
Impacts of Varying Blood Flow Restriction Cuff Size and Material on Arterial, Venous and Calf Muscle Pump-Mediated Blood Flow
 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
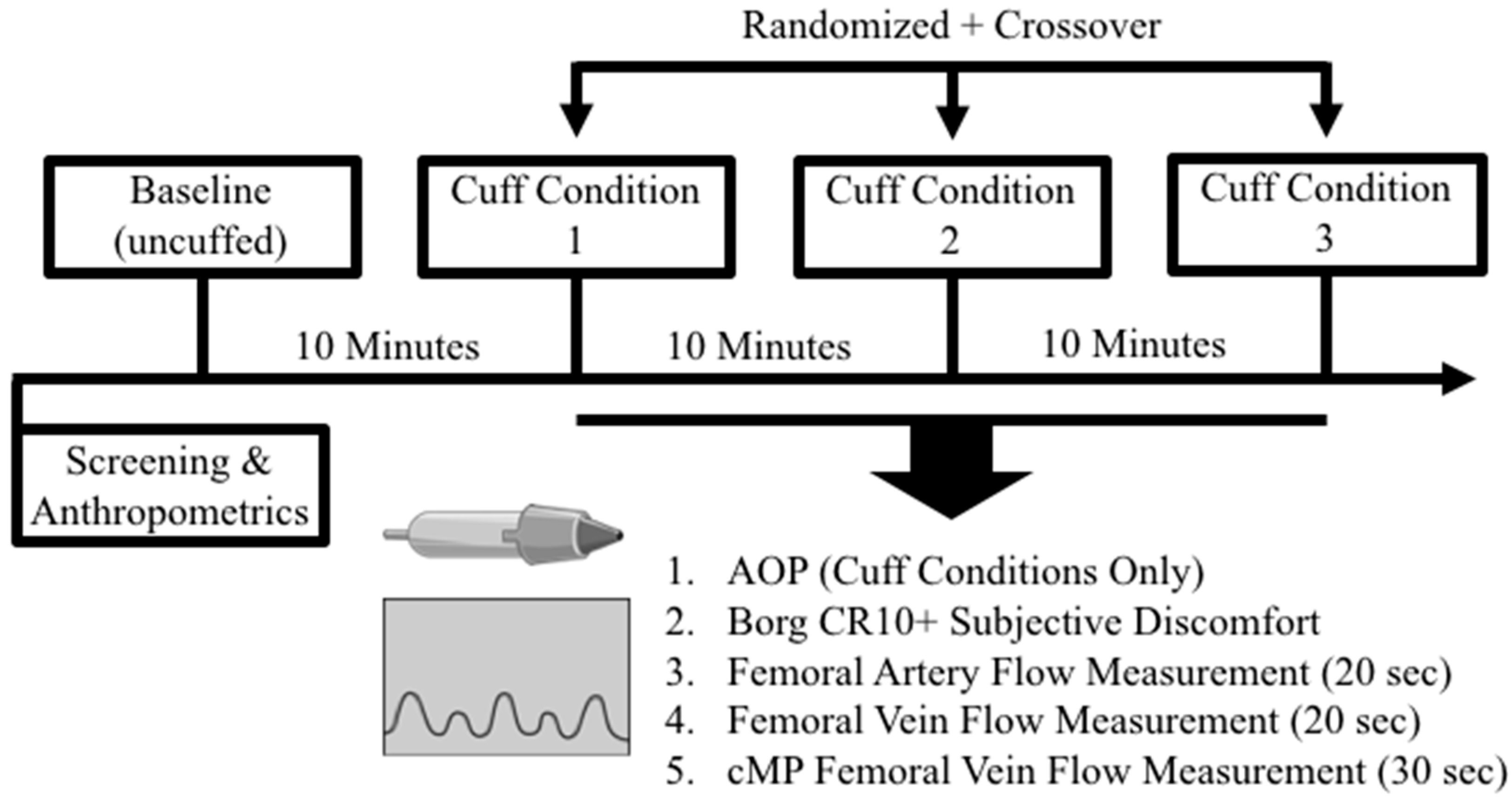
2.1. Experimental Approach to the Problem
2.2. Participants
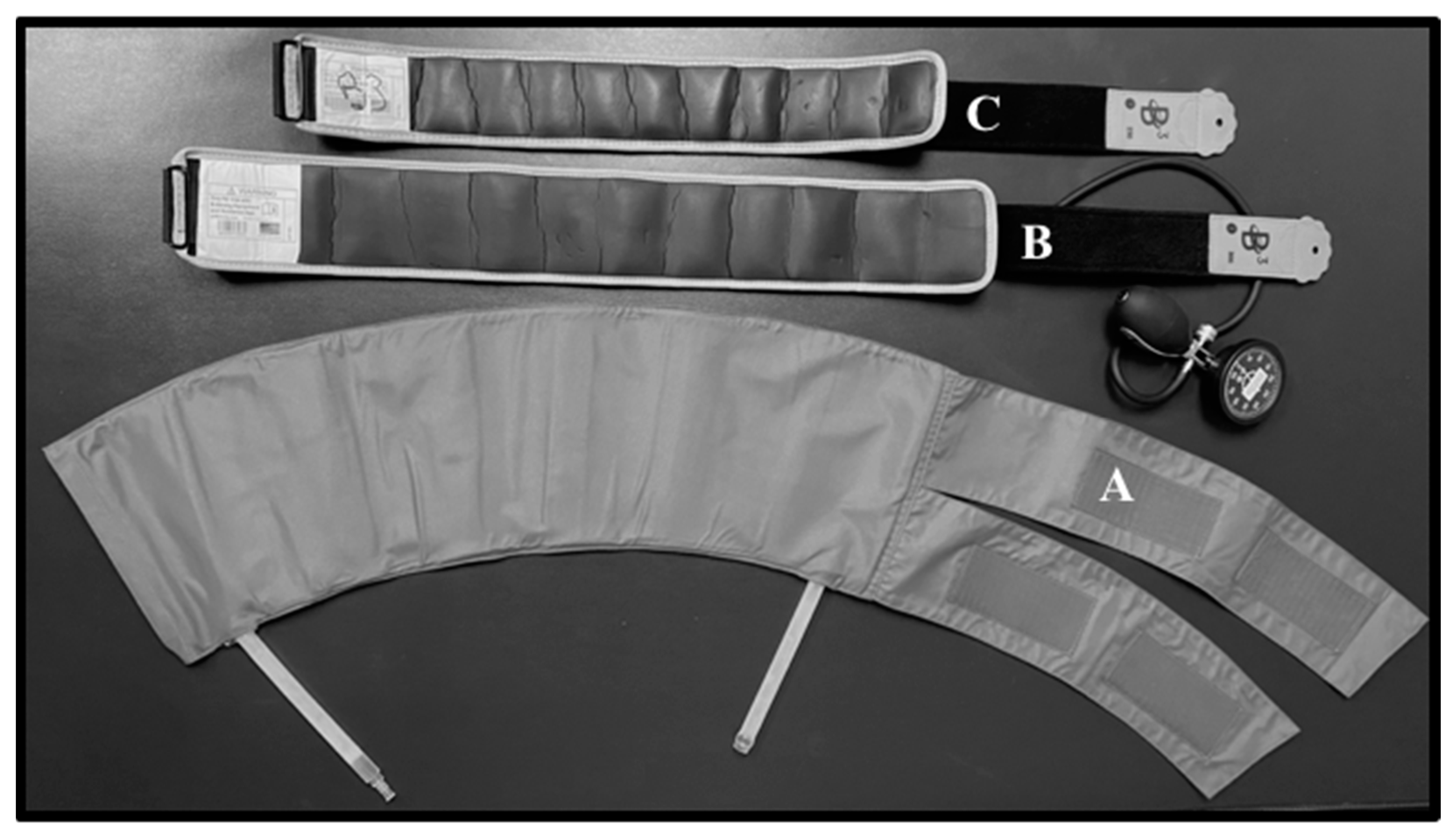
2.3. Cuff Procedures
2.4. Ultrasound Arterial Occlusion Pressure and Blood Flow Assessments
2.5. Subjective Discomfort
2.6. Statistical Analyses
3. Results
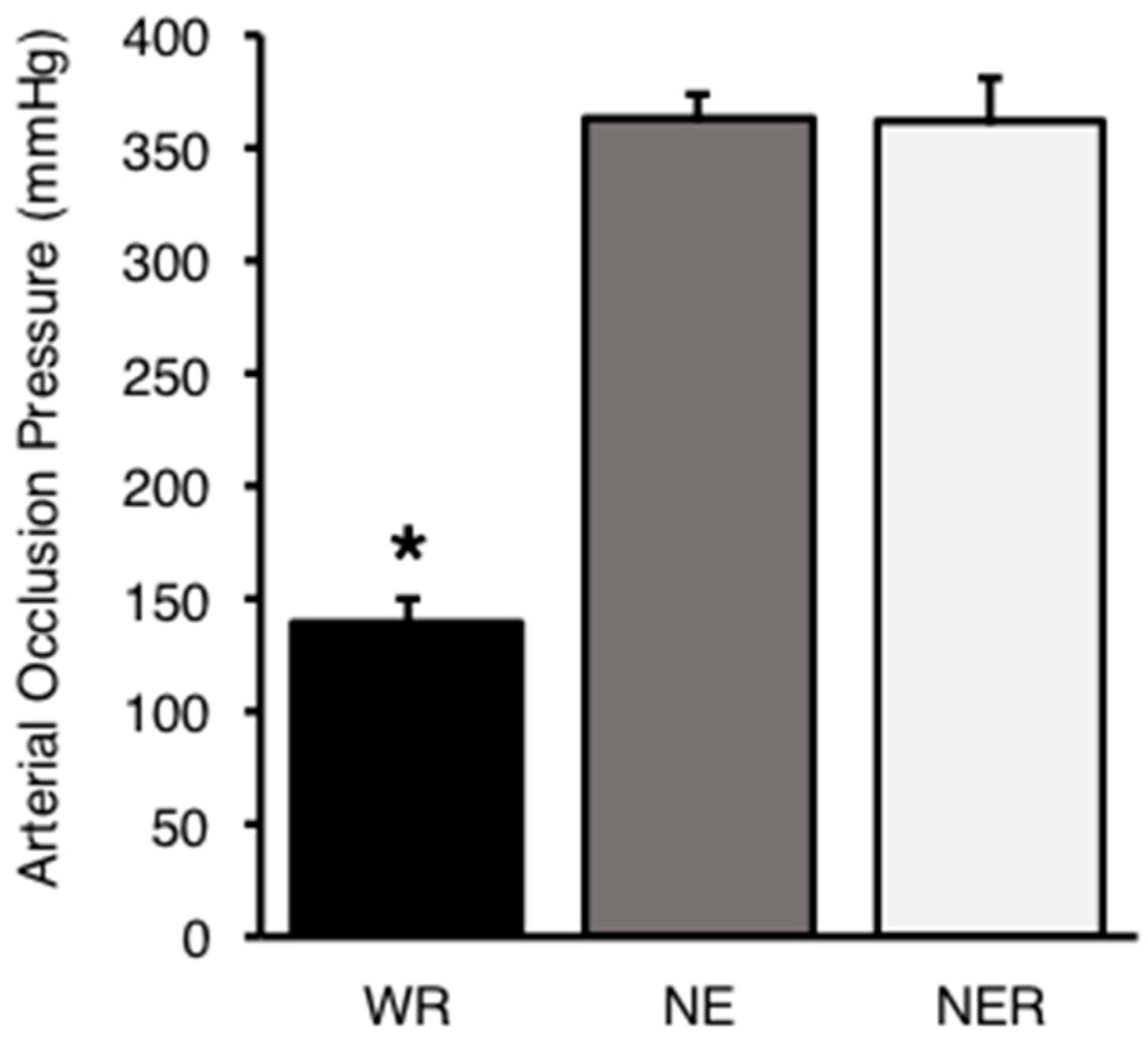
3.1. Arterial Occlusion Pressure
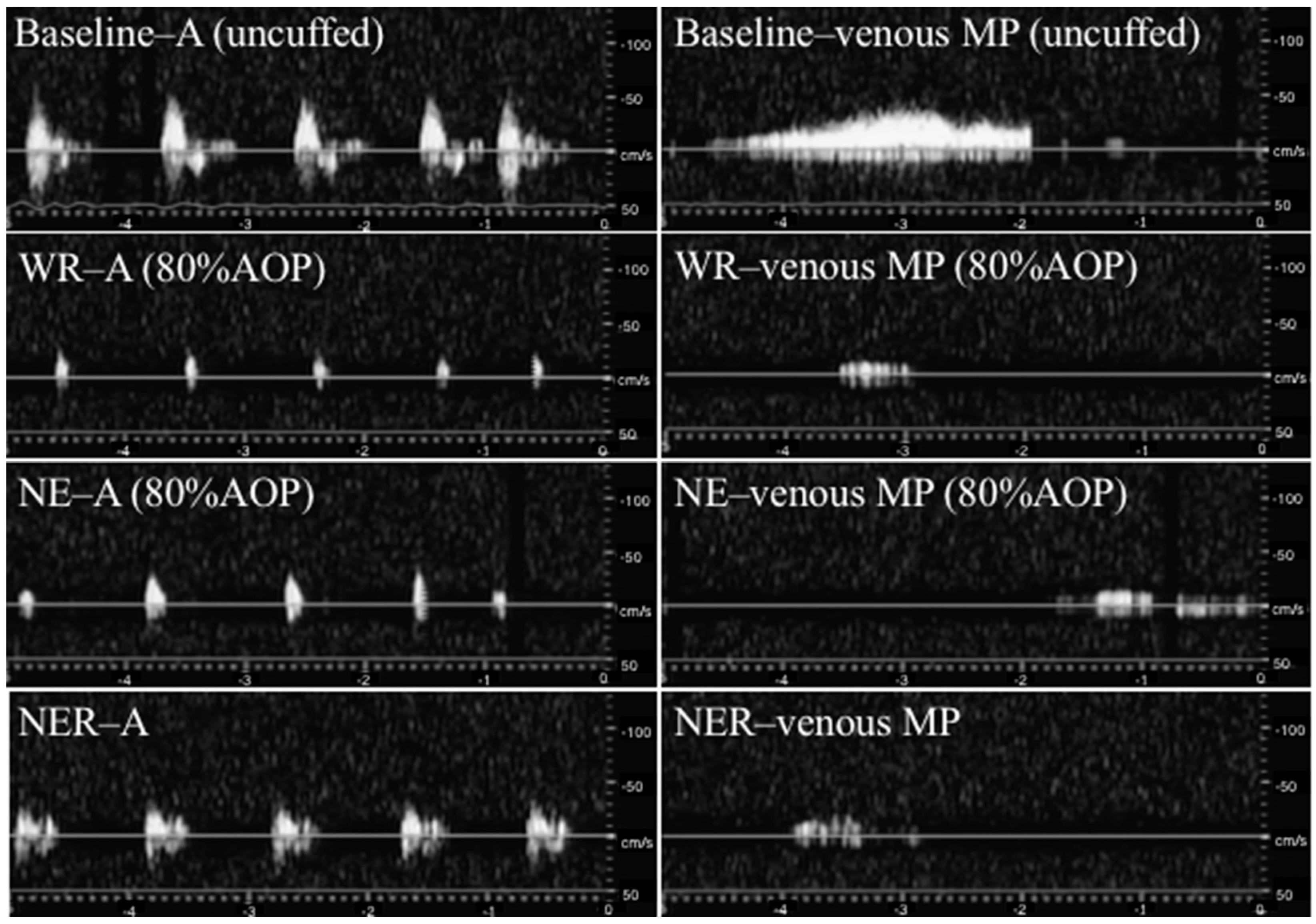
3.2. Blood Flow Assessments
3.3. Subjective Discomfort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Machek, S.B.; Cardaci, T.D.; Willoughby, D.S. Blood flow restriction training and betaine supplementation as a novel combined modalitiy to augment skeletal muscle adaptation: A short review. Strength Cond. J. 2021, 43, 50–63. [Google Scholar] [CrossRef]
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Exercise with blood flow restriction: An updated evidence-based approach for enhanced muscular development. Sports Med. 2015, 45, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Fatela, P.; Mendonca, G.V.; Veloso, A.P.; Avela, J.; Mil-Homens, P. Blood Flow Restriction Alters Motor Unit Behavior During Resistance Exercise. Int. J. Sports Med. 2019, 40, 555–562. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Thiebaud, R.S.; Mattocks, K.T.; Abe, T.; Bemben, M.G. Blood flow restriction pressure recommendations: A tale of two cuffs. Front. Physiol. 2013, 4, 249. [Google Scholar] [CrossRef]
- Wooten, S.V.; Stray-Gundersen, S.; Tanaka, H. Hemodynamic and Pressor Responses to Combination of Yoga and Blood Flow Restriction. Int. J. Sports Med. 2020, 41, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Stray-Gundersen, S.; Wooten, S.; Tanaka, H. Walking With Leg Blood Flow Restriction: Wide-Rigid Cuffs vs. Narrow-Elastic Bands. Front. Physiol. 2020, 11, 568. [Google Scholar] [CrossRef] [PubMed]
- Spranger, M.D.; Krishnan, A.C.; Levy, P.D.; O’Leary, D.S.; Smith, S.A. Blood flow restriction training and the exercise pressor reflex: A call for concern. Am. J. Physiol. Heart Circ. Physiol. 2015, 309, H1440–H1452. [Google Scholar] [CrossRef]
