
Peripheral Blood CD8+ T-Lymphocyte Subsets Are Associated with Prognosis in Prostate Cancer Patients

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Blood Sample Collection
2.3. Flow Cytometry
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
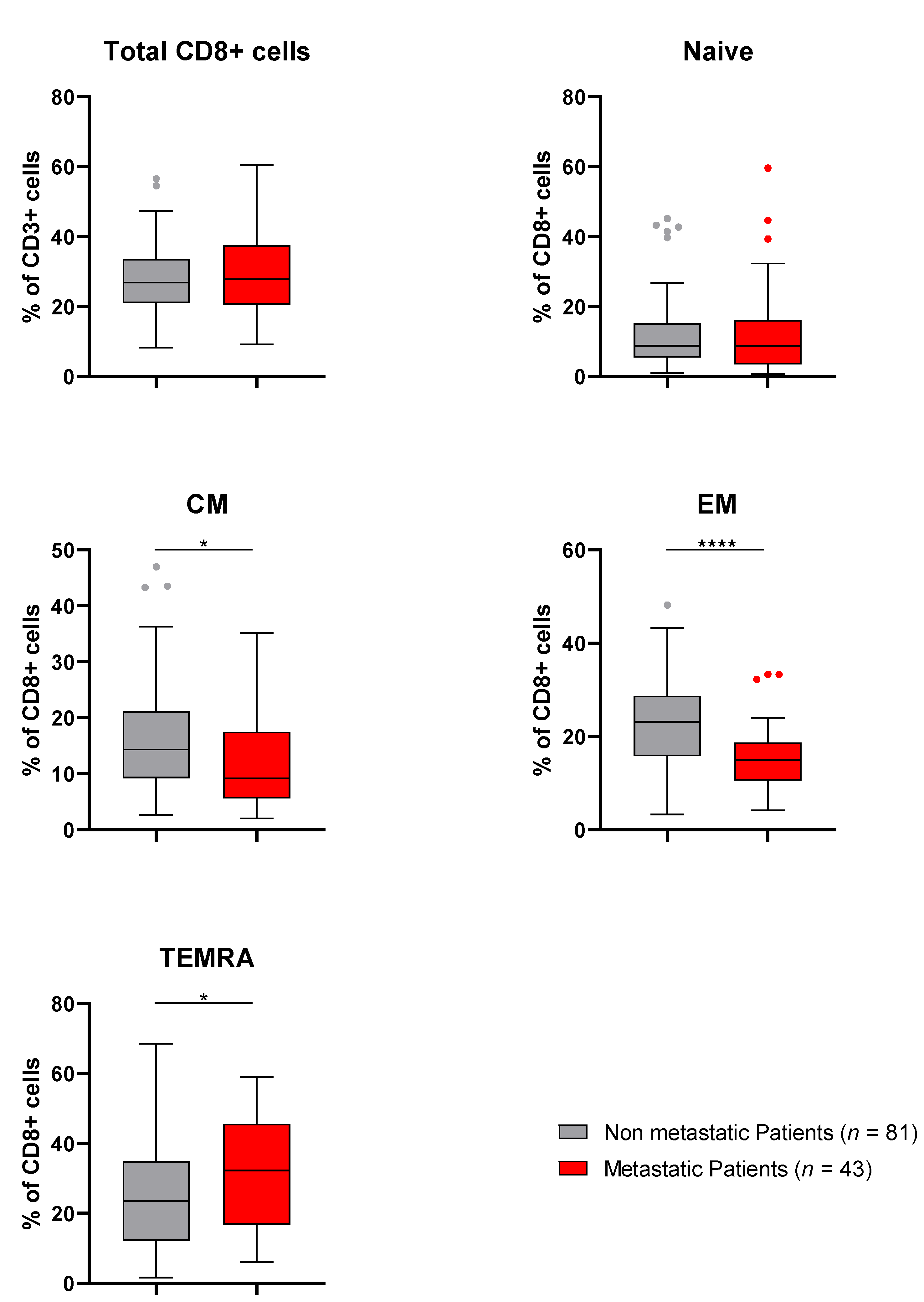
3.2. Comparison of CD8+ T-Lymphocyte Subsets between N-MD PCa and MD PCa Patients
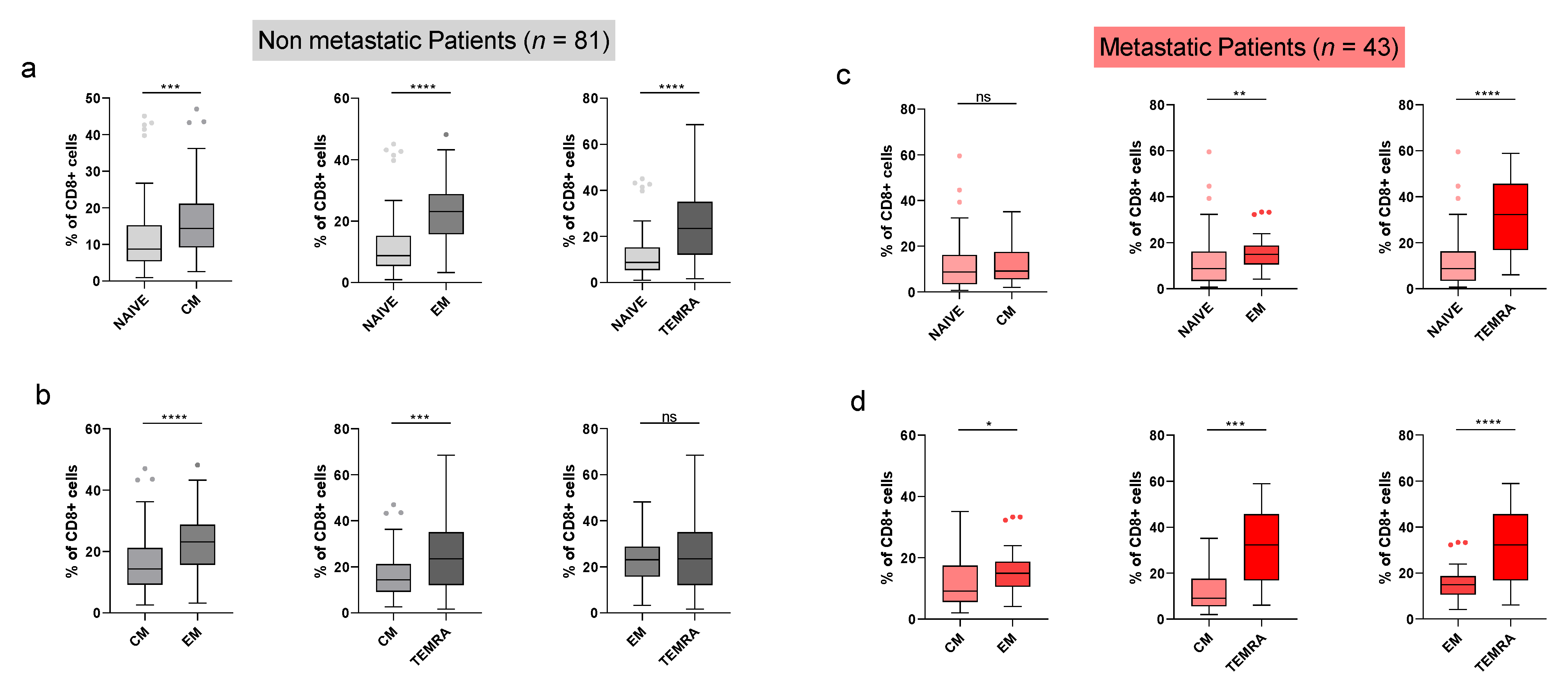
3.3. Intragroup Comparisons of CD8+ T-Lymphocyte Subsets
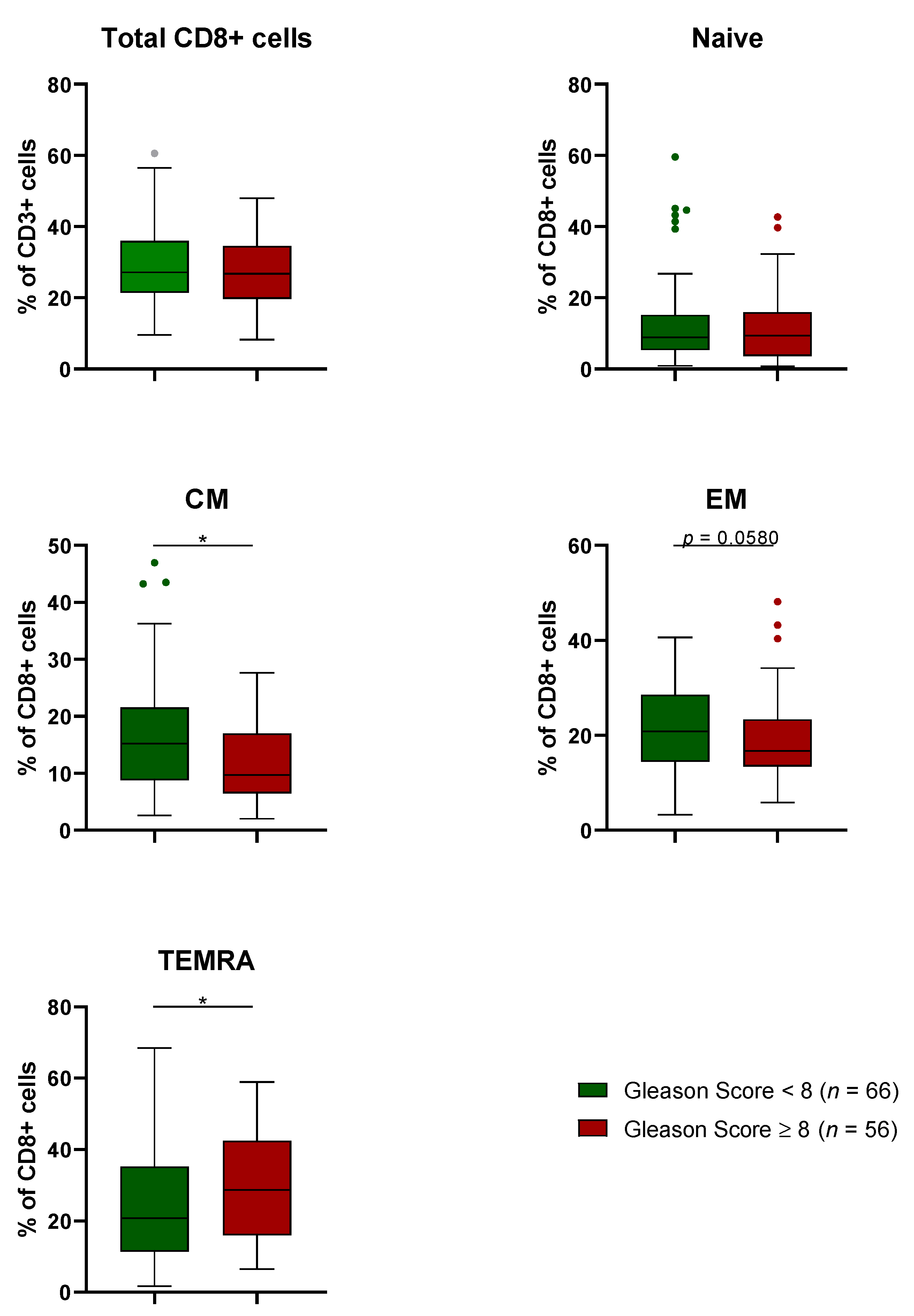
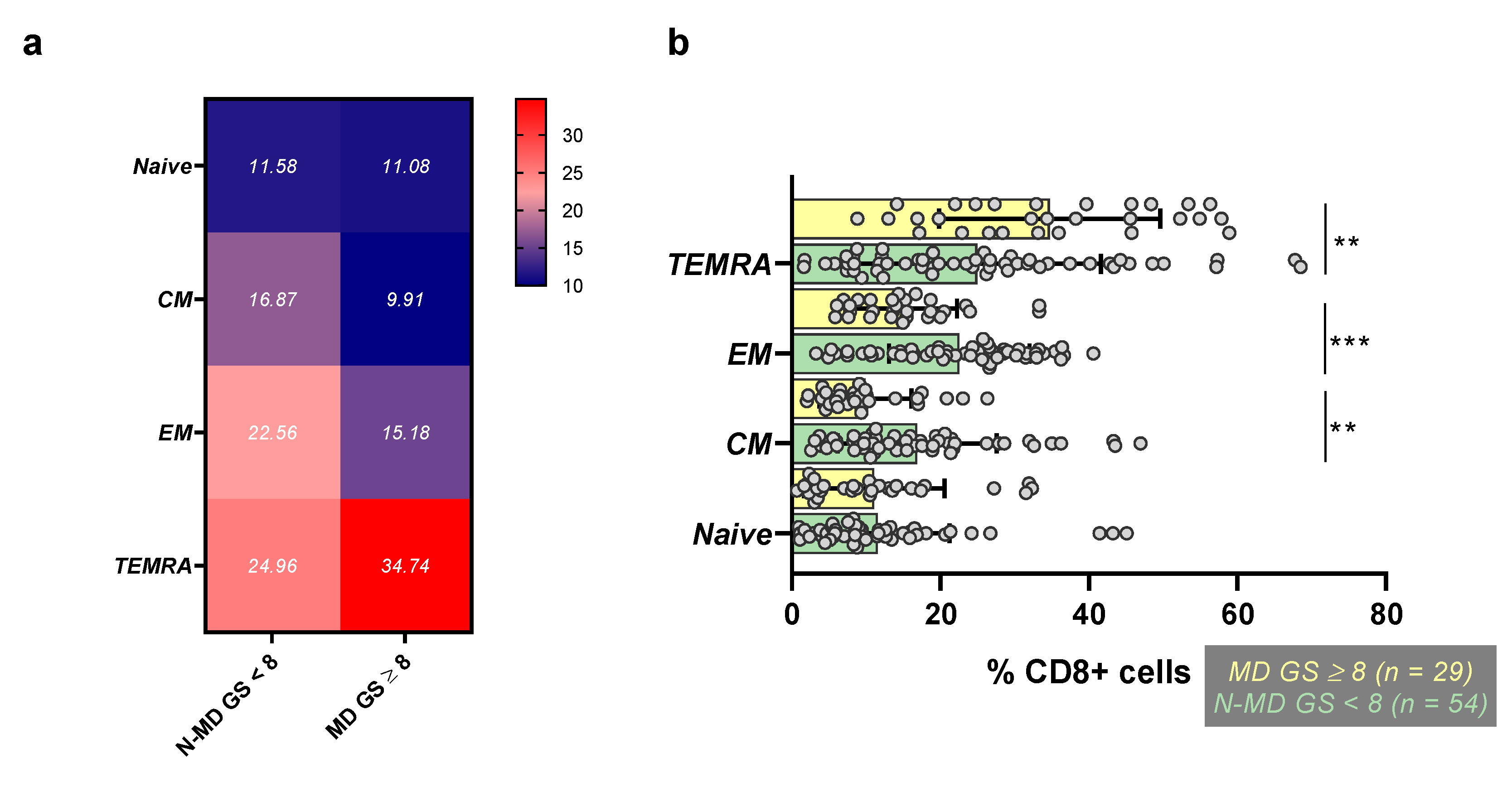
3.4. Comparison of CD8+ T-Lymphocyte Subsets based on Gleason Score (GS)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer immunoediting: Integrating immunity’s roles in cancer suppression and promotion. Science 2011, 331, 1565–1570. [Google Scholar] [CrossRef] [Green Version]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The immunobiology of cancer immunosurveillance and immunoediting. Immunity 2004, 21, 137–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, R.; Coxon, A.T.; Dunn, G.P. Therapeutic applications of the cancer immunoediting hypothesis. Semin. Cancer Biol. 2022, 78, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Baxevanis, C.N.; Voutsas, I.F.; Tsitsilonis, O.E.; Gritzapis, A.D.; Sotiriadou, R.; Papamichail, M. Tumor-specific CD4+ T lymphocytes from cancer patients are required for optimal induction of cytotoxic T cells against the autologous tumor. J. Immunol. 2000, 164, 3902–3912. [Google Scholar] [CrossRef] [Green Version]
