

Flash Radiotherapy: Innovative Cancer Treatment



1
Radiation Medicine Program, Princess Margaret Cancer Centre, University Health Network, Toronto, ON M5G 1X6, Canada
2
Department of Radiation Oncology, University of Toronto, Toronto, ON M5T 1P5, Canada
3
Centre of Advance Nanotechnology, Faculty of Applied Science and Engineering, University of Toronto, Toronto, ON M5S 3E4, Canada
4
Department of Materials Science and Engineering, University of Toronto, Toronto, ON M5S 3E4, Canada
*
Author to whom correspondence should be addressed.
Encyclopedia 2023, 3(3), 808-823; https://doi.org/10.3390/encyclopedia3030058
Submission received: 18 May 2023
/
Revised: 12 June 2023
/
Accepted: 23 June 2023
/
Published: 26 June 2023
(This article belongs to the Section Medicine & Pharmacology)
Definition
:Flash radiotherapy (Flash-RT) is an innovative technique used in radiotherapy for cancer treatment because it delivers an extremely high dose of radiation (>40 Gy/s) to the tumour in a very short period of time, typically within a fraction of a second. This ultra-fast delivery of radiation distinguishes Flash-RT from conventional radiotherapy, which typically involves the delivery of radiation over a longer time period, often several minutes. Studies conducted in cell and preclinical models suggested that Flash-RT may spare normal tissues from radiation-related side effects, such as skin toxicity, gastrointestinal complications, and damage to organs-at-risk. This is believed to be due to the unique normal tissue response to the ultra-high dose rate. Nevertheless, while Flash-RT shows promising results in preclinical and early clinical studies, one should note that the technique is still in the early stages of development. This entry provides a comprehensive exploration of the immense potentials of Flash-RT, covering its background, mechanisms, radiation sources, recent experimental findings based on cell and preclinical models, and future prospects. It aims to provide valuable insights into this innovative radiotherapy technology for anyone interested in the subject.
1. Introduction
Radiotherapy is a common treatment method used for cancer. It involves the use of high-energy radiation, such as X-rays or protons, to target and destroy cancer cells in the body [1,2]. Radiotherapy works by damaging the DNA inside cancer cells, which prevents them from growing and dividing further [3,4]. Radiotherapy can be highly effective in treating various types of cancer. It can be used either as a primary treatment to eliminate tumours, or in combination with other treatments like surgery or chemotherapy to enhance the overall effectiveness [5]. Moreover, radiotherapy allows for precise targeting of cancer cells. It can target specific areas of the body where the tumour is located, minimizing damage to healthy surrounding tissues. This makes it particularly useful for tumours that are confined to a specific region.
Although this treatment modality is the most commonly employed and highly efficient for combating tumours, it can lead to acute and long-term damage to healthy tissues [6]. The dosage of radiation administered to the tumour is restricted due to the potential toxicity to neighboring healthy tissues. This limitation can result in incomplete eradication of the tumour and a reduction in the overall effectiveness of radiotherapy [7]. Consequently, the prevention or mitigation of radiation-induced injuries to healthy tissues has always been a significant focus in radiotherapy research. Thus far, several techniques for delivering radiation doses, such as stereotactic body radiotherapy and intensity-modulated radiotherapy, have been developed to enhance the targeted radiation to the tumour while minimizing exposure to surrounding healthy tissues [8,9,10]. Despite these advancements, the treatment process typically involves multiple sessions, ranging from two to over twenty fractions. Consequently, patients are required to travel to the cancer center for a period of one to a couple of weeks in order to complete the radiotherapy treatment [11]. This is often an additional burden to already stressed patients and families.
Flash-RT offers an attractive potential solution. It is an emerging technique in radiation therapy that delivers an ultra-high dose of radiation to a tumour in an extremely short amount of time, typically within a fraction of a second (dose rate > 40 Gy/s) [12]. Unlike conventional radiotherapy, which delivers radiation in multiple fractions over several weeks, Flash-RT administers the entire treatment dose in a single Flash [13]. This novel approach to radiotherapy has shown promising results in preclinical and early clinical studies [14]. The main advantage of Flash-RT is its potential to increase the therapeutic ratio by selectively damaging cancer cells while minimizing damage to surrounding normal tissues. This is achieved by exploiting the differences in cellular response to high-dose radiation between tumour cells and normal cells [15]. A comparison between conventional and Flash radiotherapy can be found in Table 1. At present, Flash-RT continues to be a subject of ongoing research, and its implementation in clinical practice is currently limited to select research institutions [16,17]. Further studies are ongoing to evaluate its safety, efficacy, and optimal clinical applications [18,19]. The aim is to determine the full potential of Flash-RT to improve cancer treatment outcomes while reducing treatment duration and potential side effects. This entry will present a comprehensive overview of Flash-RT, covering its background, mechanisms, radiation sources, current cell and preclinical results, as well as future prospects. The intention is to make this innovative radiotherapy technology accessible to a wide range of experts, including those with backgrounds in engineering, science, and medicine. By providing a comprehensive understanding, this entry seeks to facilitate knowledge transfer and promote further exploration and collaboration in the field of Flash-RT.
2. Background and History
Flash-RT is a relatively new concept in the field of radiotherapy. Its history can be traced back to the early 20th century when researchers observed certain notable effects of high-dose radiation [16,18,20]. One of the earliest observations related to Flash-RT occurred in the late 1950s. Dewey and Boag reported on the phenomenon known as the Flash effect, which is now referred to as Flash-RT [21]. They conducted an experiment using ultra-high-dose-rate megavoltage X-rays to irradiate Serratia marcescens. The study demonstrated that the bacteria, when exposed to ultra-high dose rates (UHDRs) (10–20 krads/2 μs), exhibited lower radiosensitivity in a nitrogen–oxygen mixture compared to the situation when irradiated at normal dose rates (1 krads/min) in 100% nitrogen. This lower radiosensitivity corresponded to the response typically observed under anaerobic conditions. Such findings indicated that the radiosensitivity of Serratia marcescens was influenced by both the oxygen content and the dose rate of the radiation. Town [22] discovered that mammalian cells irradiated at an UHDR of 3.5 × 106 krad/s showed interesting results. When the cells received a dose of up to 1 krads, a single pulse had a higher survival rate compared to two pulses. The result from Town is supported by Berry et al. [23] who observed similar outcomes in their experiments with hamster and HeLa cells, using ultra-high-dose-rate irradiation of 1 krads for a 15 ns pulse.
In small-animal experiments conducted by Hornsey et al. [24], it was discovered that the effectiveness of whole-body irradiation in mice was diminished when oxygen was administered during irradiation at dose rates exceeding 6 krads/min. This finding indicated a reduction in the impact of radiation in inducing lethality when oxygen was present during irradiation. Similarly, Field et al. [25] investigated the effects of high-dose-rate irradiation on the skin reactions and late deformities in rats by utilizing 7 MeV electron beams. Their study revealed that at a dose rate of 0.5 Mrads/min, there was a significant decrease in the radiation’s ability to cause skin reactions. This further supported the notion that the Flash effect, characterized by reduced effectiveness, is closely linked to oxygen consumption. These cell and preclinical experiments collectively underscored the relationship between the Flash effect and the presence of oxygen during irradiation. The results emphasized the impact of oxygen consumption on the observed reduction in radiation effectiveness, highlighting the importance of oxygen-related factors in Flash-RT [26,27,28].
In 2014, Favaudon et al. [29] compared the effects of Flash UHDR and conventional dose rate irradiation on lung tissue in mice. They locally irradiated the mice and assessed the outcomes. The findings revealed that all mice subjected to conventional dose rate irradiation of 17 Gy experienced significant pneumonia and fibrosis. However, the opposite was observed in mice irradiated with Flash; none of them developed pneumonia or fibrosis after receiving the same dose of Flash. When the dose was raised to 30 Gy, pneumonia and fibrosis started to emerge in Flash-irradiated mice. Favaudon et al. [29] also discovered that Flash irradiation at 17 Gy prevented the activation of transforming growth factor beta and the occurrence of acute apoptosis in bronchi and blood vessels. For larger animals, a clinical trial was conducted on six cats with locally advanced T2/T3N0M0 nasal plane squamous cell carcinoma, exhibiting hair loss and fibrinoid necrosis. The trial involved a Phase I escalation study, where a single dose ranging from 25 Gy to 41 Gy was administered [30]. The trial aimed to assess the acute and late endpoints of the treatment, specifically looking at the damage to heathy tissue compared to conventional radiotherapy. The results indicated a “protective effect” of Flash-RT, where the damage to normal tissue was less than that observed with conventional radiotherapy. The experimental group showed an 84% progression-free survival rate over a 16-month period. The results affirmed the potential advantages of Flash-RT and laid the groundwork for future investigations into its impact on humans [30]. In 2019, Bourhis et al. [31] conducted a study involving the first human patient to receive Flash-RT. The patient had a multi-resistant CD30+ T-cell cutaneous lymphoma and was prescribed a dose of 15 Gy. The treatment was delivered using a 5.6-MeV linear accelerator in an ultra-short duration of 90 ms. Following the treatment, a clinical examination conducted three weeks later revealed only grade 1 epithelitis and oedema in the soft tissues surrounding the tumour. Based on the follow-up examination, Bourhis et al. [31] concluded that this Flash treatment was both feasible and safe, resulting in a favorable outcome for the patient.
