
Selective Change in the Bacteria Cultured and Isolated in Respiratory Sputum from Elderly Patients during the SARS-CoV-2 Pandemic

Abstract
:1. Introduction
2. Method
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Binns, E.; Koenraads, M.; Hristeva, L.; Flamant, A.; Baier-Grabner, S.; Loi, M.; Lempainen, J.; Osterheld, E.; Ramly, B.; Chakakala-Chaziya, J.; et al. Influenza and respiratory syncytial virus during the COVID-19 pandemic: Time for a new paradigm? Pediatr. Pulmonol. 2022, 57, 38–42. [Google Scholar] [CrossRef]
- Dhanasekaran, V.; Sullivan, S.; Edwards, K.M.; Xie, R.; Khvorov, A.; Valkenburg, S.A.; Cowling, B.J.; Barr, I.G. Human seasonal influenza under COVID-19 and the potential consequences of influenza lineage elimination. Nat. Commun. 2022, 13, 1721. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Xu, C.; Huang, W.; Xu, X.; Xie, W.; Long, X. The incidence of influenza in children was decreased in the first flu season after COVID-19 pandemic in Wuhan. J. Infect. Public Health 2021, 14, 1279–1281. [Google Scholar] [CrossRef]
- Chiu, N.C.; Chi, H.; Tai, Y.L.; Peng, C.C.; Tseng, C.Y.; Chen, C.C.; Tan, B.F.; Lin, C.Y. Impact of Wearing Masks, Hand Hygiene, and Social Distancing on Influenza, Enterovirus, and All-Cause Pneumonia During the Coronavirus Pandemic: Retrospective National Epidemiological Surveillance Study. J. Med. Internet Res. 2020, 22, e21257. [Google Scholar] [CrossRef] [PubMed]
- Amin-Chowdhury, Z.; Aiano, F.; Mensah, A.; Sheppard, C.L.; Litt, D.; Fry, N.K.; Andrews, N.; Ramsay, M.E.; Ladhani, S.N. Impact of the Coronavirus Disease 2019 (COVID-19) Pandemic on Invasive Pneumococcal Disease and Risk of Pneumococcal Coinfection With Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Prospective National Cohort Study, England. Clin. Infect. Dis. 2021, 72, e65–e75. [Google Scholar] [CrossRef] [PubMed]
- Brueggemann, A.B.; Jansen van Rensburg, M.J.; Shaw, D.; McCarthy, N.D.; Jolley, K.A.; Maiden, M.C.J.; van der Linden, M.P.G.; Amin-Chowdhury, Z.; Bennett, D.E.; Borrow, R.; et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the Invasive Respiratory Infection Surveillance Initiative: A prospective analysis of surveillance data. Lancet Digit. Health 2021, 3, e360–e370. [Google Scholar] [CrossRef]
- Chan, K.F.; Ma, T.F.; Ip, M.S.; Ho, P.L. Invasive pneumococcal disease, pneumococcal pneumonia and all-cause pneumonia in Hong Kong during the COVID-19 pandemic compared with the preceding 5 years: A retrospective observational study. BMJ Open 2021, 11, e055575. [Google Scholar] [CrossRef]
- Dirkx, K.K.T.; Mulder, B.; Post, A.S.; Rutten, M.H.; Swanink, C.M.A.; Wertheim, H.F.L.; Cremers, A.J.H. The drop in reported invasive pneumococcal disease among adults during the first COVID-19 wave in the Netherlands explained. Int. J. Infect. Dis. 2021, 111, 196–203. [Google Scholar] [CrossRef]
- Takashita, E.; Kawakami, C.; Momoki, T.; Saikusa, M.; Shimizu, K.; Ozawa, H.; Kumazaki, M.; Usuku, S.; Tanaka, N.; Okubo, I.; et al. Increased risk of rhinovirus infection in children during the coronavirus disease-19 pandemic. Influenza Other Respir. Viruses 2021, 15, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Champredon, D.; Bancej, C.; Lee, L.; Buckrell, S. Implications of the unexpected persistence of human rhinovirus/enterovirus during the COVID-19 pandemic in Canada. Influenza Other Respir. Viruses 2022, 16, 190–192. [Google Scholar] [CrossRef] [PubMed]
- Merenstein, C.; Liang, G.; Whiteside, S.A.; Cobián-Güemes, A.G.; Merlino, M.S.; Taylor, L.J.; Glascock, A.; Bittinger, K.; Tanes, C.; Graham-Wooten, J.; et al. Signatures of COVID-19 Severity and Immune Response in the Respiratory Tract Microbiome. mBio 2021, 12, e0177721. [Google Scholar] [CrossRef] [PubMed]
- Geckler, R.W.; Gremillion, D.H.; McAllister, C.K.; Ellenbogen, C. Microscopic and bacteriological comparison of paired sputa and transtracheal aspirates. J. Clin. Microbiol. 1977, 6, 396–399. [Google Scholar] [CrossRef]
- Japanese Committee for Clinical Laboratory Standards. Available online: https://www.jccls.org/active/public2/ (accessed on 26 June 2023).