- Sallusto, F.; Geginat, J.; Lanzavecchia, A. Central memory and effector memory T cell subsets: Function, generation, and maintenance. Annu. Rev. Immunol. 2004, 22, 745–763. [Google Scholar] [CrossRef]
- Saule, P.; Trauet, J.; Dutriez, V.; Lekeux, V.; Dessaint, J.P.; Labalette, M. Accumulation of memory T cells from childhood to old age: Central and effector memory cells in CD4(+) versus effector memory and terminally differentiated memory cells in CD8(+) compartment. Mech. Ageing Dev. 2006, 127, 274–281. [Google Scholar] [CrossRef]
- Buggert, M.; Price, D.A.; Mackay, L.K.; Betts, M.R. Human circulating and tissue-resident memory CD8(+) T cells. Nat. Immunol. 2023, 24, 1076–1086. [Google Scholar] [CrossRef]
- Sun, L.; Su, Y.; Jiao, A.; Wang, X.; Zhang, B. T cells in health and disease. Signal Transduct. Target. Ther. 2023, 8, 235. [Google Scholar] [CrossRef]
- Teramatsu, K.; Oono, T.; Oyama, K.; Fujimori, N.; Murakami, M.; Yasumori, S.; Ohno, A.; Matsumoto, K.; Takeno, A.; Nakata, K.; et al. Circulating CD8(+)CD122(+) T cells as a prognostic indicator of pancreatic cancer. BMC Cancer 2022, 22, 1134. [Google Scholar] [CrossRef]
- Larsson, A.M.; Nordström, O.; Johansson, A.; Rydén, L.; Leandersson, K.; Bergenfelz, C. Peripheral Blood Mononuclear Cell Populations Correlate with Outcome in Patients with Metastatic Breast Cancer. Cells 2022, 11, 1639. [Google Scholar] [CrossRef]
