
Outcomes and Safety with Utilization of Metallic Midfoot Wedges in Foot and Ankle Orthopedic Surgery: A Systematic Review of the Literature
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Creation
2.2. Eligibility Criteria
2.3. Study Definitions
2.4. Article Screening
2.5. Data Extraction
2.6. Article Quality Grading
2.7. Statistical Analysis
3. Results
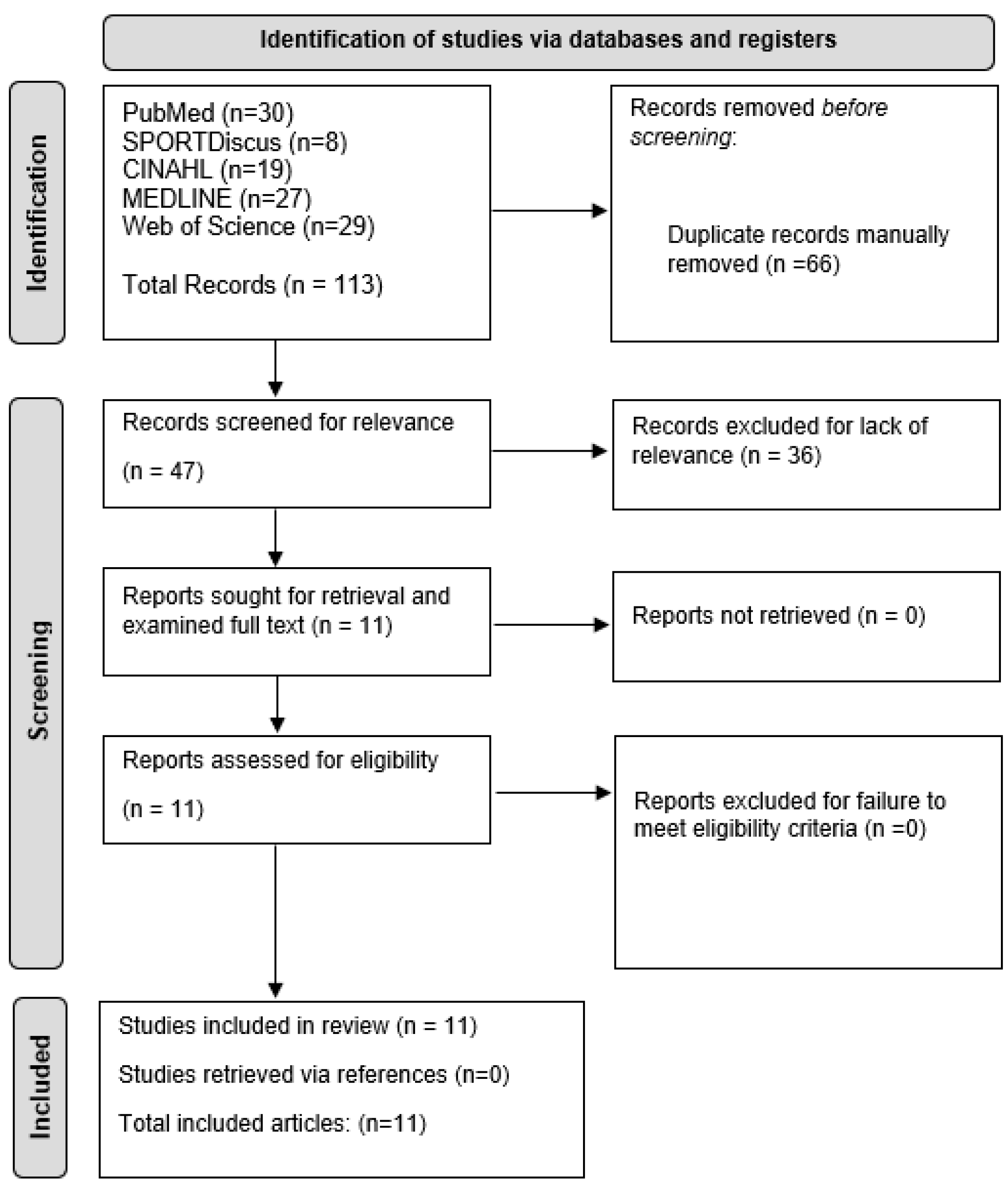
3.1. Search Results
3.2. Article Quality Results
3.3. Patient Demographics
3.4. Radiographic Outcomes after Wedge Utilization
3.5. Success Rates with Wedge Utilization
3.6. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evans, D. Calcaneo-valgus deformity. J. Bone Jt. Surg. Br. Vol. 1975, 57, 270–278. [Google Scholar] [CrossRef]
- Cotton, F.J. Foot statics and surgery. N. Engl. J. Med. 1936, 214, 353–362. [Google Scholar] [CrossRef]
- Cook, E.A.; Cook, J.J. Bone graft substitutes and allografts for reconstruction of the foot and ankle. Clin. Podiatr. Med. Surg. 2009, 26, 589–605. [Google Scholar] [CrossRef] [PubMed]
- Kamath, A.F.; Gee, A.O.; Nelson, C.L.; Garino, J.P.; Lotke, P.A.; Lee, G.-C. Porous tantalum patellar components in revision total knee arthroplasty: Minimum 5-year follow-up. J. Arthroplast. 2012, 27, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Long, W.J.; Scuderi, G.R. Porous tantalum cones for large metaphyseal tibial defects in revision total knee arthroplasty: A minimum 2-year follow-up. J. Arthroplast. 2009, 24, 1086–1092. [Google Scholar] [CrossRef] [PubMed]
- Sagherian, B.H.; Claridge, R.J. Porous tantalum as a structural graft in foot and ankle surgery. Foot Ankle Int. 2012, 33, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Bobyn, J.; Stackpool, G.J.; Hacking, S.A.; Tanzer, M.; Krygier, J.J. Characteristics of bone ingrowth and interface mechanics of a new porous tantalum biomaterial. J. Bone Jt. Surg. Br. Vol. 1999, 81, 907–914. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new Instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Au, B.; Patel, N.B.; Smith, C.N.; Burns, P.R. Short-to intermediate-term radiographic outcomes following Cotton osteotomy. J. Foot Ankle Surg. 2022, 61, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Ellis, S.J.; Williams, B.R.; Garg, R.; Campbell, G.; Pavlov, H.; Deland, J.T. Incidence of plantar lateral foot pain before and after the use of trial metal wedges in lateral column lengthening. Foot Ankle Int. 2011, 32, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Fraser, T.W.; Kadakia, A.R.; Doty, J.F. Complications and early radiographic outcomes of flatfoot deformity correction with metallic midfoot opening wedge implants. Foot Ankle Orthop. 2019, 4, 2473011419868971. [Google Scholar] [CrossRef]
- García-Jarabo, E.; Ramos-Ramos, L.; Sánchez-Morata, E.; Hernanz-González, Y.; Mellado-Romero, M.; Rico, J.V.Y. [Translated article] Surgical treatment at adult acquired flatfoot stage IIB: Spring ligament repair. Rev. Esp. Cir. Ortop. Y Traumatol. 2023, 67, T62–T67. [Google Scholar] [CrossRef]
- Gross, C.E.; Huh, J.; Gray, J.; Demetracopoulos, C.; Nunley, J.A. Radiographic outcomes following lateral column lengthening with a porous titanium wedge. Foot Ankle Int. 2015, 36, 953–960. [Google Scholar] [CrossRef]
