
Systemic Inflammasome Biomarkers as Predictors of Diabetic Retinopathy Progression: Evidence from a Pilot Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Bariatric Surgery Cohort
2.2. Ethics
2.3. Participants
2.4. DR Screening in New Zealand
2.5. Blood Collection
2.6. Luminex Multiplex Assay
2.7. Data Analysis
3. Results
3.1. Overall Patient Profile Pre-Surgery and 12 Months Post-Surgery
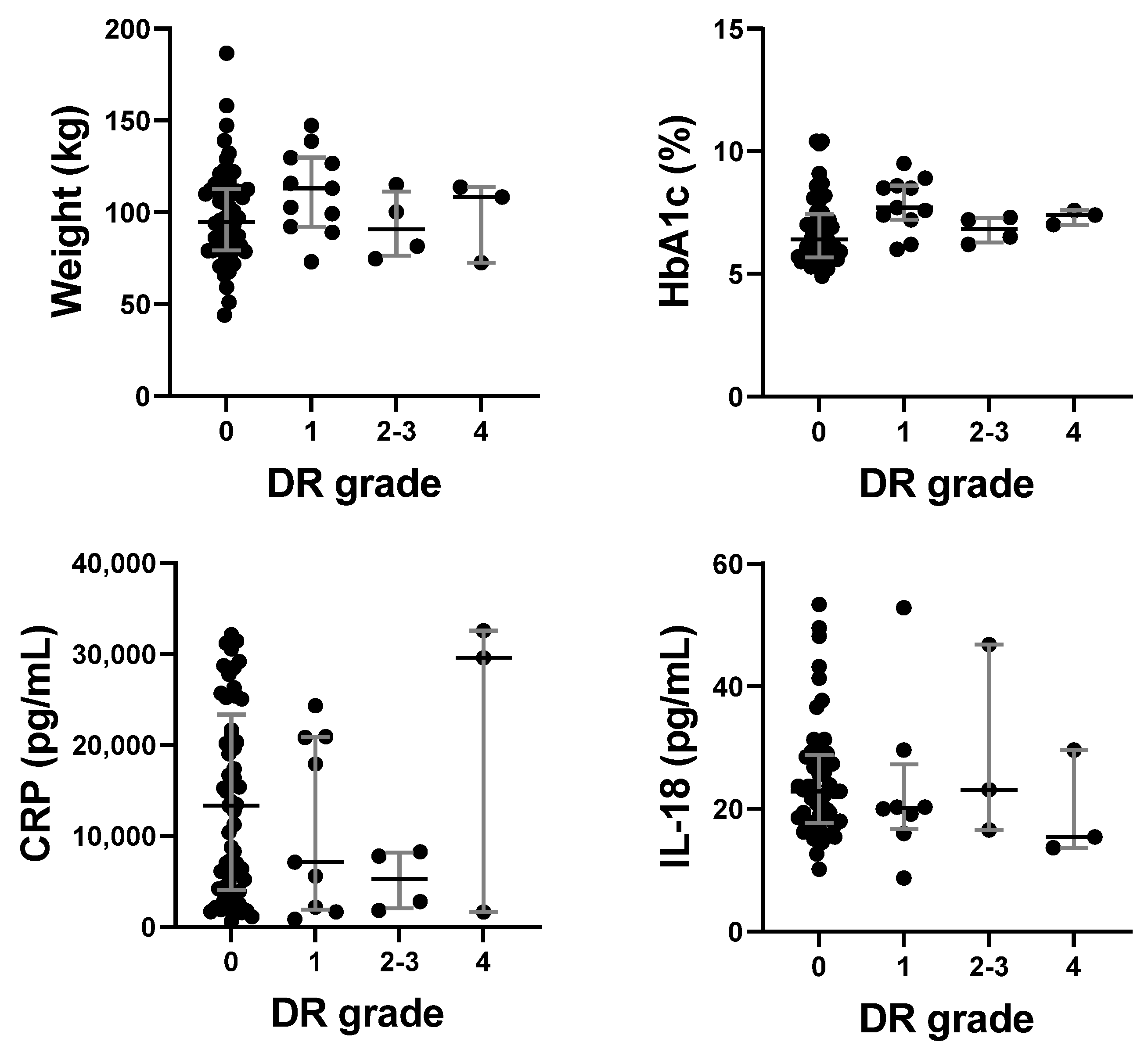
3.2. Inflammasome, Inflammation, and Clinical Biomarker Levels Did Not Correlate with DR Severity Cross-Sectionally
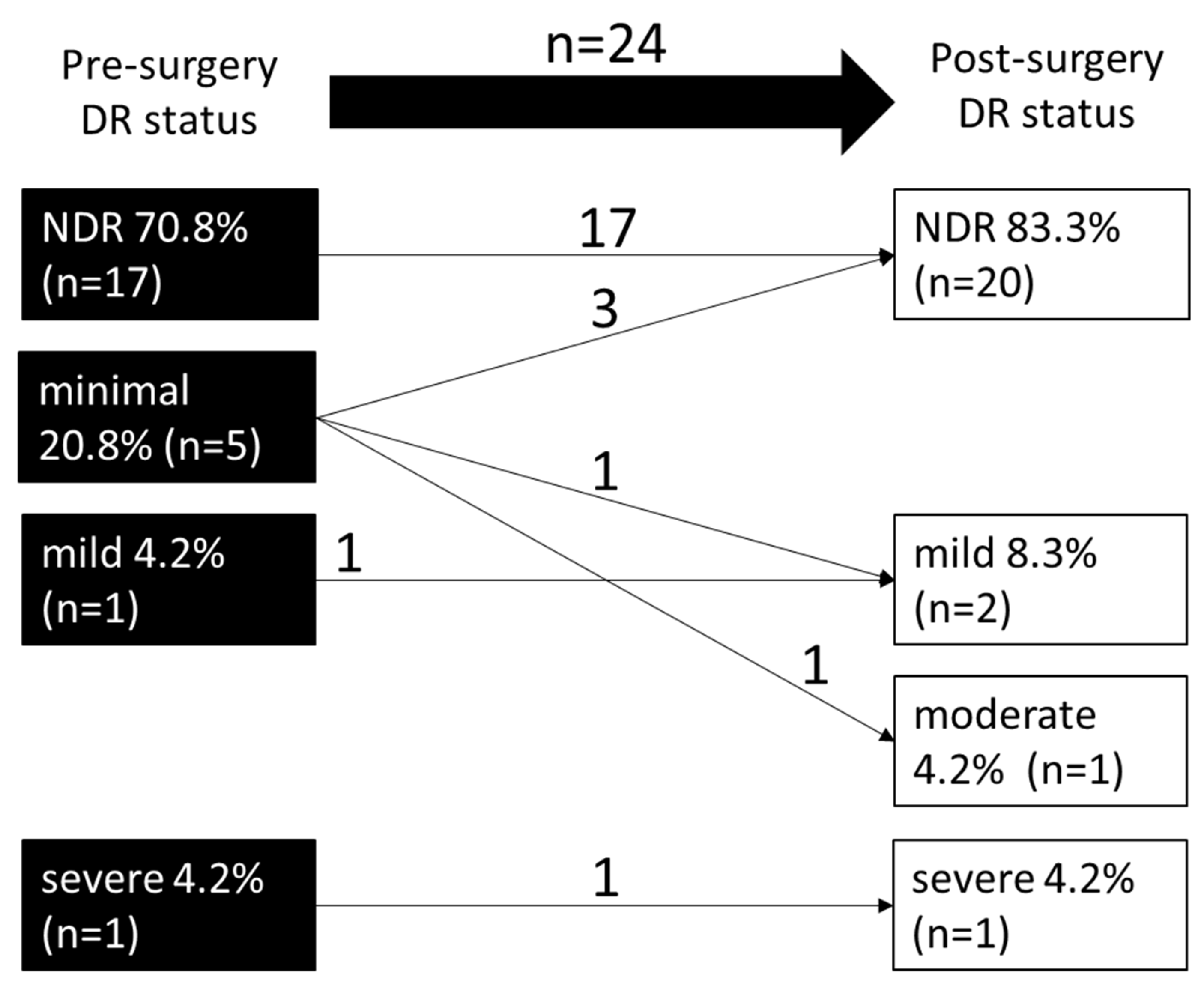
3.3. Change in DR Severity from Baseline to 1 Year Post-Surgery
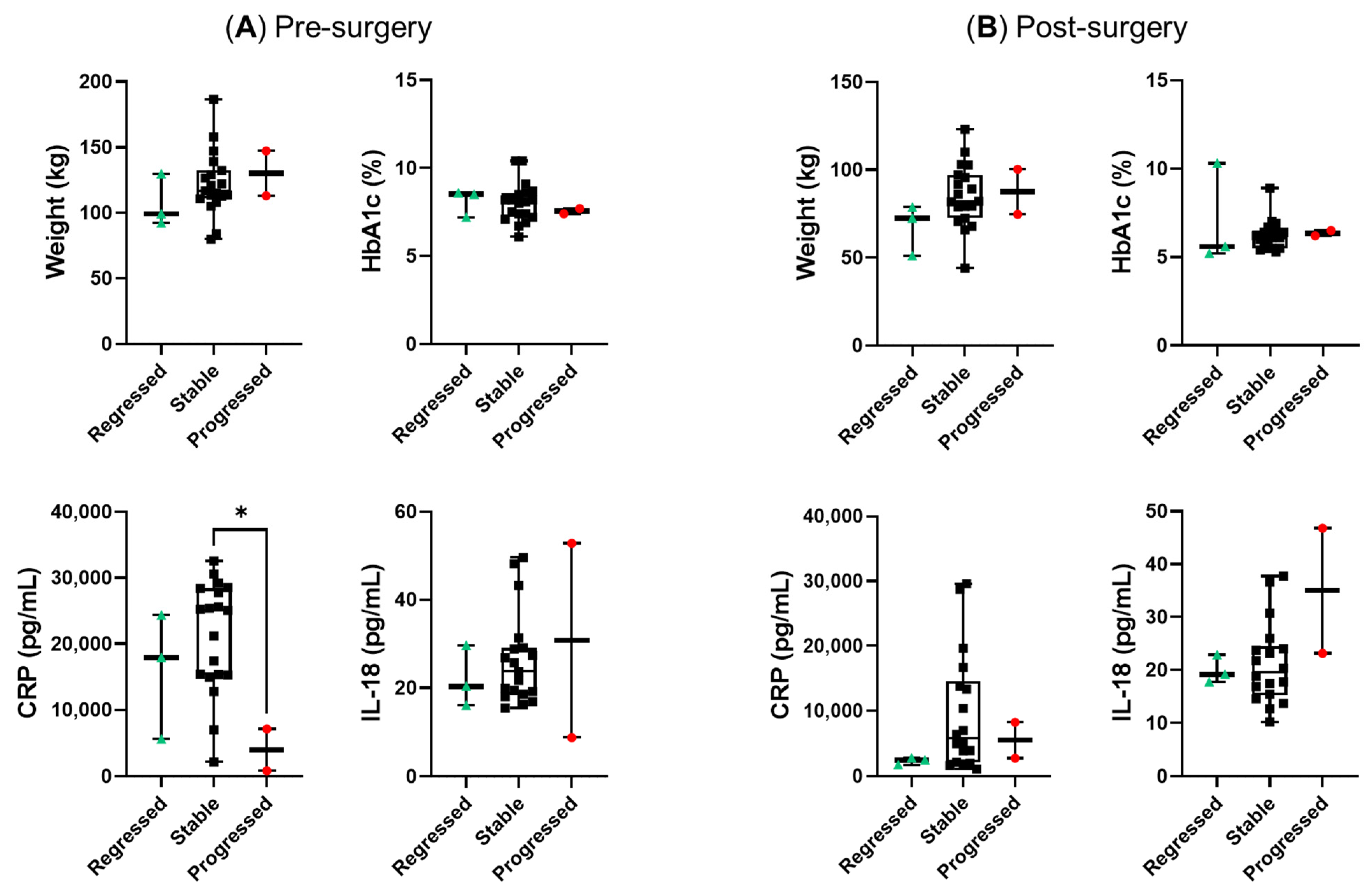
3.4. Comparison of Plasma Biomarkers between Regressed, Stable and Progressed Groups at Pre-Surgery and 1 Year Post-Surgery
3.5. The Progressed Group Showed a Substantial Increase in CRP Compared to the Regressed Group
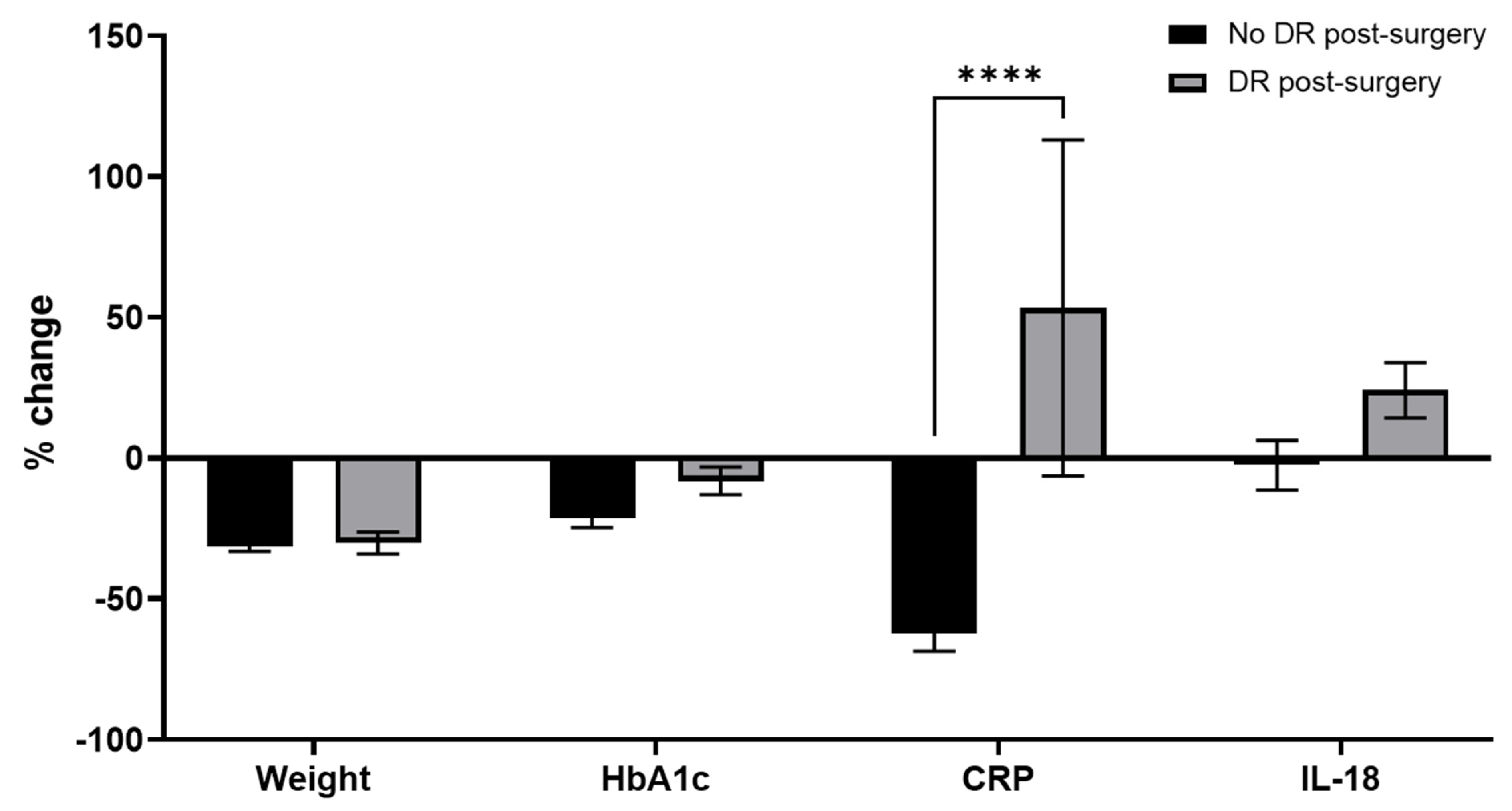
3.6. Relative Change in CRP Was Significantly Higher in the Group with No DR Compared to the Group with DR Post-Surgery
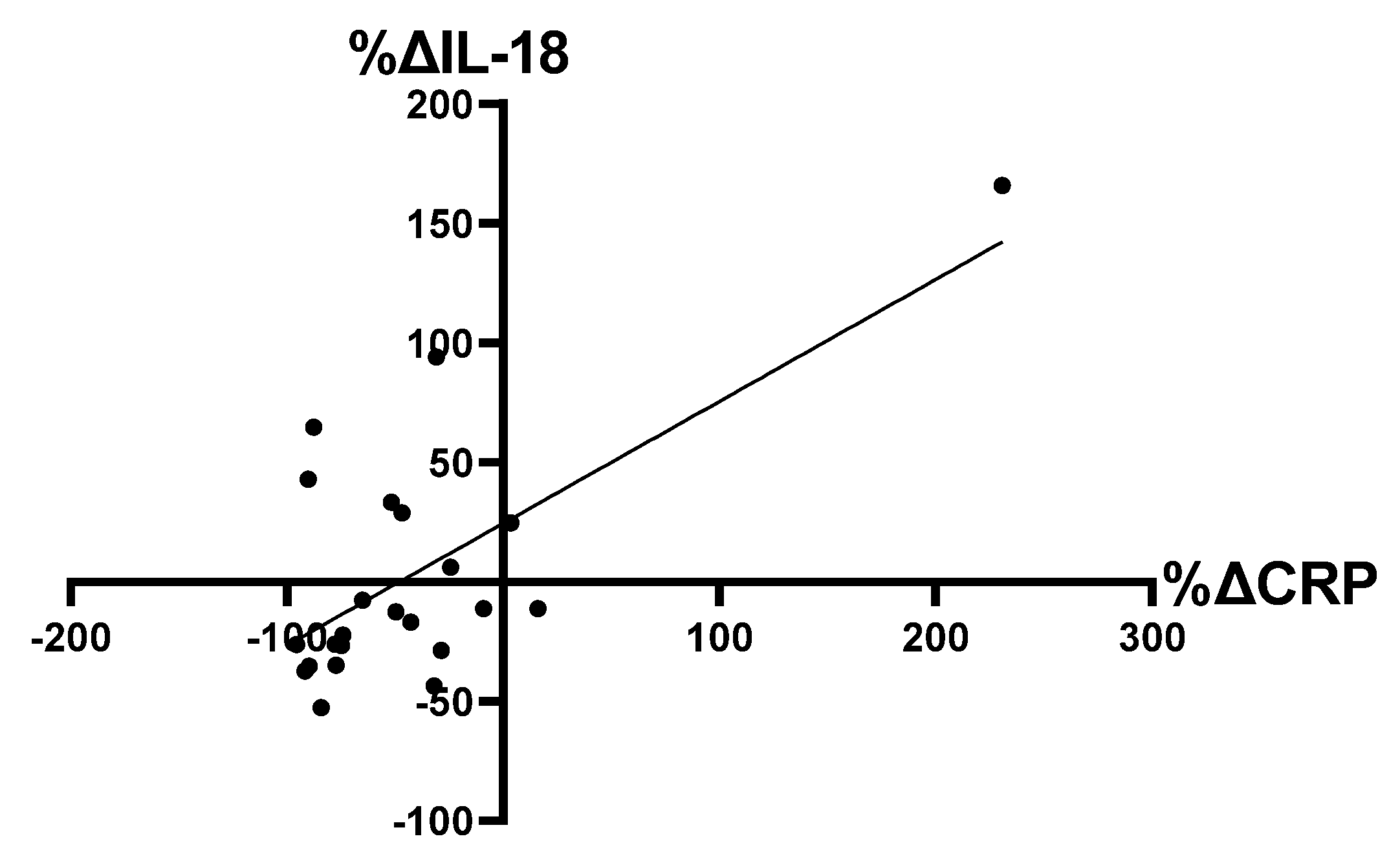
3.7. Correlation between Relative Changes in Plasma CRP and IL-18 Levels
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teo, Z.L.; Tham, Y.-C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y. Global prevalence of diabetic retinopathy and projection of burden through 2045: Systematic review and meta-analysis. Ophthalmology 2021, 128, 1580–1591. [Google Scholar] [CrossRef] [PubMed]
- Azad, N.; Agrawal, L.; Emanuele, N.V.; Klein, R.; Bahn, G.D.; Reaven, P. Association of blood glucose control and pancreatic reserve with diabetic retinopathy in the Veterans Affairs Diabetes Trial (VADT). Diabetologia 2014, 57, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Ipp, E.; Kumar, M. A Clinical Conundrum: Intensifying Glycemic Control in the Presence of Advanced Diabetic Retinopathy. Diabetes Care 2021, 44, 2192–2193. [Google Scholar] [CrossRef] [PubMed]