- Zhang, G.; Liu, A.; Yang, Y.; Xia, Y.; Li, W.; Liu, Y.; Zhang, J.; Cui, Q.; Wang, D.; Liu, X.; et al. Clinical predictive value of naïve and memory T cells in advanced NSCLC. Front. Immunol. 2022, 13, 996348. [Google Scholar] [CrossRef]
- Yuan, C.; Huang, J.; Li, H.; Zhai, R.; Zhai, J.; Fang, X.; Wu, Y. Association of clinical outcomes and the predictive value of T lymphocyte subsets within colorectal cancer patients. Front. Surg. 2023, 10, 1102545. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Shi, L.; Zhao, Z.; Du, P.; Ye, X.; Li, D.; Cai, Z.; Han, J.; Cai, J. Disruption of CTLA-4 expression on peripheral blood CD8 + T cell enhances anti-tumor efficacy in bladder cancer. Cancer Chemother. Pharmacol. 2019, 83, 911–920. [Google Scholar] [CrossRef]
- Yang, Y.; Attwood, K.; Bshara, W.; Mohler, J.L.; Guru, K.; Xu, B.; Kalinski, P.; Chatta, G. High intratumoral CD8(+) T-cell infiltration is associated with improved survival in prostate cancer patients undergoing radical prostatectomy. Prostate 2021, 81, 20–28. [Google Scholar] [CrossRef]
- McAllister, M.; Constâncio, V.; Patek, S.; Gan, H.W.G.; Bailey, P.; Wheadon, H.; Underwood, M.; Leung, H.; Edwards, J. Inflammatory infiltration is associated with AR expression and poor prognosis in hormone naïve prostate cancer. Prostate 2020, 80, 1353–1364. [Google Scholar] [CrossRef]
- McArdle, P.A.; Canna, K.; McMillan, D.C.; McNicol, A.M.; Campbell, R.; Underwood, M.A. The relationship between T-lymphocyte subset infiltration and survival in patients with prostate cancer. Br. J. Cancer 2004, 91, 541–543. [Google Scholar] [CrossRef]