- Matthews, M.; Cook, E.A.; Cook, J.; Johnson, L.; Karthas, T.; Collier, B.; Hansen, D.; Manning, E.; McKenna, B.; Basile, P. Long-term outcomes of corrective osteotomies using porous titanium wedges for flexible flatfoot deformity correction. J. Foot Ankle Surg. 2018, 57, 924–930. [Google Scholar] [CrossRef]
- Moore, S.H.; Carstensen, S.E.; Burrus, M.T.; Cooper, T.; Park, J.S.; Perumal, V. Porous titanium wedges in lateral column lengthening for adult-acquired flatfoot deformity. Foot Ankle Spec. 2018, 11, 347–356. [Google Scholar] [CrossRef]
- Romeo, G.; Bianchi, A.; Cerbone, V.; Parrini, M.M.; Malerba, F.; Martinelli, N. Medial cuneiform opening wedge osteotomy for correction of flexible flatfoot deformity: Trabecular titanium vs. bone allograft wedges. BioMed Res. Int. 2019, 2019, 1472471. [Google Scholar]
- Siebert, M.; Hedrick, B.N.; Zide, J.R.; Thomas, D.M.; Shivers, C.; Pierce, W.A.; Kanaan, Y.; Harris, M.C.; Riccio, A.I. Do we really need to worry about calcaneocuboid subluxation during lateral column lengthening for planovalgus foot deformity? J. Pediatr. Orthop. 2021, 41, e246–e251. [Google Scholar] [CrossRef]
- Stamatos, N.J.; Murasko, M.J.; Richardson, K.; O’connor, C.; Anoushiravani, A.A.; Adams, C.; Rosenbaum, A. Radiographic Outcomes of Titanium Augment vs Bone Graft in Lateral Column Lengthening for Adult-Acquired Flatfoot Deformity. Foot Ankle Orthop. 2023, 8, 24730114231176554. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.; McDonald, E.; Sutton, R.; Raikin, S.M. Severe flexible pes planovalgus deformity correction using trabecular metallic wedges. Foot Ankle Int. 2019, 40, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Myerson, M.S.; Thordarson, D.B.; Johnson, J.E.; Hintermann, B.; Sangeorzan, B.J.; Deland, J.T.; Schon, L.C.; Ellis, S.J.; Netto, C.d.C. Classification and nomenclature: Progressive collapsing foot deformity. Foot Ankle Int. 2020, 41, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhu, M.; Gu, W.; Hamati, M.; Hunt, K.J.; Netto, C.d.C.; Simonson, T.S.; Myerson, M.S. Diagnostic accuracy of the progressive collapsing foot deformity (PCFD) classification. Foot Ankle Int. 2022, 43, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Mansur, N.S.B.; Lalevée, M.; Dibbern, K.N.; Myerson, M.S.; Ellis, S.J.; Femino, J.E.; Netto, C.d.C. Intra-and interobserver reliability of the new classification system of progressive collapsing foot deformity. Foot Ankle Int. 2022, 43, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Nayak, R.; Patel, M.S.; Kadakia, A.R. Patient-reported outcomes and radiographic assessment in primary and revision stage II, III, and IV progressive collapsing foot deformity surgery. Foot Ankle Orthop. 2021, 6, 2473011421992111. [Google Scholar] [CrossRef] [PubMed]
- Momberger, N.; Morgan, J.M.; Bachus, K.N.; West, J.R. Calcaneocuboid joint pressure after lateral column lengthening in a cadaveric planovalgus deformity model. Foot Ankle Int. 2000, 21, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Zhang, P.; Yang, Y.-F.; Zhou, J.-Q.; Li, Q.-M.; Yu, G.-R. Biomechanical analysis of the calcaneocuboid joint pressure after sequential lengthening of the lateral column. Foot Ankle Int. 2013, 34, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Vosseller, J.T.; Ellis, S.J.; O’malley, M.J.; Elliott, A.J.; Levine, D.S.; Deland, J.T.; Roberts, M.M. Autograft and allograft unite similarly in lateral column lengthening for adult acquired flatfoot deformity. HSS J. 2013, 9, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Oh, I.; Imhauser, C.; Choi, D.; Williams, B.; Ellis, S.; Deland, J. Sensitivity of plantar pressure and talonavicular alignment to lateral column lengthening in flatfoot reconstruction. J. Bone Jt. Surg. Am. Vol. 2013, 95, 1094. [Google Scholar] [CrossRef]
