
Retrospective Comparison of Hospital Outcomes among Mechanically Ventilated COVID-19 Patients in ICU Who Received Methylprednisolone or Dexamethasone

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Demographic, Clinical and Laboratory Characteristics
2.3. Outcome Variables
2.4. Ethical Consideration
2.5. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/ (accessed on 16 January 2023).
- Sabetian, G.; Moghadami, M.; Hashemizadeh Fard Haghighi, L.; Shahriarirad, R.; Fallahi, M.J.; Asmarian, N.; Moeini, Y.S. COVID-19 infection among healthcare workers: A cross-sectional study in southwest Iran. Virol. J. 2021, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Søreide, K.; Hallet, J.; Matthews, J.B.; Schnitzbauer, A.A.; Line, P.D.; Lai, P.; Otero, J.; Callegaro, D.; Warner, S.G.; Baxter, N.N. Immediate and long-term impact of the COVID-19 pandemic on delivery of surgical services. J. Br. Surg. 2020, 107, 1250–1261. [Google Scholar] [CrossRef] [PubMed]
- Young, B.; Tan, T.T.; Leo, Y.S. The place for remdesivir in COVID-19 treatment. Lancet Infect. Dis. 2021, 21, 20–21. [Google Scholar] [CrossRef] [PubMed]
- Vetter, P.; Kaiser, L.; Calmy, A.; Agoritsas, T.; Huttner, A. Dexamethasone and remdesivir: Finding method in the COVID-19 madness. Lancet Microbe 2020, 1, e309–e310. [Google Scholar] [CrossRef]
- Shahriarirad, R.; Khodamoradi, Z.; Erfani, A.; Hosseinpour, H.; Ranjbar, K.; Emami, Y.; Mirahmadizadeh, A.; Lotfi, M.; Shirazi Yeganeh, B.; Dorrani Nejad, A. Epidemiological and clinical features of 2019 novel coronavirus diseases (COVID-19) in the South of Iran. BMC Infect. Dis. 2020, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arabi, Y.M.; Mandourah, Y.; Al-Hameed, F.; Sindi, A.A.; Almekhlafi, G.A.; Hussein, M.A.; Jose, J.; Pinto, R.; Al-Omari, A.; Kharaba, A. Corticosteroid therapy for critically ill patients with Middle East respiratory syndrome. Am. J. Respir. Crit. Care Med. 2018, 197, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Stockman, L.J.; Bellamy, R.; Garner, P. SARS: Systematic review of treatment effects. PLoS Med. 2006, 3, e343. [Google Scholar] [CrossRef] [Green Version]
