
Non-Multisystem Inflammatory Syndrome in Children—Postacute Sequelae of Paediatric COVID-19: Autoimmune or Autoinflammatory? A Systematic Review of the Reported Cases
 ,
,  , ,
, ,
Abstract
:1. Introduction
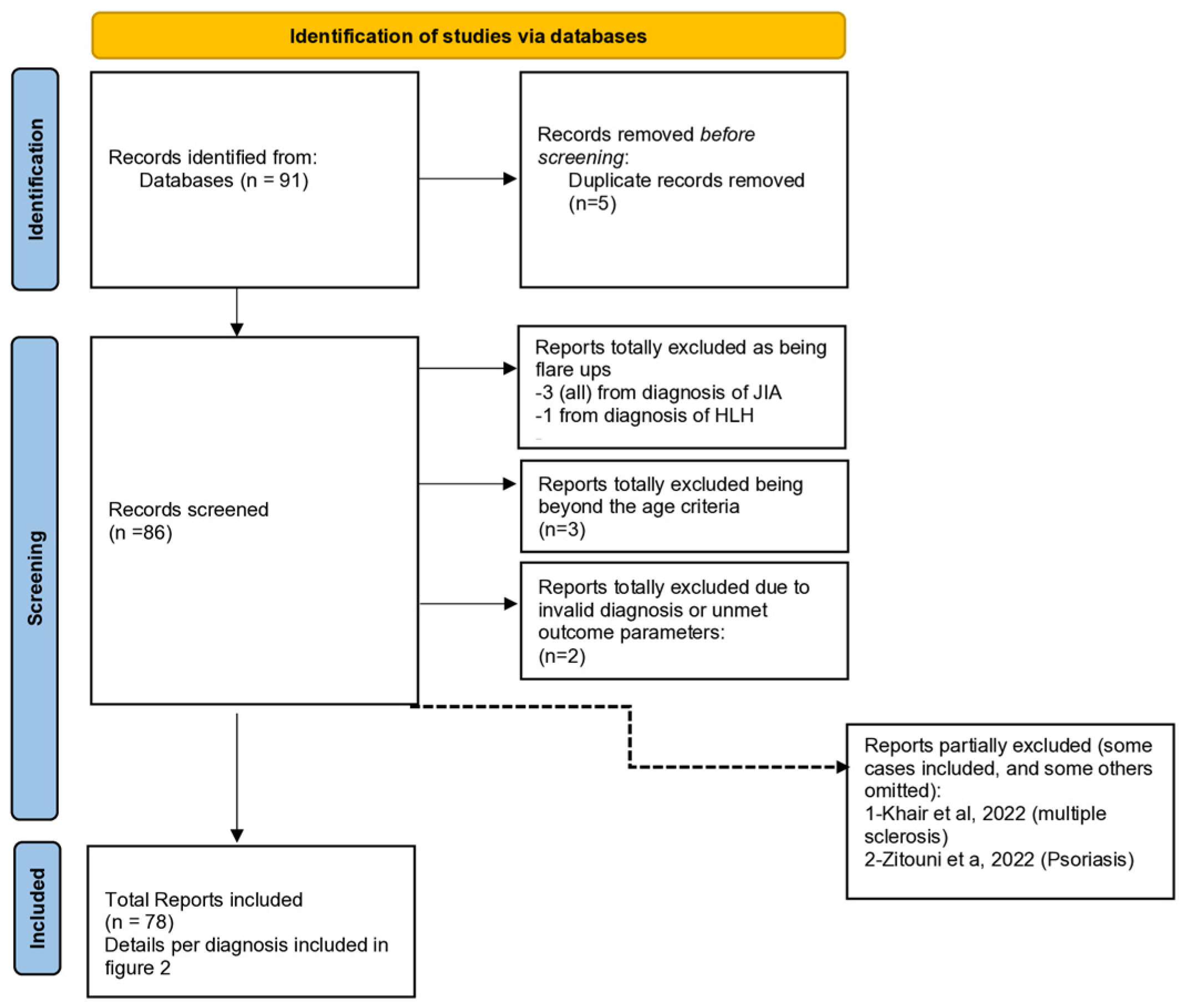
2. Materials and Methods
2.1. Databases Used
2.2. Search Terms Inclusion and Exclusion Criteria
2.2.1. Inclusion Criteria
- 1.
- Diagnoses
- 2.
- Age: 0–18 Years
2.2.2. Exclusion Criteria
- −
- Any case with a multi-inflammatory syndrome of children (MIS-C) or Kawasaki disease was excluded, and any flare-up of a pre-existing autoinflammatory condition was excluded.
- −
- Any case not addressing the outcome parameters was excluded.
2.2.3. Outcome Parameters
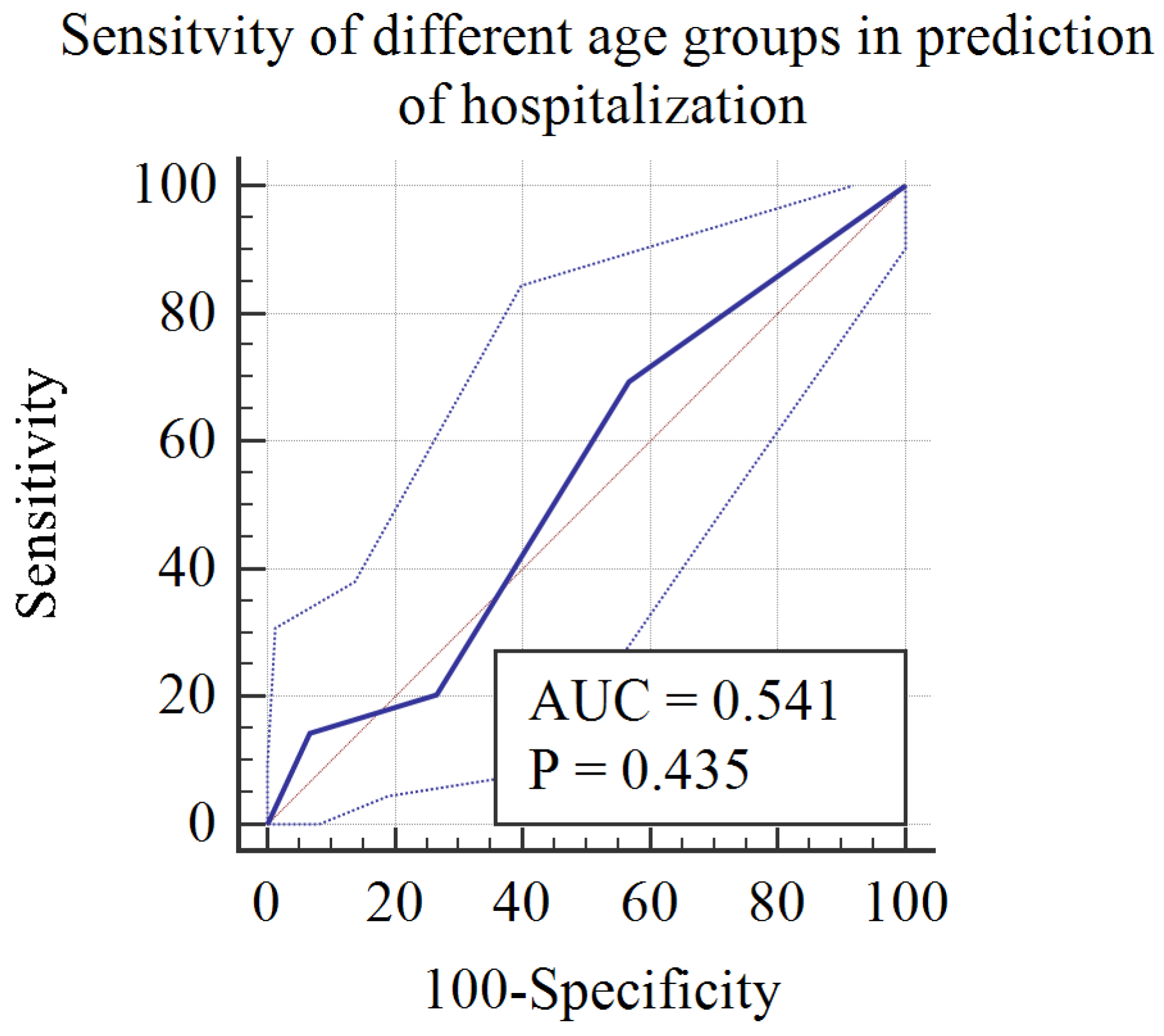
3. Statistical Analyses
4. Results
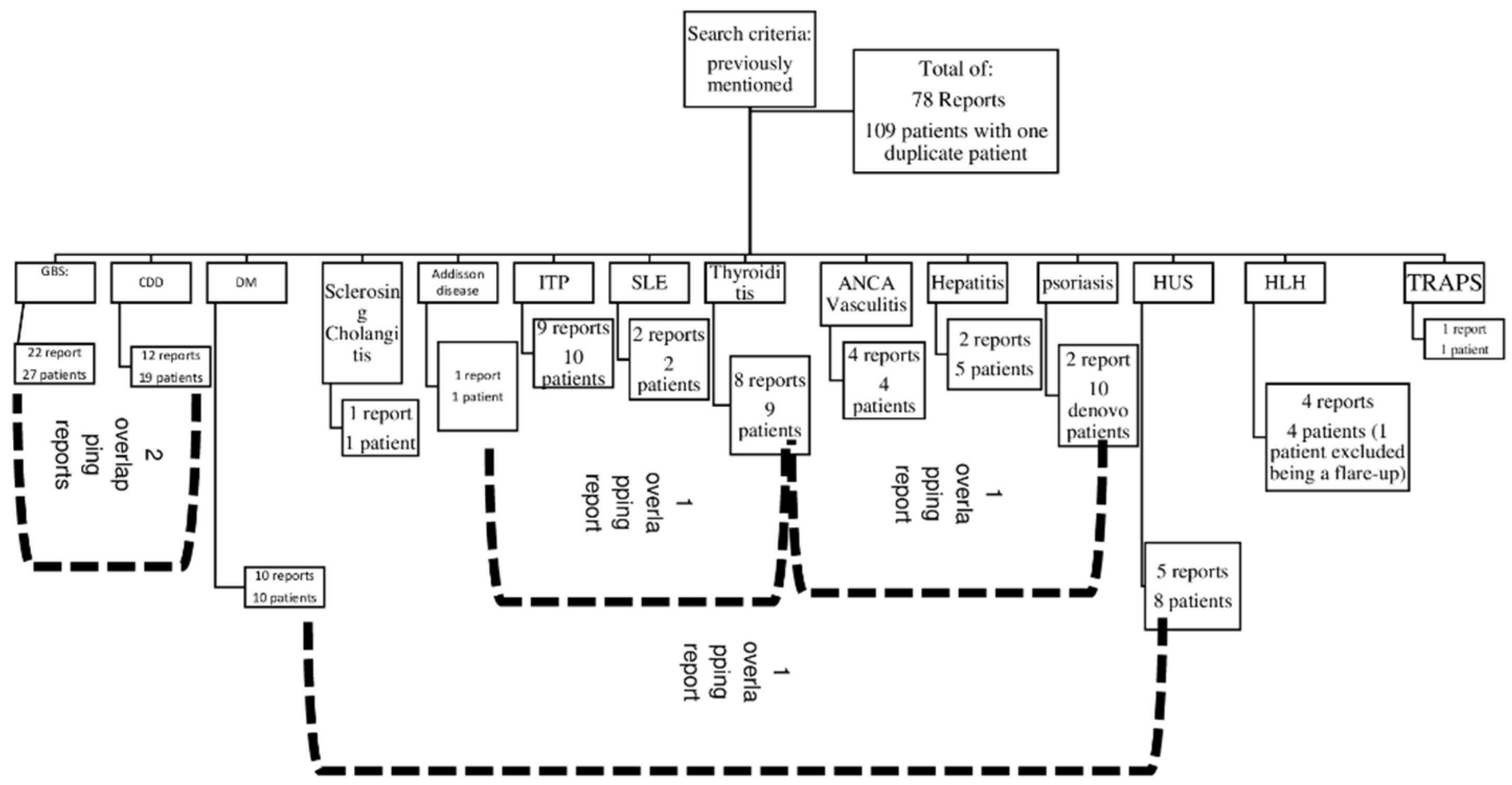
4.1. Overall Results
4.2. Individual Results (by Alphabetical Order of the Respective Autoimmune Disorder)
4.2.1. Addison’s Disease (Table 2)
4.2.2. Anti-Neutrophil Cytoplasmic Antibody (Table 3)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Age (Years) | Sex | Interval between COVID-19 Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [17] | 17 | Male | 7 days | Presented with fever, drenching night sweats, cough, nasal congestion, haemoptysis, and chest tightness. | Recovered |
|
| [18] | 16 | Female | 7 days | Mild upper respiratory symptoms with anosmia. | Recovered |
|
| [19] | 17 | Male | 60 days |
| Recovered after treatment and resolution of AKI and diffuse alveolar haemorrhage (DAH). |
|
| [20] | 12 | Female | 14 to 28 days | Asymptomatic |
|
|
4.2.3. Central Demyelinating Disorders (Table 4)
| Ref. | Age (Years) | Sex | Interval between Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [22] | 8 | Male | One month | Mild respiratory symptoms. | Complete recovery. |
|
| 13 | Female | 2 months | Fatigue and loss of sense of smell and taste. | Moderate improvement with residual diffuse weakness. |
| |
| 14 | Female | 5 to 6 weeks | Asymptomatic. | Unreported. |
| |
| [23] | 16 | Female | 4 months | Unreported | Patient was placed on Rituximab. Follow-up information unreported. |
|
| [24] | 14 | Male | Positive PCR | Complete strength recovery, persistent hyperreflexia in the left lower limb, right eye papilledema, and increased blind spot. |
| |
| [25] | 14 | Female | 8 weeks | No respiratory involvement | No complications |
|
| 4 | Male | 8 weeks | No respiratory involvement | No complications |
| |
| 3 | Male | 6 weeks | No respiratory involvement | No complications |
| |
| [26] | 16 | Male | At the time of presentation | Asymptomatic | Full recovery |
|
| [27] | 9 | Male | 3 days | Fever, headache, and vomiting | Tracheotomized. Discharged after 60 months of hospital stay with incomplete recovery. |
|
| 9 | Female | 5 days | Fever, vomiting, and diarrhoea | Complete recovery |
| |
| [28] | 10 | Male | During disease course | fever, headache, and myalgia | Incomplete recovery |
|
| [29] | 7 | Female | 1 week | Asymptomatic | Incomplete recovery with resolution of sensory deficits but little improvement in lower limb strength. |
|
| [30] | 12 | Female | 5 days | Skin rash, headache, and fever | Incomplete recovery |
|
| [31] | 6 | Male | 10 days | Asymptomatic | Full recovery |
|
| [32] | 5 | Female | 2 days | Mild cough and fever | Patient received IVIG, showed clinical improvement, and was discharged after two weeks of hospitalization. |
|
| [33] | 15 | Female | During the course of the disease | Fever, headache, and vomiting | Needed hospitalization.Visual acuity fully recovered after treatment. |
|
| 14 | Female | During the course of the disease | Headache, myalgia, and arthralgia | Needed hospitalization. Visual acuity fully recovered after treatment. |
| |
| 14 | Male | During the course of the disease | Asymptomatic | Rankin Score: 0 and absolute control of epilepsy. Presence of psychiatric symptoms post discharge. |
|
4.2.4. Guillain–Barré Syndrome (Table 5)
| Ref. | Age (Years) | Sex | Interval between COVID-19 Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [35] | 3 | Female | 2 weeks | Not specified |
|
|
| [36] | 3 | Female | 1 week | Mild (Flu-like) |
|
|
| [37] | 8 | Male | During the course of COVID-19 infection | Asymptomatic |
|
|
| [38] | 13 | Female | 1 month | Fever |
|
|
| [39] | 11 | Female | Not specified | Fever |
|
|
| [40] | 7 | Male | Not specified | Asymptomatic |
|
|
| [41] | 15 | Male | During the course of COVID-19 infection | Mild (no respiratory symptoms) |
|
|
| [42] | 14 | Female | 3 weeks | Upper respiratory tract infection 3 weeks Earlier. |
|
|
| [43] | 11 | Male | 3 weeks | Vomiting, diarrhoea, abdominal pain, and headache for 3 weeks. |
|
|
| [33] | 9 | Male | Not specified | Asymptomatic |
|
|
| 14 | Male | Not specified | Fever and rhinorrhoea |
|
| |
| 12 | Female | Not specified | Not specified |
|
| |
| [44] | 16 | Female | During the course of COVID-19 infection | Mild |
|
|
| 15 | Male | 15 days | Mild (no respiratory involvement) |
|
| |
| 5 | Female | During the course of the disease | Mild (No respiratory involvement) |
|
| |
| 0.2 | Male | 15 days | Dry cough, fever, and diarrhoea. 15 days later, symptoms developed into dyspnoea and hypoxemia requiring mechanical ventilation. |
|
| |
| [45] | Adolescent (age is not specified) | Male | 2 weeks | Mild; fever |
|
|
| [46] | 4 | Female | 2 weeks | Mild; fever |
|
|
| [47] | 9 | Female | Not specified | Not specified |
|
|
| [48] | 16 | Female | During the course of COVID-19 infection | Asymptomatic |
|
|
| [49] | 9 | Male | During the course of COVID-19 infection | Asymptomatic |
|
|