- Bjornsen, T.; Wernbom, M.; Kirketeig, A.; Paulsen, G.; Samnoy, L.; Bækken, L.; Cameron-Smith, D.; Berntsen, S.; Raastad, T. Type 1 muscle fiber hypertrophy after blood flow-restricted training in powerlifters. Med. Sci. Sports Exerc. 2018, 51, 288–298. [Google Scholar] [CrossRef]
- Behringer, M.; Behlau, D.; Montag, J.C.K.; McCourt, M.L.; Mester, J. Low-Intensity Sprint Training With Blood Flow Restriction Improves 100-m Dash. J. Strength Cond. Res. 2017, 31, 2462–2472. [Google Scholar] [CrossRef]
- Patterson, S.D.; Hughes, L.; Warmington, S.; Burr, J.; Scott, B.R.; Owens, J.; Abe, T.; Nielsen, J.L.; Libardi, C.A.; Laurentino, G.; et al. Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Front. Physiol. 2019, 10, 533. [Google Scholar] [CrossRef]
- Lima-Soares, F.; Pessoa, K.A.; Torres Cabido, C.E.; Lauver, J.; Cholewa, J.; Rossi, F.; Zanchi, N.E. Determining the Arterial Occlusion Pressure for Blood Flow Restriction: Pulse Oximeter as a New Method Compared With a Handheld Doppler. J. Strength Cond. Res. 2022, 36, 1120–1124. [Google Scholar] [CrossRef]
- Buckner, S.L.; Dankel, S.J.; Counts, B.R.; Jessee, M.B.; Mouser, J.G.; Mattocks, K.T.; Laurentino, G.C.; Abe, T.; Loenneke, J.P. Influence of cuff material on blood flow restriction stimulus in the upper body. J. Physiol. Sci. 2017, 67, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Weatherholt, A.M.; Vanwye, W.R.; Lohmann, J.; Owens, J.G. The Effect of Cuff Width for Determining Limb Occlusion Pressure: A Comparison of Blood Flow Restriction Devices. Int. J. Exerc. Sci. 2019, 12, 136–143. [Google Scholar] [PubMed]
- Loenneke, J.P.; Thiebaud, R.S.; Fahs, C.A.; Rossow, L.M.; Abe, T.; Bemben, M.G. Blood flow restriction: Effects of cuff type on fatigue and perceptual responses to resistance exercise. Acta Physiol. Hung. 2014, 101, 158–166. [Google Scholar] [CrossRef]
- Kilgas, M.A.; McDaniel, J.; Stavres, J.; Pollock, B.S.; Singer, T.J.; Elmer, S.J. Limb blood flow and tissue perfusion during exercise with blood flow restriction. Eur. J. Appl. Physiol. 2019, 119, 377–387. [Google Scholar] [CrossRef]