3. Rationale and Mechanism
Flash-RT is still an emerging area of research, and its full rationale and potential applications may not be completely understood [32,33,34]. However, based on the current findings, the rationale behind Flash-RT based on the observation that high-dose radiation delivered at an ultra-fast rate may have several potential advantages over conventional radiotherapy using a number of fractions. These advantages include normal tissue sparing as Flash-RT has shown promise in sparing healthy tissues while still effectively targeting cancer cells [35,36,37]. Preclinical studies have suggested that Flash-RT may reduce damage to normal tissues due to the unique biological response of tissues to UHDRs [38,39,40,41]. On the other hand, Flash-RT can improve the tumour control, which is also supported by preclinical studies. These studies indicated that Flash-RT may enhance tumour control by delivering a high dose of radiation that overwhelms cancer cells’ DNA repair mechanisms, making them less likely to survive and reproduce [42,43]. Concerning the radiation dose delivery, since Flash-RT delivers the radiation dose much more quickly, treatment times could potentially be significantly reduced. This would greatly enhance the patient experience, as a much shortened treatment time improves patient comfort and convenience, as well as reduces the potential for intrafraction patient motion during treatment. From the early clinical study, Flash-RT has been proven to be effective and safe and could potentially reduce treatment costs by shortening the overall treatment time and increasing treatment capacity [44]. However, it is important to note that this aspect is still speculative at this stage.
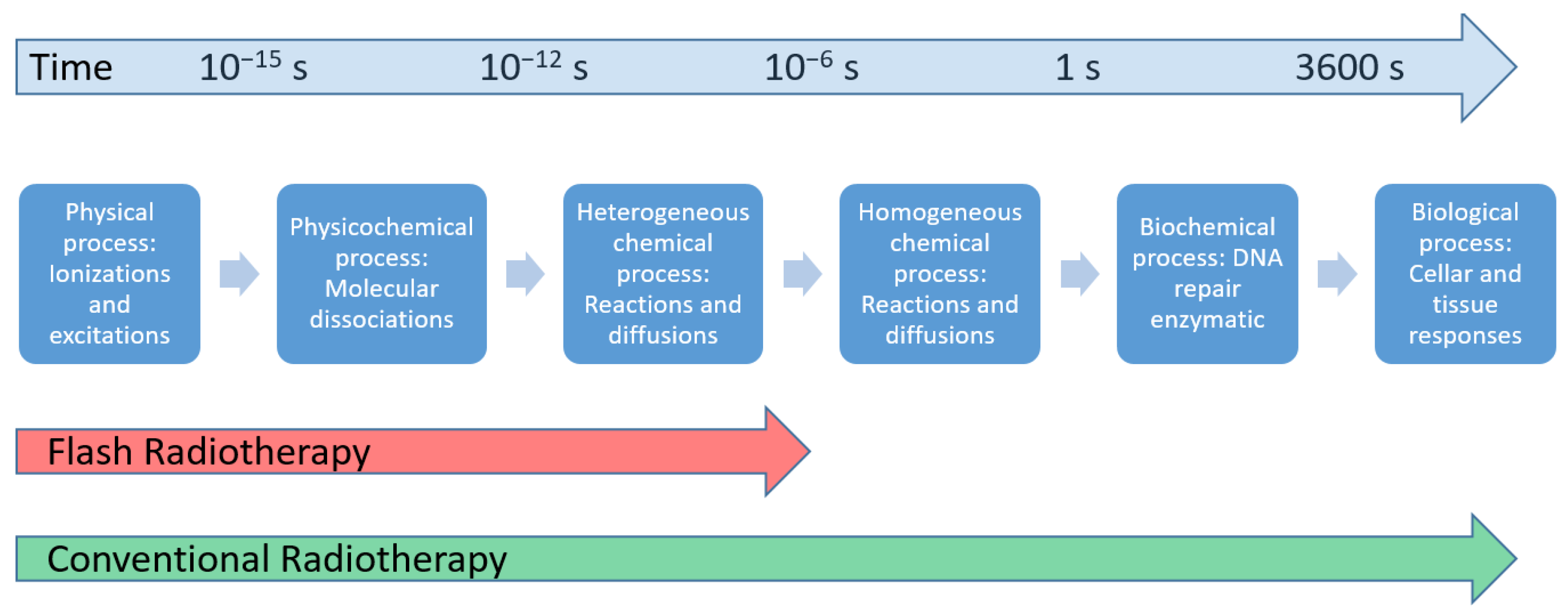
When comparing the distinct physiochemical processes over time between Flash and conventional radiotherapies, it is important to highlight that Flash irradiation is approximately 1000 times faster than conventional irradiation, as depicted in Figure 1. This exceptional speed allows Flash to provide substantial and enduring preservation of healthy tissue within microseconds. Such rapid interventions are simply beyond the reach of most biological and pharmacological strategies, which usually operate on timescales that are six orders of magnitude slower [45].
The exact mechanism of Flash-RT is not yet fully understood, and there are many ongoing preclinical and clinical studies [24,25,26,27,28,31]. However, several hypotheses havebeen proposed to explain the potential benefits observed with Flash-RT. Theses hypotheses include the oxygen effect, reactive oxygen species (ROS)-mediated cell damage, and a modified immune and inflammatory response. This emphasizes the potential of Flash technology to transform the field of radiotherapy, not only by immobilizing organ and tumour motion but also by recognizing the distinct responses of normal tissues and tumours to this technique.
3.1. Oxygen Effect
According to the prevailing belief, Flash-RT utilizes the oxygen effect, which denotes the heightened vulnerability of tumour cells to radiation when oxygen is present. The hypothesis suggests that the exceptionally rapid delivery of UHDR in Flash-RT could potentially deplete the oxygen within the affected tissue, leading to a temporary state of hypoxia and a transient resistance to radiation [46]. Oxygen plays a crucial role in the Flash effect and serves as a measurable parameter to assess its impact. Research suggests that many normal tissues can sustain a limited number of cell populations for ongoing renewal and regeneration even under conditions of low physiological oxygen levels [47]. When a high radiation dose is delivered at an UHDR, it results in a rapid oxygen depletion, leading to a diffusion of oxygen to maintain adequate oxygenation levels. Consequently, healthy tissue responds similarly to hypoxic tissue. At UHDRs, oxygen depletion occurs, mimicking hypoxia and leading to enhanced resistance of normal tissue against radiation. In situations where hypoxic tumours exhibit resistance to radiation and are surrounded by oxygenated normal tissue that is susceptible to radiation, the predominant effect of UHDRs is observed on normal tissue, with minimal impact on the already hypoxic tumour tissue, similar to conventional radiotherapy [45]. When the UHDR radiation interacts with the cell, water molecules within cells undergo breakdown, generating ROS that indirectly damage DNA. A significant aspect of this damage involves the frequent attack of DNA by hydroxyl radicals. In the case of low-linear-energy transfer radiation, approximately 70% of DNA damage is attributed to reactive oxygen species (ROS), while the remaining damage arises from direct interactions between DNA and radiation [27,48]. Based on the oxygen fixation hypothesis, when oxygen radicals are accountable for this indirect DNA damage, the presence of molecular oxygen leads to the fixation of damage through the formation of more detrimental peroxy radicals [49].
Although the oxygen consumption mechanism of Flash-RT has been widely acknowledged, recent research has presented challenges to this prevailing understanding. Certain groups now question the likelihood of Flash-RT depleting oxygen to the extent of the hypoxia observed in larger tissues during radiation exposure. In comparison to conventional in vitro irradiation, Flash irradiation at the same dose has been found to result in lower oxygen consumption, possibly indicating a protective effect associated with Flash. Measuring the disparity in oxygen consumption between Flash and conventional exposure in vivo is challenging due to the influence of oxygen supplementation on blood measurements [47]. In a study conducted by Tinganelli et al. [50], the impact of Flash irradiation on CHO-K1 cells was investigated under different levels of oxygenation, ranging from 0 to 21%. They observed that the protective effect of Flash was dependent on the level of oxygenation, with a more significant effect observed in conditions with a lower oxygen content. These findings support the skepticism expressed by some research groups regarding the mechanism of oxygen consumption [51,52]. Several studies found a minor decrease in oxygenation subsequent to Flash irradiation, but they argued that this has a negligible impact on radiosensitivity [49,53,54]. Jansen et al. [53] conducted an experimental study to investigate whether oxygen depletion occurs during Flash irradiation. The measurement of oxygen concentration was carried out in vitro, involving the irradiation of water with photons, protons, and carbon ions. In a study by Jansen et al. [53], it was observed that the consumption of oxygen in water was mainly influenced by factors such as radiation dose, dose rate, and linear energy transfer. They found that higher dose rates were associated with lower levels of oxygen consumption. Additionally, they did not identify any clinically significant limits to oxygen consumption, and concluded that while Flash irradiation does consume oxygen, the amount consumed was not sufficient to deplete it entirely. They observed that for high dose rates, less oxygen was consumed compared to conversional radiotherapy dose rates. This discovery posed a challenge to the conventional hypothesis regarding oxygen consumption and its role in Flash irradiation.
3.2. ROS and Free Radicals
Flash-RT delivers an extremely high radiation dose in a very short period of time leading to the generation of ROS and free radicals, which plays a significant role in the observed benefits and mechanisms of Flash-RT. ROS, such as superoxide anion (O2•−), hydrogen peroxide (H2O2), and hydroxyl radical (•OH), are highly reactive molecules containing oxygen atoms. They can be generated through the radiolysis of water molecules by the ionizing radiation used in Flash-RT. These ROS can engage in additional reactions with various cellular components, such as DNA, proteins, and lipids, resulting in oxidative stress and cellular damage [55]. On the other hand, free radicals are molecules or atoms that contain unpaired electrons, making them highly reactive and unstable. During Flash-RT, the rapid release of high-energy radiation can generate free radicals, including oxygen-centered radicals (such as hydroxyl radicals) and carbon-centered radicals. These free radicals can initiate chain reactions and induce oxidative damage to cellular components [15,28]. This mechanism helps explain some of the potential advantages of Flash-RT, such as the differential response of normal and cancerous tissues to UHDRs. Normal tissues, which have more robust antioxidant systems, may be better equipped to handle the increased oxidative stress induced by Flash-RT compared to cancer cells. Additionally, the rapid delivery of radiation in Flash-RT may limit the diffusion of ROS and free radicals, leading to localized effects and sparing surrounding healthy tissues [45,56].