- Duman, I.; Celik, J.B.; Iyisoy, M.S.; Degirmencioglu, S.; Korkmaz, A.; Duman, A. Evaluation of personalized methylprednisolone therapy in critically ill COVID-19 patients: An observational comparative study using real-life data. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 4497–4508. [Google Scholar]
- Sterne, J.A.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; Cavalcanti, A.B. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: A meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar]
- Ranjbar, K.; Moghadami, M.; Mirahmadizadeh, A.; Fallahi, M.J.; Khaloo, V.; Shahriarirad, R.; Erfani, A.; Khodamoradi, Z.; Gholampoor Saadi, M.H. Methylprednisolone or dexamethasone, which one is superior corticosteroid in the treatment of hospitalized COVID-19 patients: A triple-blinded randomized controlled trial. BMC Infect. Dis. 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatima, S.A.; Asif, M.; Khan, K.A.; Siddique, N.; Khan, A.Z. Comparison of efficacy of dexamethasone and methylprednisolone in moderate to severe covid 19 disease. Ann. Med. Surg. 2020, 60, 413–416. [Google Scholar] [CrossRef]
- Du Plessis, E.; Lalla, U.; Allwood, B.; Louw, E.; Nortje, A.; Parker, A.; Taljaard, J.; Ayele, B.; Nyasulu, P.; Koegelenberg, C. Corticosteroids in critical COVID-19: Are all corticosteroids equal? South Afr. Med. J. 2021, 111, 550–553. [Google Scholar]
- Ko, J.J.; Wu, C.; Mehta, N.; Wald-Dickler, N.; Yang, W.; Qiao, R. A comparison of methylprednisolone and dexamethasone in intensive care patients with COVID-19. J. Intensive Care Med. 2021, 36, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Saeed, M.A.M.; Mohamed, A.H.; Owaynat, A.H. Comparison between methylprednisolone infusion and dexamethasone in COVID-19 ARDS mechanically ventilated patients. Egypt. J. Intern. Med. 2022, 34, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Analysis, A.P. Methylprednisolone Achieves Greater Concentrations in the Lung Than Prednisolone. Am. Rev. Respir Dis. 1991, 144, 586–592. [Google Scholar]