- Keech, A.C.; Mitchell, P.; Summanen, P.; O’Day, J.; Davis, T.M.; Moffitt, M.; Taskinen, M.-R.; Simes, R.J.; Tse, D.; Williamson, E. Effect of fenofibrate on the need for laser treatment for diabetic retinopathy (FIELD study): A randomised controlled trial. Lancet 2007, 370, 1687–1697. [Google Scholar] [CrossRef] [PubMed]
- The Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N. Engl. J. Med. 2008, 358, 2545–2559. [Google Scholar] [CrossRef] [PubMed]
- Chew, E.Y.; Davis, M.D.; Danis, R.P.; Lovato, J.F.; Perdue, L.H.; Greven, C.; Genuth, S.; Goff, D.C.; Leiter, L.A.; Ismail-Beigi, F. The effects of medical management on the progression of diabetic retinopathy in persons with type 2 diabetes: The Action to Control Cardiovascular Risk in Diabetes (ACCORD) Eye Study. Ophthalmology 2014, 121, 2443–2451. [Google Scholar] [CrossRef] [PubMed]
- ADVANCE Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 2008, 358, 2560–2572. [Google Scholar] [CrossRef] [PubMed]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Action to Control Cardiovascular Risk in Diabetes Follow-On (ACCORDION) Eye Study Group; the Action to Control Cardiovascular Risk in Diabetes Follow-On (ACCORDION) Study Group. Persistent effects of intensive glycemic control on retinopathy in type 2 diabetes in the action to control cardiovascular risk in diabetes (ACCORD) follow-on study. Diabetes Care 2016, 39, 1089–1100. [Google Scholar] [CrossRef]
- Stratton, I.; Kohner, E.; Aldington, S.; Turner, R.; Holman, R.; Manley, S.; Matthews, D.; The UKPDS Group. UKPDS 50: Risk factors for incidence and progression of retinopathy in Type II diabetes over 6 years from diagnosis. Diabetologia 2001, 44, 156–163. [Google Scholar] [CrossRef]
- Kim, E.L.; Moshfeghi, A.A. Effect of Intravitreal Anti-VEGF Therapy on the Severity of Diabetic Retinopathy. Curr. Ophthalmol. Rep. 2016, 4, 61–70. [Google Scholar] [CrossRef]
- Nicholson, B.P.; Schachat, A.P. A review of clinical trials of anti-VEGF agents for diabetic retinopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2010, 248, 915–930. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.Y.; Maran, J.J.; Jamieson, E.G.; Rupenthal, I.D.; Murphy, R.; Mugisho, O.O. Characterization of NLRP3 Inflammasome Activation in the Onset of Diabetic Retinopathy. Int. J. Mol. Sci. 2022, 23, 14471. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.Y.J.; Murphy, R.; Rupenthal, I.D.; Mugisho, O.O. Correlation between the progression of diabetic retinopathy and inflammasome biomarkers in vitreous and serum—A systematic review. BMC Ophthalmol. 2022, 22, 238. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhang, X.; Liao, N.; Mi, L.; Peng, Y.; Liu, B.; Zhang, S.; Wen, F. Enhanced Expression of NLRP3 Inflammasome-Related Inflammation in Diabetic Retinopathy. Investig. Ophthalmol. Vis. Sci. 2018, 59, 978–985. [Google Scholar] [CrossRef]
- Louie, H.H.; Shome, A.; Kuo, C.Y.; Rupenthal, I.D.; Green, C.R.; Mugisho, O.O. Connexin43 hemichannel block inhibits NLRP3 inflammasome activation in a human retinal explant model of diabetic retinopathy. Exp. Eye Res. 2020, 202, 108384. [Google Scholar] [CrossRef] [PubMed]
- Lyon, H.; Shome, A.; Rupenthal, I.D.; Green, C.R.; Mugisho, O.O. Tonabersat Inhibits Connexin43 Hemichannel Opening and Inflammasome Activation in an In Vitro Retinal Epithelial Cell Model of Diabetic Retinopathy. Int. J. Mol. Sci. 2021, 22, 298. [Google Scholar] [CrossRef] [PubMed]
- Mugisho, O.O.; Green, C.R.; Squirrell, D.M.; Bould, S.; Danesh-Meyer, H.V.; Zhang, J.; Acosta, M.L.; Rupenthal, I.D. Connexin43 hemichannel block protects against the development of diabetic retinopathy signs in a mouse model of the disease. J. Mol. Med. 2019, 97, 215–229. [Google Scholar] [CrossRef]
- Mugisho, O.O.; Rupenthal, I.D.; Paquet-Durand, F.; Acosta, M.L.; Green, C.R. Targeting connexin hemichannels to control the inflammasome: The correlation between connexin43 and NLRP3 expression in chronic eye disease. Expert Opin. Ther. Targets 2019, 23, 855–863. [Google Scholar] [CrossRef]
- Wright, A.; Dodson, P. Medical management of diabetic retinopathy: Fenofibrate and ACCORD Eye studies. Eye 2011, 25, 843–849. [Google Scholar] [CrossRef]
