
Hemodynamic Responses to a Handgrip Exercise Session, with and without Blood Flow Restriction, in Healthy Volunteers
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measures
2.3.1. Blood Pressure with Digital Sphygmomanometer
2.3.2. Heart Rate with Oscilloscope
2.3.3. Blood Oxygen Saturation with Pulse Oximeter
2.3.4. Rating of Perceived Exertion with the Borg Scale
2.4. Exercise Protocol
2.5. Statistical Analysis
3. Results
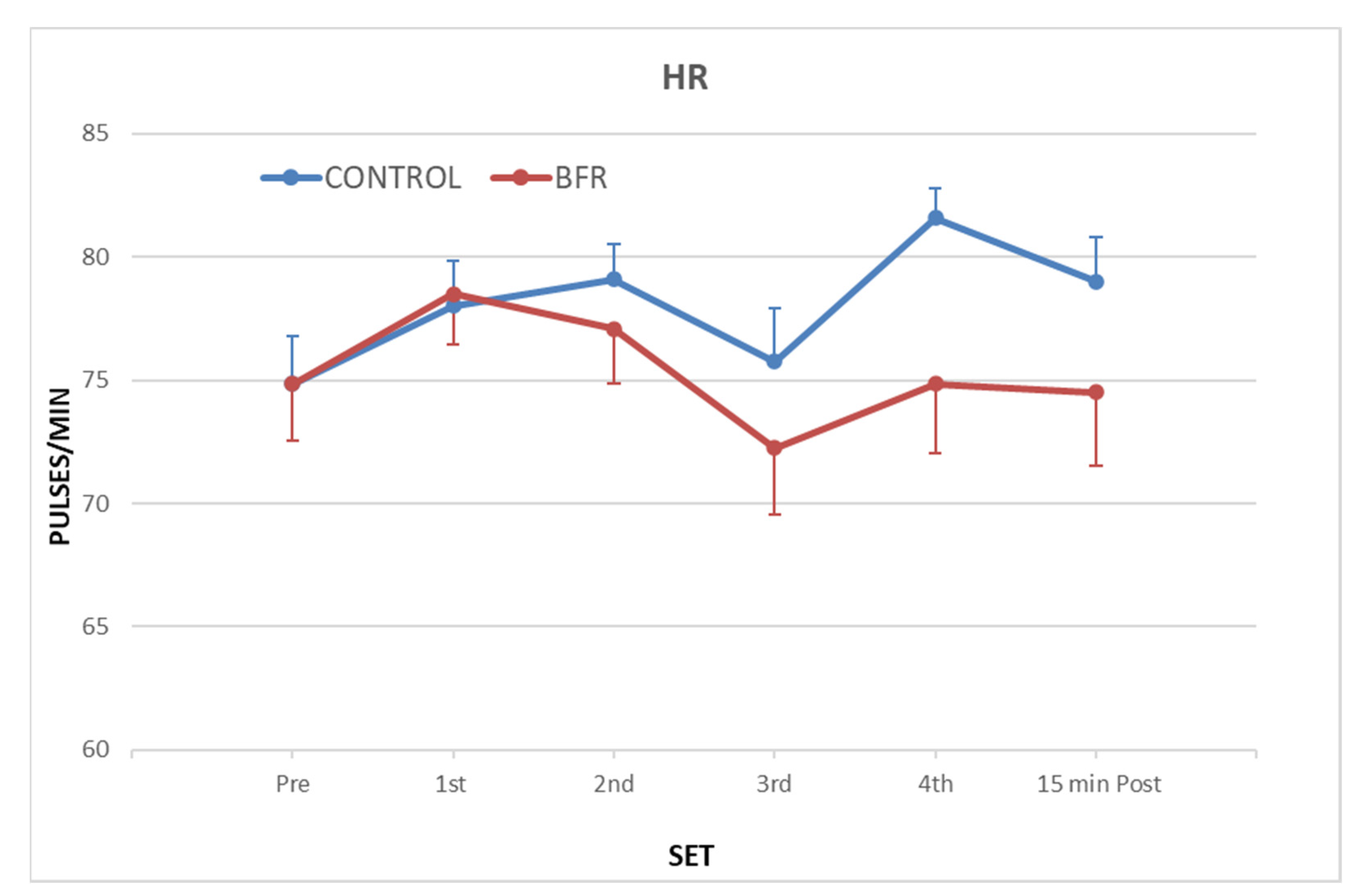
3.1. Heart Rate (HR)
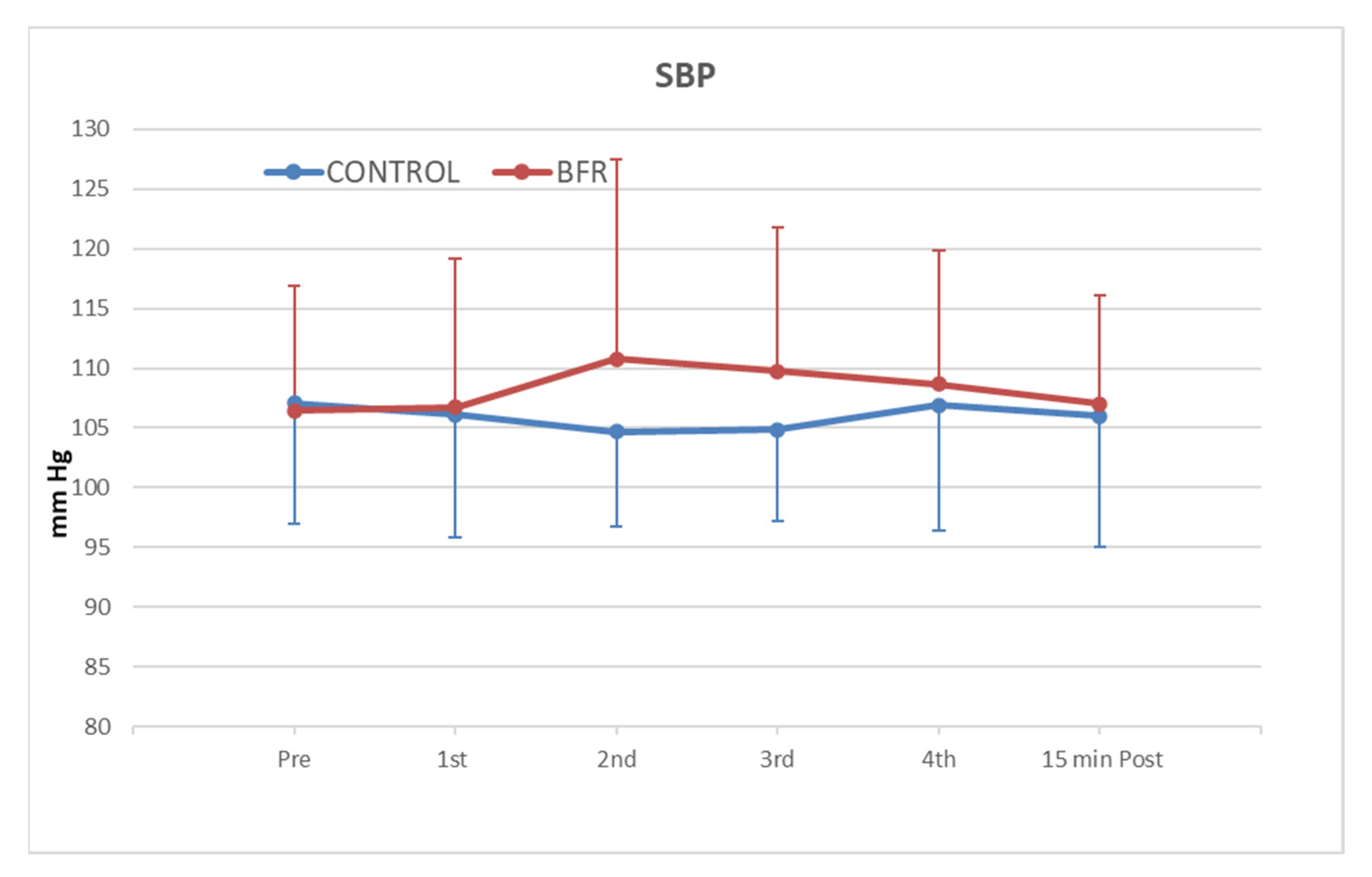
3.2. Systolic Blood Pressure (SBP)
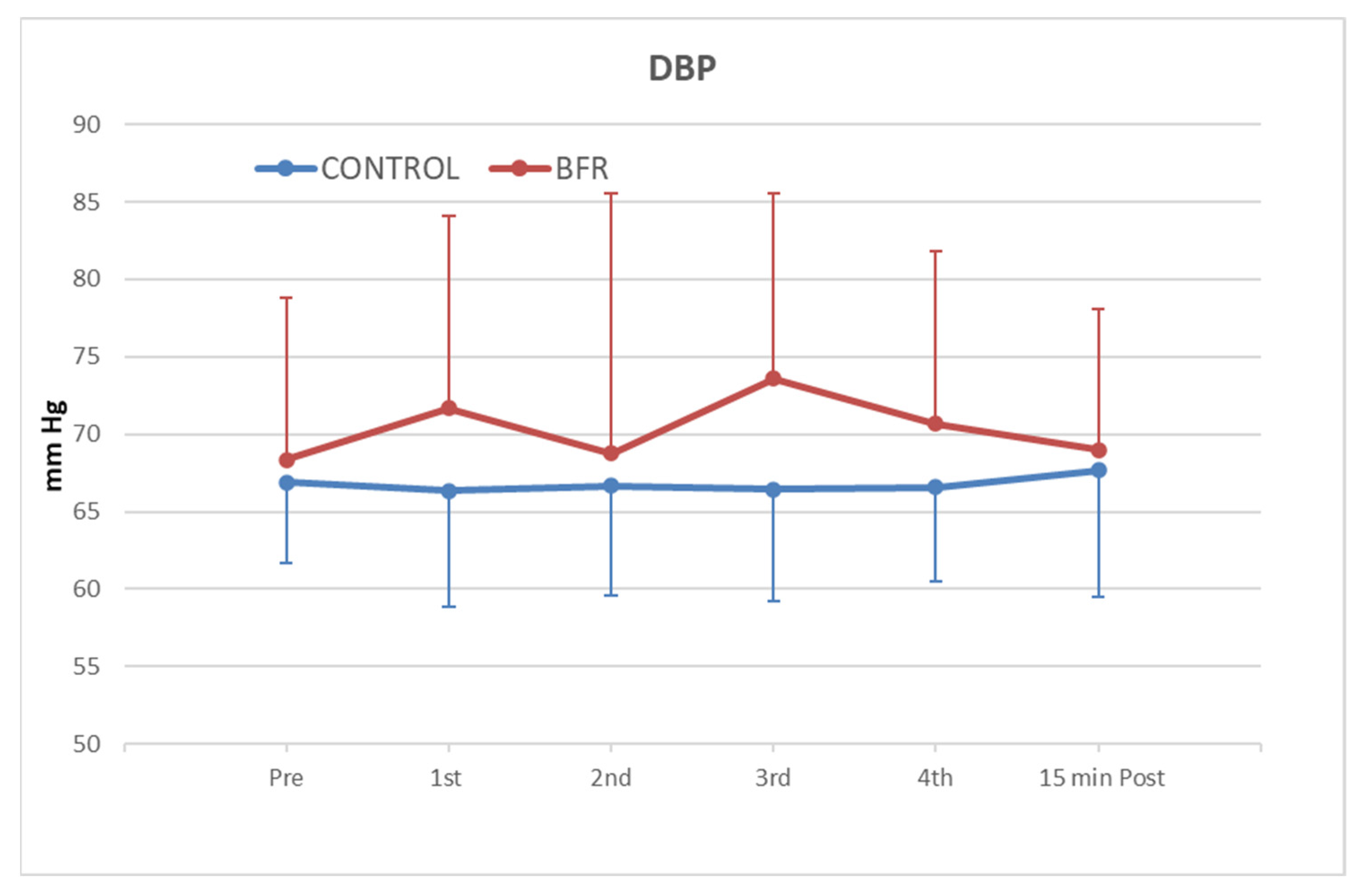
3.3. Diastolic Blood Pressure (DBP)
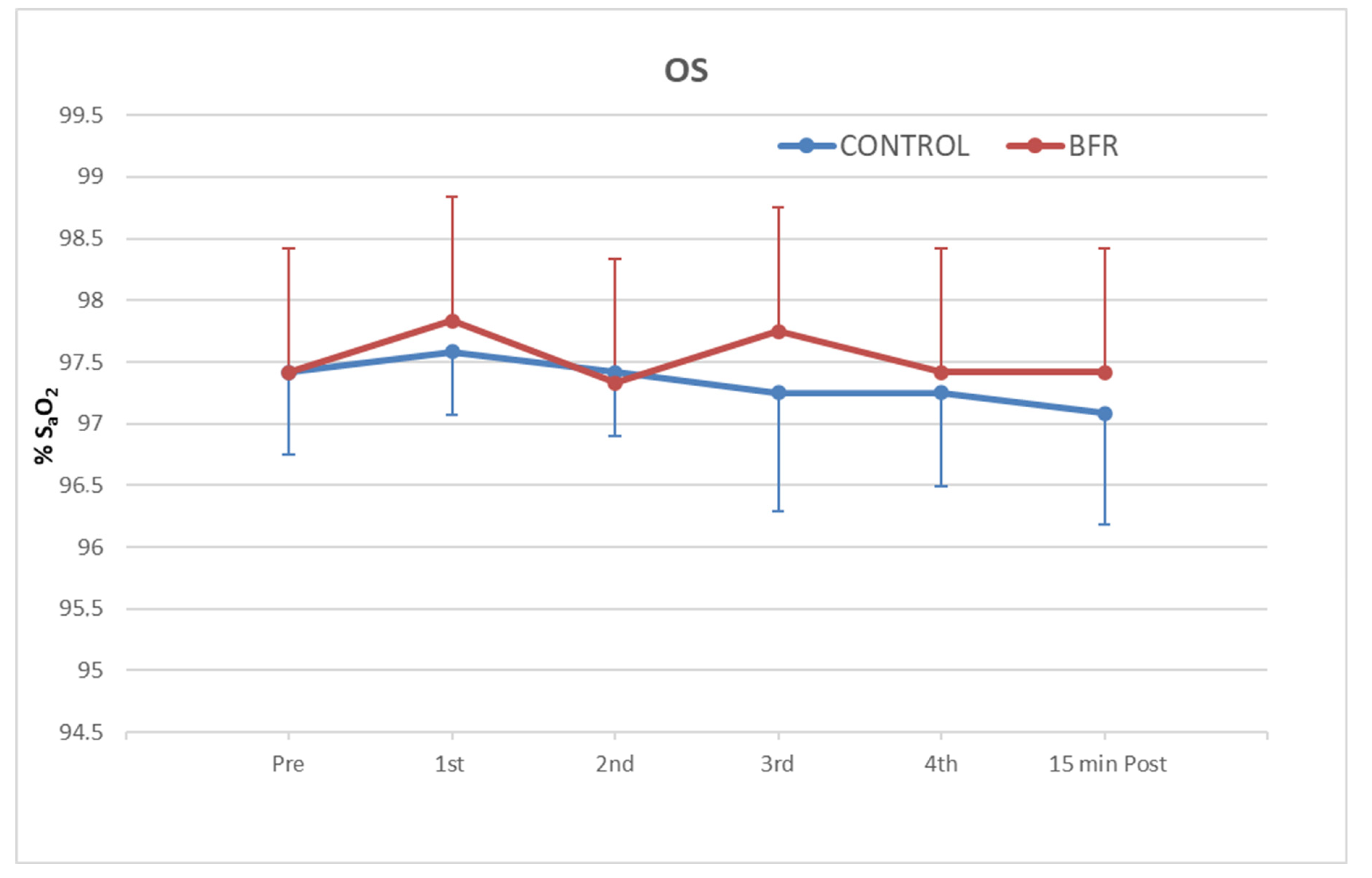
3.4. Oxygen Saturation (SpO2)
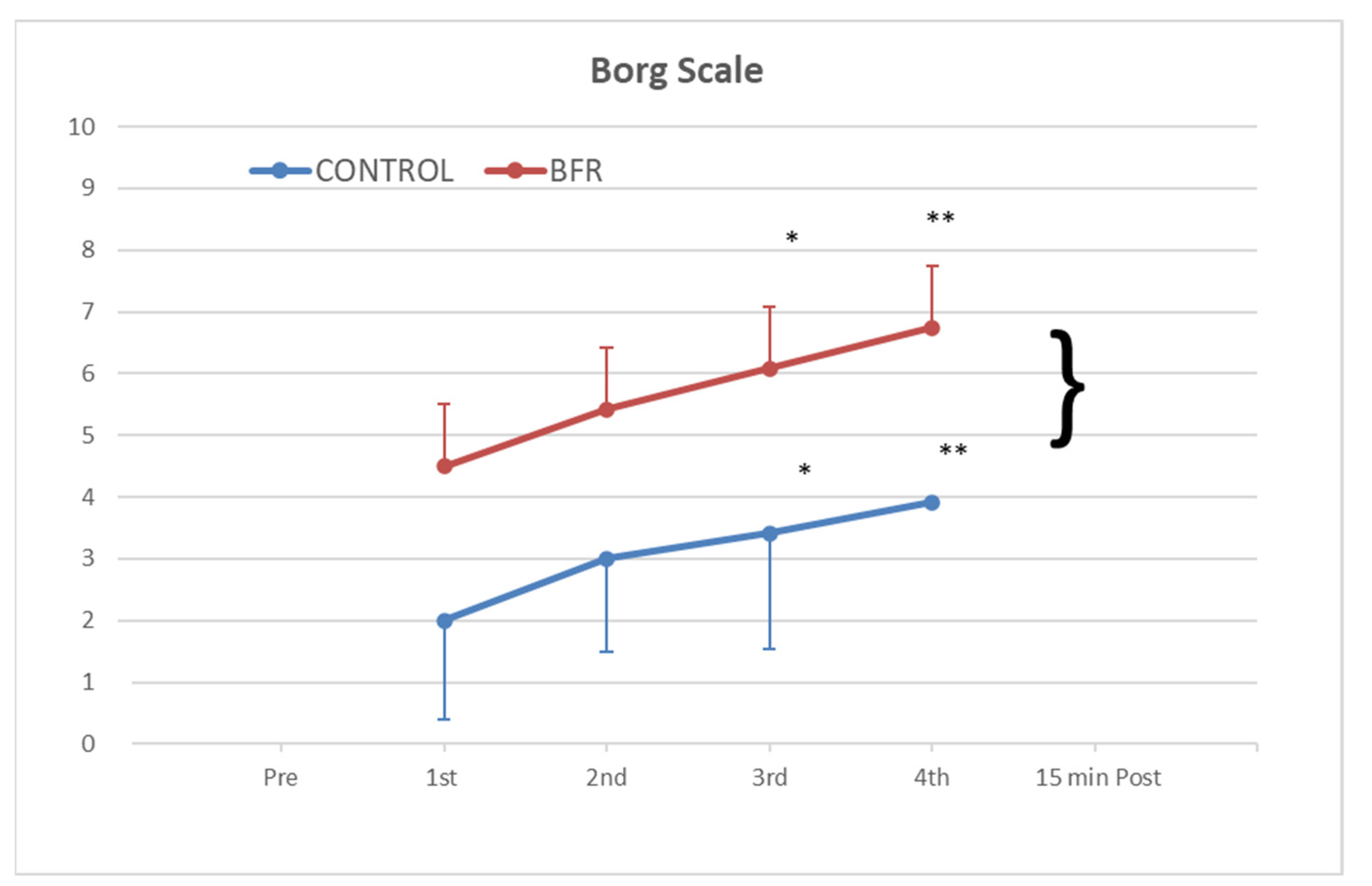
3.5. Rating of Perceived Exertion with the Borg Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 5 October 2022).
- Hughes, L.; Paton, B.; Rosenblatt, B.; Gissane, C.; Patterson, S. Blood flow restriction training in clinical musculoskeletal rehabilitation: A systematic review and meta-analysis. Br. J. Sport. Med. 2017, 51, 1003–1011. [Google Scholar] [CrossRef]
- Neto, G.R.; Sousa, M.S.C.; Silva, G.V.C.E.; Gil, A.L.S.; Salles, B.F.; Novaes, J.S. Acute resistance exercise with blood flow restriction effects on heart rate, double product, oxygen saturation and perceived exertion. Clin. Physiol. Funct. Imaging 2016, 36, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.D.; Hughes, L.; Warmington, S.; Burr, J.; Scott, B.; Owens, J.; Abe, T.; Nielsen, J.; Libardi, C.A.; Laurentino, G.; et al. Blood Flow Restriction Exercise position stand: Considerations of Methodology, Application, and Safety. Front. Physiol. 2019, 10, 1–15. [Google Scholar] [CrossRef]
- Vanwye, W.R.; Weatherholt, A.M.; Mikesky, A.E. Blood Flow Restriction Training: Implementation into Clinical Practice. Int. J. Exerc. Sci. 2017, 10, 649–654. [Google Scholar] [PubMed]