| [50] | 6 | Male | 1 week | Two days of fever followed by severe respiratory muscle weakness requiring mechanical ventilation. |
|
|
| [51] | 12 | Male | 1 week | Mild and treated symptomatically at home. |
|
|
| [52] | 11 | Male | 20 days | An acute upper respiratory tract infection with low-grade fever treated at home with acetaminophen and azithromycin. Chest CT showed patchy subsegmental faint opacifications with atelectasis in the lingula. |
|
|
| [53] | 6 | Female | 1 month | Asymptomatic |
|
|
| [54] | 17 | Female | 8 days | Fever, nausea, severe vomiting, and diarrhoea. |
|
|
| [24] | 8 | Male | During the course of COVID-19 | Asymptomatic |
|
|
4.2.5. Hepatitis (Table 6)
| Ref. | Age (years) | Sex | Interval between COVID-19 Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [56] | 3 | Female | 21 days |
| Recovered and discharged after 18 days of hospitalization on azathioprine as steroid-sparing maintenance therapy. |
|
| [57] | 0.5 | Female | During the course of COVID-19 infection |
|
|
|
| 0.33 | Male | During the course of COVID-19 infection | Presented to ER with feeding difficulties, vomiting, hypotonia, diaphoresis, and progressive lethargy over 12 h. |
|
| |
| 16 | Female | 3 days | Presented with cough, congestion, and fever. |
|
| |
| 11 | Male | 2 days | Afebrile without other symptoms. |
| Presented with non-bloody, non-bilious emesis and abdominal pain. |
4.2.6. Haemophagocytic Lymphohistiocytosis (Table 7)
| Ref. | Age (years) | Sex | Interval between Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [59] | 5 years | Female | 4.5 weeks | Presented with fever and papular rash for three days. | 8 months in remission. | Condition caused:
|
| [60] | 7 years | Male | 2 weeks | Mild attack. | Recovery after 3 days of steroid therapy. | |
| [61] | 2 years | Male | 2 weeks | The disease course showed feeding intolerance, fever (39.6 °C), diarrhoea, and vomiting for two days. | Monitored in PICU at the time of publishing. |
|
| [62] | 6 weeks | female | During the course | Fever of up to 40 °C and poor feeding. | Recovery. |
|
4.2.7. Haemolytic–Uremic Syndrome (Table 8)
| Ref. | Age | Sex | Interval between Infection and HUS | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [64] | 4 months | Male | 4 weeks | Fever and mild respiratory symptoms. |
|
|
| 4.5 months | Male | During the course of COVID-19 infection | Presented with pyrexia, diarrhoea, and reduced drinking. |
| ||
| [65] | 16 months | Male | During the course of COVID-19 infection | Fever, emesis, and respiratory distress. |
|
|
| [66] | 3 years | Male | During the course of COVID-19 infection | The patient presented with fever, coryza, cough, decreased urine output lasting for 3 days, and a history of non-bloody diarrhoea 1 week prior to admission. |
| |
| [67] 3 patients were excluded as they are flare-ups of pre-existing conditions | 10 years | Female | 10 | Fever without respiratory manifestations. |
| |
| 4 years | Male | 21 |
| |||
| [68] | 6 years | Male | During the course of the disease |
| ||
| 10 years | Male | During the course of the disease | Bloody diarrhoea, oliguria, and thrombocytopenia. |
4.2.8. Immune Thrombocytopenic Purpura (Table 9)
| Ref. | Age (Yrs) | Sex | Interval between Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [70] | 0.75 | Male | During the course of COVID-19 infection | Yes | Recovery after megadose methylprednisolone. | |
| [71] | 8 | Female | During the course of COVID-19 infection | Yes | Recovery after IV methylprednisolone, platelet concentrate, and two doses of IVIG. |
|
| [72] | 5.5 | Female | 22 days | Yes | Hospitalized for 4 weeks. Recovery after prednisolone (tapering dose) and eltrombopag. |
|
| [73] | 11 | Male | 4 weeks | Yes | Recovery after 2 doses of IVIG. |
|
| [74] | 15 | Male | 5 weeks | No | Recovered after IVIG. |
|
| 3 | Female | 3 weeks | No | Recovered after IVIG. |
| |
| [75] (One patient excluded only AIHA) | 16 | Male | 3–4 weeks | No | Recovery after corticosteroid therapy. |
|
| [76] | 1.5 | Female | 5 weeks | No | Recovery after a single dose of IVIG. |
|
| [77] | 10 | Female | 3 weeks | No | Clinical improvement after acetaminophen, diphenhydramine, and IVIG. |
|
| [78] | 12 | Female | During the course of COVID-19 infection | Yes | Recovery after IVIG and corticosteroids. ARDS improved with tocilizumab and remdesivir. |
|
4.2.9. Psoriasis (Table 10)
| Ref. | Age | Sex | Interval between Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [80] | 2.5 yrs | Male | Mean interval of 28 days | Only one of the nine patients needed hospital admission. | Unreported. |
|
| 15 yrs | Male | |||||
| 9 yrs | Male | |||||
| 9 yrs | Female | |||||
| 7 yrs | Male | |||||
| 16 yrs | Female | |||||
| 8 yrs | Male | |||||
| 10 yrs | Male | |||||
| 16 yrs | Female | |||||
| [81] | 13 yrs | Male | 8 weeks | No | Full recovery after receiving topical steroids. |
|
4.2.10. Sclerosing Cholangitis (Table 11)
| Ref. | Age | Sex | Interval between Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [83] | 14 yrs | Male | 8 weeks | Yes |
|
|
4.2.11. Systemic Lupus Erythematosus (Table 12)
| Ref. | Age | Sex | Interval between Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [85] | 13 yrs | Female | 2 months | Yes | Improvement only after receiving six sessions of plasma exchange. |
|
| [86] | 18 yrs | Female | During COVID | Yes | Death. |
|
4.2.12. Thyroiditis (Table 13)
| Ref. | Age | Sex | Interval between COVID-19 Infection and Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [81] | 13 | Male | 56 days | Mild course with low-grade fever, congestion, cough, and body aches that resolved in a few days. |
