
A Longitudinal Assessment of Substance Use Treatment during the COVID-19 Pandemic Using Staff and Service Data

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment and Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Treatment Staff Self-Report Data
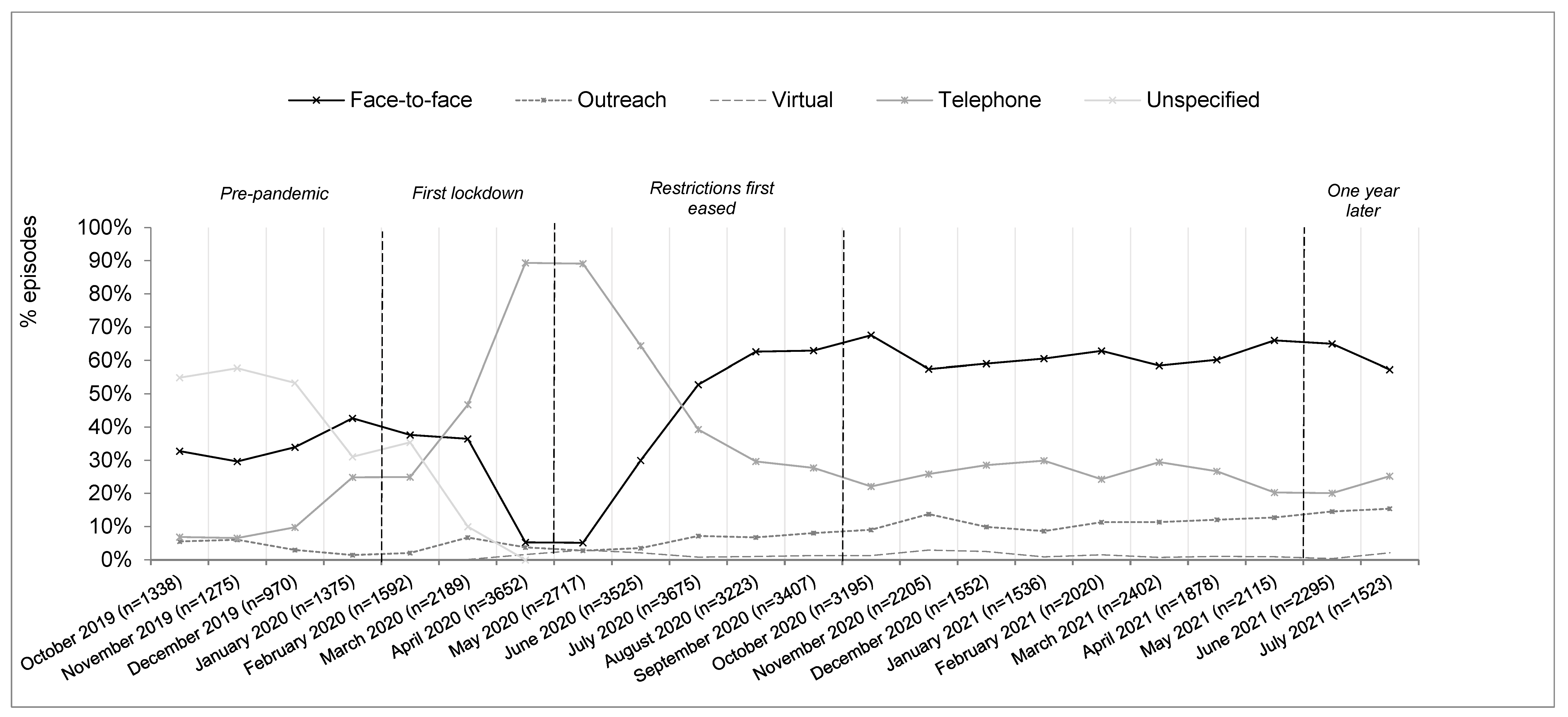
3.2. Service Treatment Record Data
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carlyle, M.; Leung, J.; Walter, Z.C.; Juckel, J.; Salom, C.; Quinn, C.A.; Davidson, L.; Ellem, R.; Newland, G.; Hides, L. Changes in Substance Use Among People Seeking Alcohol and Other Drug Treatment During the COVID-19 Pandemic: Evaluating Mental Health Outcomes and Resilience. Subst. Abus. Res. Treat. 2021, 15, 11782218211061746. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef] [PubMed]
- Molfenter, T.; Roget, N.; Chaple, M.; Behlman, S.; Cody, O.; Hartzler, B.; Johnson, E.; Nichols, M.; Stilen, P.; Becker, S. Use of telehealth in substance use disorder services during and after COVID-19: Online survey study. JMIR Ment. Health 2021, 8, e25835. [Google Scholar] [CrossRef] [PubMed]
- Cantor, J.; McBain, R.K.; Kofner, A.; Hanson, R.; Stein, B.D.; Yu, H. Telehealth adoption by mental health and substance use disorder treatment facilities in the COVID-19 pandemic. Psychiatr. Serv. 2022, 73, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Pham, H.; Zhu, Y.; Clingan, S.E.; Lin, L.A.; Murphy, S.M.; Campbell, C.I.; Sorrell, T.R.; Liu, Y.; Mooney, L.J.; et al. Telemedicine along the cascade of care for substance use disorders during the COVID-19 pandemic in the United States. Drug Alcohol Depend. 2023, 242, 109711. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.B.; Fitzsimmons-Craft, E.E.; Graham, A.K. Digital technology can revolutionize mental health services delivery: The COVID-19 crisis as a catalyst for change. Int. J. Eat. Disord. 2020, 53, 1155–1157. [Google Scholar] [CrossRef] [PubMed]
- Da, B.L.; Im, G.Y.; Schiano, T.D. Coronavirus disease 2019 hangover: A rising tide of alcohol use disorder and alcohol-associated liver disease. Hepatology 2020, 72, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.Q.; Kaelber, D.C.; Xu, R.; Volkow, N.D. COVID-19 risk and outcomes in patients with substance use disorders: Analyses from electronic health records in the United States. Mol. Psychiatry 2021, 26, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Brener, L.; Horwitz, R.; Rance, J.; Caruana, T.; Bryant, J. Health worker perceptions of the impact of COVID-19 on harm reduction services for people who inject drugs. Health Soc. Care Community 2022, 30, 2320–2329. [Google Scholar] [CrossRef] [PubMed]