- Wortman, R.J.; Brown, S.M.; Savage-Elliott, I.; Finley, Z.J.; Mulcahey, M.K. Blood Flow Restriction Training for Athletes: A Systematic Review. Am. J. Sport. Med. 2020, 49, 1938–1944. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.L.V.; Sardeli, A.V.; De Souza, G.V.; Bonganha, V.; Santos, L.D.C.; Castro, A.; Cavaglieri, C.R.; Chacon-Mikahil, M.P.T. Cardiac autonomic and haemodynamic recovery after a single session of aerobic exercise with and without blood flow restriction in older adults. J. Sport. Sci. 2017, 35, 2412–2420. [Google Scholar] [CrossRef]
- Shimizu, R.; Hotta, K.; Yamamoto, S.; Matsumoto, T.; Kamiya, K.; Kato, M.; Hamazaki, N.; Kamekawa, D.; Akiyama, A.; Kamada, Y.; et al. Low-intensity resistance training with blood flow restriction improves vascular endothelial function and peripheral blood circulation in healthy elderly people. Eur. J. Appl. Physiol. 2016, 116, 749–757. [Google Scholar] [CrossRef]
- Bocalini, D.S.; Olher, R.D.R.V.; Bacurau, R.F.; Junior, A.F.; Junior, F.L.P.; Navarro, F.; Simoes, H.G.; Araujo, R.; de Moraes, M.R.; Rodriguez, D. Isometric handgrip does not elicit cardiovascular overload or post-exercise hypotension in hypertensive older women. Clin. Interv. Aging 2013, 8, 649–655. [Google Scholar] [CrossRef]
- Pinto, R.R.; Karabulut, M.; Poton, R.; Polito, M.D. Acute resistance exercise with blood flow restriction in elderly hypertensive women: Haemodynamic, rating of perceived exertion and blood lactate. Clin. Physiol. Funct. Imaging 2018, 38, 17–24. [Google Scholar] [CrossRef]
- Biazon, T.M.P.C.; Ugrinowitsch, C.; Soligon, S.D.; Oliveira, R.M.; Bergamasco, J.G.; Borghi-Silva, A.; Libardi, C.A. The Association between Muscle Deoxygenation and Muscle Hypertrophy to Blood Flow Restricted Training Performed at High and Low Loads. Front. Physiol. 2019, 10, 446. [Google Scholar] [CrossRef]
- Curran, M.T.; Bedi, A.; Mendias, C.L.; Wojtys, E.M.; Kujawa, M.V.; Palmieri-Smith, R.M. Blood Flow Restriction Training Applied with High-Intensity Exercise Does Not Improve Quadriceps Muscle Function after Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial. Am. J. Sport. Med. 2020, 48, 825–837. [Google Scholar] [CrossRef] [PubMed]
- Counts, B.R.; Dankel, S.J.; Barnett, B.E.; Kim, D.; Mouser, J.G.; Allen, K.M.; Thiebaud, R.S.; Abe, T.; Bemben, M.G.; Loenneke, J.P. Influence of relative blood flow restriction pressure on muscle activation and muscle adaptation. Muscle Nerve 2016, 53, 438–445. [Google Scholar] [CrossRef]