- Swanson, K.V.; Deng, M.; Ting, J.P.-Y. The NLRP3 inflammasome: Molecular activation and regulation to therapeutics. Nat. Rev. Immunol. 2019, 19, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Kowluru, R.A.; Mohammad, G.; Santos, J.M.; Tewari, S.; Zhong, Q. Interleukin-1β and mitochondria damage, and the development of diabetic retinopathy. J. Ocul. Biol. Dis. Infor. 2011, 4, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.M.; Faulenbach, M.; Vaag, A.; Vølund, A.; Ehses, J.A.; Seifert, B.; Mandrup-Poulsen, T.; Donath, M.Y. Interleukin-1–receptor antagonist in type 2 diabetes mellitus. N. Engl. J. Med. 2007, 356, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.M.; Faulenbach, M.; Vaag, A.; Ehses, J.A.; Donath, M.Y.; Mandrup-Poulsen, T. Sustained effects of interleukin-1 receptor antagonist treatment in type 2 diabetes. Diabetes Care 2009, 32, 1663–1668. [Google Scholar] [CrossRef] [PubMed]
- Stahel, M.; Becker, M.; Graf, N.; Michels, S. Systemic interleukin 1β inhibition in proliferative diabetic retinopathy: A prospective open-label study using canakinumab. Retina 2016, 36, 385. [Google Scholar] [CrossRef] [PubMed]
- Blankenberg, S.; Luc, G.; Ducimetière, P.; Arveiler, D.; Ferrières, J.; Amouyel, P.; Evans, A.; Cambien, F.o.; Tiret, L. Interleukin-18 and the risk of coronary heart disease in European men: The Prospective Epidemiological Study of Myocardial Infarction (PRIME). Circulation 2003, 108, 2453–2459. [Google Scholar] [CrossRef] [PubMed]
- Jefferis, B.J.; Papacosta, O.; Owen, C.G.; Wannamethee, S.G.; Humphries, S.E.; Woodward, M.; Lennon, L.T.; Thomson, A.; Welsh, P.; Rumley, A. Interleukin 18 and coronary heart disease: Prospective study and systematic review. Atherosclerosis 2011, 217, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Yasin, S.; Fall, N.; Brown, R.A.; Henderlight, M.; Canna, S.W.; Girard-Guyonvarc’h, C.; Gabay, C.; Grom, A.A.; Schulert, G.S. IL-18 as a biomarker linking systemic juvenile idiopathic arthritis and macrophage activation syndrome. Rheumatology 2020, 59, 361–366. [Google Scholar] [CrossRef]
- Miyauchi, K.; Takiyama, Y.; Honjyo, J.; Tateno, M.; Haneda, M. Upregulated IL-18 expression in type 2 diabetic subjects with nephropathy: TGF-β1 enhanced IL-18 expression in human renal proximal tubular epithelial cells. Diabetes Res. Clin. Pract. 2009, 83, 190–199. [Google Scholar] [CrossRef]