- Andersen, L.B.; Nørgaard, M.; Rasmussen, M.; Fredsøe, J.; Borre, M.; Ulhøi, B.P.; Sørensen, K.D. Immune cell analyses of the tumor microenvironment in prostate cancer highlight infiltrating regulatory T cells and macrophages as adverse prognostic factors. J. Pathol. 2021, 255, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Mao, F.; Yang, C.; Luo, W.; Wang, Y.; Xie, J.; Wang, H. Peripheral blood lymphocyte subsets are associated with the clinical outcomes of prostate cancer patients. Int. Immunopharmacol. 2022, 113, 109287. [Google Scholar] [CrossRef]
- Derksen, L.Y.; Tesselaar, K.; Borghans, J.A.M. Memories that last: Dynamics of memory T cells throughout the body. Immunol. Rev. 2023, 316, 38–51. [Google Scholar] [CrossRef] [PubMed]
- Golubovskaya, V.; Wu, L. Different Subsets of T Cells, Memory, Effector Functions, and CAR-T Immunotherapy. Cancers 2016, 8, 36. [Google Scholar] [CrossRef] [Green Version]
- Rodems, T.S.; Heninger, E.; Stahlfeld, C.N.; Gilsdorf, C.S.; Carlson, K.N.; Kircher, M.R.; Singh, A.; Krueger, T.E.G.; Beebe, D.J.; Jarrard, D.F.; et al. Reversible epigenetic alterations regulate class I HLA loss in prostate cancer. Commun. Biol. 2022, 5, 897. [Google Scholar] [CrossRef] [PubMed]
- Bansal, D.; Reimers, M.A.; Knoche, E.M.; Pachynski, R.K. Immunotherapy and Immunotherapy Combinations in Metastatic Castration-Resistant Prostate Cancer. Cancers 2021, 13, 334. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.L. Immunotherapy in treatment of metastatic prostate cancer: An approach to circumvent immunosuppressive tumor microenvironment. Prostate 2021, 81, 1125–1134. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Li, Y.; Guo, Z.; Ma, X.; Li, Y.; Wei, X.; Han, D.; Zhang, T.; Chen, X.; Yan, C.; et al. Comparison of dynamic changes in the peripheral CD8(+) T cells function and differentiation in ESCC patients treated with radiotherapy combined with anti-PD-1 antibody or concurrent chemoradiotherapy. Front. Immunol. 2022, 13, 1060695. [Google Scholar] [CrossRef]
- Adorno Febles, V.R.; Hao, Y.; Ahsan, A.; Wu, J.; Qian, Y.; Zhong, H.; Loeb, S.; Makarov, D.V.; Lepor, H.; Wysock, J.; et al. Single-cell analysis of localized prostate cancer patients links high Gleason score with an immunosuppressive profile. Prostate 2023, 83, 840–849. [Google Scholar] [CrossRef]
- Unger, K.; Hess, J.; Link, V.; Buchner, A.; Eze, C.; Li, M.; Stief, C.; Kirchner, T.; Klauschen, F.; Zitzelsberger, H.; et al. DNA-methylation and genomic copy number in primary tumors and corresponding lymph node metastases in prostate cancer from patients with low and high Gleason score. Clin. Transl. Radiat. Oncol. 2023, 39, 100586. [Google Scholar] [CrossRef]
- Kane, N.; Romero, T.; Diaz-Perez, S.; Rettig, M.B.; Steinberg, M.L.; Kishan, A.U.; Schaue, D.; Reiter, R.E.; Knudsen, B.S.; Nickols, N.G. Significant changes in macrophage and CD8 T cell densities in primary prostate tumors 2 weeks after SBRT. Prostate Cancer Prostatic Dis. 2023, 26, 207–209. [Google Scholar] [CrossRef]