- Lalchhuanawma, A.; Sanhgi, D. The effect of strength training on the calf muscle pump on cardiovascular parameters. Arch. Med. Health Sci. 2020, 8, 26–30. [Google Scholar] [CrossRef]
- Holder, S.M.; Brislane, A.; Dawson, E.A.; Hopkins, N.D.; Hopman, M.T.E.; Cable, N.T.; Jones, H.; Schreuder, T.H.A.; Sprung, V.S.; Naylor, L.; et al. Relationship Between Endothelial Function and the Eliciting Shear Stress Stimulus in Women: Changes Across the Lifespan Differ to Men. J. Am. Heart Assoc. 2019, 8, e010994. [Google Scholar] [CrossRef] [PubMed]
- Keiler, J.; Seidel, R.; Wree, A. The femoral vein diameter and its correlation with sex, age and body mass index—An anatomical parameter with clinical relevance. Phlebology 2019, 34, 58–69. [Google Scholar] [CrossRef]
- Machek, S.B.; Harris, D.R.; Zawieja, E.E.; Heileson, J.L.; Wilburn, D.T.; Radziejewska, A.; Chmurzynska, A.; Cholewa, J.M.; Willoughby, D.S. The Impacts of Combined Blood Flow Restriction Training and Betaine Supplementation on One-Leg Press Muscular Endurance, Exercise-Associated Lactate Concentrations, Serum Metabolic Biomarkers, and Hypoxia-Inducible Factor-1alpha Gene Expression. Nutrients 2022, 14, 5040. [Google Scholar] [CrossRef]
- Machek, S.B.; Zawieja, E.E.; Heileson, J.L.; Harris, D.R.; Wilburn, D.T.; Fletcher, E.A.; Cholewa, J.M.; Szwengiel, A.; Chmurzynska, A.; Willoughby, D.S. Human Serum Betaine and Associated Biomarker Concentrations Following a 14 Day Supplemental Betaine Loading Protocol and during a 28 Day Washout Period: A Pilot Investigation. Nutrients 2022, 14, 498. [Google Scholar] [CrossRef]
- Wilburn, D.T.; Machek, S.B.; Zechmann, B.; Willoughby, D.S. Comparison of skeletal muscle ultrastructural changes between normal and blood flow restricted resistance exercise: A case report. Exp. Physiol. 2021, 106, 2177–2184. [Google Scholar] [CrossRef] [PubMed]
- Riebe, D.; Franklin, B.A.; Thompson, P.D.; Garber, C.E.; Whitfield, G.P.; Magal, M.; Pescatello, L.S. Updating ACSM’s Recommendations for Exercise Preparticipation Health Screening. Med. Sci. Sports Exerc. 2015, 47, 2473–2479. [Google Scholar] [CrossRef]