- Doyle, S.L.; López, F.J.; Celkova, L.; Brennan, K.; Mulfaul, K.; Ozaki, E.; Kenna, P.F.; Kurali, E.; Hudson, N.; Doggett, T. IL-18 immunotherapy for neovascular AMD: Tolerability and efficacy in nonhuman primates. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5424–5430. [Google Scholar] [CrossRef]
- Doyle, S.L.; Ozaki, E.; Brennan, K.; Humphries, M.M.; Mulfaul, K.; Keaney, J.; Kenna, P.F.; Maminishkis, A.; Kiang, A.-S.; Saunders, S.P. IL-18 attenuates experimental choroidal neovascularization as a potential therapy for wet age-related macular degeneration. Sci. Transl. Med. 2014, 6, 230ra244. [Google Scholar] [CrossRef] [PubMed]
- Hirano, Y.; Yasuma, T.; Mizutani, T.; Fowler, B.J.; Tarallo, V.; Yasuma, R.; Kim, Y.; Bastos-Carvalho, A.; Kerur, N.; Gelfand, B.D. IL-18 is not therapeutic for neovascular age-related macular degeneration. Nat. Med. 2014, 20, 1372–1375. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; MacFadyen, J.G.; Everett, B.M.; Libby, P.; Thuren, T.; Glynn, R.J.; Kastelein, J.; Koenig, W.; Genest, J.; Lorenzatti, A. Relationship of C-reactive protein reduction to cardiovascular event reduction following treatment with canakinumab: A secondary analysis from the CANTOS randomised controlled trial. Lancet 2018, 391, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Murphy, R.; Clarke, M.G.; Evennett, N.J.; John Robinson, S.; Lee Humphreys, M.; Hammodat, H.; Jones, B.; Kim, D.D.; Cutfield, R.; Johnson, M.H. Laparoscopic sleeve gastrectomy versus banded Roux-en-Y gastric bypass for diabetes and obesity: A prospective randomised double-blind trial. Obes. Surg. 2018, 28, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Murphy, R.; Jiang, Y.; Booth, M.; Babor, R.; MacCormick, A.; Hammodat, H.; Beban, G.; Barnes, R.M.; Vincent, A.L. Progression of diabetic retinopathy after bariatric surgery. Diabet. Med. 2015, 32, 1212–1220. [Google Scholar] [CrossRef]
- Diabetic Retinal Screening, Grading, Monitoring and Referral Guidance; Ministry of Health: Wellington, New Zealand, 2016; pp. 16–17.
- Davies, N.K. Clinical, Metabolic, and Microbial Responses to Sleeve Gastrectomy and Roux-en-Y Gastric Bypass: Results from a Randomised Clinical Trial. Doctoral Thesis, The University of Auckland, Auckland, New Zealand, 1023. [Google Scholar]