- Braude, A.; Rebuck, A. Prednisone and methylprednisolone disposition in the lung. Lancet 1983, 322, 995–997. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-reactive protein and clinical outcomes in patients with COVID-19. Eur. Heart J. 2021, 42, 2270–2279. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Nguy, V.; Aphinyanaphongs, Y.; Newman, J.D.; Xia, Y.; Reynolds, H.R.; Hochman, J.S.; Fishman, G.I.; Berger, J.S. Multiple biomarker approach to risk stratification in COVID-19. Circulation 2021, 143, 1338–1340. [Google Scholar] [CrossRef]
- Alfano, G.; Ferrari, A.; Fontana, F.; Mori, G.; Ligabue, G.; Giovanella, S.; Magistroni, R.; Meschiari, M.; Franceschini, E.; Menozzi, M. Twenty-four-hour serum creatinine variation is associated with poor outcome in the novel coronavirus disease 2019 (COVID-19) patients. Kidney Res. Clin. Pract. 2021, 40, 231. [Google Scholar] [CrossRef] [PubMed]
- Lameire, N.; Van Biesen, W.; Hoste, E.; Vanholder, R. The prevention of acute kidney injury: An in-depth narrative review Part 1: Volume resuscitation and avoidance of drug- and nephrotoxin-induced AKI. Clin. Kidney J. 2008, 1, 392–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Group RECOVERY Collaborative. Dexamethasone in hospitalized patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Bahl, A.; Johnson, S.; Chen, N.-W. Timing of corticosteroids impacts mortality in hospitalized COVID-19 patients. Intern. Emerg. Med. 2021, 16, 1593–1603. [Google Scholar] [CrossRef] [PubMed]
- Fadel, R.; Morrison, A.R.; Vahia, A.; Smith, Z.R.; Chaudhry, Z.; Bhargava, P.; Miller, J.; Kenney, R.M.; Alangaden, G.; Ramesh, M.S. Early short-course corticosteroids in hospitalized patients with COVID-19. Clin. Infect. Dis. 2020, 71, 2114–2120. [Google Scholar] [CrossRef]
- Lee, N.; Chan, K.C.A.; Hui, D.S.; Ng, E.K.O.; Wu, A.; Chiu, R.W.K.; Wong, V.W.S.; Chan, P.K.S.; Wong, K.T.; Wong, E.; et al. Effects of early corticosteroid treatment on plasma SARS-associated Coronavirus RNA concentrations in adult patients. J. Clin. Virol. 2004, 31, 304–309. [Google Scholar] [CrossRef]