- Abe, T.; Fujita, S.; Nakajima, T.; Sakamaki, M.; Ozaki, H.; Ogasawara, R.; Sugaya, M.; Kudo, M.; Kurano, M.; Yasuda, T.; et al. Effects of Low-Intensity Cycle Training with Restricted Leg Blood Flow on Thigh Muscle Volume and VO2MAX in Young Men. J. Sport. Sci. Med. 2010, 9, 452–458. [Google Scholar]
- Araújo, J.P.; Neto, G.R.; Loenneke, J.P.; Bemben, M.G.; Laurentino, G.C.; Batista, G.R.; Silva, J.C.G.; Freitas, E.; Sousa, M.S.C. The effects of water-based exercise in combination with blood flow restriction on strength and functional capacity in post-menopausal women. Age 2015, 37, 110. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, M.; Conway, L.; Warmington, S.A. Blood flow restriction walking and physical function in older adults: A randomized control trial. J. Sci. Med. Sport 2017, 20, 1041–1046. [Google Scholar] [CrossRef]
- Barbalho, M.; Rocha, A.C.; Seus, T.L.; Raiol, R.; Del Vecchio, F.B.; Coswig, V.S. Addition of blood flow restriction to passive mobilization reduces the rate of muscle wasting in elderly patients in the intensive care unit: A within-patient randomized trial. Clin. Rehabil. 2019, 33, 233–240. [Google Scholar] [CrossRef]
- Jeffries, O.; Waldron, M.; Pattison, J.R.; Patterson, S. Enhanced Local Skeletal Muscle Oxidative Capacity and Microvascular Blood Flow following 7-Day Ischemic Preconditioning in Healthy Humans. Front. Physiol. 2018, 9, 463. [Google Scholar] [CrossRef]
- De Freitas, M.C.; Gerosa-Neto, J.; Zanchi, N.E.; Lira, F.S.; Rossi, F.E. Role of metabolic stress for enhancing muscle adaptations: Practical applications. World J. Methodol. 2017, 7, 46–54. [Google Scholar] [CrossRef]
- Pearson, S.J.; Hussain, S.R. A Review on the Mechanisms of Blood-Flow Restriction Resistance Training-Induced Muscle Hypertrophy. Sport. Med. 2015, 45, 187–200. [Google Scholar] [CrossRef]
- Soucek, M.; Frana, P.; Kara, T.; Sitar, J.; Halamek, J.; Jurak, P.; Rihacek, I.; Spinarova, L.; Oral, I. The Effect of Short-term Isometric Muscle Contraction and the Valsalva Maneuver on Systemic and Pulmonary Hemodynamics in Patients with Severe Heart Failure. Clin. Cardiol. 2009, 32, E31–E38. [Google Scholar] [CrossRef]