- CLSI. The Clinical and Laboratory Standards Institute. Available online: https://clsiorg/ (accessed on 26 June 2023).
- Okada, T.; Morozumi, M.; Sakata, H.; Takayanagi, R.; Ishiwada, N.; Sato, Y.; Oishi, T.; Tajima, T.; Haruta, T.; Kawamura, N.; et al. A practical approach estimating etiologic agents using real-time PCR in pediatric inpatients with community-acquired pneumonia. J. Infect. Chemother. 2012, 18, 832–840. [Google Scholar] [CrossRef]
- Borges, I.C.; Andrade, D.C.; Vilas-Boas, A.L.; Fontoura, M.S.; Laitinen, H.; Ekström, N.; Adrian, P.V.; Meinke, A.; Cardoso, M.R.; Barral, A.; et al. Detection of antibody responses against Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis proteins in children with community-acquired pneumonia: Effects of combining pneumococcal antigens, pre-existing antibody levels, sampling interval, age, and duration of illness. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1551–1557. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Wong, A.H.C.; Hon, K.L. Community-Acquired Pneumonia in Children. Recent Pat. Inflamm. Allergy Drug Discov. 2018, 12, 136–144. [Google Scholar] [CrossRef]
- Ishiwada, N. Current situation and need for prevention of invasive pneumococcal disease and pneumococcal pneumonia in 6- to 64-year-olds in Japan. J. Infect. Chemother. 2021, 27, 7–18. [Google Scholar] [CrossRef]
- Suaya, J.A.; Fletcher, M.A.; Georgalis, L.; Arguedas, A.G.; McLaughlin, J.M.; Ferreira, G.; Theilacker, C.; Gessner, B.D.; Verstraeten, T. Identification of Streptococcus pneumoniae in hospital-acquired pneumonia in adults. J. Hosp. Infect. 2021, 108, 146–157. [Google Scholar] [CrossRef]
- Thomas, R.E. Pneumococcal Pneumonia and Invasive Pneumococcal Disease in Those 65 and Older: Rates of Detection, Risk Factors, Vaccine Effectiveness, Hospitalisation and Mortality. Geriatrics 2021, 6, 13. [Google Scholar] [CrossRef]
- Torres, A.; Ewig, S.; Lode, H.; Carlet, J.; For The European HAPwg. Defining, treating and preventing hospital acquired pneumonia: European perspective. Intensive Care Med. 2009, 35, 9–29. [Google Scholar] [CrossRef]
