1. Introduction
Egomotion is defined as an actual body motion in response to optic flow or the environmental displacement of the observer [
1,
2]. The sensory information needed to maintain postural stability, maintaining the body’s center of mass (COM) within the base of support (BOS), is acquired from the visual, vestibular, and somatosensory–proprioceptive systems, and alterations to these systems can affect one’s ability to maintain postural control, especially when the visual system is manipulated [
3,
4]. Changes in the environment provide changing visual input, creating a sensory conflict between the visual, vestibular, and somatosensory–proprioceptive sensory systems of postural control. Any changes in the optic flow with a changing environment can induce an increase in postural sway, causing postural instability [
1,
5,
6,
7,
8,
9].
With the advancement of technology, the role of VR in research, clinical applications, and rehabilitation has grown tremendously. As such, the impact of VR on postural control in a variety of populations and applications is constantly being investigated. In particular, several VR-based studies have shown that optic flow cues, as presented in a head-mounted display (HMD), play an important role in both one’s posture when standing [
10] and when judging self-motion [
11]. Specific to postural control and fall prevention research, VR has been used to induce visual conflicts in virtual environments (VEs) [
6]. An induced postural perturbation and failure to recover from an imbalance caused by the perturbation are the primary reasons for postural instability, leading to falls and fall-related injuries (both fatal and non-fatal) [
3,
12]. However, when provided in a controlled and repetitive manner over time, these postural perturbations can aid in improving postural control and preventing falls. This approach is described as perturbation-based balance training (PBBT), which is an emerging task-specific intervention for fall prevention, where physical mechanical perturbations are applied to the body in a controlled setting. Physical perturbations can range from simple therapist-induced pushes/pulls, support surface movements inducing slip or trip perturbations, computerized force platform perturbations, and more clinically followed treadmill belt perturbations [
13,
14]. These computerized, split-belt treadmills are very expensive, averaging about USD 150,000, and additional add-ons such as the virtual reality surround environment, fall harness system, etc., can easily reach around USD 500,000. As such, there is a greater need for more cost-effective PBBT equipment.
While extensive research has been performed on the impacts, methods, and applications of PBBT in several populations [
4,
13,
14,
15], limited research exists on the impact of visual perturbations on postural control behavior, especially using both non-immersive and immersive VR. Immersive VR is delivered using a head-mounted display (HMD) where an individual is fully immersed into the virtual environment with no other visual feedback. On the other hand, non-immersive VR is usually delivered in front of the individual on a screen, and the individual is not wearing a head-mounted display and is not fully immersed. Visual perturbations such as the tilting of the VE, the rotation of the VE in randomized clockwise or counterclockwise directions, and changes in environmental conditions by adding snowfall or high-altitude scenes to simulate hazardous conditions have been utilized in VR and reported to impact postural stability [
15,
16,
17,
18]. However, to help understand the impact of egomotion, specifically taking inspiration from the classical “moving room experiment”, Slobounov and colleagues (2006) [
1] reported increased center of pressure (COP) postural sway while viewing a virtual moving room, compared with when the virtual room was stationary. However, the virtual room in this experiment was created using a wall projector, and the participants wore Crystal Eyes StereoGraphic glasses to be exposed to the VE [
1].