- Tennant, J.N.; Carmont, M.; Phisitkul, P. Calcaneus osteotomy. Curr. Rev. Musculoskelet. Med. 2014, 7, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Catanzariti, A.; Zdenek, C.M. Complications of Stage II Flatfoot Surgery. In Complications in Foot and Ankle Surgery: Management Strategies; Springer: Berlin/Heidelberg, Germany, 2017; pp. 279–290. [Google Scholar]



{kind=link}
{kind=link}
| Author (Year) | Study Type | Total MINORS Score | Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | End Points Appropriate to Study Aim | Unbiased Assessment of Study End Point | Follow-Up Period Appropriate to Study Aim | Less than 5% Lost to Follow Up | Prospective Calculation of the Study Size | Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analysis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Au (2022) | Non-comparative | 12 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | - | - | - | - |
| Ellis (2011) | Comparative | 19 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 2 |
| Fraser (2019) | Non-comparative | 10 | 1 | 2 | 0 | 2 | 2 | 1 | 2 | 0 | - | - | - | - |
| García-Jarabo (2023) | Non-comparative | 12 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | - | - | - | - |
| Gross (2015) | Non-comparative | 12 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | - | - | - | - |
| Matthews (2018) | Non-comparative | 11 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 0 | - | - | - | - |
| Moore (2018) | Non-comparative | 12 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | - | - | - | - |
| Romeo (2019) | Comparative | 20 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 |
| Siebert (2021) | Non-comparative | 12 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | - | - | - | - | - |
| Stamatos (2023) | Comparative | 20 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 |
| Tsai (2019) | Non-comparative | 12 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | - | - | - | - |
| Author (Year) | Type of Study | Treatment Group | Type of Wedge | Patients (n) | Feet (n) | Age | Description of Cohort | Wedge Size | Type of Surgery |
|---|---|---|---|---|---|---|---|---|---|
| Ellis (2011) | Retrospective | Group 1 (Metal Wedge) | Metal | 13 | 13 | 62.5 | Patients who underwent flatfoot reconstruction using lateral column lengthening with iliac crest autograft or allograft by the senior author made up of those patients with either a pain level greater or equal to 4 on the visual analog scale or had undergone revision lateral column lengthening | 10 mm (max) | Calcaneal osteotomy and/or flexor tendon transfer |
| Group 2 (Metal Wedge) | Metal | 97 | 103 | 61.7 | Patients who underwent flatfoot reconstruction using lateral column lengthening with iliac crest autograft or allograft by the senior author including those patients with pain less than 4 on the visual analog scale and no revision surgery | 10 mm (max) | Calcaneal osteotomy and/or flexor tendon transfer | ||