|
|
| [87] | 16 | Male | 56 days | Presented with a diminished sense of smell, cough, chills, nausea, and fatigue. | Patients improved after methimazole and propranolol. |
|
| [88] | 16 | Female | 3 days |
|
|
|
| [89] | 16 | Male | During the course of the disease |
|
|
|
| [14] | 14 | Female | 21 days |
|
|
|
| [90] | 14 | Female and male twins | 56 days |
|
|
|
| [91] | 18 | Female | 14 days |
|
|
|
| [92] | 3 | Female | 42 days |
|
|
|
4.2.13. Tumour Necrosis Factor Receptor-Associated Periodic Syndrome (Table 14)
| Ref. | Age (Yrs) | Sex | Interval between Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [93] | 6 | Female | 4 months | Asymptomatic |
|
|
4.2.14. Type 1 Diabetes Mellitus (Table 15)
| Ref. | Age (Years) | Sex | Interval between Infection and Autoimmune Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [94] | 10 | Male | 0 | Presented with respiratory distress and drowsiness. |
|
|
| [95] | 13 | Male | During the course of COVID | Afebrile, tachycardic, tachypneic. |
|
|
| 8 | Male | During the course of COVID-19 infection | Afebrile and mildly dehydrated. |
|
| |
| [96] | 12 | Female | 4 days | Presented with rhinorrhea progressing to dry cough, post-tussive non-bilious emesis, shortness of breath, mottled skin, and altered mental status. |
|
|
| [97] | 7 | Male | During the course of COVID-19 infection | Asymptomatic |
|
|
| [98] | 3 | Male | During the course of COVID-19 infection |
|
|
|
| [99] | 16 | Male | During the course of COVID-19 infection. | Mild dyspnoea and productive cough. |
|
|
| [100] | 0.7 | Male | During the course of COVID-19 infection | Tachycardia, tachypnoea, and fever. |
|
|
| [101] | 8 | Female | 8 weeks | Cough, rhinorrhoea, anorexia, and weight loss. |
|
|
| [102] | 15 | Female | During the course of COVID-19 infection | Fever, abdominal pain, and vomiting. |
|
|
| [65] | 16 months | Male | During the course of COVID-19 infection | Fever, emesis, and respiratory distress. |
|
|
5. Discussion
6. Limitations
7. Conclusions and Clinical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| Abbreviation | Definition |
| A-ANCA | acute anti-neutrophil cytoplasmic antibody |
| ACE-2 | angiotensin-converting enzyme 2 |
| ACTH | adrenocorticotropic hormone |
| ADEM | acute disseminated encephalomyelitis |
| AHA | acute haemolytic anaemia |
| AIH | autoimmune hepatitis |
| AIHA | autoimmune haemolytic anaemia |
| AKI | acute kidney injury |
| ALL | acute lymphocytic leukaemia |
| ALT | alanine aminotransferase |
| ANA antibodies | anti-nuclear antibodies |
| ANCA | anti-neutrophil cytoplasmic antibody |
| Anti-MOG | anti-myelin oligodendrocyte glycoprotein |
| Anti-NMDA-R | anti-N-methyl-d-aspartate (NMDA)-receptor encephalitis |
| APS2 | autoimmune polyglandular syndrome type 2 |
| ARDS | acute respiratory distress syndrome |
| AST | aspartate aminotransferase |
| BAL | bronchoalveolar lavage |
| BUN | blood urea nitrogen |
| C-ANCA | cytoplasmic anti-neutrophil cytoplasmic antibody |
| CD | celiac disease |
| CD4+ | cluster of differentiation 4 (a co-receptor for t-helper receptor) |
| CD8+ | cluster of differentiation 8 |
| CDD | central demyelinating disorders |
| CMV | cytomegalovirus |
| COVID | coronavirus disease |
| COVID 19: | coronavirus disease of 2019 |
| Cr | creatinine |
| CSF | cerebrospinal fluid |
| CT | computed tomography |
| CTLA-4 | cytotoxic T-lymphocyte-associated antigen 4 |
| DAMPs | damage-associated molecular patterns |
| DKA | diabetic ketoacidosis |
| DVT | deep venous thrombosis |
| EEG | electroencephalography |
| ER | emergency room |
| FFB | flexible fibreoptic bronchoscopy |
| FiO2 | fraction of inspired oxygen |
| FT3 | free triiodothyronine |
| FT4 | free thyroxine |
| GBS | Guillain–Barré syndrome |
| GCS | Glasgow Coma Scale |
| GGT | bamma-glutamyl transferase |
| Hb | haemoglobin |
| Hct | haematocrit |
| HFNC | high-flow nasal cannula |
| HIV | human immunodeficiency virus |
| HLH | haemophagocytic lymphocytic histiocytosis |
| HUS | haemolytic–uremic syndrome |
| ICU | intensive care unit |
| IFN | interferon |
| INR | international normalized ratio |
| ITP | idiopathic thrombocytopenic purpura |
| ITP | immune thrombocytopenic purpura |
| IV | intravenous |
| IVIG | intravenous immune globulin |
| LETM | longitudinal extensive transverse myelitis |
| MAS | macrophage activation syndrome |
| MERS-CoV | Middle East respiratory syndrome coronavirus |
| MIS-C | multi-inflammatory syndrome of children |
| MPO antibodies | myeloperoxidase antibodies |
| MRI | magnetic resonance imaging |
| MS | multiple sclerosis |
| NK | natural killer cell |
| NKT | natural killer T cell |
| NMSOD | neuromyelitis optica spectrum disorder |
| PAIS | postacute infection sequelae |
| P-ANCA | perinuclear anti-neutrophil cytoplasmic antibody |
| PAS | postacute sequelae |
| PASC | postacute sequelae of COVID-19 |
| PCR | polymerase chain reaction |
| PD-1 | programmed cell death protein 1 |
| PICS | post-intensive care syndrome |
| PICU | paediatric intensive care unit |
| PIS | post-infectious sequelae |
| PR3 antibodies | anti-protease 3 antibodies |
| PSC | primary sclerosing cholangitis |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| SLE | systemic lupus erythematosus |
| T1DM | type 1 diabetes mellitus |
| Tg | thyroglobulin |
| Th1 | T-helper type 1 |
| Th17 | T-helper type 17 |
| TIGIT | T-cell immunoreceptor with Ig and ITIM domains |
| TPO | thyroid peroxidase |
| TRAPS | tumour necrosis factor receptor-associated periodic syndrome |
| Tregs | regulatory T cells |
| TSH | thyroid-stimulating hormone |