- Sugawara, J.; Tomoto, T.; Tanaka, H. Impact of leg blood flow restriction during walking on central arterial hemodynamics. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 309, R732–R739. [Google Scholar] [CrossRef] [PubMed]
- Citherlet, T.; Willis, S.J.; Chaperon, A.; Millet, G.P. Differences in the limb blood flow between two types of blood flow restriction cuffs: A pilot study. Front. Physiol. 2022, 13, 931270. [Google Scholar] [CrossRef]
- Wooten, S.V.; Fleming, R.Y.D.; Wolf, J.S., Jr.; Stray-Gundersen, S.; Bartholomew, J.B.; Mendoza, D.; Stanforth, P.R.; Stanforth, D.; Hernandez, L.M.; Tanaka, H. Prehabilitation program composed of blood flow restriction training and sports nutrition improves physical functions in abdominal cancer patients awaiting surgery. Eur. J. Surg. Oncol. 2021, 47, 2952–2958. [Google Scholar] [CrossRef]
- Papadakis, Z.; Forsse, J.S.; Peterson, M.N. Acute partial sleep deprivation and high-intensity interval exercise effects on postprandial endothelial function. Eur. J. Appl. Physiol. 2020, 120, 2431–2444. [Google Scholar] [CrossRef]
- Woodman, R.J.; Playford, D.A.; Watts, G.F.; Cheetham, C.; Reed, C.; Taylor, R.R.; Puddey, I.B.; Beilin, L.J.; Burke, V.; Mori, T.A.; et al. Improved analysis of brachial artery ultrasound using a novel edge-detection software system. J. Appl. Physiol. 2001, 91, 929–937. [Google Scholar] [CrossRef]
- Lixandrao, M.E.; Ugrinowitsch, C.; Laurentino, G.; Libardi, C.A.; Aihara, A.Y.; Cardoso, F.N.; Tricoli, V.; Roschel, H. Effects of exercise intensity and occlusion pressure after 12 weeks of resistance training with blood-flow restriction. Eur. J. Appl. Physiol. 2015, 115, 2471–2480. [Google Scholar] [CrossRef]
- Ilett, M.J.; Rantalainen, T.; Keske, M.A.; May, A.K.; Warmington, S.A. The Effects of Restriction Pressures on the Acute Responses to Blood Flow Restriction Exercise. Front. Physiol. 2019, 10, 1018. [Google Scholar] [CrossRef] [PubMed]
- Cristomo, R.; Candeias, M.; Armada-da-Siva, P. The use of ultrasound in the evaluation of the efficacy of calf muscle pump function in primary chronic venous disease. Phlebology 2012, 29, 247–256. [Google Scholar] [CrossRef]