A recent study demonstrated that exposing zebrafish embryos to irradiation using conventional and Flash-RT had minimal effects on their morphology even five days after fertilization [57]. The observed phenomenon was attributed to the limited generation of ROS, suggesting that the enhanced radiation resistance of normal tissues in response to Flash-RT is closely linked to decreased ROS levels. Another study conducted by Abolfath et al. [46] employed molecular dynamics simulations to explore the generation of reactive species near DNA at various dose rates and oxidation levels. In conditions of normal oxygen levels and high dose rates, individual ROS molecules aggregate and form resonant or metastable molecular states interconnected by hydrogen bonds. These resulting clusters exhibit limited diffusivity and have a lower potential for causing biological damage compared to ROS. In their study, Favaudon et al. [27] put forth some hypotheses and compared them to the current findings. The first hypothesis, known as the Transient Oxygen Depletion hypothesis, suggests that the preservation of normal tissue at UHDRs is due to transient hypoxic radiation protection caused by oxygen depletion. Although in vivo data indicated that local oxygen levels significantly influenced the final outcomes [45], the isoefficiency of tumour cell destruction under normoxic and hypoxic conditions provided less support for this hypothesis. Furthermore, both direct measurements of oxygen consumption during Flash irradiation using optical methods in vitro and in vivo, as well as observations of the Flash effect in oxygenated cultured cells with assessments of DNA damage and cell survival, lend support to the Transient Oxygen Depletion hypothesis [27]. This suggests that self-destruction of free radicals is a more plausible explanation for the observed effects of Flash irradiation. In a study conducted by Montay-Gruel et al. [45], it was found that UHDR radiation promotes the protection of normal tissues by inhibiting the production of ROS through oxygen consumption. To simulate physiological oxygen levels, Montay-Gruel et al. [45] irradiated water containing 4% oxygen using both Flash and conventional radiotherapies. Following Flash irradiation, there was a significant decrease in the concentration of hydrogen peroxide (H2O2) in the aqueous solution. Spitz et al. [58] further emphasized the relationship between the Flash effect and the instantaneous generation of free radicals, as well as the inherent differences in redox and free radical chemistry between normal and tumour tissues. They suggested that normal tissue cells had a lower content of unstable iron compared to tumour tissue cells. As a result, the further reaction of ROS was more easily restricted in normal tissue cells, leading to a reduction in cellular damage. These findings highlight the role of oxygen consumption in Flash-RT, its impact on ROS production, and the subsequent cellular damage. This study suggests that the protective effect observed in normal tissues during Flash-RT may be attributed to the differences in redox chemistry and iron content, which limit the detrimental effects of ROS and free radicals [58].
3.3. Immune and Inflammatory Response
The immune and inflammatory hypothesis in Flash-RT suggests that the unique characteristics of Flash-RT, such as the UHDR and the absence of an inflammatory response, may contribute to the modulation of immune and inflammatory processes within the tumour microenvironment [59,60,61,62]. This hypothesis proposes that Flash-RT can elicit a distinct immune and inflammatory response compared to conventional radiotherapy, potentially leading to enhanced anti-tumour effects. Transforming growth factor beta (TGF-β), a crucial pro-inflammatory cytokine, has been specifically associated with modulating the effects of Flash-RT in comparison to conventional dose-rate radiotherapy [63,64]. Studies indicated that the signaling pathway of TGF-β is downregulated in mice treated with radiotherapy [65,66,67]. TGF-β has been identified as a key factor in the radiation resistance of tumour-infiltrating T cells. Other research has suggested that TGF-β signaling inhibits the immune system and promotes cancer progression, leading to the conclusion that inhibitors targeting the TGF-β pathway may enhance the treatment of malignant tumours [66]. Flash irradiation, characterized by reduced treatment time, allows a greater number of circulating immune cells to survive compared to conventional radiotherapy. However, this time reduction also results in the loss of the efficacy of fractionated irradiation [68]. Rama et al. [69] found that Flash proton beams improved the control of lung tumours, possibly due to the recruitment of CD3+ T lymphocytes into the tumour. Some studies compared Flash and conventional radiotherapies in immunocompromised animal models, but no significant differences in tumour response have been observed [70,71,72].
In comparison to conventional dose rates, the UHDR in Flash was found to induce a 1.8-fold increase in TGF-β levels 24 h after irradiation, while conventional dose rates led to a 6.5-fold increase [73]. This suggests that Flash radiation has the potential to reduce radiation-induced chronic inflammation. Previous studies have also reported a reduction in TGF-β signaling in mice irradiated with Flash compared to conventional dose rates [24,45,74]. Clinical studies have observed that differences in high dose rate and total treatment time can reduce the proportion of circulating blood cells exposed to radiation, thus preserving the immune system [28,75]. It has been proposed that this Flash approach may be more effective than subconventional dosing. Additionally, the occurrence of chromosomal aberrations in circulating lymphocytes following radiation exposure has been found to be dependent on exposure time and volume, although this has not been specifically confirmed for Flash exposure [76]. Furthermore, research on the effect of whole-brain irradiation in mice demonstrated that Flash irradiation resulted in lower levels of pro-inflammatory cytokines in the hippocampus compared to conventional dose-rate irradiation [77]. At 10 weeks post-irradiation, conventional dose rates led to a statistically significant increase in five out of ten tested cytokines, while Flash radiation only increased three cytokines. These results showed that less pro-inflammatory cytokines were induced by Flash-RT compared to conventional radiotherapy. Some recent studies on the mechanism of Flash radiotherapy are shown in Table 2.
4. Flash Radiation Beams and Dosimetry
Flash-RT can be delivered using different types of radiation beams, including electron, photon, proton, and heavy-ion beams. These beams can be shaped and directed to target the tumour while minimizing exposure to nearby healthy tissues. In radiotherapy, the majority of tumours such as lung, liver, and prostate are often situated at depths that cannot be reached by megavoltage electrons (e.g., 4–16 MeV) and kilovoltage photons generated by linear accelerators and orthovoltage X-ray units, respectively [1]. Consequently, radiotherapy for humans must be capable of delivering a therapeutic dose at depths in the range of 10–15 cm in the patient’s body [2]. Potential solutions to overcome this limitation involve megavoltage photon- or proton-beam-based Flash-RT, as well as the utilization of very high energy electrons (VHEEs).
4.1. Very High Energy Electron Beams
VHEEs refers to electrons with an energy range of 50–250 MeV, enabling them to penetrate deeper into the body [82]. However, the implementation of VHEEs is currently constrained by technical challenges associated with accelerating electrons in a suitably sized medical device that is neither overly large nor overly complex. Nonetheless, ongoing efforts are being made to construct appropriate accelerators for this purpose. For example, the technology developed for the proposed Compact Linear Collider (CLIC) at CERN in 2022 holds the potential to bring Flash-RT into existence [83]. On the other hand, Maxim et al. [84] developed a Pluridirectional High-Energy Agile Scanning Electronic Radiotherapy (PHASER) platform using the cutting-edge advancements in medical linear accelerator technology. This platform for clinical translation of Flash-RT has the potential to deliver VHEEs with energies between 100 and 200 MeV. PHASER incorporates a range of core innovations to facilitate the near-instantaneous administration of precise and conformal image-guided radiotherapy. By doing so, it effectively eliminates the influence of tumour motion and can harness a superior Flash radiobiological therapeutic index.
4.2. Photon Beams
In Flash-RT, to achieve UHDRs using photons, we face technical challenges associated with the low efficiency when converting electron beams into photon beams. In a typical linear accelerator for conventional radiotherapy, only a small portion of the energy fluence carried by electrons is effectively transferred to photons, while the majority of the energy fluence is dissipated through different phenomena, including heat. To enable the development of a Flash photon accelerator, these technical hurdles need to be overcome. Such an accelerator would require a source capable of generating significantly larger numbers of electrons compared to currently available devices. Moreover, the challenges related to accelerating such a large quantity of electrons and efficiently transferring their energy to photons need to be addressed. Resolving these technical issues surrounding electron-to-photon conversion and the efficient utilization of energy in the process is crucial for the advancement of Flash-RT using photons. By finding solutions to these challenges, we can unlock the potential for delivering UHDRs in radiotherapy, thereby enhancing its effectiveness in treating various types of tumours.
Currently, various synchrotron facilities worldwide have conducted preclinical experiments using synchrotron-based techniques such as Spatially Fractionated Radiation Therapy, Microbeam Radiation Therapy, or Minibeam Radiation Therapy [85,86,87,88]. These irradiations have demonstrated peak dose rates exceeding 40 Gy s−1. For instance, at the Spring-8 BL28B2 beamline in Hyogo, Japan, operating at 8 GeV, a peak dose rate of 140 Gy s−1 (air kerma rate) with a mean energy of 90 keV has been achieved using a stable electron current of 100 mA [89]. Similarly, the x17B beamline at the 2.8 GeV National Synchrotron Light Source in Brookhaven National Laboratory, New York, has reached dose rates of up to 830 Gy s−1 with a mean energy between 50 and 120 keV and a pulse repetition frequency of 53 Hz using 2 ns pulses [90]. Although these findings are promising, the use of synchrotron X-ray beams in Flash experiments requires further investigation. This is because the inherently small field size necessitates scanning the beam across the extended irradiation volume to achieve the desired broad beam coverage. However, this scanning process reduces the dose rate, which may compromise the overall irradiation time and the manifestation of the Flash effect. Hence, a crucial consideration in synchrotron Flash experiment is whether the beam scanning can be completed within a fraction of a second, regardless of the employed dose rates. Further research is needed to explore and optimize synchrotron-based approaches for Flash-RT.