- Hartog, R.; Bolignano, D.; Sijbrands, E.; Pucci, G.; Mattace-Raso, F. Short-term vascular hemodynamic responses to isometric exercise in young adults and in the elderly. Clin. Interv. Aging 2018, 13, 509–514. [Google Scholar] [CrossRef]
- Perry, B.G.; De Hamel, T.; Thomas, K.N.; Wilson, L.C.; Gibbons, T.D.; Cotter, J.D. Cerebrovascular haemodynamics during isometric resistance exercise with and without the Valsalva manoeuvre. Eur. J. Appl. Physiol. 2020, 120, 467–479. [Google Scholar] [CrossRef]
- Jin, Y.Z.; Yan, S.; Yuan, W.X. Effect of isometric handgrip training on resting blood pressure in adults: A meta-analysis of randomized controlled trials. J. Sport. Med. Phys. Fit. 2017, 57, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Loaiza-Betancur, A.F.; Chulvi-Medrano, I. Is Low-Intensity Isometric Handgrip Exercise an Efficient Alternative in Lifestyle Blood Pressure Management? A Systematic Review. Sport. Health 2020, 12, 470–477. [Google Scholar] [CrossRef]
- Farah, B.Q.; Germano-Soares, A.H.; Rodrigues, S.L.C.; Santos, C.X.; Barbosa, S.S.; Vianna, L.C.; Cornelissen, V.A.; Ritti-Dias, R.M. Acute and Chronic Effects of Isometric Handgrip Exercise on Cardiovascular Variables in Hypertensive Patients: A Systematic Review. Sports 2017, 5, 55. [Google Scholar] [CrossRef]
- Maga, M.; Schönborn, M.; Wachsmann-Maga, A.; Śliwka, A.; Krężel, J.; Włodarczyk, A.; Olszewska, M.; Nowobilski, R. Stimulation of the Vascular Endothelium and Angiogenesis by Blood-Flow-Restricted Exercise. Int. J. Environ. Res. Public Health 2022, 19, 15859. [Google Scholar] [CrossRef]
- Horiuchi, M.; Okita, K. Blood Flow Restricted Exercise and Vascular Function. Int. J. Vasc. Med. 2012, 2012, 543218. [Google Scholar] [CrossRef] [PubMed]
- Larkin, K.A.; Macneil, R.G.; Dirain, M.; Sandesara, B.; Manini, T.M.; Buford, T.W. Blood Flow Restriction Enhances Post–Resistance Exercise Angiogenic Gene Expression. Med. Sci. Sport. Exerc. 2012, 44, 2077–2083. [Google Scholar] [CrossRef]
- Ferguson, R.A.; Hunt, J.E.A.; Lewis, M.P.; Martin, N.R.W.; Player, D.J.; Stangier, C.; Taylor, C.W.; Turner, M.C. The Acute An-giogenic Signalling Response to Low-Load Resistance Exercise with Blood Flow Restriction. Eur. J. Sport Sci. 2018, 18, 397–406. [Google Scholar] [CrossRef]