| TSI | thyroid-stimulating immunoglobulins |
| UDCA | ursodeoxycholic acid |
| URI | upper respiratory infection |
| VZV | varicella zoster virus |
| Yrs | years |
References
- Bozzola, E.; Spina, G.; Valeriani, M.; Papetti, L.; Ursitti, F.; Agostiniani, R.; Mascolo, C.; Ruggiero, M.; Di Camillo, C.; Quondamcarlo, A.; et al. Management of pediatric post-infectious neurological syndromes. Ital. J. Pediatr. 2021, 47, 17. [Google Scholar] [CrossRef]
- Kundu, S.; Rogal, S.; Alam, A.; Levinthal, D.J. Rapid improvement in post-infectious gastroparesis symptoms with mirtazapine. World J. Gastroenterol. 2014, 20, 6671–6674. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, N.; Kapoor, P.; Dhole, T.N. Antibody and inflammatory response-mediated severity of pandemic 2009 (pH1N1) influenza virus. J. Med. Virol. 2014, 86, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-N.; Liu, L.; Qiao, H.-M.; Cheng, H.; Cheng, H.-J. Post-infectious bronchiolitis obliterans in children: A review of 42 cases. BMC Pediatr. 2014, 14, 238. [Google Scholar] [CrossRef] [PubMed]
- Plesca, D.A.; Luminos, M.; Spatariu, L.; Stefanescu, M.; Cinteza, E.; Balgradean, M. Postinfectious arthritis in pediatric practice. Maedica 2013, 8, 164–169. [Google Scholar]
- Lilleberg, H.S.; Eide, I.A.; Geitung, J.T.; Svensson, M.H.S. Akutt glomerulonefritt utløst av parvovirus B19. Tidsskr. Den Nor. Legeforen. 2018. Available online: https://tidsskriftet.no/2018/10/kort-kasuistikk/akutt-glomerulonefritt-utlost-av-parvovirus-b19 (accessed on 30 October 2018). [CrossRef]
- Mancera-Páez, O.; Román, G.C.; Pardo-Turriago, R.; Rodríguez, Y.; Anaya, J.-M. Concurrent Guillain-Barré syndrome, transverse myelitis and encephalitis post-Zika: A case report and review of the pathogenic role of multiple arboviral immunity. J. Neurol. Sci. 2018, 395, 47–53. [Google Scholar] [CrossRef]
- Blitz, J.; Riddle, M.S.; Porter, C.K. The Risk of Chronic Gastrointestinal Disorders Following Acute Infection with Intestinal Parasites. Front. Microbiol. 2018, 9, 17. [Google Scholar] [CrossRef]
- Jubber, A.; Moorthy, A. Reactive arthritis: A clinical review. J. R. Coll. Physicians Edinb. 2021, 51, 288–297. [Google Scholar] [CrossRef]
- Hermann, E. T cells in reactive arthritis. APMIS 1993, 101, 177–186. [Google Scholar] [CrossRef]
- Rostami, K.; Rostami-Nejad, M.; Al Dulaimi, D. Post gastroenteritis gluten intolerance. Gastroenterol. Hepatol. Bed Bench 2015, 8, 66–70. [Google Scholar]
- Joli, J.; Buck, P.; Zipfel, S.; Stengel, A. Post-COVID-19 fatigue: A systematic review. Front. Psychiatry 2022, 13, 947973. [Google Scholar] [CrossRef] [PubMed]
- Messiah, S.E.; Xie, L.; Mathew, M.S.; Shaikh, S.; Veeraswamy, A.; Rabi, A.; Francis, J.; Lozano, A.; Ronquillo, C.; Sanchez, V.; et al. Comparison of Long-Term Complications of COVID-19 Illness among a Diverse Sample of Children by MIS-C Status. Int. J. Environ. Res. Public Health 2022, 19, 13382. [Google Scholar] [CrossRef] [PubMed]
- Flokas, M.E.; Bustamante, V.H.; Kanakatti Shankar, R. New-Onset Primary Adrenal Insufficiency and Autoimmune Hypothyroidism in a Pediatric Patient Presenting with MIS-C. Horm. Res. Paediatr. 2022, 95, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, J.; Cohen, M.; Zapater, J.L.; Eisenberg, Y. Primary Adrenal Insufficiency After COVID-19 Infection. AACE Clin. Case Rep. 2022, 8, 51–53. [Google Scholar] [CrossRef]
- Christodoulou, M.; Iatridi, F.; Chalkidis, G.; Lioulios, G.; Nikolaidou, C.; Badis, K.; Fylaktou, A.; Papagianni, A.; Stangou, M. ANCA-Associated Vasculitis May Result as a Complication to Both SARS-CoV-2 Infection and Vaccination. Life 2022, 12, 1072. [Google Scholar] [CrossRef]
- Reiff, D.D.; Meyer, C.G.; Marlin, B.; Mannion, M.L. New onset ANCA-associated vasculitis in an adolescent during an acute COVID-19 infection: A case report. BMC Pediatr. 2021, 21, 333. [Google Scholar] [CrossRef]
- Bryant, M.C.; Spencer, L.T.; Yalcindag, A. A case of ANCA-associated vasculitis in a 16-year-old female following SARS-CoV-2 infection and a systematic review of the literature. Pediatr. Rheumatol. 2022, 20, 65. [Google Scholar] [CrossRef]
- Fireizen, Y.; Shahriary, C.; Imperial, M.E.; Randhawa, I.; Nianiaris, N.; Ovunc, B. Pediatric P-ANCA vasculitis following COVID-19. Pediatr. Pulmonol. 2021, 56, 3422–3424. [Google Scholar] [CrossRef]
- Powell, W.T.; Campbell, J.A.; Ross, F.; Peña Jiménez, P.; Rudzinski, E.R.; Dickerson, J.A. Acute ANCA Vasculitis and Asymptomatic COVID-19. Pediatrics 2021, 147, e2020033092. [Google Scholar] [CrossRef]
- MacDougall, M.; El-Hajj Sleiman, J.; Beauchemin, P.; Rangachari, M. SARS-CoV-2 and Multiple Sclerosis: Potential for Disease Exacerbation. Front. Immunol. 2022, 13, 871276. [Google Scholar] [CrossRef] [PubMed]
- Khair, A.M.; Nikam, R.; Husain, S.; Ortiz, M.; Kaur, G. Para and Post-COVID-19 CNS Acute Demyelinating Disorders in Children: A Case Series on Expanding the Spectrum of Clinical and Radiological Characteristics. Cureus 2022, 14, e23405. [Google Scholar] [CrossRef] [PubMed]
- Das, D.; Bhattacharjee, H.; Rehman, O.; Deori, N.; Magdalene, D.; Bharali, G.; Mishra, S.; Godani, K. Neuromyelitis optica spectrum disorder post-COVID-19 infection: A rare case report from Northeast India. Indian J. Ophthalmol. 2022, 70, 1833. [Google Scholar] [CrossRef]
- Sandoval, F.; Julio, K.; Méndez, G.; Valderas, C.; Echeverría, A.C.; Perinetti, M.J.; Suarez, N.M.; Barraza, G.; Piñera, C.; Alarcón, M.; et al. Neurologic Features Associated With SARS-CoV-2 Infection in Children: A Case Series Report. J. Child Neurol. 2021, 36, 853–866. [Google Scholar] [CrossRef]