4.3. Proton and Heavy-Ion Beams
Protons with energies around 250 MeV or carbon ions with energies of 300 MeV have the potential to reach sufficient depths in the body (10–15 cm) to deliver therapeutic energy for the majority of tumours [91]. Proton therapy sources currently available have shown potential for the clinical implementation of Flash-RT. In clinical radiation therapy, proton beams are typically accelerated using synchrotrons or cyclotrons [92,93]. Proton pencil beams generated by these machines are capable of delivering UHDRs, making them suitable for treating small targets without significant modifications to the existing systems. Therapy using heavy-ion beams, such as carbon-ion beams, is a growing modality in particle therapy, although it is less commonly used compared to other forms of therapy mentioned earlier. It takes advantage of the physical and biological properties of densely ionizing radiation with high linear energy transfer. Currently, there are several carbon ion therapy centers worldwide, and numerous clinical trials are in progress [94,95,96]. It is worth noting that attempts to use ions heavier than carbon (such as neon) resulted in high toxicities. The detection of a Flash effect in the context of carbon ions would carry substantial implications for this therapeutic modality. It could provide substantial benefits and open doors for using ion beams with atomic numbers greater than 6 to target radioresistant and hypoxic tumours. Further research is needed to investigate the potential of the Flash effect with carbon ions and its potential application in improving the efficacy of carbon-ion-beam treatment. However, the challenge with proton and carbon-ion Flash-RT lies in delivering UHDR beamlets across an extended target volume to create the Bragg peak. In this context, achieving sufficiently high mean dose rates throughout the target volume can be challenging. While there is currently a lack of in vivo data regarding conformal Flash irradiations, it is reasonable to hypothesize that UHDRs could be achieved in the plateau region. Therefore, it is plausible that the Flash effect may still be observed in the normal tissues located within the plateau region. Further research is needed to validate this assumption and explore the potential of proton and heavy-ion Flash-RT in clinical practice.
In the study conducted by Buonanno et al. [73], the long-term effects of proton irradiations at the Flash dose rate were investigated in vitro. Utilizing an innovative irradiation platform, they examined both acute and long-term effects in human lung fibroblasts (IMR90) that were exposed to the 4.5 MeV proton beam. The study measured various endpoints, including clonogenic cell survival, formation of γH2AX foci (a marker of DNA damage), induction of premature senescence (identified through β-galactosidase activity), and the expression of the pro-inflammatory marker TGF-β. From the results, the cell survival was found to be unaffected by the proton dose rate. However, at the highest dose rate of 1 kGy/s, foci formation, which is indicative of DNA damage, reached saturation beyond a dose of 10 Gy. Buonanno et al. [73] therefore concluded that in normal lung fibroblasts, the dose rate of proton irradiation had insignificant acute effects. However, it played a significant role in influencing the expression of long-term biological responses in vitro. These findings suggest that utilizing Flash dose rates in proton irradiation can potentially reduce long-term negative effects on biological responses, providing a promising avenue for improving treatment outcomes. In a small-animal experiment conducted by Berreuther et al. [57], the embryonic survival of zebrafish embryos was compared between proton irradiation using the Flash dose rate and conventional dose rate. The study aimed at assessing the effect of various dose rates on embryonic survival and the induction of morphological malformations. The follow-up measurements revealed that the proton dose rate did not significantly influence embryonic survival or the rate of spinal curvature. However, a notable difference was observed between the Flash proton and conventional proton beam in terms of the rate of pericardial edema, which served as an acute radiation effect for a specific dose point. These findings highlight the potential differences in acute radiation effects between Flash proton irradiation and conventional proton beam, indicating the importance of considering dose rates in determining treatment outcomes. A summary of various Flash radiation sources can be found in Table 3.
5. Current Challenges and Future Prospects
Flash-RT presents several challenges that need to be addressed for its successful implementation. One crucial aspect is ensuring accurate dose monitoring and delivery at UHDRs [102]. The ability to precisely measure and control the dose during treatment is essential for the safety and effectiveness of Flash-RT. Technologies such as VHEE beams, laser particle accelerators, and PHASER have been proposed as potential solutions to provide Flash radiation that can reach tumours located at deep depths in a human patient’s body [42,84,99].
Radiation dosimetry is another critical challenge in Flash-RT. Dose detectors capable of measuring the beam fluence at UHDRs in real-time are needed [103]. Detailed Monte Carlo simulations and mathematical modeling of the detector behavior specific to the environment of Flash-RT are necessary for accurate dosimetry [104]. Factors such as sensor linearity, tissue equivalent, saturation, and recombination effects with dose rate must be considered and accounted for. Calibration and quality assurance tools are also essential to ensure the accuracy and reliability of the delivered dose. Precise beam characterization tools such as dosimeters, phantoms, and radiation dose simulation models are required for treatment planning and quality assurance in Flash-RT [16]. Verification of machine output, measurement of delivered dose per pulse, and monitoring of dose rate in real-time are crucial in such an UHDR [105]. Additionally, the pulse duration, interval, and overall irradiation time need to be precisely controlled. In the case of proton beam-based Flash-RT, full pencil-beam scanning capabilities are necessary for optimal treatment planning and delivery [72,106].
Radiation dosimeters can be made based on luminescence, charge, and chemical detection. The key performance requirements for Flash dosimeters are dose-rate independence, temporal, and spatial resolution of a detector [103]. Of the different types of dosimeters, those based on luminescence offer unparalleled spatial–temporal resolution and dose-rate independence. Hence, such dosimeters are among the best candidates to address the challenging requirements for Flash. Luminescent dosimeters generate light as a surrogate for dose and include thermally and optically stimulated luminescence (TLD and OSL, respectively). Flash irradiation increases the concentration of metastable trap states in a dosimeter material from which light emission occurs on either through heating or by low-energy optical stimulation. For the case of scintillators, incident radiation directly causes light emission. Conventional OSL has been reported to be dose-rate independent up to 4 × 109 Gy/s [107] although the technique is passive and cannot provide time-dependent measurements. However, 2D planar detector OSL arrays have been used to measure the spatial distribution of the dose [108]. Unfortunately, only a handful of materials, which were first introduced in the 1960s including Al2O3:C, continue to be the materials chosen for OSL and now Flash, without consideration for the much more challenging requirements. It is likely that new materials with engineered properties will need to be developed for the demanding requirements of Flash—in particular, having tunable bandgap, high efficiency, excellent carrier transport, and well-defined and accessible trap states. Regarding scintillators, they can offer important capabilities for Flash including direct real-time dosimetry, even though they are typically independent of doses up to ~106 Gy/s [97]. Organic scintillators have been reported, but their efficiency is poor [103], whereas inorganic scintillators offer fast nanosecond rise/decay times, radiation hardness, and high detection efficiency because of the increased photoelectric interaction probability for X-rays [103]. Again, with development of new materials, particularly inorganics, scintillators for Flash can be envisaged with a dose-rate independence up to levels of conventional OSL may be feasible along with the specific advantages of time-dependent and spatially dependent measurements.
Radiobiology and clinical practice aspects of Flash-RT need further investigation. Understanding the relationship between the Flash effect, linear energy transfer, and oxygen concentration is crucial. Experimental evidence is needed to distinguish the oxygen levels between normal and malignant tissue and quantify their differences. Treatment planning systems specifically designed for Flash-RT need to be developed to optimize treatment delivery [109,110]. The immune response in both normal and tumour tissues exposed to Flash irradiation should also be studied to assess its impact on treatment outcomes. Mechanisms related to immune and DNA damage responses following Flash-RT require thorough investigation to better comprehend the underlying biological effects [15,18]. Lastly, clinical studies are necessary once beam technologies capable of reaching deep depths in a human patient’s body become available. These studies will evaluate the safety and efficacy of Flash-RT in a clinical setting and provide valuable insights for its integration into standard treatment protocols [16,31,44,111].
6. Conclusions
Flash-RT offers theoretical advantages over conventional radiotherapy, and preclinical experiments have shown promising results. However, these experiments have been limited to depths of several centimeters due to the range limitations of current linear accelerators that accelerate megavoltage electrons. To fully realize the potentials of Flash-RT, significant technological advancements are required. These advancements involve the development of sources that can generate Flash radiations, enabling the delivery of the required dose distribution at greater depths within the human body where most tumours are located. Moreover, the delivery techniques should be adapted to accommodate larger radiation fields, allowing for the treatment of tumours in various locations. Conformal radiation to multiple fields may be required to achieve optimal treatment outcomes. These advanced radiation sources would expand the applicability of Flash-RT.
The emergence of Flash-RT has the potential to revolutionize radiobiology and reshape the field of radiotherapy. It offers the possibility of reducing radiation doses to healthy tissues while maintaining effective tumour control and opens up new avenues for combining radiotherapy with other anti-tumour treatments. However, before Flash-RT can become the primary technology in radiotherapy clinically, further animal experiments are necessary to gather more data and insights. It is crucial to redefine the dose limits for normal tissue and establish radical irradiation doses for cancer.
Over the past few years, Flash-RT emerged as an exceptionally promising treatment approach for cancer patients. This innovative modality sparked significant enthusiasm within the radiation oncology community due to its potential to revolutionize cancer treatment. However, while Flash-RT holds tremendous promise, there are still numerous unanswered questions regarding its overall impact, mechanisms, and clinical viability. It has become evident that unraveling the mystery of Flash is now one of the primary objectives in the field of radiotherapy. Researchers are actively working to understand and explore the full potential of this innovative treatment approach.