- Bell, Z.W.; Dankel, S.J.; Spitz, R.W.; Chatakondi, R.N.; Abe, T.; Loenneke, J.P. The Perceived Tightness Scale Does Not Provide Reliable Estimates of Blood Flow Restriction Pressure. J. Sport Rehabil. 2020, 29, 516–518. [Google Scholar] [CrossRef] [PubMed]
- Billinger, S.A.; Gajewski, B.J.; Guo, L.X.; Kluding, P.M. Single limb exercise induces femoral artery remodeling and improves blood flow in the hemiparetic leg poststroke. Stroke 2009, 40, 3086–3090. [Google Scholar] [CrossRef]
- Radegran, G. Ultrasound Doppler estimates of femoral artery blood flow during dynamic knee extensor exercise in humans. J. Appl. Physiol. 1997, 83, 1383–1388. [Google Scholar] [CrossRef]
- Merkx, M.A.; Bescos, J.O.; Geerts, L.; Bosboom, E.M.; van de Vosse, F.N.; Breeuwer, M. Accuracy and precision of vessel area assessment: Manual versus automatic lumen delineation based on full-width at half-maximum. J. Magn. Reson. Imaging 2012, 36, 1186–1193. [Google Scholar] [CrossRef]
- O’Connor, K.; Stip, E.; Pelissier, M.C.; Aardema, F.; Guay, S.; Gaudette, G.; Van Haaster, I.; Robillard, S.; Grenier, S.; Careau, Y.; et al. Treating delusional disorder: A comparison of cognitive-behavioural therapy and attention placebo control. Can. J. Psychiatry 2007, 52, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Mouser, J.G.; Dankel, S.J.; Jessee, M.B.; Mattocks, K.T.; Buckner, S.L.; Counts, B.R.; Loenneke, J.P. A tale of three cuffs: The hemodynamics of blood flow restriction. Eur. J. Appl. Physiol. 2017, 117, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Larkin, K.A.; Macneil, R.G.; Dirain, M.; Sandesara, B.; Manini, T.M.; Buford, T.W. Blood flow restriction enhances post-resistance exercise angiogenic gene expression. Med. Sci. Sports Exerc. 2012, 44, 2077–2083. [Google Scholar] [CrossRef]
- Fahs, C.A.; Rossow, L.M.; Thiebaud, R.S.; Loenneke, J.P.; Kim, D.; Abe, T.; Beck, T.W.; Feeback, D.L.; Bemben, D.A.; Bemben, M.G. Vascular adaptations to low-load resistance training with and without blood flow restriction. Eur. J. Appl. Physiol. 2014, 114, 715–724. [Google Scholar] [CrossRef]