- Bayers, T.; Strohmaier, T.; Shreffler, J.; Huecker, M. Perceptions of individuals in treatment for substance use disorder during COVID-19: Insight on mental health, sobriety, access to treatment, and telehealth. J. Addict. Dis. 2022, 40, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Busch, A.B.; Sugarman, D.E.; Horvitz, L.E.; Greenfield, S.F. Telemedicine for treating mental health and substance use disorders: Reflections since the pandemic. Neuropsychopharmacology 2021, 46, 1068–1070. [Google Scholar] [CrossRef] [PubMed]
- Hawke, L.D.; Sheikhan, N.Y.; MacCon, K.; Henderson, J. Going virtual: Youth attitudes toward and experiences of virtual mental health and substance use services during the COVID-19 pandemic. BMC Health Serv. Res. 2021, 21, 340. [Google Scholar] [CrossRef] [PubMed]
- Duraisingam, V.; Roche, A.M.; Kostadinov, V.; Hodge, S.; Chapman, J. Predictors of work engagement among Australian non-government drug and alcohol employees: Implications for policy and practice. Int. J. Drug Policy 2020, 76, 102638. [Google Scholar] [CrossRef] [PubMed]
- Roche, A.; Nicholas, R. Workforce development: An important paradigm shift for the alcohol and other drugs sector. Drugs Educ. Prev. Policy 2017, 24, 443–454. [Google Scholar] [CrossRef] [Green Version]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlyle, M.; Newland, G.; Morris, L.; Ellem, R.; Tisdale, C.; Quinn, C.A.; Hides, L. A Longitudinal Assessment of Substance Use Treatment during the COVID-19 Pandemic Using Staff and Service Data. BioMed 2023, 3, 217-224. https://doi.org/10.3390/biomed3020019
Carlyle M, Newland G, Morris L, Ellem R, Tisdale C, Quinn CA, Hides L. A Longitudinal Assessment of Substance Use Treatment during the COVID-19 Pandemic Using Staff and Service Data. BioMed. 2023; 3(2):217-224. https://doi.org/10.3390/biomed3020019
Chicago/Turabian StyleCarlyle, Molly, Grace Newland, Leith Morris, Rhiannon Ellem, Calvert Tisdale, Catherine A. Quinn, and Leanne Hides. 2023. "A Longitudinal Assessment of Substance Use Treatment during the COVID-19 Pandemic Using Staff and Service Data" BioMed 3, no. 2: 217-224. https://doi.org/10.3390/biomed3020019