Author Contributions
Conceptualization, J.C.L.C. and H.E.R.; methodology, J.C.L.C. and H.E.R.; resources, J.C.L.C. and H.E.R.; writing—original draft preparation, J.C.L.C.; writing—review and editing, J.C.L.C. and H.E.R.; visualization, J.C.L.C.; project administration, J.C.L.C. and H.E.R.; funding acquisition, J.C.L.C. and H.E.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by New Frontiers in Research Fund—Exploration, grant number: NFRFE-2022-00707.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chandra, R.A.; Keane, F.K.; Voncken, F.E.; Thomas, C.R. Contemporary radiotherapy: Present and future. Lancet 2021, 398, 171–184. [Google Scholar] [CrossRef]
- Citrin, D.E. Recent developments in radiotherapy. N. Engl. J. Med. 2017, 377, 1065–1075. [Google Scholar] [CrossRef]
- Lomax, M.E.; Folkes, L.K.; O’neill, P. Biological consequences of radiation-induced DNA damage: Relevance to radiotherapy. Clin. Oncol. 2013, 25, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Groelly, F.J.; Fawkes, M.; Dagg, R.A.; Blackford, A.N.; Tarsounas, M. Targeting DNA damage response pathways in cancer. Nat. Rev. Cancer 2023, 23, 78–94. [Google Scholar] [CrossRef]
- Abbas, Z.; Rehman, S. An overview of cancer treatment modalities. Neoplasm 2018, 1, 139–157. [Google Scholar]
- Barazzuol, L.; Coppes, R.P.; van Luijk, P. Prevention and treatment of radiotherapy-induced side effects. Mol. Oncol. 2020, 14, 1538–1554. [Google Scholar] [CrossRef]
- Stone, H.B.; Coleman, C.N.; Anscher, M.S.; McBride, W.H. Effects of radiation on normal tissue: Consequences and mechanisms. Lancet Oncol. 2003, 4, 529–536. [Google Scholar] [CrossRef]
- Kirkpatrick, J.P.; Kelsey, C.R.; Palta, M.; Cabrera, A.R.; Salama, J.K.; Patel, P.; Perez, B.A.; Lee, J.; Yin, F.F. Stereotactic body radiotherapy: A critical review for nonradiation oncologists. Cancer 2014, 120, 942–954. [Google Scholar] [CrossRef]
- Chiavassa, S.; Bessieres, I.; Edouard, M.; Mathot, M.; Moignier, A. Complexity metrics for IMRT and VMAT plans: A review of current literature and applications. Br. J. Radiol. 2019, 92, 20190270. [Google Scholar] [CrossRef]
- Staffurth, J. A review of the clinical evidence for intensity-modulated radiotherapy. Clin. Oncol. 2010, 2, 643–657. [Google Scholar] [CrossRef]
- Murray, L.J.; Robinson, M.H. Radiotherapy: Technical aspects. Medicine 2016, 44, 10–14. [Google Scholar] [CrossRef]
- Vozenin, M.C.; Hendry, J.H.; Limoli, C.L. Biological benefits of UHDR FLASH radiotherapy: Sleeping beauty awoken. Clin. Oncol. 2019, 31, 407–415. [Google Scholar] [CrossRef]
- Matuszak, N.; Suchorska, W.M.; Milecki, P.; Kruszyna-Mochalska, M.; Misiarz, A.; Pracz, J.; Malicki, J. FLASH Radiotherapy: An emerging approach in radiation therapy. Rep. Pract. Oncol. Radiother. 2022, 27, 343–351. [Google Scholar] [CrossRef]
- Borghini, A.; Vecoli, C.; Labate, L.; Panetta, D.; Andreassi, M.G.; Gizzi, L.A. FLASH UHDRs in radiotherapy: Preclinical and radiobiological evidence. Int. J. Radiat. Biol. 2022, 98, 127–135. [Google Scholar] [CrossRef]
- Marcu, L.G.; Bezak, E.; Peukert, D.D.; Wilson, P. Translational research in FLASH radiotherapy—From radiobiological mechanisms to in vivo results. Biomedicines 2021, 9, 181. [Google Scholar] [CrossRef]
- Taylor, P.A.; Moran, J.M.; Jaffray, D.A.; Buchsbaum, J.C. A roadmap to clinical trials for FLASH. Med. Phys. 2022, 49, 4099–4108. [Google Scholar] [CrossRef]
- Lv, Y.; Lv, Y.; Wang, Z.; Lan, T.; Feng, X.; Chen, H.; Zhu, J.; Ma, X.; Du, J.; Hou, G.; et al. FLASH radiotherapy: A promising new method for radiotherapy. Oncol. Lett. 2022, 24, 1–14. [Google Scholar] [CrossRef]
- Lin, B.; Gao, F.; Yang, Y.; Wu, D.; Zhang, Y.; Feng, G.; Dai, T.; Du, X. FLASH radiotherapy: History and future. Front. Oncol. 2021, 11, 1890. [Google Scholar] [CrossRef]
- Kamperis, E.; Kodona, C.; Giannouzakos, V. A FLASH back to radiotherapy’s past and then fast forward to the future. J. Cancer Prev. Curr. Res. 2019, 10, 142–144. [Google Scholar] [CrossRef]
- Do Huh, H.; Kim, S. History of radiation therapy technology. Prog. Med. Phys. 2020, 31, 124–134. [Google Scholar] [CrossRef]
- Dewey, D.L.; Boag, J.W. Modification of the oxygen effect when bacteria are given large pulses of radiation. Nature 1959, 183, 1450–1451. [Google Scholar] [CrossRef]
- Town, C.D. Effect of high dose rates on survival of mammalian cells. Nature 1967, 215, 847–848. [Google Scholar] [CrossRef]
- Berry, R.J.; Hall, E.J.; Forster, D.W.; Storr, T.H.; Goodman, M.J. Survival of mammalian cells exposed to x-rays at ultra-high dose-rates. Br. J. Radiol. 1969, 42, 102–107. [Google Scholar] [CrossRef]
- Hornsey, S.; Bewley, D.K. Hypoxia in mouse intestine induced by electron irradiation at high dose-rates. Int. J. Radiat. Biol. Relat. Stud. Phys. Chem. Med. 1971, 19, 479–483. [Google Scholar] [CrossRef]
- Field, S.B.; Bewley, D.K. Effects of dose-rate on the radiation response of rat skin. Int. J. Radiat. Biol. Relat. Stud. Phys. Chem. Med. 1974, 26, 259–267. [Google Scholar] [CrossRef]
- Zhang, Q.; Gerweck, L.E.; Cascio, E.; Yang, Q.; Huang, P.; Niemierko, A.; Bertolet, A.; Nesteruk, K.P.; McNamara, A.; Schuemann, J. Proton FLASH effects on mouse skin at different oxygen tensions. Phys. Med. Biol. 2023, 68, 055010. [Google Scholar] [CrossRef]
- Favaudon, V.; Labarbe, R.; Limoli, C.L. Model studies of the role of oxygen in the FLASH effect. Med. Phys. 2022, 49, 2068–2081. [Google Scholar] [CrossRef]
- Hageman, E.; Che, P.P.; Dahele, M.; Slotman, B.J.; Sminia, P. Radiobiological Aspects of FLASH Radiotherapy. Biomolecules 2022, 12, 1376. [Google Scholar] [CrossRef]
- Favaudon, V.; Caplier, L.; Monceau, V.; Pouzoulet, F.; Sayarath, M.; Fouillade, C.; Poupon, M.F.; Brito, I.; Hupé, P.; Bourhis, J.; et al. Ultrahigh dose-rate FLASH irradiation increases the differential response between normal and tumour tissue in mice. Sci. Transl. Med. 2014, 6, 245ra93. [Google Scholar] [CrossRef]
- Vozenin, M.C.; De Fornel, P.; Petersson, K.; Favaudon, V.; Jaccard, M.; Germond, J.F.; Petit, B.; Burki, M.; Ferrand, G.; Patin, D.; et al. The Advantage of FLASH Radiotherapy Confirmed in Mini-pig and Cat-cancer Patients the Advantage of Flash Radiotherapy. Clin. Cancer Res. 2019, 25, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Bourhis, J.; Sozzi, W.J.; Jorge, P.G.; Gaide, O.; Bailat, C.; Duclos, F.; Patin, D.; Ozsahin, M.; Bochud, F.; Germond, J.F.; et al. Treatment of a first patient with FLASH-radiotherapy. Radiother. Oncol. 2019, 139, 18–22. [Google Scholar] [CrossRef]
- Schulte, R.; Johnstone, C.; Boucher, S.; Esarey, E.; Geddes, C.G.; Kravchenko, M.; Kutsaev, S.; Loo, B.W., Jr.; Méot, F.; Mustapha, B.; et al. Transformative Technology for FLASH Radiation Therapy. Appl. Sci. 2023, 13, 5021. [Google Scholar] [CrossRef]
- Zou, W.; Zhang, R.; Schueler, E.; Taylor, P.A.; Mascia, A.E.; Diffenderfer, E.S.; Zhao, T.; Ayan, A.S.; Sharma, M.; Yu, S.J.; et al. Framework for Quality Assurance of UHDR Clinical Trials Investigating FLASH Effects and Current Technology Gaps. Int. J. Radiat. Oncol. Biol. Phys. 2023. Epub ahead of print. [Google Scholar] [CrossRef]
- Vozenin, M.C.; Bourhis, J.; Durante, M. Towards clinical translation of FLASH radiotherapy. Nat. Rev. Clin. Oncol. 2022, 27, 1–13. [Google Scholar] [CrossRef]
- Tinganelli, W.; Weber, U.; Puspitasari, A.; Simoniello, P.; Abdollahi, A.; Oppermann, J.; Schuy, C.; Horst, F.; Helm, A.; Fournier, C.; et al. FLASH with carbon ions: Tumour control, normal tissue sparing, and distal metastasis in a mouse osteosarcoma model. Radiother. Oncol. 2022, 175, 185–190. [Google Scholar] [CrossRef]