- Luminex Assay Human Premixed Multi-Analyte Kit. Available online: https://resources.rndsystems.com/pdfs/datasheets/lxsahm.pdf (accessed on 8 September 2020).
- Koenig, W.; Khuseyinova, N.; Baumert, J.; Thorand, B.; Loewel, H.; Chambless, L.; Meisinger, C.; Schneider, A.; Martin, S.; Kolb, H. Increased concentrations of C-reactive protein and IL-6 but not IL-18 are independently associated with incident coronary events in middle-aged men and women: Results from the MONICA/KORA Augsburg case–cohort study, 1984–2002. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2745–2751. [Google Scholar] [CrossRef]
- Bresnihan, B.; Roux-Lombard, P.; Murphy, E.; Kane, D.; FitzGerald, O.; Dayer, J. Serum interleukin 18 and interleukin 18 binding protein in rheumatoid arthritis. Ann. Rheum. Dis. 2002, 61, 726–729. [Google Scholar] [CrossRef]
- Ridker, P.M.; MacFadyen, J.G.; Thuren, T.; Libby, P. Residual inflammatory risk associated with interleukin-18 and interleukin-6 after successful interleukin-1β inhibition with canakinumab: Further rationale for the development of targeted anti-cytokine therapies for the treatment of atherothrombosis. Eur. Heart J. 2020, 41, 2153–2163. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Ambrosius, W.T.; Danis, R.; Ismail-Beigi, F.; Cushman, W.; Calles, J.; Banerji, M.; Schubart, U.; Chew, E.Y.; Group, A.S. Diabetic retinopathy, its progression, and incident cardiovascular events in the ACCORD trial. Diabetes Care 2013, 36, 1266–1271. [Google Scholar] [CrossRef]
- Kramer, C.K.; Rodrigues, T.C.; Canani, L.H.; Gross, J.L.; Azevedo, M.J. Diabetic retinopathy predicts all-cause mortality and cardiovascular events in both type 1 and 2 diabetes: Meta-analysis of observational studies. Diabetes Care 2011, 34, 1238–1244. [Google Scholar] [CrossRef]