- Takano, H.; Morita, T.; Iida, H.; Asada, K.; Kato, M.; Uno, K.; Hirose, K.; Matsumoto, A.; Takenaka, K.; Hirata, Y.; et al. Hemodynamic and hormonal responses to a short-term low-intensity resistance exercise with the reduction of muscle blood flow. Eur. J. Appl. Physiol. 2005, 95, 65–73. [Google Scholar] [CrossRef]
- Abe, T.; Fujita, S.; Nakajima, T.; Sakamaki, M.; Ozaki, H.; Ogasawara, R.; Sugaya, M.; Kudo, M.; Kurano, M.; Yasuda, T.; et al. Effects of Low-Intensity Cycle Training with Restricted Leg Blood Flow on Thigh Muscle Volume and VO2MAX in Young Men. J. Sports Sci. Med. 2010, 9, 452–458. [Google Scholar]
- Rolnick, N.; Kimbrell, K.; de Queiros, V. Beneath the cuff: Often overlooked and under-reported blood flow restriction device features and their potential impact on practice—A review of the current state of the research. Front. Physiol. 2023, 14, 436. [Google Scholar] [CrossRef] [PubMed]
- Jazuli, F.; Pyke, K.E. The impact of baseline artery diameter on flow-mediated vasodilation: A comparison of brachial and radial artery responses to matched levels of shear stress. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, H1667–H1677. [Google Scholar] [CrossRef] [PubMed]
- Sandgren, T.; Sonesson, B.; Ahlgren, R.; Lanne, T. The diameter of the common femoral artery in healthy human: Influence of sex, age, and body size. J. Vasc. Surg. 1999, 29, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Casey, D.P. Regulation of increased blood flow (hyperemia) to muscles during exercise: A hierarchy of competing physiological needs. Physiol. Rev. 2015, 95, 549–601. [Google Scholar] [CrossRef]
- Hamann, J.J.; Valic, Z.; Buckwalter, J.B.; Clifford, P.S. Muscle pump does not enhance blood flow in exercising skeletal muscle. J. Appl. Physiol. 2003, 94, 6–10. [Google Scholar] [CrossRef]
- Singer, T.J.; Stavres, J.; Elmer, S.J.; Kilgas, M.A.; Pollock, B.S.; Kearney, S.G.; McDaniel, J. Knee extension with blood flow restriction: Impact of cuff pressure on hemodynamics. Eur. J. Appl. Physiol. 2020, 120, 79–90. [Google Scholar] [CrossRef]
- Osada, T.; Saltin, B.; Mortensen, S.; Radergran, G. Measurement of the exercising blood flow during rythmical muscle contractiosn assessed by Doppler ultrasound: Methodological considerations. J. Biomed. Sci. Eng. 2012, 5, 10. [Google Scholar] [CrossRef]