- Böhlen, T.T.; Germond, J.F.; Bourhis, J.; Vozenin, M.C.; Ozsahin, E.M.; Bochud, F.; Bailat, C.; Moeckli, R. Normal Tissue Sparing by FLASH as a Function of Single-Fraction Dose: A Quantitative Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 1032–1044. [Google Scholar] [CrossRef]
- Sørensen, B.S.; Sitarz, M.K.; Ankjærgaard, C.; Johansen, J.; Andersen, C.E.; Kanouta, E.; Overgaard, C.; Grau, C.; Poulsen, P. In vivo validation and tissue sparing factor for acute damage of pencil beam scanning proton FLASH. Radiother. Oncol. 2022, 167, 109–115. [Google Scholar] [CrossRef]
- Schüler, E.; Acharya, M.; Montay-Gruel, P.; Loo, B.W., Jr.; Vozenin, M.C.; Maxim, P.G. Ultra-high dose rate electron beams and the FLASH effect: From preclinical evidence to a new radiotherapy paradigm. Med. Phys. 2022, 49, 2082–2095. [Google Scholar] [CrossRef]
- Diffenderfer, E.S.; Sørensen, B.S.; Mazal, A.; Carlson, D.J. The current status of preclinical proton FLASH radiation and future directions. Med. Phys. 2022, 49, 2039–2054. [Google Scholar] [CrossRef]
- Adrian, G.; Ruan, J.L.; Paillas, S.; Cooper, C.R.; Petersson, K. In vitro assays for investigating the FLASH effect. Expert Rev. Mol. Med. 2022, 24, e10. [Google Scholar] [CrossRef]
- Rohrer Bley, C.; Wolf, F.; Gonçalves Jorge, P.; Grilj, V.; Petridis, I.; Petit, B.; Böhlen, T.T.; Moeckli, R.; Limoli, C.; Bourhis, J.; et al. Dose-and volume-limiting late toxicity of FLASH radiotherapy in cats with squamous cell carcinoma of the nasal planum and in mini pigs. Clin. Cancer Res. 2022, 28, 3814–3823. [Google Scholar] [CrossRef]
- Durante, M.; Bräuer-Krisch, E.; Hill, M. Faster and safer? FLASH UHDR in radiotherapy. Br. J. Radiol. 2018, 91, 20170628. [Google Scholar]
- Jolly, S.; Owen, H.; Schippers, M.; Welsch, C. Technical challenges for FLASH proton therapy. Phys. Med. 2020, 78, 71–82. [Google Scholar] [CrossRef]
- Bourhis, J.; Montay-Gruel, P.; Jorge, P.G.; Bailat, C.; Petit, B.; Ollivier, J.; Jeanneret-Sozzi, W.; Ozsahin, M.; Bochud, F.; Moeckli, R.; et al. Clinical translation of FLASH radiotherapy: Why and how? Radiother. Oncol. 2019, 139, 11–17. [Google Scholar] [CrossRef]
- Montay-Gruel, P.; Acharya, M.M.; Petersson, K.; Alikhani, L.; Yakkala, C.; Allen, B.D.; Ollivier, J.; Petit, B.; Jorge, P.G.; Syage, A.R.; et al. Long-term neurocognitive benefits of FLASH radiotherapy driven by reduced reactive oxygen species. Proc. Natl. Acad. Sci. USA 2019, 116, 10943–10951. [Google Scholar] [CrossRef] [Green Version]
- Abolfath, R.; Grosshans, D.; Mohan, R. Oxygen depletion in FLASH ultra-high-dose-rate radiotherapy: A molecular dynamics simulation. Med. Phys. 2020, 47, 6551–6561. [Google Scholar] [CrossRef]
- Cao, X.; Zhang, R.; Esipova, T.V.; Allu, S.R.; Ashraf, R.; Rahman, M.; Gunn, J.R.; Bruza, P.; Gladstone, D.J.; Williams, B.B.; et al. Quantification of oxygen depletion during FLASH irradiation in vitro and in vivo. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 240–248. [Google Scholar] [CrossRef]
- Perstin, A.; Poirier, Y.; Sawant, A.; Tambasco, M. Quantifying the DNA-damaging effects of FLASH irradiation with plasmid DNA. Int. J. Radiat. Oncol. Biol. Phys. 2022, 113, 437–447. [Google Scholar] [CrossRef]
- Liew, H.; Mein, S.; Dokic, I.; Haberer, T.; Debus, J.; Abdollahi, A.; Mairani, A. Deciphering time-dependent DNA damage complexity, repair, and oxygen tension: A mechanistic model for FLASH-dose-rate radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 574–586. [Google Scholar] [CrossRef]
- Tinganelli, W.; Sokol, O.; Quartieri, M.; Puspitasari, A.; Dokic, I.; Abdollahi, A.; Durante, M.; Haberer, T.; Debus, J.; Boscolo, D.; et al. UHDR (FLASH) carbon ion irradiation: Dosimetry and first cell experiments. Int. J. Radiat. Oncol. Biol. Phys. 2022, 112, 1012–1022. [Google Scholar] [CrossRef]
- Adrian, G.; Konradsson, E.; Lempart, M.; Bäck, S.; Ceberg, C.; Petersson, K. The FLASH effect depends on oxygen concentration. Br. J. Radiol. 2020, 92, 20190702. [Google Scholar] [CrossRef]
- Kranzer, R.; Poppinga, D.; Weidner, J.; Schüller, A.; Hackel, T.; Looe, H.K.; Poppe, B. Ion collection efficiency of ionization chambers in ultra-high dose-per-pulse electron beams. Med. Phys. 2021, 48, 819–830. [Google Scholar] [CrossRef]
- Jansen, J.; Knoll, J.; Beyreuther, E.; Pawelke, J.; Skuza, R.; Hanley, R.; Brons, S.; Pagliari, F.; Seco, J. Does FLASH deplete oxygen? Experimental evaluation for photons, protons, and carbon ions. Med. Phys. 2021, 48, 3982–3990. [Google Scholar] [CrossRef]
- Boscolo, D.; Scifoni, E.; Durante, M.; Krämer, M.; Fuss, M.C. May oxygen depletion explain the FLASH effect? A chemical track structure analysis. Radiother. Oncol. 2021, 162, 68–75. [Google Scholar] [CrossRef]
- Labarbe, R.; Hotoiu, L.; Barbier, J.; Favaudon, V. A physicochemical model of reaction kinetics supports peroxyl radical recombination as the main determinant of the FLASH effect. Radiother. Oncol. 2020, 153, 303–310. [Google Scholar] [CrossRef]
- Zhou, G. Mechanisms underlying FLASH radiotherapy, a novel way to enlarge the differential responses to ionizing radiation between normal and tumour tissues. Radiat. Med. Prot. 2020, 1, 35–40. [Google Scholar] [CrossRef]
- Beyreuther, E.; Brand, M.; Hans, S.; Hideghéty, K.; Karsch, L.; Leßmann, E.; Schürer, M.; Szabó, E.R.; Pawelke, J. Feasibility of proton FLASH effect tested by zebrafish embryo irradiation. Radiother. Oncol. 2019, 139, 46–50. [Google Scholar] [CrossRef]
- Spitz, D.R.; Buettner, G.R.; Petronek, M.S.; St-Aubin, J.J.; Flynn, R.T.; Waldron, T.J.; Limoli, C.L. An integrated physico-chemical approach for explaining the differential impact of FLASH versus conventional dose rate irradiation on cancer and normal tissue responses. Radiother. Oncol. 2019, 139, 23–27. [Google Scholar] [CrossRef]
- Zhu, H.; Xie, D.; Yang, Y.; Huang, S.; Gao, X.; Peng, Y.; Wang, B.; Wang, J.; Xiao, D.; Wu, D.; et al. Radioprotective effect of X-ray abdominal FLASH irradiation: Adaptation to oxidative damage and inflammatory response may be benefiting factors. Med. Phys. 2022, 49, 4812–4822. [Google Scholar] [CrossRef]
- Velalopoulou, A.; Karagounis, I.V.; Cramer, G.M.; Kim, M.M.; Skoufos, G.; Goia, D.; Hagan, S.; Verginadis, I.I.; Shoniyozov, K.; Chiango, J.; et al. FLASH proton radiotherapy spares normal epithelial and mesenchymal tissues while preserving sarcoma response. Cancer Res. 2021, 81, 4808–4821. [Google Scholar] [CrossRef]
- Moon, E.J.; Petersson, K.; Olcina, M.M. The importance of hypoxia in radiotherapy for the immune response, metastatic potential and FLASH-RT. Int. J. Radiat. Biol. 2022, 98, 439–451. [Google Scholar] [CrossRef]
- Jin, J.Y.; Gu, A.; Wang, W.; Oleinick, N.L.; Machtay, M. UHDR effect on circulating immune cells: A potential mechanism for FLASH effect? Radiother. Oncol. 2020, 149, 55–62. [Google Scholar] [CrossRef]
- Hughes, J.R.; Parsons, J.L. FLASH radiotherapy: Current knowledge and future insights using proton-beam therapy. Int. J. Mol. Sci. 2020, 21, 6492. [Google Scholar] [CrossRef]
- Samanta, S.; Mossahebi, S.; Miller, A.R. FLASH Radiotherapy. In Principles and Practice of Particle Therapy; Malouf TD and Trifiletti DM: Hoboken, NJ, USA, 2022; Chapter 8; pp. 115–120. [Google Scholar] [CrossRef]
- Arina, A.; Beckett, M.; Fernandez, C.; Zheng, W.; Pitroda, S.; Chmura, S.J.; Luke, J.J.; Forde, M.; Hou, Y.; Burnette, B.; et al. Tumour-reprogrammed resident T cells resist radiation to control tumours. Nat. Commun. 2019, 10, 3959. [Google Scholar] [CrossRef] [Green Version]