- Kollef, M.H.; Shorr, A.; Tabak, Y.P.; Gupta, V.; Liu, L.Z.; Johannes, R.S. Epidemiology and outcomes of health-care-associated pneumonia: Results from a large US database of culture-positive pneumonia. Chest 2005, 128, 3854–3862. [Google Scholar] [CrossRef] [PubMed]
- Nagasawa, M.; Nakagawa, R.; Sugita, Y.; Ono, E.; Yamaguchi, Y.; Kato, T.; Kajiwara, H.; Taki, R.; Harada, N. Investigation of Respiratory Viruses by the Multiplex PCR Method in the Community Suggested Reciprocal Virus Transmission between Children and Adults. J. Vaccines Vaccin. 2022, 13, S19. [Google Scholar] [CrossRef]
- Danino, D.; Ben-Shimol, S.; van der Beek, B.A.; Givon-Lavi, N.; Avni, Y.S.; Greenberg, D.; Weinberger, D.M.; Dagan, R. Decline in Pneumococcal Disease in Young Children During the Coronavirus Disease 2019 (COVID-19) Pandemic in Israel Associated With Suppression of Seasonal Respiratory Viruses, Despite Persistent Pneumococcal Carriage: A Prospective Cohort Study. Clin. Infect. Dis. 2022, 75, e1154–e1164. [Google Scholar] [CrossRef] [PubMed]