- Montgomery, R.; Paterson, A.; Williamson, C.; Florida-James, G.; Ross, M.D. Blood Flow Restriction Exercise Attenuates the Exercise-Induced Endothelial Progenitor Cell Response in Healthy, Young Men. Front. Physiol. 2019, 10, 447. [Google Scholar] [CrossRef] [PubMed]
- Hudlicka, O.; Brown, M.D. Adaptation of Skeletal Muscle Microvasculature to Increased or Decreased Blood Flow: Role of Shear Stress, Nitric Oxide and Vascular Endothelial Growth Factor. J. Vasc. Res. 2009, 46, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.M.; Sobrinho, M.F.L.; Ritti-Dias, R.M.; Sobral, B.P.S.V.; Pirauá, A.L.T.; De Oliveira, L.M.F.T.; Farah, B.Q. Cardiovascular responses after isometric handgrip exercise at different intensities in healthy men. J. Phys. Educ. 2019, 30, 3020. [Google Scholar] [CrossRef]
- Araújo, C.G.S.D.; Duarte, C.V.; Gonçalves, F.D.A.; Medeiros, H.; Lemos, F.A.; Gouvêa, A.L. Hemodynamic responses to an isometric handgrip training protocol. Arq. Bras. Cardiol. 2011, 97, 413–419. [Google Scholar] [CrossRef]
- Cayot, T.E.; Lauver, J.; Silette, C.R.; Scheuermann, B.W. Effects of blood flow restriction duration on muscle activation and microvascular oxygenation during low-volume isometric exercise. Clin. Physiol. Funct. Imaging 2014, 36, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, M.S.; Pereira, R.; de Mesquita, G.N.; Rocha, T.; de Moura Filho, A.G. Influence of Blood Flow Restriction Level on Muscle Fatigue during an Intermittent Isometric Exercise Taken to Failure. Muscle Ligaments Tendons J. 2020, 10, 408. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 27 December 2022).
- American Heart Association. Understanding Blood Pressure Readings. Available online: https://www.heart.org/en/health-topics/high-blood-pressure/understanding-blood-pressure-readings (accessed on 10 January 2023).
- Stergiou, G.S.; Yiannes, N.G.; Rarra, V.C. Validation of the Omron 705 IT oscillometric device for home blood pressure measurement in children and adolescents: The Arsakion School Study. Blood Press. Monit. 2006, 11, 229–234. [Google Scholar] [CrossRef]