- Ni, Y.-N.; Chen, G.; Sun, J.; Liang, B.-M.; Liang, Z.-A. The effect of corticosteroids on mortality of patients with influenza pneumonia: A systematic review and meta-analysis. Crit. Care 2019, 23, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Immunosuppression in sepsis: A novel understanding of the disorder and a new therapeutic approach. Lancet Infect. Dis. 2013, 13, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Bajaj, D.; Gupta, M.; Manek, G.; Manek, G.; Hu, K.; Boregowda, U. Dexamethasone versus Methylprednisolone in Hospitalized COVID-19 Patients: A Systematic Review and Meta-Analysis. Int. J. Crit. Care Emerg. Med. 2021, 7, 128. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Total n = 121 (100%) | Methylprednisolone n = 53 (43.8%) | Dexamethasone n = 68 (56.2%) | p Value |
|---|---|---|---|---|
| Age, median (IQR) | 71.0 (59.0, 78.0) | 70.0 (56.0, 80.0) | 71.5 (62.0, 78.0) | 0.644 |
| Sex, n (%) | ||||
| Female | 36 (29.8) | 17 (32.1) | 19 (27.9) | 0.769 |
| Male | 85 (70.2) | 36 (67.9) | 49 (72.1) | |
| Race, n (%) | 0.012 | |||
| Hispanic | 96 (79.3) | 36 (67.9) | 60 (88.2) | |
| Non-Hispanic | 25 (20.7) | 17 (32.1) | 8 (11.8) | |
| Days on steroids, median (IQR) | 12.0 (7.0, 18.0) | 9.0 (6.0, 13.0) | 15.5 (9.0, 21.5) | <0.001 |
| Hydroxychloroquine, n (%) | 16 (13.2) | 16 (30.2) | 0 (0) | --- |
| Tocilizumab, n (%) | 15 (12.4) | 11 (20.8) | 4 (5.9) | 0.029 |
| RBS in mg/dL, mean (SD) | 192.5 (96.7) | 174.0 (95.6) | 206.3 (95.9) | 0.074 |
| Insulin in µg/dL, mean (SD) | 5.6 (5.0) | 4.7 (4.1) | 6.4 (5.5) | 0.094 |
| CRP in mg/dL, mean (SD) | 154.4 (346.3) | 193.8 (517.6) | 123.8 (72.5) | 0.338 |
| Ferritin in mg/dL, mean (SD) | 2010.8 (7742.1) | 3278.6 (11,407.1) | 996.5 (1612.1) | 0.158 |
| D-dimer in µg/mL, mean (SD) | 4.3 (6.3) | 4.6 (6.4) | 4.0 (6.3) | 0.633 |
| Lactic acid in mg/dL, mean (SD) | 2.5 (2.8) | 2.7 (3.6) | 2.4 (2.0) | 0.570 |
| PO2 in mm Hg, mean (SD) | 91.8 (53.6) | 99.7 (60.2) | 85.5 (47.3) | 0.162 |
| SpO2 mm Hg, mean (SD) | 90.3 (9.8) | 91.5 (8.3) | 89.3 (10.8) | 0.202 |
| Bicarbonate mEq/L, mean (SD) | 24.4 (4.0) | 23.9 (3.9) | 24.7 (4.0) | 0.269 |
| Hematocrit in %, mean (SD) | 37.9 (5.9) | 37.7 (5.4) | 38.0 (6.3) | 0.795 |
| Hemoglobin in gm/dL, mean (SD) | 12.4 (2.0) | 12.4 (2.0) | 12.5 (2.1) | 0.917 |
| WBC in 103 cells/µL, mean (SD) | 11.5 (6.0) | 11.3 (7.1) | 11.6 (5.1) | 0.816 |