| Fraser (2019) | Retrospective | Metal Wedge | Titanium | 31 | 32 | 41.1 | Patients all had titanium wedge placement in the medial cuneiform at the time of dorsal opening wedge osteotomy | 7 mm | Operative correction for flatfoot deformity with a porous titanium wedge used to correct the forefoot varus component of the multiplanar deformity |
| Siebert (2021) | Retrospective # (C) | Metal Wedge | Titanium | 7 | 14 | 60.7 | Patients who did not have prior foot surgery on either foot or severe osteopenia as determined by computed tomography attenuation | 12 mm (mean) | Lateral column lengthening was performed through an anterior calcaneus osteotomy using a standard sinus tarsi approach |
| Matthews (2018) | Retrospective | Metal Wedge | Titanium | 34 | 43 | 27.35 | Patients who had undergone flexible flatfoot reconstruction using porous titanium wedges within the study period (1 June 2009–30 June 2015) | Evans-size: 8–12 mm, Cotton: 4.5–9.5 mm | Surgical correction of flexible flatfoot deformities using porous titanium wedges |
| Romeo (2019) | Retrospective | Group 1 (Metal Wedge) | Metal | 18 | - | 36.7 | Patients who had Cotton osteotomies and medializing calcaneal osteotomies performed on them by the senior surgeon, and they were randomly allocated into Group 1 (metallic Cotton wedges) and Group 2 (bone allograft) | 7.3 mm | Cotton osteotomies and medializing calcaneal osteotomies |
| Group 2 (Bone Allograft Wedge) | Bone Allograft | 18 | - | 38.5 | Patients who had Cotton osteotomies and medializing calcaneal osteotomies performed on them by the senior surgeon, and they were randomly allocated into Group 1 (metallic Cotton wedges) and Group 2 (bone allograft) | - | Cotton osteotomies and medializing calcaneal osteotomies | ||
| Moore (2018) | Retrospective | Metal Wedge | Titanium | 30 | 34 | 39 | All patients had stage II adult-acquired flatfoot deformity and were treated only after initially failing conservative management | Evans-size: 8 mmCotton: 4.5 and 6 mm | Lateral column lengthening procedure |
| Gross (2015) | Retrospective | Metal Wedge | Titanium | 26 | 28 | 46 | All patients who underwent lateral column lengthening with a porous titanium wedge at the institution | 8 mm | Lateral column lengthening with a porous titanium wedge |
| Stamatos (2023) | Retrospective | Group 1 (Metal Wedge) | Titanium | 17 | - | 47.2 | All of the patients had the following criteria: over 18 years of age with at least stage II AAFD, history of flatfoot reconstruction with LCL by one of 3 surgeons in a single practice between October 2008 until October 2018, all causes of adult-acquired flatfoot deformity, and a history of other concomitant accessory procedures including medializing calcaneal osteotomy, excision of accessory navicular, and flexor digitorum longus transfer, among others | - | Flatfoot reconstruction with lateral column lengthening, and the possibility of other concomitant accessory procedures including medializing calcaneal osteotomy, excision of accessory navicular, and flexor digitorum longus transfer, among others |