- Vera-Cala, L.M.; Orostegui, M.; Valencia-Angel, L.I.; López, N.; Bautista, L.E. Accuracy of the Omron HEM-705 CP for blood pressure measurement in large epidemiologic studies. Arq. Bras. Cardiol. 2011, 96, 393–398. [Google Scholar] [CrossRef]
- Essner, A.; Sjöström, R.; Ahlgren, E.; Lindmark, B. Validity and reliability of Polar® RS800CX heart rate monitor, measuring heart rate in dogs during standing position and at trot on a treadmill. Physiol. Behav. 2013, 114–115, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Louie, A.; Feiner, J.R.; Bickler, P.E.; Rhodes, L.; Bernstein, M.; Lucero, J. Four Types of Pulse Oximeters Accurately Detect Hypoxia during Low Perfusion and Motion. Anesthesiology 2018, 128, 520–530. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sport. Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Williams, N. The Borg Rating of Perceived Exertion (RPE) scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2013. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Perceived Exertion (Borg Rating of Perceived Exertion Scale). Available online: https://www.cdc.gov/physicalactivity/basics/measuring/exertion.htm (accessed on 15 December 2022).
- Poton, R.; Polito, M.D. Hemodynamic response to resistance exercise with and without blood flow restriction in healthy subjects. Clin. Physiol. Funct. Imaging 2014, 36, 231–236. [Google Scholar] [CrossRef]
- Vieira, P.J.; Chiappa, G.R.; Umpierre, D.; Stein, R.; Ribeiro, J.P. Hemodynamic Responses to Resistance Exercise with Restricted Blood Flow in Young and Older Men. J. Strength Cond. Res. 2013, 27, 2288–2294. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.; Vicil, F. Post-exercise aortic hemodynamic responses to low-intensity resistance exercise with and without vascular occlusion. Scand. J. Med. Sci. Sport. 2011, 21, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Credeur, D.P.; Jones, R.; Stanford, D.; Stoner, L.; McCoy, S.; Jessee, M. Central cardiovascular hemodynamic response to unilateral handgrip exercise with blood flow restriction. Eur. J. Appl. Physiol. 2019, 119, 2255–2263. [Google Scholar] [CrossRef] [PubMed]