- Saini, L.; Krishna, D.; Tiwari, S.; Goyal, J.P.; Kumar, P.; Khera, D.; Choudhary, B.; Didel, S.; Gadepalli, R.; Singh, K. Post-COVID-19 Immune-Mediated Neurological Complications in Children: An Ambispective Study. Pediatr. Neurol. 2022, 136, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Carta, A.; Bellucci, C.; Tagliavini, V.; Turco, E.C.; Farci, R.; Cerasti, D.; Bozzetti, F.; Mora, P. Atypical presentation of juvenile multiple sclerosis in a patient with COVID-19. Eur. J. Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Akçay, N.; Bektaş, G.; Menentoğlu, M.E.; Oğur, M.; Sofuoğlu, A.İ.; Palabiyik, F.B.; Şevketoğlu, E. COVID-19–associated Acute Disseminated Encephalomyelitis–like Disease in 2 Children. Pediatr. Infect. Dis. J. 2021, 40, e445–e450. [Google Scholar] [CrossRef]
- Poyrazoğlu, H.G.; Kırık, S.; Sarı, M.Y.; Esen, İ.; Toraman, Z.A.; Eroğlu, Y. Acute demyelinating encephalomyelitis and transverse myelitis in a child with COVID-19. Turk. J. Pediatr. 2022, 64, 133. [Google Scholar] [CrossRef]
- Cay-Martínez, K.C.; Shen, M.Y.; Silver, W.G.; Vargas, W.S. Postinfectious Encephalomyelitis Associated With Myelin Oligodendrocyte Glycoprotein Antibody in a Pediatric Patient with COVID-19. Pediatr. Neurol. 2021, 124, 40–41. [Google Scholar] [CrossRef]
- de Miranda Henriques-Souza, A.M.; de Melo, A.C.M.G.; de Aguiar Coelho Silva Madeiro, B.; Freitas, L.F.; Sampaio Rocha-Filho, P.A.; Gonçalves, F.G. Acute disseminated encephalomyelitis in a COVID-19 pediatric patient. Neuroradiology 2021, 63, 141–145. [Google Scholar] [CrossRef]
- Manzo, M.L.; Galati, C.; Gallo, C.; Santangelo, G.; Marino, A.; Guccione, F.; Pitino, R.; Raieli, V. ADEM post-SARS-CoV-2 infection in a pediatric patient with Fisher-Evans syndrome. Neurol. Sci. 2021, 42, 4293–4296. [Google Scholar] [CrossRef] [PubMed]
- Urso, L.; Distefano, M.G.; Cambula, G.; Colomba, A.I.; Nuzzo, D.; Picone, P.; Giacomazza, D.; Sicurella, L. The case of encephalitis in a COVID-19 pediatric patient. Neurol. Sci. 2022, 43, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Morales, A.E.; Urrutia-Osorio, M.; Camacho-Mendoza, E.; Rosales-Pedraza, G.; Dávila-Maldonado, L.; González-Duarte, A.; Herrera-Mora, P.; Ruiz-García, M. Neurological manifestations temporally associated with SARS-CoV-2 infection in pediatric patients in Mexico. Child’s Nerv. Syst. 2021, 37, 2305–2312. [Google Scholar] [CrossRef] [PubMed]
- Ivan, A.P.; Odajiu, I.; Popescu, B.O.; Davidescu, E.I. COVID-19 Associated Guillain–Barré Syndrome: A Report of Nine New Cases and a Review of the Literature. Medicina 2022, 58, 977. [Google Scholar] [CrossRef]
- El Mezzeoui, S.; Aftiss, F.z.; Aabdi, M.; Bkiyar, H.; Housni, B. Guillan barre syndrome in post COVID-19 infection in children. Ann. Med. Surg. 2021, 67, 102524. [Google Scholar] [CrossRef]
- Costa, H.S.C.; de Castro, P.N.P.; Ventura, N.; Leite, L.C.; Rego, C.T.O.; Santos, R.Q.D.; Machado, D.C.; Zaeyen, E.J.B. COVID-19-related Guillain-Barré Syndrome variant with multiple cranial neuropathies in a child. EuroRad 2022. [Google Scholar] [CrossRef]
- Curtis, M.; Bhumbra, S.; Felker, M.V.; Jordan, B.L.; Kim, J.; Weber, M.; Friedman, M.L. Guillain-Barré syndrome in a child with COVID-19 infection. Pediatrics 2021, 147, e2020015115. [Google Scholar] [CrossRef]
- Mehra, B.; Aggarwal, V.; Kumar, P.; Kundal, M.; Gupta, D.; Kumar, A.; Dugaya, S.K. COVID-19 associated severe multisystem inflammatory syndrome in children with encephalopathy and neuropathy in an adolescent girl with the successful outcome: An unusual presentation. Indian J. Crit. Care Med. 2020, 24, 1276–1278. [Google Scholar] [CrossRef] [PubMed]
- Khera, D.; Didel, S.; Panda, S.; Tiwari, S.; Singh, K. Concurrent Longitudinally Extensive Transverse Myelitis and Guillain-Barré Syndrome in a Child Secondary to COVID-19 Infection. Pediatr. Infect. Dis. J. 2021, 40, e236–e239. [Google Scholar] [CrossRef]
- Das, K.Y.; Midhun Raj, K.T.; Samprathi, M.; Sridhar, M.; Adiga, R.; Vemgal, P. Guillain–Barré Syndrome Associated with SARS-CoV-2 Infection. Indian J. Pediatr. 2021, 88, 479. [Google Scholar] [CrossRef]
- Frank, C.H.M.; Almeida, T.V.R.; Marques, E.A.; de Sousa Monteiro, Q.; Feitoza, P.V.S.; Borba, M.G.S.; Vasconcelos, H.L.; de Souza Bastos, M.; Lacerda, M.V.G. Guillain–Barré Syndrome Associated with SARS-CoV-2 Infection in a Pediatric Patient. J. Trop. Pediatr. 2021, 67, fmaa044. [Google Scholar] [CrossRef] [PubMed]
- Paybast, S.; Gorji, R.; Mavandadi, S. Guillain-Barré Syndrome as a Neurological Complication of Novel COVID-19 Infection. Neurologist 2020, 25, 101–103. [Google Scholar] [CrossRef] [PubMed]
- Al Haboob, A.A. Miller Fischer and posterior reversible encephalopathy syndromes post COVID-19 infection. Neurosciences 2021, 26, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Krueger, M.B.; Montenegro, R.C.; de Araújo Coimbra, P.P.; de Queiroz Lemos, L.; Fiorenza, R.M.; da Silva Fernandes, C.J.; Pessoa, M.S.L.; Rodrigues, C.L.; da Cruz, C.G.; de Araújo Verdiano, V.; et al. A wide spectrum of neurological manifestations in pediatrics patients with the COVID-19 infection: A case series. J. Neurovirol. 2021, 27, 782–786. [Google Scholar] [CrossRef]
- Krishnakumar, A.; Kewalramani, D.; Mahalingam, H.; Manokaran, R.K. Guillain–Barré Syndrome with Preserved Reflexes in a Child after COVID-19 Infection. Indian J. Pediatr. 2021, 88, 831–832. [Google Scholar] [CrossRef]
- Michael, S.N.; Madaan, P.; Shekhar, M. An Unusual Descending Presentation of Pediatric Guillain-Barre Syndrome Following COVID-19: Expanding the Spectrum. Pediatr. Neurol. 2021, 124, 13–14. [Google Scholar] [CrossRef]