| NLR, mean (SD) | 13.5 (11.5) | 14.2 (13.8) | 12.9 (9.3) | 0.544 |
| Platelet count in 103 cells/µL, mean (SD) | 233.5 (102.2) | 215.9 (103.0) | 247.3 (100.1) | 0.096 |
| Sodium in mEq/L, mean (SD) | 137.8 (4.0) | 138.3 (4.5) | 137.5 (3.6) | 0.256 |
| Potassium mEq/L, mean (SD) | 4.2 (0.5) | 4.2 (0.5) | 4.3 (0.5) | 0.727 |
| Calcium in mg/dL, mean (SD) | 8.4 (0.7) | 8.1 (0.7) | 8.6 (0.7) | 0.002 |
| Chloride in mEq/L, mean (SD) | 104.9 (4.8) | 105.5 (5.2) | 104.5 (4.4) | 0.248 |
| Creatinine in mg/dL, mean (SD) | 1.6 (1.7) | 2.0 (2.4) | 1.2 (0.9) | 0.041 |
| Bilirubin in mg/dL, mean (SD) | 0.9 (2.3) | 0.7 (0.9) | 1.0 (3.0) | 0.535 |
| Total protein in mg/dL, mean (SD) | 7.0 (0.7) | 7.0 (0.8) | 7.1 (0.6) | 0.931 |
| Albumin to globulin ratio, mean (SD) | 8.4 (3.3) | 8.6 (3.3) | 8.3 (3.4) | 0.606 |
| Alkaline phosphatase in mg/dL, mean (SD) | 96.7 (63.8) | 87.0 (42.6) | 103.4 (74.8) | 0.141 |
| SGPT in mg/dL, mean (SD) | 112.8 (364.4) | 170.4 (553.4) | 72.3 (99.6) | 0.235 |
| BMI in kg/m2, mean (SD) | 28.7 (10.3) | 26.5 (12.1) | 30.2 (8.7) | 0.083 |
| Admission quarter | ||||
| April–June | 36 (29.8) | 34 (64.2) | 2 (2.9) | <0.001 |
| July–September | 38 (31.4) | 18 (34.0) | 20 (29.4) | |
| October–December | 47 (38.8) | 1 (1.9) | 46 (67.6) | |
| APR Severity | ||||
| 1 | 0 (0) | 0 (0) | 0 (0) | |
| 2 | 3 (2.5) | 3 (5.7) | 0 (0) | 0.042 |
| 3 | 19 (15.7) | 5 (9.4) | 14 (20.6) | |
| 4 | 99 (81.8) | 45 (84.9) | 54 (79.4) | |
| APR Mortality Risk | ||||
| 1 | 2 (1.7) | 2 (3.8) | 0 (0) | 0.044 |
| 2 | 2 (1.7) | 2 (3.8) | 0 (0) | |
| 3 | 20 (16.5) | 5 (9.4) | 15 (22.1) | |
| 4 | 97 (80.2) | 44 (83.0) | 53 (77.9) | |
| Charlson comorbidity index, n (%) | ||||
| 0 | 28 (23.1) | 13 (24.5) | 15 (22.1) | 0.809 |
| 1 | 45 (37.2) | 18 (34.0) | 27 (39.7) | |
| ≥2 | 48 (39.7) | 22 (41.5) | 26 (38.2) | |
| Steroid administration to death in hours, mean (SD) | 398.5 (249.3) | 321.4 (217.3) | 451.4 (257.9) | 0.014 |
| Frailty, n (%) | 0.104 | |||
| Non-frail | 15 (12.4) | 5 (9.4) | 10 (14.7) | |
| Pre-frail/Frail | 106 (87.6) | 48 (90.6) | 58 (85.3) | |
| Admission to steroid administration in hours, mean (SD) | 18.9 (31.9) | 32.3 (41.2) | 8.4 (15.8) | <0.001 |