- Rossow, L.M.; Fahs, C.A.; Loenneke, J.P.; Thiebaud, R.S.; Sherk, V.D.; Abe, T.; Bemben, M.G. Cardiovascular and perceptual responses to blood-flow-restricted resistance exercise with differing restrictive cuffs. Clin. Physiol. Funct. Imaging 2012, 32, 331–337. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Thiebaud, R.S.; Fahs, C.A.; Rossow, L.M.; Abe, T.; Bemben, M.G. Effect of cuff type on arterial occlusion. Clin. Physiol. Funct. Imaging 2013, 33, 325–327. [Google Scholar] [CrossRef]
- Bonorino, S.L.; Sá, C.A.D.; Corralo, V.D.S.; Olkoski, M.M.; Silva-Grigoletto, M.E.D.; Saretto, C.B.; Resende, A.G.D. Hemodynamic responses to strength exercise with blood flow restriction in small muscle groups. Rev. Bras. Cineantropometria Desempenho Hum. 2019, 21, e56258. [Google Scholar] [CrossRef]
- Spranger, M.D.; Krishnan, A.C.; Levy, P.D.; O’Leary, D.S.; Smith, S.A. Blood flow restriction training and the exercise pressor reflex: A call for concern. Am. J. Physiol. Circ. Physiol. 2015, 309, H1440–H1452. [Google Scholar] [CrossRef]
- Ozaki, H.; Yasuda, T.; Ogasawara, R.; Sakamaki-Sunaga, M.; Naito, H.; Abe, T. Effects of high-intensity and blood flow-restricted low-intensity resistance training on carotid arterial compliance: Role of blood pressure during training sessions. Eur. J. Appl. Physiol. 2012, 113, 167–174. [Google Scholar] [CrossRef]
- Cerqueira, M.S.; Pereira, R.; Rocha, T.; Mesquita, G.; de Paiva Lima, C.R.O.; Raposo, M.C.F.; De Moura Filho, A.G. Time to failure and neuromuscular response to intermittent isometric exercise at different levels of vascular occlusion: A randomized crossover study. Int. J. Appl. Exerc. Physiol. 2017, 6, 55–70. [Google Scholar] [CrossRef]
- Husmann, F.; Mittlmeier, T.; Bruhn, S.; Zschorlich, V.; Behrens, M. Impact of Blood Flow Restriction Exercise on Muscle Fatigue Development and Recovery. Med. Sci. Sport. Exerc. 2018, 50, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Copithorne, D.B.; Rice, C.L. The effect of blood flow occlusion during acute low-intensity isometric elbow flexion exercise. Eur. J. Appl. Physiol. 2019, 119, 587–595. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Mean ± SE |