- Wood, I.S.; Wang, B.; Jenkins, J.R.; Trayhurn, P. The pro-inflammatory cytokine IL-18 is expressed in human adipose tissue and strongly upregulated by TNFα in human adipocytes. Biochem. Biophys. Res. Commun. 2005, 337, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Rooney, T.; Murphy, E.; Benito, M.; Roux-Lombard, P.; FitzGerald, O.; Dayer, J.; Bresnihan, B. Synovial tissue interleukin-18 expression and the response to treatment in patients with inflammatory arthritis. Ann. Rheum. Dis. 2004, 63, 1393–1398. [Google Scholar] [CrossRef] [PubMed]
- Blankenberg, S.; Tiret, L.; Bickel, C.; Peetz, D.; Cambien, F.; Meyer, J.; Rupprecht, H.J. Interleukin-18 is a strong predictor of cardiovascular death in stable and unstable angina. Circulation 2002, 106, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Yamagami, H.; Kitagawa, K.; Hoshi, T.; Furukado, S.; Hougaku, H.; Nagai, Y.; Hori, M. Associations of serum IL-18 levels with carotid intima-media thickness. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1458–1462. [Google Scholar] [CrossRef] [PubMed]
- Qiu, F.; Ma, X.; Shin, Y.-H.; Chen, J.; Chen, Q.; Zhou, K.; Wu, W.; Liang, W.; Wu, Y.; Song, Q. Pathogenic role of human C-reactive protein in diabetic retinopathy. Clin. Sci. 2020, 134, 1613–1629. [Google Scholar] [CrossRef] [PubMed]
- Thykjær, A.S.; Rosengaard, L.; Andersen, N.; Andresen, J.; Bek, T.; Hajari, J.; Heegaard, S.; Højlund, K.; Kawasaki, R.; Laugesen, C.S. Bariatric surgery in individuals with type 2 diabetes is not associated with short or long-term risk of diabetic retinopathy progression: Results from a nationwide cohort study. Acta Diabetol. 2023. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade and Description | Clinical Signs |
|---|---|
| R0, no DR | No abnormalities |
| R1, minimal | Less than 5 microaneurysms (MA) or dot hemorrhages |
| R2, mild | >4 MAs or dot hemorrhages. Exudates more than 3 disc diameters from fovea. Some blots and larger hemorrhages acceptable. If more than 20 MAs or hemorrhages per photographic field, upgrade to R3 moderate |
| R3, moderate | Any features of mild. Blot or large hemorrhages. Up to one quadrant of venous beading |
| R4, severe | One or more of (1) definite intra-retinal microvascular abnormalities, (2) two quadrants or more of venous beading, (3) four quadrants of blot or larger hemorrhages |