- Nickols, N.G.; Ganapathy, E.; Nguyen, C.; Kane, N.; Lin, L.; Diaz-Perez, S.; Nazarian, R.; Mathis, C.; Felix, C.; Basehart, V.; et al. The intraprostatic immune environment after stereotactic body radiotherapy is dominated by myeloid cells. Prostate Cancer Prostatic Dis. 2021, 24, 135–139. [Google Scholar] [CrossRef]
- Ollivier, L.; Labbé, M.; Fradin, D.; Potiron, V.; Supiot, S. Interaction Between Modern Radiotherapy and Immunotherapy for Metastatic Prostate Cancer. Front. Oncol. 2021, 11, 744679. [Google Scholar] [CrossRef]
- Zhu, S.; Wang, Y.; Tang, J.; Cao, M. Radiotherapy induced immunogenic cell death by remodeling tumor immune microenvironment. Front. Immunol. 2022, 13, 1074477. [Google Scholar] [CrossRef] [PubMed]
- Kubo, M.; Satoh, T.; Ishiyama, H.; Tabata, K.I.; Tsumura, H.; Komori, S.; Iwamura, M.; Baba, S.; Hayakawa, K.; Kawamura, T.; et al. Enhanced activated T cell subsets in prostate cancer patients receiving iodine-125 low-dose-rate prostate brachytherapy. Oncol. Rep. 2018, 39, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brusa, D.; Simone, M.; Gontero, P.; Spadi, R.; Racca, P.; Micari, J.; Degiuli, M.; Carletto, S.; Tizzani, A.; Matera, L. Circulating immunosuppressive cells of prostate cancer patients before and after radical prostatectomy: Profile comparison. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2013, 20, 971–978. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | ||
|---|---|---|
| Non Metastatic Disease (N-MD) at Enrolment | Metastatic Disease (MD) at Enrolment | |