| Admitted to ICU, n (%) | 111 (91.7%) | 50 (94.3%) | 61 (89.7%) | 0.501 |
| Admission to ICU admission in hours, mean (SD) | 221.6 (316.4) | 90.7 (195.0) | 429.5 (363.8) | 0.002 |
| Disposition status, n (%) | 0.548 | |||
| Home | 15 (12.4) | 8 (15.1) | 7 (10.3) | |
| Other than home | 20 (16.5) | 10 (18.9) | 10 (14.7) | |
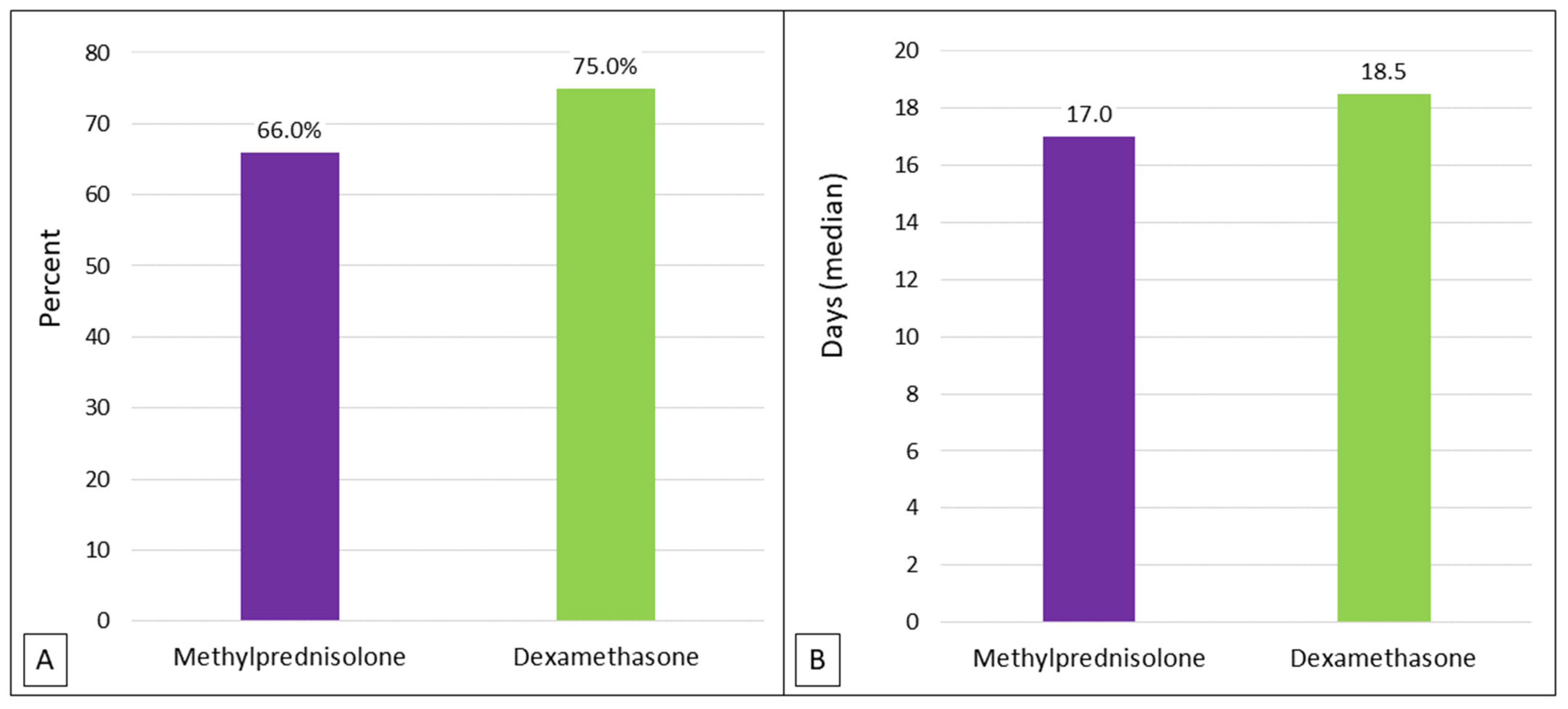
| Expired | 86 (71.1) | 35 (66.0) | 51 (75.0) | |
| In-hospital mortality, n (%) | 86 (71.1) | 35 (66.0) | 51 (75.0) | 0.381 |
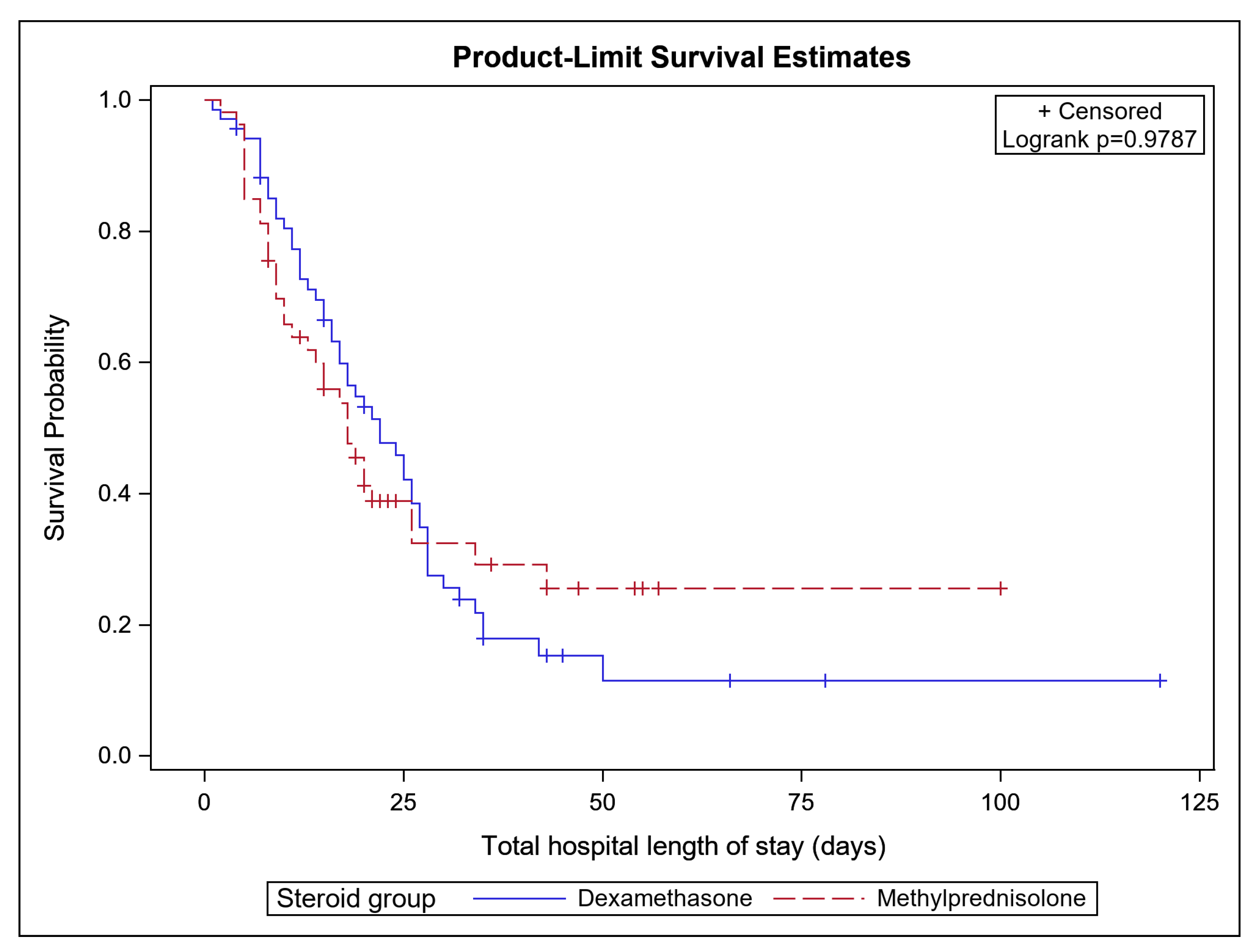
| Length of stay in days, median (IQR) | 18.0 (9.0, 27.0) | 17.0 (8.0, 23.0) | 18.5 (11.0, 28.0) | 0.307 |
| ICU length of stay in days, median (IQR) | 10.0 (4.0, 17.0) | 8.0 (4.0, 14.0) | 10.0 (4.0, 20.0) | 0.234 |
| APACHE III Score, mean (SD) | 75.7 (33.7) | 71.7 (26.8) | 90.2 (53.6) | 0.492 |
| APS Score, mean (SD) | 64.3 (32.5) | 60.2 (25.8) | 79.0 (51.0) | 0.465 |
| Days on ventilator, median (IQR) | 11.0 (6.0, 19.0) | 11.5 (5.5, 22.0) | 10.0 (6.0, 15.0) | 0.175 |
| PaO2/FiO2 ratio, median (IQR) | 194.1 (178.7, 204.7) | 197.3 (172.1, 211.1) | 182.1 (169.7, 198.3) | 0.452 |
| Variables | HR (95% CI) | p Value |
|---|---|---|
| Steroids | ||
| Dexamethasone | Reference | 0.137 |
| methylprednisone | 0.64 (0.35–3.17) | |
| Age | 1.02 (1.01–1.03) | 0.024 |
| Sex | ||
| Female | Reference | 0.072 |
| Male | 0.62 (0.37–1.04) | |
| Race | ||
| Hispanic | Reference | 0.937 |
| Non-Hispanic | 0.97 (0.52–1.81) | |
| Days on steroid | 0.87 (0.83–0.92) | <0.001 |
| CRP | 1.44 (1.06–1.97) | 0.018 |
| D-dimer | 1.78 (0.62–1.98) | 0.128 |
| Calcium | 0.05 (0.00–1.99) | 0.113 |
| Creatinine | 1.72 (1.10–2.69) | 0.016 |
| PO2 | 0.98 (0.53–1.85) | 0.972 |
| SpO2 | 0.25 (0.04–1.49) | 0.130 |
| Tocilizumab | 0.35 (0.14–0.86) | 0.021 |
| Admission to steroid administration | 0.97 (0.96–0.99) | 0.001 |
| Frailty | ||
| Non-frail | Reference | 0.843 |
| Pre-frail/Frail | 1.10 (0.41–2.98) |
| Variables | Estimate (95% CI) | p Value |
|---|---|---|
| Steroids | ||
| Dexamethasone | Reference | |
| methylprednisone | 3.83 (−0.53, 8.18) | 0.084 |
| Age | 0.19 (0.08, 0.30) | <0.001 |
| Sex | ||