| R5, proliferative | One or more of (1) neovascularization, (2) sub-hyaloid or vitreous hemorrhage, (3) tractional retinal detachment or retinal gliosis |
| Assay Sensitivity | Pre-Surgery (n = 24) | Post-Surgery (n = 24) | p | |
|---|---|---|---|---|
| Weight (kg) | N/A | 115.90 (108.7–131.6) | 80.55 (72.43–96.65) | <0.0001 |
| HbA1c (%) | N/A | 8.00 (7.20–8.50) | 6.10 (5.50–6.50) | <0.0001 |
| IL-18 (pg/mL) | 1.93 | 22.72 (18.16–29.49) | 21.01 (17.01–25.48) | 0.51 |
| CRP (pg/mL) | 116 | 17,909 (12,775–27,742) | 4983 (2145–13,348) | <0.0001 |
| TNF-α (pg/mL) | 1.2 | 0.73 (0.48–1.09) | 0.61 (0.480.95) | 0.70 |
| IL-6 (pg/mL) | 1.7 | 0.25 (0.12–0.46) | 0.12 (0.08–0.43) | 0.71 |
| IL-8 (pg/mL) | 1.8 | 0.64 (0.48–1.09) | 0.65 (0.46–1.33) | 0.48 |
| VEGF (pg/mL) | 2.1 | 1.69 (1.17–4.26) | 1.73 (1.00–3.67) | 0.43 |
| IL-1β | 0.8 | 0.34 (0.18–0.65) | 0.34 (0.18–0.86) | 0.0677 |
| IL-10 | 1.6 | 0.64 (0.49–0.78) | 0.97 (0.68–1.34) | 0.1609 |
| DR Grade | % Change | |||||
|---|---|---|---|---|---|---|
| Pre | Post | Weight | HbA1c | IL-18 | CRP | |
| Regressed | 1 | 0 | −27.02 | 21.18 | −12.68 | −49.60 |
| 1 | 0 | −39.32 | −27.78 | −35.33 | −89.82 | |
| 1 | 0 | −44.64 | −34.88 | 42.86 | −90.24 | |
| Progressed | 1 | 2 | −33.89 | −15.58 | −11.40 | 15.96 |
| 1 | 3 | −31.91 | −16.22 | 165.85 | 230.80 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, C.Y.-J.; Rupenthal, I.D.; Booth, M.; Murphy, R.; Mugisho, O.O. Systemic Inflammasome Biomarkers as Predictors of Diabetic Retinopathy Progression: Evidence from a Pilot Study. Future Pharmacol. 2023, 3, 612-624. https://doi.org/10.3390/futurepharmacol3030039
Kuo CY-J, Rupenthal ID, Booth M, Murphy R, Mugisho OO. Systemic Inflammasome Biomarkers as Predictors of Diabetic Retinopathy Progression: Evidence from a Pilot Study. Future Pharmacology. 2023; 3(3):612-624. https://doi.org/10.3390/futurepharmacol3030039
Chicago/Turabian StyleKuo, Charisse Y.-J., Ilva D. Rupenthal, Michael Booth, Rinki Murphy, and Odunayo O. Mugisho. 2023. "Systemic Inflammasome Biomarkers as Predictors of Diabetic Retinopathy Progression: Evidence from a Pilot Study" Future Pharmacology 3, no. 3: 612-624. https://doi.org/10.3390/futurepharmacol3030039