| Group 2 (Bone Allograft) | Bone Allograft | 27 | - | 58.6 | All of the patients had the following criteria: over 18 years of age with at least stage II AAFD, history of flatfoot reconstruction with LCL by one of 3 surgeons in a single practice between October 2008 until October 2018, all causes of adult-acquired flatfoot deformity, and a history of other concomitant accessory procedures including medializing calcaneal osteotomy, excision of accessory navicular, and flexor digitorum longus transfer, among others | - | Flatfoot reconstruction with lateral column lengthening, and the possibility of other concomitant accessory procedures including medializing calcaneal osteotomy, excision of accessory navicular, and flexor digitorum longus transfer, among others | ||
| Tsai (2019) | Retrospective | Metal Wedge | Titanium | 45 | 48 | 48.4 | All patients with severe flexible pes planovalgus who were treated with corrective osteotomies using trabecular titanium wedges at least 2 years following surgery | - | Corrective osteotomies using trabecular titanium wedges |
| Au (2022) | Retrospective | Metal and Non-Metal Wedges | Both | 61 | 71 | 44.6 | Patients were included if they were older than 13 years of age, had at least 10 weeks of follow-up, and had a diagnosis of either adult acquired flatfoot disorder, tibialis posterior tendon dysfunction, or pes planovalgus. Patients with metal wedges (N = 11) were classified as Group 1, and patients with nonmetal wedges (N = 60) as Group 2 | 6.83 mm | A Cotton procedure for pes planovalgus |
| García-Jarabo (2023) | Retrospective | Metal Wedge | Titanium | 20 | 23 | 63 | Patients who had been diagnosed with adult-acquired flatfoot deformity grade IIB, had no previous surgery, and conservative osteoprosthetic treatment with medial support insoles and supinator gradient had failed | 8 mm | Lateral column lengthening osteotomy, Cotton osteotomy, and medial sliding osteotomy |
| Author (Year) | Treatment Group | Type of Wedge | Patients (n) | Mean Preoperative Lateral Calcaneal Pitch Angle (°) | Mean Postoperative Lateral Calcaneal Pitch Angle (°) | Mean Preoperative Lateral Talus-First MT Angle (°)/Meary’s Angle (°) | Mean Postoperative Lateral Talus-First MT Angle/Meary’s Angle (°) | Mean Preoperative Anterior–Posterior Talonavicular Coverage Angle (°) | Mean Postoperative Anterior–Posterior Talonavicular Coverage Angle (°) | Mean Preoperative Anterior–Posterior Talus-First MT Angle (°) | Mean Postoperative Anterior–Posterior Talus-First MT Angle (°) | Mean Preoperative Anterior–Posterior Talocalcaneal Angle (°)/Kite’s Angle (°) | Mean Postoperative Anterior–Posterior Talocalcaneal Angle (°)/Kite’s Angle (°) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ellis (2011) | Group 1 (Metal Wedge) | Metal | 13 | 15.0 (2–30) | - | 22.6 (6–45) | - | 19.4 (0–46) | - | 16.8 (−11–49) | - | - | - |
| Group 2 (Metal Wedge) | Metal | 97 | 14.2 (1–24) | - | 20.9 (13–36) | - | 21.3 (3–55) | - | 17.8 (1–29) | - | - | - | |
| Romeo (2019) | Group 1 (Metal Wedge) | Metal | 18 | - | - | 9.5 (4.1) | 1.4 (1.9) | - | - | - | - | 29.5 (4.2) | 21.5 (2.5) |
| Group 2 (Bone Allograft Wedge) | Bone Allograft | 18 | - | - | 9.8 (4.0) | 1.8 (1.7) | - | - | - | - | 30.0 (4.0) | 21.8 (2.4) | |
| Moore (2018) | Metal Wedge | Titanium | 30 | - | - | 10.9 (5.6) | 5.6 (4.9) | 37.6 (14.8) | 11.0 (14.8) | - | - | - | - |
| Gross (2015) | Metal Wedge | Titanium | 26 | 13.7 (4.7) | 18.9 (5.9) | 15.2 (8.6) | 8.7 (7.7) | 26.4 (9.6) | 14.0 (7.2) | 21.6 (11.4) | 8.8 (7.4) | - | - |