- Mussinatto, I.; Benevenuta, C.; Caci, A.; Calvo, M.; Impastato, M.; Barra, M.; Genovese, E.; Timeus, F. Possible association between Guillain-Barré syndrome and SARS-CoV-2 infection in children: A case report and literature review. Exp. Ther. Med. 2022, 24, 462. [Google Scholar] [CrossRef]
- Terencio, B.B.; Patiño, R.F.; Jamora, R.D.G. Guillain-Barré Syndrome in a Pediatric Patient with COVID-19: A Case Report and Review of Literature. Acta Med. Philipp. 2021, 56, 53–60. [Google Scholar] [CrossRef]
- Kanou, S.; Wardeh, L.; Govindarajan, S.; Macnay, K. Guillain-Barre syndrome (GBS) associated with COVID-19 infection that resolved without treatment in a child. BMJ Case Rep. 2022, 15, e245455. [Google Scholar] [CrossRef]
- Akçay, N.; Menentoğlu, M.E.; Bektaş, G.; Şevketoğlu, E. Axonal Guillain-Barre syndrome associated with SARS-CoV-2 infection in a child. J. Med. Virol. 2021, 93, 5599–5602. [Google Scholar] [CrossRef]
- Manji, H.K.; George, U.; Mkopi, N.P.; Manji, K.P. Guillain-Barré syndrome associated with COVID-19 infection. Pan Afr. Med. J. 2020, 35, 118. [Google Scholar] [PubMed]
- Khalifa, M.; Zakaria, F.; Ragab, Y.; Saad, A.; Bamaga, A.; Emad, Y.; Rasker, J.J. Guillain-Barré syndrome associated with severe acute respiratory syndrome coronavirus 2 detection and coronavirus disease 2019 in a child. J. Pediatr. Infect. Dis. Soc. 2020, 9, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Qamar, T.; Kumar, S.; Gupta, S.; Awasthi, S. Guillain–Barré Syndrome with Normal Nerve Conduction Study Associated with COVID-19 Infection in a Child. Indian J. Pediatr. 2022, 89, 631. [Google Scholar] [CrossRef] [PubMed]
- Araújo, N.M.; Ferreira, L.C.; Dantas, D.P.; Silva, D.S.; dos Santos, C.A.; Cipolotti, R.; Martins-Filho, P.R. First Report of SARS-CoV-2 Detection in Cerebrospinal Fluid in a Child with Guillain-Barré Syndrome. Pediatr. Infect. Dis. J. 2021, 40, e274–e276. [Google Scholar] [CrossRef] [PubMed]
- Pinazo-Bandera, J.M.; Hernández-Albújar, A.; García-Salguero, A.I.; Arranz-Salas, I.; Andrade, R.J.; Robles-Díaz, M. Acute hepatitis with autoimmune features after COVID-19 vaccine: Coincidence or vaccine-induced phenomenon? Gastroenterol. Rep. 2022, 10, goac014. [Google Scholar] [CrossRef] [PubMed]
- Osborn, J.; Szabo, S.; Peters, A.L. Pediatric Acute Liver Failure Due to Type 2 Autoimmune Hepatitis Associated with SARS-CoV-2 Infection: A Case Report. JPGN Rep. 2022, 3, e204. [Google Scholar] [CrossRef]
- Antala, S.; Diamond, T.; Kociolek, L.K.; Shah, A.A.; Chapin, C.A. Severe Hepatitis in Pediatric Coronavirus Disease 2019. J. Pediatr. Gastroenterol. Nutr. 2022, 74, 631–635. [Google Scholar] [CrossRef]
- Retamozo, S.; Brito-Zerón, P.; Sisó-Almirall, A.; Flores-Chávez, A.; Soto-Cárdenas, M.-J.; Ramos-Casals, M. Haemophagocytic syndrome and COVID-19. Clin. Rheumatol. 2021, 40, 1233–1244. [Google Scholar] [CrossRef]
- Greenmyer, J.R.; Wyatt, K.D.; Milanovich, S.; Kohorst, M.A.; Ferdjallah, A. COVID-19-associated secondary hemophagocytic lymphohistiocytosis requiring hematopoietic cell transplant. eJHaem 2022, 3, 1025–1028. [Google Scholar] [CrossRef]
- Rjoop, A.; Barukba, M.; Rusan, O.A. A rare case of post COVID-19 hemophagocytic lymphohistiocytosis in a pediatric patient. Am. J. Clin. Pathol. 2021, 156, S93. [Google Scholar] [CrossRef]
- Kalita, P.; Laishram, D.; Dey, B.; Mishra, J.; Barman, B.; Barman, H. Secondary Hemophagocytic Lymphohistiocytosis in Post-COVID-19 Patients: A Report of Two Cases. Cureus 2021, 13, e17328. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Linden, T.; Müller, H.L.; Flasskuehler, M.A.; Koester, H.; Lehmberg, K.; Ledig, S.; Ehl, S.; Heep, A.; Beske, F. Primary haemophagocytic lymphohistiocytosis (Chédiak-Higashi Syndrome) triggered by acute SARS-CoV-2 infection in a six-week-old infant. Br. J. Haematol. 2021, 195, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Kurian, C.J.; French, Z.; Kukulich, P.; Lankiewicz, M.; Ghimire, S.; Maarouf, O.H.; Rizk, S.; Rhoades, R. Case series: Coronavirus disease 2019 infection as a precipitant of atypical hemolytic uremic syndrome: Two case reports. J. Med. Case Rep. 2021, 15, 587. [Google Scholar] [CrossRef] [PubMed]
- Van Quekelberghe, C.; Latta, K.; Kunzmann, S.; Grohmann, M.; Hansen, M. Atypical hemolytic uremic syndrome induced by SARS-CoV2 infection in infants with EXOSC3 mutation. Pediatr. Nephrol. 2022, 37, 2781–2784. [Google Scholar] [CrossRef]
- Alizadeh, F.; O’Halloran, A.; Alghamdi, A.; Chen, C.; Trissal, M.; Traum, A.; DeCourcey, D. Toddler With New Onset Diabetes and Atypical Hemolytic-Uremic Syndrome in the Setting of COVID-19. Pediatrics 2021, 147, e2020016774. [Google Scholar] [CrossRef] [PubMed]
- Azukaitis, K.; Stankute-Kolosova, A.; Burokiene, V.; Saulyte Trakymiene, S.; Jankauskiene, A. Possible microangiopathic overlap between COVID-19 and Shiga toxin-associated hemolytic uremic syndrome. Pediatr. Blood Cancer 2022, 69, e29798. [Google Scholar] [CrossRef]
- Khandelwal, P.; Krishnasamy, S.; Govindarajan, S.; Kumar, M.; Marik, B.; Sinha, A.; Hari, P.; Bagga, A. Anti-factor H antibody associated hemolytic uremic syndrome following SARS-CoV-2 infection. Pediatr. Nephrol. 2022, 37, 2151–2156. [Google Scholar] [CrossRef]
- Richardson, G.M.; Su, S.W.; Iragorri, S. Case report: Diarrhea-associated hemolytic uremic syndrome in the Era of COVID-19. Front. Pediatr. 2022, 10, 979850. [Google Scholar] [CrossRef]
- Xu, P.; Zhou, Q.; Xu, J. Mechanism of thrombocytopenia in COVID-19 patients. Ann. Hematol. 2020, 99, 1205–1208. [Google Scholar] [CrossRef]
- Ringoringo, H.P.; Hartoyo, E. Megadose Methylprednisolone for Immune Thrombocytopenia in an Infant Positive for SARS-CoV-2: A Case Report. Am. J. Case Rep. 2021, 22, e931517. [Google Scholar] [CrossRef]