| No. of PCa patients | 81 | 43 |
| Age (Median) | ||
| 68.7 | 68.6 | |
| Gleason Score | ||
| <8 | 54 (66.7%) | 12 (27.9%) |
| ≥8 | 27 (33.3%) | 29 (67.4%) |
| Missing | 0 | 2 (4.7%) |
| pT stage | ||
| T1c | 16 (19.8%) | - |
| T2a, T2b, T2c | 42 (51.9%) | - |
| T3a, T3b | 22 (27.1%) | - |
| Missing | 1 (1.2%) | - |
| Site of metastases at the time of blood sampling | ||
| Bone metastases | - | 19 (44.2%) |
| Soft tissue metastases | - | 11 (25.6%) |
| Bone metastases and soft tissue metastases | - | 13 (30.2%) |
| Type of therapy received at the time of blood sampling | ||
| RP | 32 (39.5%) | - |
| PRTX | 9 (11.1%) | - |
| BRACHY | 2 (2.5%) | - |
| ADT | - | 10 (23.3%) |
| ΝOΝΕ | 38 (46.9%) | 33 (76.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baxevanis, C.N.; Stokidis, S.; Goulielmaki, M.; Gritzapis, A.D.; Fortis, S.P. Peripheral Blood CD8+ T-Lymphocyte Subsets Are Associated with Prognosis in Prostate Cancer Patients. Onco 2023, 3, 165-174. https://doi.org/10.3390/onco3030012
Baxevanis CN, Stokidis S, Goulielmaki M, Gritzapis AD, Fortis SP. Peripheral Blood CD8+ T-Lymphocyte Subsets Are Associated with Prognosis in Prostate Cancer Patients. Onco. 2023; 3(3):165-174. https://doi.org/10.3390/onco3030012
Chicago/Turabian StyleBaxevanis, Constantin N., Savvas Stokidis, Maria Goulielmaki, Angelos D. Gritzapis, and Sotirios P. Fortis. 2023. "Peripheral Blood CD8+ T-Lymphocyte Subsets Are Associated with Prognosis in Prostate Cancer Patients" Onco 3, no. 3: 165-174. https://doi.org/10.3390/onco3030012