- Bertran, M.; Amin-Chowdhury, Z.; Sheppard, C.L.; Eletu, S.; Zamarreño, D.V.; Ramsay, M.E.; Litt, D.; Fry, N.K.; Ladhani, S.N. Increased Incidence of Invasive Pneumococcal Disease among Children after COVID-19 Pandemic, England. Emerg. Infect. Dis. 2022, 28, 1669–1672. [Google Scholar] [CrossRef] [PubMed]




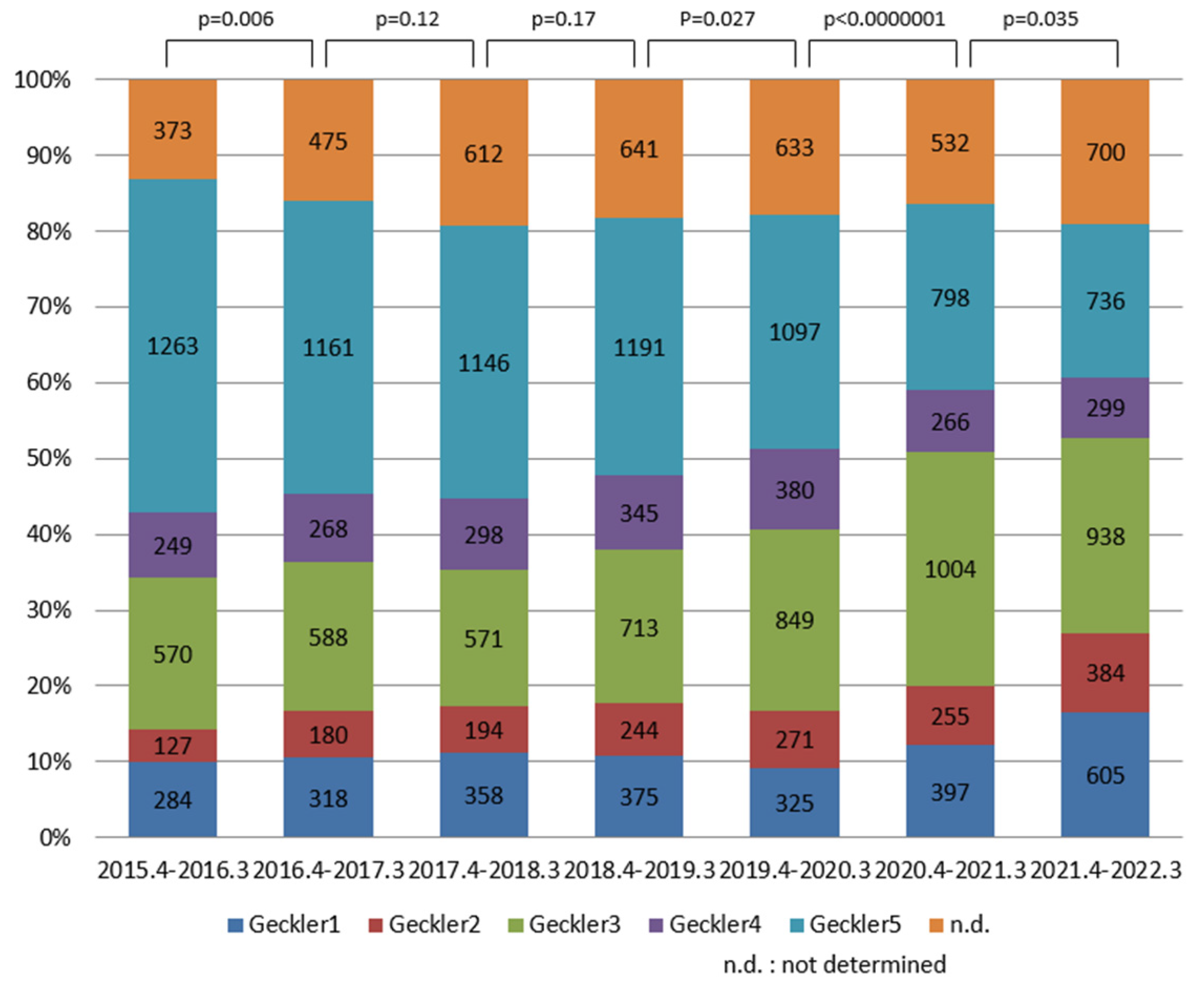{kind=link}
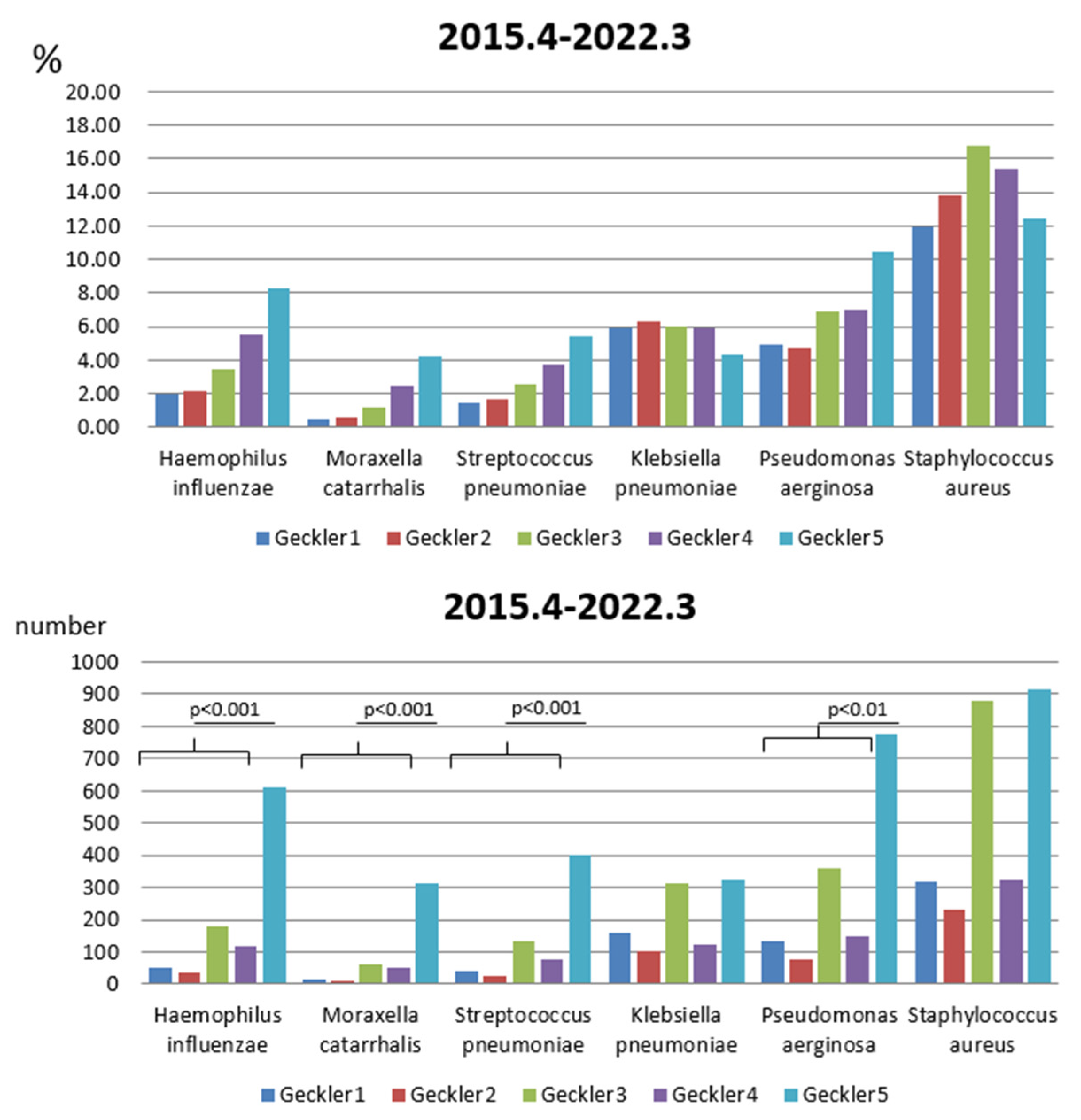{kind=link}
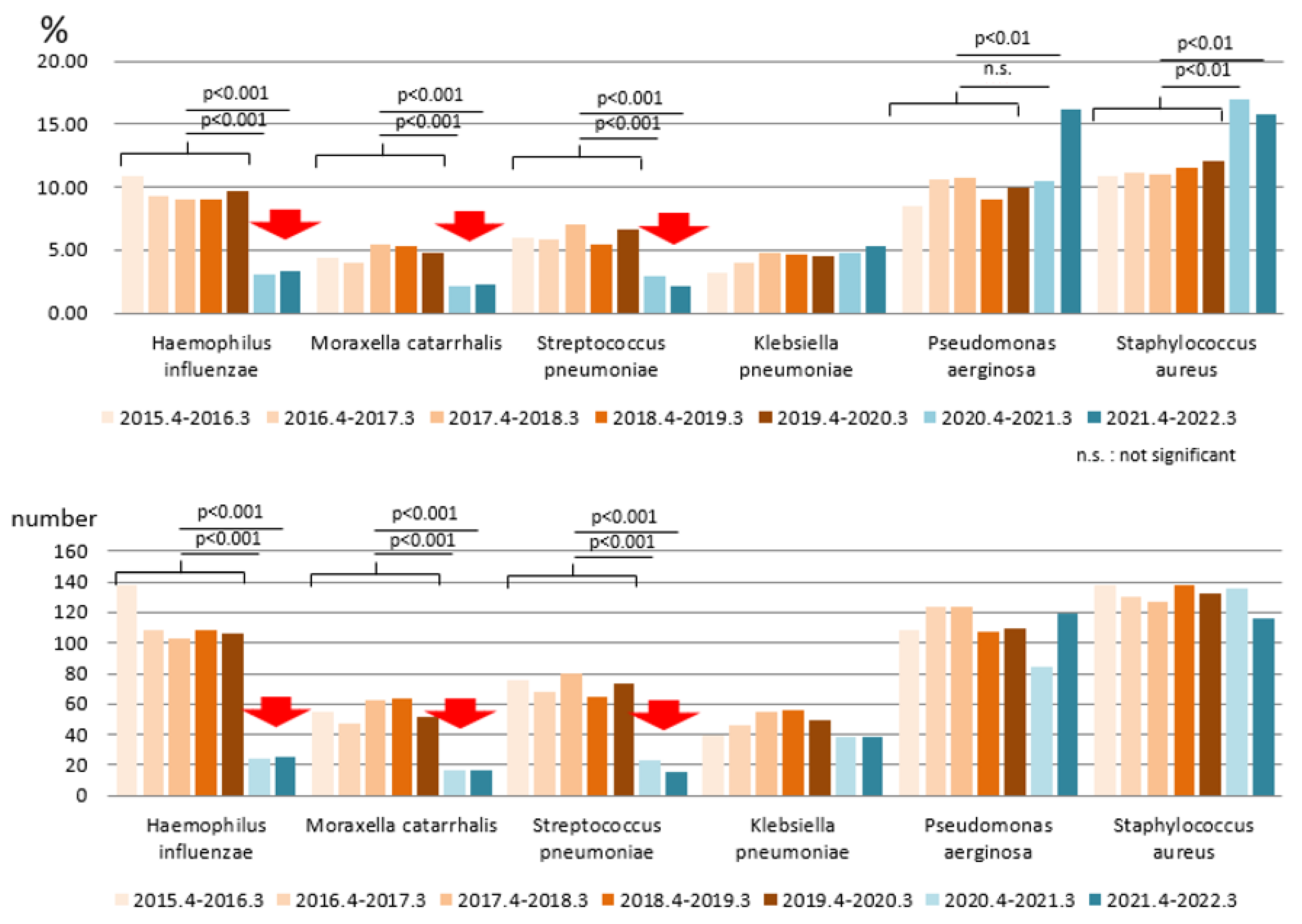{kind=link}
| 2015.4–2016.3 | 2016.4–2017.3 | 2017.4–2018.3 | 2018.4–2019.3 | 2019.4–2020.3 | 2020.4–2021.3 | 2021.4–2022.3 | |
|---|---|---|---|---|---|---|---|
| sample number | 2814 | 2960 | 3152 | 3498 | 3583 | 3456 | 3589 |
| average age(y) | 69.32 | 70.73 | 72.11 | 72.58 | 72.67 | 72.68 | 72.51 |
| median age (y) | 74 | 74 | 75 | 76 | 76 | 76 | 75 |
| SD (y) | 18.18 | 16.66 | 15.59 | 15.96 | 15.90 | 15.00 | 14.60 |
| female ratio | 0.37 | 0.39 | 0.36 | 0.42 | 0.43 | 0.37 | 0.39 |
| Age (y) | Sample Number | % |
|---|---|---|
| 0–14 | 95 | 0.4 |
| 15–19 | 104 | 0.5 |
| 20–29 | 382 | 1.7 |