- Marinescu, A.R.; Lazureanu, V.E.; Musta, V.F.; Nicolescu, N.D.; Mocanu, A.; Cut, T.G.; Muresan, C.O.; Tudoran, C.; Licker, M.; Laza, R. Severe Thrombocytopenic Purpura Associated with COVID-19 in a Pediatric Patient. Infect. Drug Resist. 2022, 15, 3405–3415. [Google Scholar] [CrossRef] [PubMed]
- Dongre, A.; Jameel, P.Z.; Deshmukh, M.; Bhandarkar, S. Immune thrombocytopenic purpura secondary to SARS-CoV-2 infection in a child with acute lymphoblastic leukaemia: A case report and review of literature. BMJ Case Rep. 2021, 14, e245869. [Google Scholar] [CrossRef] [PubMed]
- Ceglie, G.; De Ioris, M.A.; Mercadante, S.; Olivini, N.; Del Bufalo, F.; Marchesani, S.; Cocca, F.; Monteferrario, E.; Boccieri, E.; Pianese, J.; et al. Immune thrombocytopenia in a child with COVID-19: Is it the calm after the (cytokine) storm? Pediatr. Blood Cancer 2022, 69, e29326. [Google Scholar] [CrossRef] [PubMed]
- Behlivani, E.; Tragiannidis, A.; Hatzipantelis, E.; Panagopoulou, P. Immune thrombocytopenia secondary to COVID-19 infection: Report of two cases. Pediatr. Blood Cancer 2021, 68, e29175. [Google Scholar] [CrossRef]
- Rosenzweig, J.D.; McThenia, S.S.; Kaicker, S. SARS-CoV-2 infection in two pediatric patients with immune cytopenias: A single institution experience during the pandemic. Pediatr. Blood Cancer 2020, 67, e28503. [Google Scholar] [CrossRef]
- Vadakkekara, J.; Mathew, R.; Khera, S. COVID-19–Associated Immune Thrombocytopenia in a Toddler. Indian J. Pediatr. 2022, 89, 623. [Google Scholar] [CrossRef]
- Tsao, H.S.; Chason, H.M.; Fearon, D.M. Immune Thrombocytopenia (ITP) in a Pediatric Patient Positive for SARS-CoV-2. Pediatrics 2020, 146, e20201419. [Google Scholar] [CrossRef]
- Patel, P.A.; Chandrakasan, S.; Mickells, G.E.; Yildirim, I.; Kao, C.M.; Bennett, C.M. Severe Pediatric COVID-19 Presenting with Respiratory Failure and Severe Thrombocytopenia. Pediatrics 2020, 146, e20201437. [Google Scholar] [CrossRef]
- Shah, H.; Busquets, A.C. Psoriasis Flares in Patients With COVID-19 Infection or Vaccination: A Case Series. Cureus 2022, 14, e25987. [Google Scholar] [CrossRef]
- Zitouni, J.; Bursztejn, A.-C.; Fortina, A.B.; Beauchet, A.; Di Lernia, V.; Lesiak, A.; Thomas, J.; Topkarci, Z.; Murashkin, N.; Brzezinski, P.; et al. Children with psoriasis and COVID-19: Factors associated with an unfavourable COVID-19 course, and the impact of infection on disease progression (Chi-PsoCov registry). J. Eur. Acad. Dermatol. Venereol. 2022, 36, 2076–2086. [Google Scholar] [CrossRef]
- Qureshi, N.K.; Bansal, S.K. Autoimmune Thyroid Disease and Psoriasis Vulgaris after COVID-19 in a Male Teenager. Case Rep. Pediatr. 2021, 2021, 7584729. [Google Scholar] [CrossRef] [PubMed]
- Klindt, C.; Jensen, B.; Brandenburger, T.; Feldt, T.; Killer, A.; Schimmöller, L.; Antoch, G.; Senff, T.; Hauka, S.; Timm, J.; et al. Secondary sclerosing cholangitis as a complication of severe COVID-19: A case report and review of the literature. Clin. Case Rep. 2021, 9, e04068. [Google Scholar] [CrossRef] [PubMed]
- Zdanowicz, K.; Bobrus-Chociej, A.; Kopiczko, A.; Uścinowicz, M.; Tomczuk-Ostapczuk, M.; Janica, J.; Łotowska, J.M.; Białokoz-Kalinowska, I.; Lebensztejn, D.M. Autoimmune sclerosing cholangitis might be triggered by SARS-CoV-2 infection in a child—A case report. Cent. Eur. J. Immunol. 2022, 47, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Guga, S.; Wu, K.; Khaw, Z.; Tzoumkas, K.; Tombleson, P.; Comeau, M.E.; Langefeld, C.D.; Cunninghame Graham, D.S.; Morris, D.L.; et al. COVID-19 and systemic lupus erythematosus genetics: A balance between autoimmune disease risk and protection against infection. PLoS Genet. 2022, 18, e1010253. [Google Scholar] [CrossRef]
- Asseri, A.A.; Al-Murayeh, R.; Abudiah, A.M.; Elgebally, E.I.; Aljaser, A.M. A case report of pediatric systemic lupus erythematosus with diffuse alveolar hemorrhage following COVID-19 infection: Causation, association, or chance? Medicine 2022, 101, e30071. [Google Scholar] [CrossRef]
- Cardoso, E.M.; Hundal, J.; Feterman, D.; Magaldi, J. Concomitant new diagnosis of systemic lupus erythematosus and COVID-19 with possible antiphospholipid syndrome. Just a coincidence? A case report and review of intertwining pathophysiology. Clin. Rheumatol. 2020, 39, 2811–2815. [Google Scholar] [CrossRef]
- Rockett, J.; Nelson, C.; Pierce, R.; Morlan, A. Van A case report of Graves’ disease following SARS-CoV-2 infection. Int. J. Contemp. Pediatr. 2021, 8, 1260. [Google Scholar] [CrossRef]
- Das, B.B.; Shakti, D.; Akam-Venkata, J.; Obi, O.; Weiland, M.D.; Moskowitz, W. SARS-CoV-2 infection induced thyroid storm and heart failure in an adolescent girl. Cardiol. Young 2022, 32, 988–992. [Google Scholar] [CrossRef]
- Nicksic, V.B.; Logel, S.; Srinivasan, S.; Mann, E.; Rehm, J.L. Thyroid Storm with Concurrent COVID-19 Infection in a Pediatric Patient. J. Endocr. Soc. 2021, 5, A962–A963. [Google Scholar] [CrossRef]
- Kumar, V.S.; Dhananjaya, S.R.; Sathish, H.S.; Gowda, S. Auto-immune thyroiditis in SARS-CoV-2 exposed twins. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 4881–4883. [Google Scholar] [CrossRef]
- Brancatella, A.; Ricci, D.; Viola, N.; Sgrò, D.; Santini, F.; Latrofa, F. Subacute Thyroiditis After SARS-CoV-2 Infection. J. Clin. Endocrinol. Metab. 2020, 105, 2367–2370. [Google Scholar] [CrossRef] [PubMed]
- Maithani, T.; Gupta, M.; Dogra, R.; Hernot, S. Pediatric thyroid abscess: An unusual late complication of COVID-19 infection. Int. J. Otorhinolaryngol. Head Neck Surg. 2022, 8, 406. [Google Scholar] [CrossRef]