- Mattocks, K.T.; Jessee, M.B.; Counts, B.R.; Buckner, S.L.; Grant Mouser, J.; Dankel, S.J.; Laurentino, G.C.; Loenneke, J.P. The effects of upper body exercise across different levels of blood flow restriction on arterial occlusion pressure and perceptual responses. Physiol. Behav. 2017, 171, 181–186. [Google Scholar] [CrossRef]
- Barnett, B.E.; Dankel, S.J.; Counts, B.R.; Nooe, A.L.; Abe, T.; Loenneke, J.P. Blood flow occlusion pressure at rest and immediately after a bout of low load exercise. Clin. Physiol. Funct. Imaging 2016, 36, 436–440. [Google Scholar] [CrossRef]
- Cerqueira, M.S.; Costa, E.C.; Santos Oliveira, R.; Pereira, R.; Brito Vieira, W.H. Blood Flow Restriction Training: To Adjust or Not Adjust the Cuff Pressure Over an Intervention Period? Front. Physiol. 2021, 12, 678407. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Fujita, T.; Miyagi, Y.; Kubota, Y.; Sato, Y.; Nakajima, T.; Bemben, M.G.; Abe, T. Electromyographic responses of arm and chest muscle during bench press exercise with and without Kaatsu. Int. J. Kaatsu Train. Res. 2006, 2, 15–18. [Google Scholar] [CrossRef]
- Abe, T.; Kawamoto, K.; Yasuda, T.; Kearns, C.F.; Midorikawa, T.; Sato, Y. Eight days KAATSU-resistance training improved sprint but not jump performance in collegiate male track and field athletes. Int. J. Kaatsu Train. Res. 2005, 1, 19–23. [Google Scholar] [CrossRef]
- Fujita, S.; Abe, T.; Drummond, M.J.; Cadenas, J.G.; Dreyer, H.C.; Sato, Y.; Volpi, E.; Rasmussen, B.B. Blood flow restriction during low-intensity resistance exercise increases S6K1 phosphorylation and muscle protein synthesis. J. Appl. Physiol. 2007, 103, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, T.; Yasuda, T.; Fukumura, K.; Lida, H.; Morita, T.; Sato, Y.; Nakajima, T. Low-intensity kaatsu resistance exercises using an elastic band enhance muscle activation in patients with cardiovascular diseases. Int. J. Kaatsu Train. Res. 2013, 9, 1–5. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject Characteristics (n = 20) | Mean ± SD |
|---|---|
| Age (years) | 25 ± 5 |