| 30–39 | 618 | 2.7 |
| 40–49 | 1035 | 4.5 |
| 50–59 | 1831 | 7.9 |
| 60–69 | 3711 | 16.1 |
| 70–79 | 6987 | 30.3 |
| 80–89 | 6585 | 28.6 |
| 90–99 | 1669 | 7.2 |
| 100- | 35 | 0.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagasawa, M.; Kato, T.; Tanaka, I.; Ono, E. Selective Change in the Bacteria Cultured and Isolated in Respiratory Sputum from Elderly Patients during the SARS-CoV-2 Pandemic. Appl. Microbiol. 2023, 3, 1003-1012. https://doi.org/10.3390/applmicrobiol3030068
Nagasawa M, Kato T, Tanaka I, Ono E. Selective Change in the Bacteria Cultured and Isolated in Respiratory Sputum from Elderly Patients during the SARS-CoV-2 Pandemic. Applied Microbiology. 2023; 3(3):1003-1012. https://doi.org/10.3390/applmicrobiol3030068
Chicago/Turabian StyleNagasawa, Masayuki, Tomoyuki Kato, Ippei Tanaka, and Emi Ono. 2023. "Selective Change in the Bacteria Cultured and Isolated in Respiratory Sputum from Elderly Patients during the SARS-CoV-2 Pandemic" Applied Microbiology 3, no. 3: 1003-1012. https://doi.org/10.3390/applmicrobiol3030068