|---|---|
| Age (years) | 23.27 ± 0.54 |
| BMI (value) | 24.86 ± 1.78 |
| Gender (%) | Women 50% n = 12 |
| Comorbidities | None |
| Medication | None |
| Smokers | n = 2 (former) |
| Baseline | 1st Set | 2nd Set | 3rd Set | 4th Set | 15 min after | |
|---|---|---|---|---|---|---|
| HR pulses/minute (SD) | ||||||
| BFRT * | 74 (8) | 78 (7) | 77 (8) | 72 (9) | 74 (10) | 74(10) |
| Control | 74 (7) | 78 (6) | 79 (5) | 75 (7) | 81 (4) | 79 (6) |
| SBP mmHg (SD) | ||||||
| BFRT | 106.4 (10.5) | 106.8 (12.4) | 110.8 (16.8) | 109.8 (12.0) | 108.7 (11.1) | 107.0 (9.1) |
| Control | 107.1 (10.1) | 106.1 (10.2) | 104.7 (7.9) | 104.8 (7.7) | 106.9 (10.5) | 106.0 (11.0) |
| DBP mmHg (SD) | ||||||
| BFRT | 68.3 (7.1) | 71.7 (6.0) | 68.8 (7.8) | 73.6 (12.2) | 70.7 (6.7) | 69.0 (5.4) |
| Control | 66.9 (5.2) | 66.3 (7.5) | 66.7 (7.1) | 66.4 (7.2) | 66.6 (6.1) | 67.7 (8.2) |
| OS SpO2 (SD) | ||||||
| BFRT | 97.4 (0.8) | 97.8 (0.8) | 97.3 (1.0) | 97.8 (0.5) | 97.4 (0.9) | 97.4 (0.9) |
| Control | 97.4 (0.7) | 97.6 (0.5) | 97.4 (0.5) | 97.3 (1.0) | 97.3 (0.8) | 97.1 (0.9) |
| Borg scale points (SD) | ||||||
| BFRT | - | 4.5 (1.8) | 5.4 (1.8) | 6.1 (2.1) | 6.8 (2.3) ** | - |
| Control * | - | 2.0 (1.4) | 3.0 (1.6) | 3.4 (1.5) | 3.9 (1.9) ** | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filippou, S.; Iakovidis, P.; Lytras, D.; Kasimis, K.; Solomonidou, F.; Kopsidas, C. Hemodynamic Responses to a Handgrip Exercise Session, with and without Blood Flow Restriction, in Healthy Volunteers. Physiologia 2023, 3, 259-271. https://doi.org/10.3390/physiologia3020018
Filippou S, Iakovidis P, Lytras D, Kasimis K, Solomonidou F, Kopsidas C. Hemodynamic Responses to a Handgrip Exercise Session, with and without Blood Flow Restriction, in Healthy Volunteers. Physiologia. 2023; 3(2):259-271. https://doi.org/10.3390/physiologia3020018
Chicago/Turabian StyleFilippou, Spyridoula, Paris Iakovidis, Dimitrios Lytras, Konstantinos Kasimis, Freideriki Solomonidou, and Christos Kopsidas. 2023. "Hemodynamic Responses to a Handgrip Exercise Session, with and without Blood Flow Restriction, in Healthy Volunteers" Physiologia 3, no. 2: 259-271. https://doi.org/10.3390/physiologia3020018