- Çağlayan, Ş.; Ulu, K.; Çakan, M.; Sözeri, B. A rare onset in tumour necrosis factor receptor–associated periodic syndrome: Recurrent macrophage activation syndrome triggered by COVID-19 infection. Rheumatology 2022, 61, e366–e367. [Google Scholar] [CrossRef] [PubMed]
- Ordooei, M.; Behniafard, N.; Soheilipour, F.; Akbarian, E. New onset of diabetes in a child infected with COVID-19: A case report. J. Diabetes Metab. Disord. 2021, 20, 2129–2132. [Google Scholar] [CrossRef] [PubMed]
- Lança, A.; Rodrigues, C.; Diamantino, C.; Fitas, A.L. COVID-19 in two children with new-onset diabetes: Case reports. BMJ Case Rep. 2022, 15, e247309. [Google Scholar] [CrossRef] [PubMed]
- Brothers, E.M.; Lidsky, K.; Simmons, J.; Nakagawa, T. A Child With COVID-19, Type 1 Diabetes, and Candida glabrata : A Case Report and Literature Review. Clin. Pediatr. 2021, 60, 554–558. [Google Scholar] [CrossRef]
- Nielsen-Saines, K.; Li, E.; Olivera, A.M.; Martin-Blais, R.; Bulut, Y. Case Report: Insulin-Dependent Diabetes Mellitus and Diabetic Keto-Acidosis in a Child with COVID-19. Front. Pediatr. 2021, 9, 628810. [Google Scholar] [CrossRef]
- Benyakhlef, S.; Abdellaoui, W.; Tahri, A.; Rouf, S.; Latrech, H. Diabetic Ketoacidosis at Onset of Pediatric Type-1 Diabetes Triggered by COVID-19: An Original Case Report. Cureus 2021, 13, e13958. [Google Scholar] [CrossRef]
- Rabizadeh, S.; Hajmiri, M.; Rajab, A.; Emadi Kouchak, H.; Nakhjavani, M. Severe diabetic ketoacidosis and coronavirus disease 2019 (COVID-19) infection in a teenage patient with newly diagnosed diabetes. J. Pediatr. Endocrinol. Metab. 2020, 33, 1241–1243. [Google Scholar] [CrossRef]
- Soliman, A.; Al-Amri, M.; Ellithy, K.; Alaaraj, N.; Hamed, N.; De Sanctis, V. Newly-onset type 1 diabetes mellitus precipitated by COVID-19 in an 8-month-old infant. Acta Biomed. 2020, 91, e2020046. [Google Scholar] [CrossRef]
- Naguib, M.N.; Raymond, J.K.; Vidmar, A.P. New onset diabetes with diabetic ketoacidosis in a child with multisystem inflammatory syndrome due to COVID-19. J. Pediatr. Endocrinol. Metab. 2021, 34, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Daniel, S.; Gadhiya, B.; Parikh, A.; Joshi, P. COVID-19 in a Child With Diabetic Ketoacidosis: An Instigator, a Deviator or a Spectator. Indian Pediatr. 2020, 57, 969–970. [Google Scholar] [CrossRef] [PubMed]
- Márquez-Hernández, J.D. Parasitic arthritis. In Infections and the Rheumatic Diseases; Springer: Berlin, Germany, 2019; pp. 301–314. [Google Scholar]
- El-Shebiny, E.M.; Zahran, E.S.; Shoeib, S.A.; Habib, E.S. Bridging autoinflammatory and autoimmune diseases. Egypt. J. Intern. Med. 2021, 33, 11. [Google Scholar] [CrossRef]
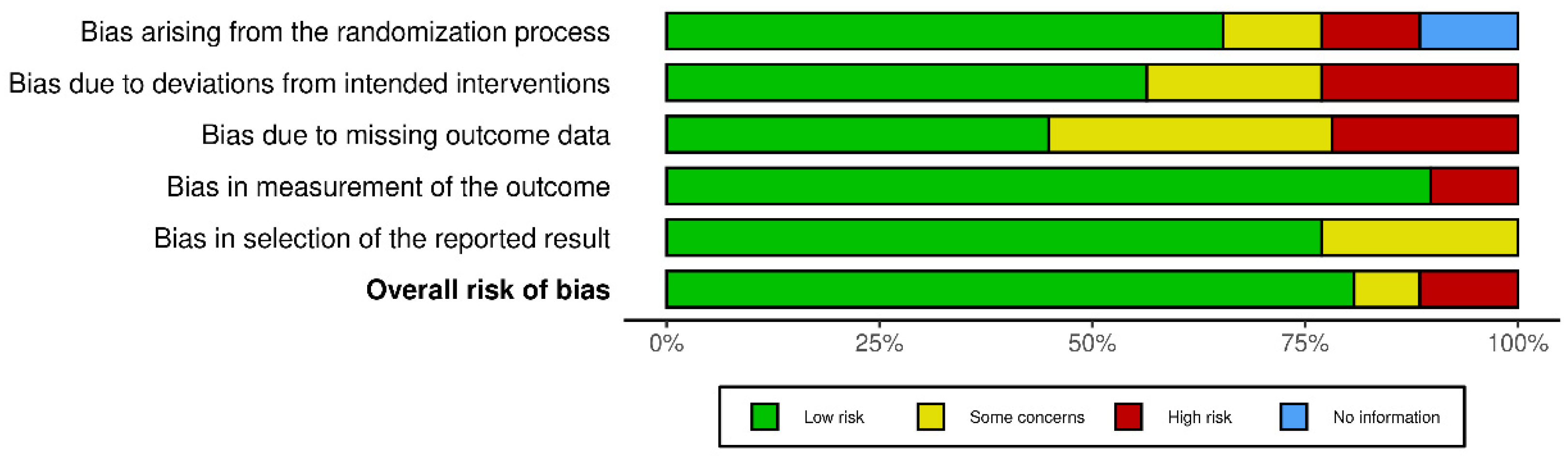
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- AbdelMassih, A.F.; Fouda, R.; Kamel, A.; Mishriky, F.; Ismail, H.-A.; El Qadi, L.; Malak, L.; Mohamed, M.; Arsanyous, M.; Hazem, M.; et al. Single cell sequencing unraveling genetic basis of severe COVID19 in obesity. Obes. Med. 2020, 20, 100303. [Google Scholar] [CrossRef] [PubMed]
- Eggenhuizen, P.J.; Ng, B.H.; Ooi, J.D. Treg Enhancing Therapies to Treat Autoimmune Diseases. Int. J. Mol. Sci. 2020, 21, 7015. [Google Scholar] [CrossRef]
- Knolle, J.; Pierau, M.; Hebel, K.; Lampe, K.; Jorch, G.; Kropf, S.; Arens, C.; Brunner-Weinzierl, M.C. Children From the Age of Three Show a Developmental Switch in T-Cell Differentiation. Front. Immunol. 2020, 11, 1640. [Google Scholar] [CrossRef]
- Batiha, G.E.S.; Al-kuraishy, H.M.; Al-Gareeb, A.I.; Welson, N.N. Pathophysiology of Post-COVID syndromes: A new perspective. Virol. J. 2022, 19, 158. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]




| p-Value | ||
|---|---|---|
| Age distribution, N (%) | Infants (0–2 y) 11 (10) | <0.001 |
| Preschool children (3–5 y) 15 (14) | ||
| School children (6–12 y) 42 (38) | ||
| Adolescents (13–18 y) 41 (38) | ||
| Sex distribution, N (%) | Female 54 (50) | 0.92 |
| Male 55 (50) | ||
| Hospital admission, N (%) | Yes 49 (45) | 0.29 |
| No 60 (55) | ||
| Interval between COVID-19 and autoimmune sequelae, N (%) | Immediate (0–14 days) 67 (61) | <0.001 |
| Classic (15–28 days) 15 (14) | ||
| Delayed (>28 days) 27 (25) |
| Reference | Age | Sex | Interval between COVID-19 Infection and Disorder | Course of COVID-19 Infection and Hospitalization Data | Outcome | Notes |
|---|---|---|---|---|---|---|
| [14] | 14 | Female | 21 days | Congestion and fatigue for three weeks. |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AbdelMassih, A.F.; Hanafy, M.H.; ElAhmady, M.; Kozman, S.; Diab, N.; Husseiny, R.; Deyab, A.; Mady, A.; Yasser, A.; AbdelHalim, A.R.; et al. Non-Multisystem Inflammatory Syndrome in Children—Postacute Sequelae of Paediatric COVID-19: Autoimmune or Autoinflammatory? A Systematic Review of the Reported Cases. Rheumato 2023, 3, 132-168. https://doi.org/10.3390/rheumato3020011
AbdelMassih AF, Hanafy MH, ElAhmady M, Kozman S, Diab N, Husseiny R, Deyab A, Mady A, Yasser A, AbdelHalim AR, et al. Non-Multisystem Inflammatory Syndrome in Children—Postacute Sequelae of Paediatric COVID-19: Autoimmune or Autoinflammatory? A Systematic Review of the Reported Cases. Rheumato. 2023; 3(2):132-168. https://doi.org/10.3390/rheumato3020011
Chicago/Turabian StyleAbdelMassih, Antoine Fakhry, Maram Hamed Hanafy, Maryam ElAhmady, Sylvia Kozman, Nourine Diab, Reem Husseiny, Ashrakat Deyab, Aalaa Mady, Alia Yasser, Amira R. AbdelHalim, and et al. 2023. "Non-Multisystem Inflammatory Syndrome in Children—Postacute Sequelae of Paediatric COVID-19: Autoimmune or Autoinflammatory? A Systematic Review of the Reported Cases" Rheumato 3, no. 2: 132-168. https://doi.org/10.3390/rheumato3020011