| Female | Reference | |
| Male | 1.71 (−1.28, 4.70) | 0.259 |
| Race | ||
| Hispanic | Reference | |
| Non-Hispanic | −0.20 (−3.56, 3.16) | 0.9052 |
| Days on steroid | 0.57 (0.36, 0.78) | <0.001 |
| CRP | −1.85 (−3.55, −0.15) | 0.033 |
| D-dimer | 0.29 (−0.86, 1.45) | 0.616 |
| Calcium | −2.49 (−19.82, 14.83) | 0.775 |
| Creatinine | 0.81 (-1.53, 3.15) | 0.493 |
| PO2 | 0.18 (−3.19, 3.55) | 0.916 |
| Tocilizumab | 0.04 (−4.24, 4.33) | 0.984 |
| Admission to steroid interval | 0.05 (0.01, 0.10) | 0.042 |
| Admission to ICU interval | 0.03 (0.02, 0.04) | <0.001 |
| Vented days | 0.67 (0.52, 0.82) | <0.001 |
| Admission quarter | ||
| April-June | Reference | |
| July-September | −1.91 (−6.15, 2.32) | 0.371 |
| October-December | −1.89 (−7.41, 3.64) | 0.499 |
| APR Severity | ||
| 2 | Reference | |
| 3 | 1.73 (−18.47, 21.94) | 0.865 |
| 4 | 10.98 (−10.04, 32.01) | 0.302 |
| APR Mortality Risk | ||
| 1 | Reference | |
| 2 | 3.42 (−13.97, 20.81) | 0.697 |
| 3 | 3.67 (−19.5, 26.84) | 0.754 |
| 4 | −4.09 (−27.87, 19.69) | 0.733 |
| Mortality | −16.99 (−20.75, -13.23) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canaan, M.; Williams, K.N.; Ahmed, M.A.; Zhang, Z.; Ramamoorthy, V.; McGranaghan, P.; Rubens, M.; Saxena, A. Retrospective Comparison of Hospital Outcomes among Mechanically Ventilated COVID-19 Patients in ICU Who Received Methylprednisolone or Dexamethasone. BioMed 2023, 3, 225-235. https://doi.org/10.3390/biomed3020020
Canaan M, Williams KN, Ahmed MA, Zhang Z, Ramamoorthy V, McGranaghan P, Rubens M, Saxena A. Retrospective Comparison of Hospital Outcomes among Mechanically Ventilated COVID-19 Patients in ICU Who Received Methylprednisolone or Dexamethasone. BioMed. 2023; 3(2):225-235. https://doi.org/10.3390/biomed3020020
Chicago/Turabian StyleCanaan, Mariangela, Kelsey N. Williams, Md Ashfaq Ahmed, Zhenwei Zhang, Venkataraghavan Ramamoorthy, Peter McGranaghan, Muni Rubens, and Anshul Saxena. 2023. "Retrospective Comparison of Hospital Outcomes among Mechanically Ventilated COVID-19 Patients in ICU Who Received Methylprednisolone or Dexamethasone" BioMed 3, no. 2: 225-235. https://doi.org/10.3390/biomed3020020