| Height (cm) | 175.2 ± 6.0 |
| Weight (kg) | 85.2 ± 12.0 |
| Right Leg Circumference (cm) | 61.3 ± 6.3 |
| Resting SBP (mmHg) | 125 ± 13 |
| Resting DBP (mmHg) | 75 ± 13 |
| Resting Heart Rate (bpm) | 66 ± 11 |
| Code | Product | Length (cm) | Width (cm) | Max Pressure (mmHg) |
|---|---|---|---|---|
| WR | Hokansen CC17 | 108.0 | 18.0 | 300 |
| NE | B3 Size #4 | 60.96 | 9.53 | 500 |
| NER * | B3 Size #4 | “ | “ | “ |
| B3 Size #3 | 50.80 | 7.62 | 500 |
| Arterial & Venous Blood Flow Parameters | ||||||
|---|---|---|---|---|---|---|
| Mean ± SD m•s−1 | Mean A Flow | Peak A Flow | Mean V Flow | Peak V Flow | Mean MP Flow | Peak MP Flow |
| Baseline | 0.101 ± 0.065 | 0.328 ± 0.101 | 0.103 ± 0.065 | 0.156 ± 0.086 | 0.215 ± 0.097 | 0.325 ± 0.133 |
| WR | 0.064 ± 0.062 | 0.283 ± 0.152 | 0.000 | 0.000 | 0.087 ± 0.049 | 0.190 ± 0.067 |
| NE | 0.051 ± 0.028 | 0.238 ± 0.050 | 0.000 | 0.000 | 0.066 ± 0.044 | 0.177 ± 0.106 |
| NER | 0.041 ± 0.019 | 0.215 ± 0.056 | 0.000 | 0.000 | 0.093 ± 0.082 | 0.200 ± 0.126 |
| NER Exceeding AOP * | ||||||
| Participant Code | NER RecP (mmHg) | NER AOP (mmHg) | NER RecP % AOP | |||
| P4 | 300 | 250 | 120 | |||
| P5 | 300 | 280 | 107 | |||
| P7 | 300 | 300 | 100 | |||
| P17 | 300 | 300 | 100 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machek, S.B.; Harris, D.R.; Heileson, J.L.; Wilburn, D.T.; Forsse, J.S.; Willoughby, D.S. Impacts of Varying Blood Flow Restriction Cuff Size and Material on Arterial, Venous and Calf Muscle Pump-Mediated Blood Flow. Oxygen 2023, 3, 190-202. https://doi.org/10.3390/oxygen3020014
Machek SB, Harris DR, Heileson JL, Wilburn DT, Forsse JS, Willoughby DS. Impacts of Varying Blood Flow Restriction Cuff Size and Material on Arterial, Venous and Calf Muscle Pump-Mediated Blood Flow. Oxygen. 2023; 3(2):190-202. https://doi.org/10.3390/oxygen3020014
Chicago/Turabian StyleMachek, Steven B., Dillon R. Harris, Jeffery L. Heileson, Dylan T. Wilburn, Jeffrey S. Forsse, and Darryn S. Willoughby. 2023. "Impacts of Varying Blood Flow Restriction Cuff Size and Material on Arterial, Venous and Calf Muscle Pump-Mediated Blood Flow" Oxygen 3, no. 2: 190-202. https://doi.org/10.3390/oxygen3020014