- Holmgaard, R.B.; Schaer, D.A.; Li, Y.; Castaneda, S.P.; Murphy, M.Y.; Xu, X.; Inigo, I.; Dobkin, J.; Manro, J.R.; Iversen, P.W.; et al. Targeting the TGFβ pathway with galunisertib, a TGFβRI small molecule inhibitor, promotes anti-tumour immunity leading to durable, complete responses, as monotherapy and in combination with checkpoint blockade. J. Immunother. Cancer 2018, 6, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Tauriello, D.V.; Sancho, E.; Batlle, E. Overcoming TGFβ-mediated immune evasion in cancer. Nat. Rev. Cancer 2022, 22, 25–44. [Google Scholar] [CrossRef]
- Fernet, V.; Ponette, E.; Deniaud-Alexandre, J.; Ménissier De-Murcia, G.; De Murcia, N.; Giocanti, F.; Megnin-Chanet, V.; Favaudon, M. Poly (ADP-ribose) polymerase, a major determinant of early cell response to ionizing radiation. Int. J. Radiat. Biol. 2000, 76, 1621–1629. [Google Scholar]
- Rama, N.; Saha, T.; Shukla, S.; Goda, C.; Milewski, D.; Mascia, A.E.; Vatner, R.E.; Sengupta, D.; Katsis, A.; Abel, E.; et al. Improved tumour control through t-cell infiltration modulated by UHDR proton FLASH using a clinical pencil beam scanning proton system. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, S164–S165. [Google Scholar] [CrossRef]
- Zhang, Y.; Ding, Z.; Perentesis, J.P.; Khuntia, D.; Pfister, S.X.; Sharma, R.A. Can rational combination of UHDR FLASH radiotherapy with immunotherapy provide a novel approach to cancer treatment? Clin. Oncol. 2021, 33, 713–722. [Google Scholar] [CrossRef]
- Soto, L.A.; Casey, K.M.; Wang, J.; Blaney, A.; Manjappa, R.; Breitkreutz, D.; Skinner, L.; Dutt, S.; Ko, R.B.; Bush, K.; et al. FLASH irradiation results in reduced severe skin toxicity compared to conventional-dose-rate irradiation. Radiat. Res. 2020, 194, 618–624. [Google Scholar] [CrossRef]
- Cunningham, S.; McCauley, S.; Vairamani, K.; Speth, J.; Girdhani, S.; Abel, E.; Sharma, R.A.; Perentesis, J.P.; Wells, S.I.; Mascia, A.; et al. FLASH proton pencil beam scanning irradiation minimizes radiation-induced leg contracture and skin toxicity in mice. Cancers 2021, 13, 1012. [Google Scholar] [CrossRef]
- Buonanno, M.; Grilj, V.; Brenner, D.J. Biological effects in normal cells exposed to FLASH dose rate protons. Radiother. Oncol. 2019, 139, 51–55. [Google Scholar] [CrossRef]
- Zlobinskaya, O.; Siebenwirth, C.; Greubel, C.; Hable, V.; Hertenberger, R.; Humble, N.; Reinhardt, S.; Michalski, D.; Röper, B.; Multhoff, G.; et al. The effects of UHDR proton irradiation on growth delay in the treatment of human tumour xenografts in nude mice. Radiat. Res. 2014, 181, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Friedl, A.A.; Prise, K.M.; Butterworth, K.T.; Montay-Gruel, P.; Favaudon, V. Radiobiology of the FLASH effect. Med. Phys. 2022, 49, 1993–2013. [Google Scholar] [CrossRef]
- Durante, M.; Yamada, S.; Ando, K.; Furusawa, Y.; Kawata, T.; Majima, H.; Nakano, T.; Tsujii, H. Measurements of the equivalent whole-body dose during radiation therapy by cytogenetic methods. Phys. Med. Biol. 1999, 44, 1289. [Google Scholar] [CrossRef]
- Simmons, D.A.; Lartey, F.M.; Schüler, E.; Rafat, M.; King, G.; Kim, A.; Ko, R.; Semaan, S.; Gonzalez, S.; Jenkins, M.; et al. Reduced cognitive deficits after FLASH irradiation of whole mouse brain are associated with less hippocampal dendritic spine loss and neuroinflammation. Radiother. Oncol. 2019, 139, 4–10. [Google Scholar] [CrossRef]
- Petersson, K.; Adrian, G.; Butterworth, K.; McMahon, S.J. A quantitative analysis of the role of oxygen tension in FLASH radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 539–547. [Google Scholar] [CrossRef]
- Alaghband, Y.; Cheeks, S.N.; Allen, B.D.; Montay-Gruel, P.; Doan, N.L.; Petit, B.; Jorge, P.G.; Giedzinski, E.; Acharya, M.M.; Vozenin, M.C.; et al. Neuroprotection of radiosensitive juvenile mice by UHDR FLASH irradiation. Cancers 2020, 12, 1671. [Google Scholar] [CrossRef]
- Froidevaux, P.; Grilj, V.; Bailat, C.; Geyer, W.R.; Bochud, F.; Vozenin, M.C. FLASH irradiation does not induce lipid peroxidation in lipids micelles and liposomes. Radiat. Phys. Chem. 2023, 205, 110733. [Google Scholar] [CrossRef]
- Cooper, C.R.; Jones, D.J.; Jones, G.D.; Petersson, K. Comet Assay Profiling of FLASH-Induced Damage: Mechanistic Insights into the Effects of FLASH Irradiation. Int. J. Mol. Sci. 2023, 24, 7195. [Google Scholar] [CrossRef]
- Zhang, G.; Zhang, Z.; Gao, W.; Quan, H. Treatment planning consideration for very high-energy electron FLASH radiotherapy. Phys. Med. 2023, 107, 102539. [Google Scholar] [CrossRef]
- Wuensch, W. The CHUV-CERN Facility for FLASH Treatment of Large, Deep-Seated Tumours: The DEFT (Deep Electron FLASH Therapy) Facility. In Proceedings of the FLASH Radiotherapy & Particle Therapy Conference, Barcelona, Spain, 1–3 December 2021. [Google Scholar]
- Maxim, P.G.; Tantawi, S.G.; Loo, B.W. PHASER: A platform for clinical translation of FLASH cancer radiotherapy. Radiother. Oncol. 2019, 139, 28–33. [Google Scholar] [CrossRef]
- Archer, J.; Li, E.; Davis, J.; Cameron, M.; Rosenfeld, A.; Lerch, M. High spatial resolution scintillator dosimetry of synchrotron microbeams. Sci. Rep. 2019, 9, 6873. [Google Scholar] [CrossRef] [Green Version]
- Annabell, N.; Yagi, N.; Umetani, K.; Wong, C.; Geso, M. Evaluating the peak-to-valley dose ratio of synchrotron microbeams using PRESAGE fluorescence. J. Synchrotron Radiat. 2012, 19, 332–339. [Google Scholar] [CrossRef]
- Dilmanian, F.A.; Krishnan, S.; Mclaughlin, W.E.; Lukaniec, B.; Baker, J.T.; Ailawadi, S.; Hirsch, K.N.; Cattell, R.F.; Roy, R.; Helfer, J. Merging orthovoltage x-ray minibeams spare the proximal tissues while producing a solid beam at the target. Sci. Rep. 2019, 9, 1198. [Google Scholar] [CrossRef]
- Prezado, Y.; Martínez-Rovira, I.; Thengumpallil, S.; Deman, P. Dosimetry protocol for the preclinical trials in white-beam minibeam radiation therapy. Med. Phys. 2011, 38, 5012–5020. [Google Scholar] [CrossRef]
- Uyama, A.; Kondoh, T.; Nariyama, N.; Umetani, K.; Fukumoto, M.; Shinohara, K.; Kohmura, E. A narrow microbeam is more effective for tumour growth suppression than a wide microbeam: An in vivo study using implanted human glioma cells. J. Synchrotron Radiat. 2011, 18, 671–678. [Google Scholar] [CrossRef] [Green Version]
- Dilmanian, F.A.; Button, T.M.; Le Duc, G.; Zhong, N.; Peña, L.A.; Smith, J.A.; Martinez, S.R.; Bacarian, T.; Tammam, J.; Ren, B.; et al. Response of rat intracranial 9L gliosarcoma to microbeam radiation therapy. Neuro-Oncology 2002, 4, 26–38. [Google Scholar] [CrossRef]
- Rackwitz, T.; Debus, J. Clinical applications of proton and carbon ion therapy. In Seminars in Oncology; WB Saunders: Philadelphia, PA, USA, 2019; Volume 46, pp. 226–232. [Google Scholar]
- Jongen, Y. Radiotherapy systems using proton and carbon beams. Bull. Et Mémoires De L’académie R. De Médecine De Belg. 2008, 163, 471–478. [Google Scholar]
- Schippers, J.M. Beam delivery systems for particle radiation therapy: Current status and recent developments. Rev. Accel. Sci. Technol. 2009, 2, 179–200. [Google Scholar] [CrossRef]
- Lazar, A.A.; Schulte, R.; Faddegon, B.; Blakely, E.A.; Roach, M., III. Clinical trials involving carbon-ion radiation therapy and the path forward. Cancer 2018, 124, 4467–4476. [Google Scholar] [CrossRef] [Green Version]
- Akakura, K.; Tsujii, H.; Morita, S.; Tsuji, H.; Yagishita, T.; Isaka, S.; Ito, H.; Akaza, H.; Hata, M.; Fujime, M.; et al. Phase I/II clinical trials of carbon ion therapy for prostate cancer. Prostate 2004, 58, 252–258. [Google Scholar] [CrossRef]
- Kamada, T.; Tsujii, H.; Blakely, E.A.; Debus, J.; De Neve, W.; Durante, M.; Jäkel, O.; Mayer, R.; Orecchia, R.; Pötter, R.; et al. Carbon ion radiotherapy in Japan: An assessment of 20 years of clinical experience. Lancet Oncol. 2015, 16, e93–e100. [Google Scholar] [CrossRef] [Green Version]
