosis: A Systematic Review" Muscles 2, no. 4: 374-388. https://doi.org/10.3390/muscles2040029