| Stamatos (2023) | Group 1 (Metal Wedge) | Titanium | 17 | 14.8 | 22.4 | - | - | 32.3 | 8.8 | 23.1 | 6.4 | - | - |
| Group 2 (Bone Allograft) | Bone Allograft | 27 | 12.9 | 25.4 | - | - | 26.8 | 6.9 | 18.6 | 5.3 | - | - | |
| Tsai (2019) | Metal Wedge | Titanium | 45 | 13.1 | 18.2 | −19.8 | −3.9 | - | - | - | - | - | - |
| García-Jarabo (2023) | Metal Wedge | Titanium | 20 | - | - | 15.7 (3.4) | 3.1 (2.2) | 21.3 (5.4) | 7.3 (3.4) | 18.3 (5.1) | 3.9 (2.4) | - | - |
| Author (Year) | Type of Wedge | Patients (n) | Complications | Success Rate (%) |
|---|---|---|---|---|
| Fraser (2019) | Titanium | 31 | No complications | 100 |
| Matthews (2018) | Titanium | 34 | No major complications, but there was a 12.6% incidence of minor complications (hardware pain from plates over grafts, 1 case of scar neuritis, and a 5% table incidence of transfer pain associated with the PTWs) | 100 |
| Romeo (2019) | Metal | 18 | One case of malpositioning of the titanium wedge, and one case of HV recurrence | 96 |
| Bone Allograft | 18 | Three cases of symptomatic bony prominence, one case of osteoarthritis of the first metatarsocuneiform joint, and one case of injury of the terminal branch of the saphenous nerve which required neurectomy | ||
| Moore (2018) | Titanium | 30 | The overall rate of complications was 20.6%. The most common complications were persistent CC joint pain (14.7%) and peroneal tendonitis (8.8%) | 100 |
| Gross (2015) | Titanium | 26 | - | 96 |
| Stamatos (2023) | Titanium | 17 | Infection (5.9%), pain (11.8%), removal of hardware (11.8%) | 100 |
| Bone Allograft | 27 | Infection (3.7%), pain (11.1%), removal of hardware (63.0%) | 89.9 | |
| Tsai (2019) | Titanium | 45 | There was an overall complication rate of 6.3% | 100 (Cotton) 95.8 (Evans) |
| Au (2022) | Both | 61 | Complications were manifested by persistent pain at the Cotton surgical site, removal of hardware from the site, subsidence of graft, non-union of the Cotton osteotomy site, anesthesia block complications, and revisions of the medial column. The overall complication rate was 5.6% | 97.0 |
| García-Jarabo (2023) | Titanium | 20 | One case of progression of the deformity requiring double medial arthrodesis and one case of dehiscence of the surgical wound should be highlighted | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talaski, G.M.; Baumann, A.; Sleem, B.; Walley, K.C.; Anastasio, A.T.; Gall, K.; Adams, S.B. Outcomes and Safety with Utilization of Metallic Midfoot Wedges in Foot and Ankle Orthopedic Surgery: A Systematic Review of the Literature. Biomechanics 2024, 4, 34-49. https://doi.org/10.3390/biomechanics4010003
Talaski GM, Baumann A, Sleem B, Walley KC, Anastasio AT, Gall K, Adams SB. Outcomes and Safety with Utilization of Metallic Midfoot Wedges in Foot and Ankle Orthopedic Surgery: A Systematic Review of the Literature. Biomechanics. 2024; 4(1):34-49. https://doi.org/10.3390/biomechanics4010003
Chicago/Turabian StyleTalaski, Grayson M., Anthony Baumann, Bshara Sleem, Kempland C. Walley, Albert T. Anastasio, Ken Gall, and Samuel B. Adams. 2024. "Outcomes and Safety with Utilization of Metallic Midfoot Wedges in Foot and Ankle Orthopedic Surgery: A Systematic Review of the Literature" Biomechanics 4, no. 1: 34-49. https://doi.org/10.3390/biomechanics4010003