- Favaudon, V.; Lentz, J.M.; Heinrich, S.; Patriarca, A.; de Marzi, L.; Fouillade, C.; Dutreix, M. Time-resolved dosimetry of pulsed electron beams in very high dose-rate, FLASH irradiation for radiotherapy preclinical studies. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2019, 944, 162537. [Google Scholar] [CrossRef]
- Schüler, E.; Trovati, S.; King, G.; Lartey, F.; Rafat, M.; Villegas, M.; Praxel, A.J.; Loo, B.W., Jr.; Maxim, P.G. Experimental platform for UHDR FLASH irradiation of small animals using a clinical linear accelerator. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 195–203. [Google Scholar] [CrossRef]
- Bazalova-Carter, M.; Liu, M.; Palma, B.; Dunning, M.; McCormick, D.; Hemsing, E.; Nelson, J.; Jobe, K.; Colby, E.; Koong, A.C.; et al. Comparison of film measurements and Monte Carlo simulations of dose delivered with very high-energy electron beams in a polystyrene phantom. Med. Phys. 2015, 42, 1606–1613. [Google Scholar] [CrossRef]
- Crosbie, J.C.; Fournier, P.; Bartzsch, S.; Donzelli, M.; Cornelius, I.; Stevenson, A.W.; Requardt, H.; Bräuer-Krisch, E. Energy spectra considerations for synchrotron radiotherapy trials on the ID17 bio-medical beamline at the European Synchrotron Radiation Facility. J. Synchrotron Radiat. 2015, 22, 1035–1041. [Google Scholar] [CrossRef] [Green Version]
- Darafsheh, A.; Hao, Y.; Zwart, T.; Wagner, M.; Catanzano, D.; Williamson, J.F.; Knutson, N.; Sun, B.; Mutic, S.; Zhao, T. Feasibility of proton FLASH irradiation using a synchrocyclotron for preclinical studies. Med. Phys. 2020, 47, 4348–4355. [Google Scholar] [CrossRef]
- Romano, F.; Bailat, C.; Jorge, P.G.; Lerch, M.L.; Darafsheh, A. Ultra-high dose rate dosimetry: Challenges and opportunities for FLASH radiation therapy. Med. Phys. 2022, 49, 4912–4932. [Google Scholar] [CrossRef]
- Ashraf, M.R.; Rahman, M.; Zhang, R.; Williams, B.B.; Gladstone, D.J.; Pogue, B.W.; Bruza, P. Dosimetry for FLASH radiotherapy: A review of tools and the role of radioluminescence and Cherenkov emission. Front. Phys. 2020, 8, 328. [Google Scholar] [CrossRef]
- Chow, J.C.; Leung, M.K. Monte Carlo simulation of MOSFET dosimeter for electron backscatter using the GEANT4 code. Med. Phys. 2008, 35 6 Pt 1, 2383–2390. [Google Scholar] [CrossRef]
- Esplen, N.; Mendonca, M.S.; Bazalova-Carter, M. Physics and biology of ultrahigh dose-rate (FLASH) radiotherapy: A topical review. Phys. Med. Biol. 2020, 65, 23TR03. [Google Scholar] [CrossRef]
- Lourenço, A.; Subiel, A.; Lee, N.; Flynn, S.; Cotterill, J.; Shipley, D.; Romano, F.; Speth, J.; Lee, E.; Zhang, Y.; et al. Absolute dosimetry for FLASH proton pencil beam scanning radiotherapy. Sci. Rep. 2023, 13, 2054. [Google Scholar] [CrossRef]
- Karsch, L.; Beyreuther, E.; Burris-Mog, T.; Kraft, S.; Richter, C.; Zeil, K. Dose rate dependence for different dosimeters and detectors: TLD, OSL, EBT films, and diamond detectors. Med. Phys. 2012, 39, 2447. [Google Scholar] [CrossRef]
- Ahmed, M.F.; Shrestha, N.; Ahmad, S.; Schnell, E.; Akselrod, M.S.; Yukihara, E.G. Demonstration of 2D dosimetry using Al2O3 optically stimulated luminescence films for therapeutic megavoltage x-ray and ion beams. Radiat. Meas. 2017, 106, 315. [Google Scholar] [CrossRef]
- Rahman, M.; Trigilio, A.; Franciosini, G.; Moeckli, R.; Zhang, R.; Böhlen, T.T. FLASH radiotherapy treatment planning and models for electron beams. Radiother. Oncol. 2022, 175, 210–221. [Google Scholar] [CrossRef]
- van Marlen, P.; Dahele, M.; Folkerts, M.; Abel, E.; Slotman, B.J.; Verbakel, W.F. Bringing FLASH to the clinic: Treatment planning considerations for ultrahigh dose-rate proton beams. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 621–629. [Google Scholar] [CrossRef]
- Wu, Y.; No, H.J.; Breitkreutz, D.Y.; Mascia, A.E.; Moeckli, R.; Bourhis, J.; Schüler, E.; Maxim, P.G.; Loo, B.W., Jr. Technological basis for clinical trials in FLASH radiation therapy: A review. Appl. Rad. Oncol. 2021, 10, 6–14. [Google Scholar] [CrossRef]
Figure 1.
Schematic diagram showing initial physical, chemical, and biological processes that occur after cells and tissues are exposed to radiation. In this context, conventional radiotherapy interferes with both the chemical and biological processes, whereas Flash-RT does not interact with the biochemical steps, allowing it to bypass these processes.
Figure 1.
Schematic diagram showing initial physical, chemical, and biological processes that occur after cells and tissues are exposed to radiation. In this context, conventional radiotherapy interferes with both the chemical and biological processes, whereas Flash-RT does not interact with the biochemical steps, allowing it to bypass these processes.


{kind=link}
Table 1.
Comparison between conventional and Flash radiotherapy. ROS: reactive oxygen species.
| Conventional Radiotherapy | Flash Radiotherapy | |
|---|---|---|
| Radiation type | X-ray, gamma-ray, electron, proton, heavy-ion | X-ray, electron, proton, heavy-ion |
| Dose rate (Gy/s) | 0.001–0.4 | >40 |
| Irradiation time (s) | >120 | <1 |
| Tumour control | Efficient | Efficient |
| Normal tissue complication | High | Low |
| Mechanism | Repair, re-oxygenation, redistribution, repopulation, oxygen depletion, ROS | Oxygen depletion, ROS, immunoinflammatory response |
Table 2.
Various studies on mechanism of Flash radiotherapy.
| References | Mechanism | Radiation | System | Dose (Gy) | Dose Rate (Gy/s) |
|---|---|---|---|---|---|
| Petersson et al., 2020 [78] | Oxygen effect | Electrons | In vitro and in vivo | 0–30 | 0–100 |
| Labarbe et al., 2020 [27] | ROS | Electrons or photons | In vitro | 10 | 10−3–107 |
| Liew et al., 2021 [49] | Mechanistic radiobiological model | Electrons and photons | In vitro and in vivo | 2–32 | 10−2–104 |
| Cao et al., 2021 [47] | Oxygen effect | Electrons | In vitro and in vivo | 0–30 | 0–300 |
| Boscolo et al., 2021 [54] | Oxygen effect | Electrons | In vitro | 0–150 | 109 |
| Jansen et al., 2021 [53] | Oxygen effect | Photons, protons, and carbon ions | In vitro | 10 | 0–340 |
| Tinganelli et al., 2022 [35] | Oxygen effect | Ions | In vitro | 0–7.5 | 0–70 |
| Alaghband et al., 2023 [79] | Inflammatory response | Electrons | In vitro | 30 | 5.6 × 106 |
| Zhang et al., 2023 [26] | Oxygen effect | Protons | In vitro | 25–30 | 130 |
| Froidevaux et al., 2023 [80] | ROS | Electrons | In vivo | 5 | 107 |
| Cooper et al., 2023 [81] | Oxygen effect | Electrons | In vivo | 20 | 2 × 103 |
Table 3.
Various Flash radiation sources with their type, energy, and mean and instantaneous dose rates.
Table 3.
Various Flash radiation sources with their type, energy, and mean and instantaneous dose rates.
| Source | Radiation Type | Energy (MeV) | Mean Dose Rate (Gy/s) | Instantaneous Dose Rate (Gy/s) |
|---|---|---|---|---|
| Kinetron [97] | Electrons | 4.5 | 1000 | 2 × 107 |
| Varian 21 EX [98] | Electrons | 9 | 900 | 1.7 × 106 |
| NLCTA [99] | VHEEs | 120 | 90 | 9 × 1012 |
| ESRF [100] | X-rays | 0.102 | 37 | 18 × 103 |
| HyperScan [101] | Protons | 230 | 200 | 13 × 103 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chow, J.C.L.; Ruda, H.E. Flash Radiotherapy: Innovative Cancer Treatment. Encyclopedia 2023, 3, 808-823. https://doi.org/10.3390/encyclopedia3030058
AMA Style
Chow JCL, Ruda HE. Flash Radiotherapy: Innovative Cancer Treatment. Encyclopedia. 2023; 3(3):808-823. https://doi.org/10.3390/encyclopedia3030058
Chicago/Turabian StyleChow, James C. L., and Harry E. Ruda. 2023. "Flash Radiotherapy: Innovative Cancer Treatment" Encyclopedia 3, no. 3: 808-823. https://doi.org/10.3390/encyclopedia3030058