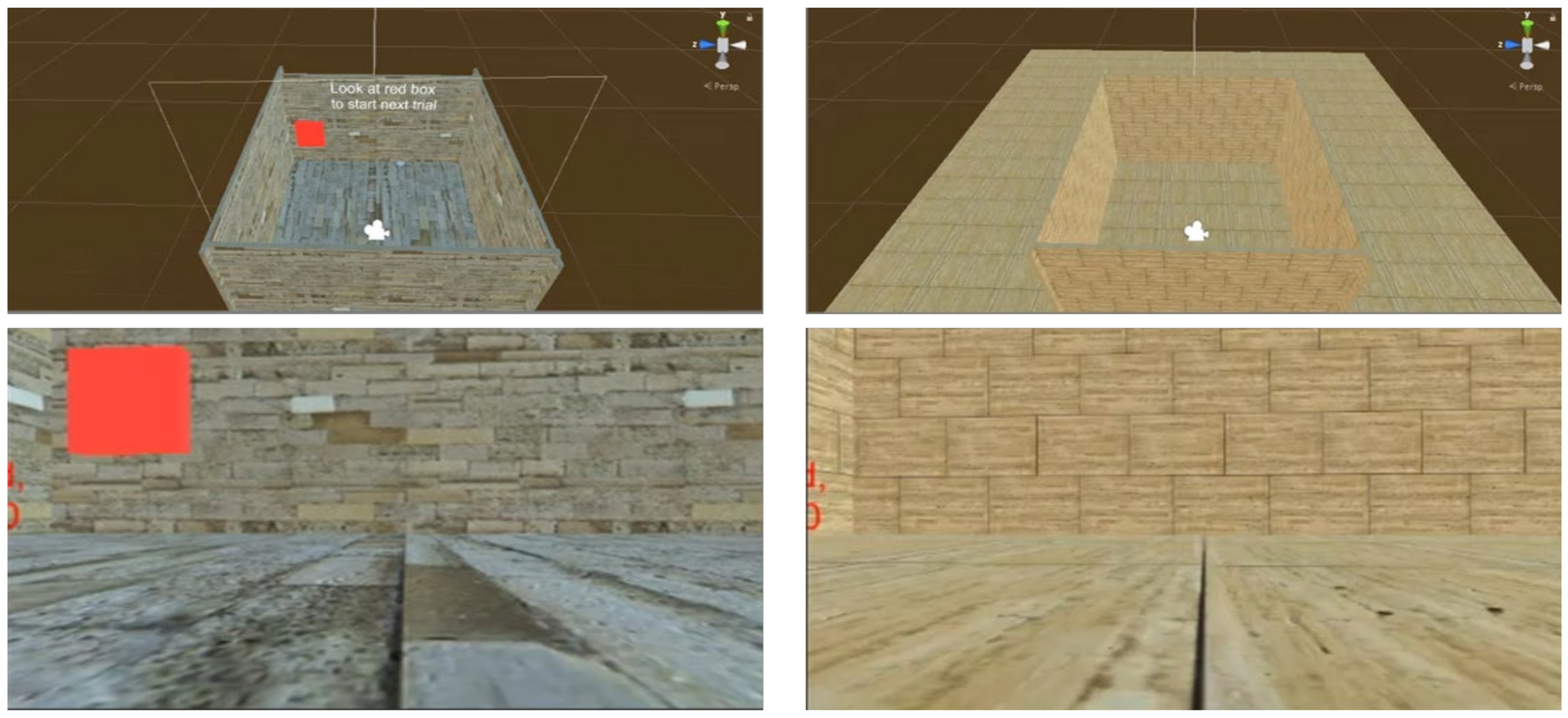
More recently, from the current research team, Chander and colleagues (2019) [
6] created a virtual room in a fully immersive VR, delivered through a head-mounted display (HMD), and assessed the impact of a moving wall in both unexpected and expected conditions. During unexpected virtual and visual perturbations, overall postural sway was higher than during expected perturbations, providing evidence for both compensatory postural responses (CPRs) during unexpected perturbations and anticipatory postural responses (APRs) during expected perturbations [
6]. However, in this experiment, only the front wall of the virtual room was designed to move and provide visual perturbations, while the walls on the side did not move. Hence, the impact of a “Vroom paradigm” in a fully immersive VR delivered through an HMD, with randomized unexpected and expected trials on postural stability, is still unknown. Finally, participants’ subjective experience in VR is an important determinant of the success of a VR intervention, as subjective variables of simulator sickness; presence in the VE focusing on immersion, involvement, visual fidelity, and interface quality; and the subjective perception of one’s own postural stability when exposed to a fully immersive VR-generated “(Vroom) paradigm” are still not known. Therefore, the purpose of this study was to investigate the impact of a Vroom paradigm that provided both unexpected and expected visual and virtual postural perturbations on postural stability and to investigate participants’ subjective experience with the Vroom paradigm, through simulator sickness, presence, and balance confidence questionnaires. It was hypothesized that the virtual moving room paradigm will induce visual and virtual postural perturbations negatively impacting postural stability and without detrimental subjective experiences of such exposure.
3. Results
During the virtual moving room paradigm experiment, the repeated-measure ANOVA revealed a significant main effect between moving room directions and the knowledge of the moving room, without any significant interactions.
Significant differences between moving room directions were observed for the following variables:
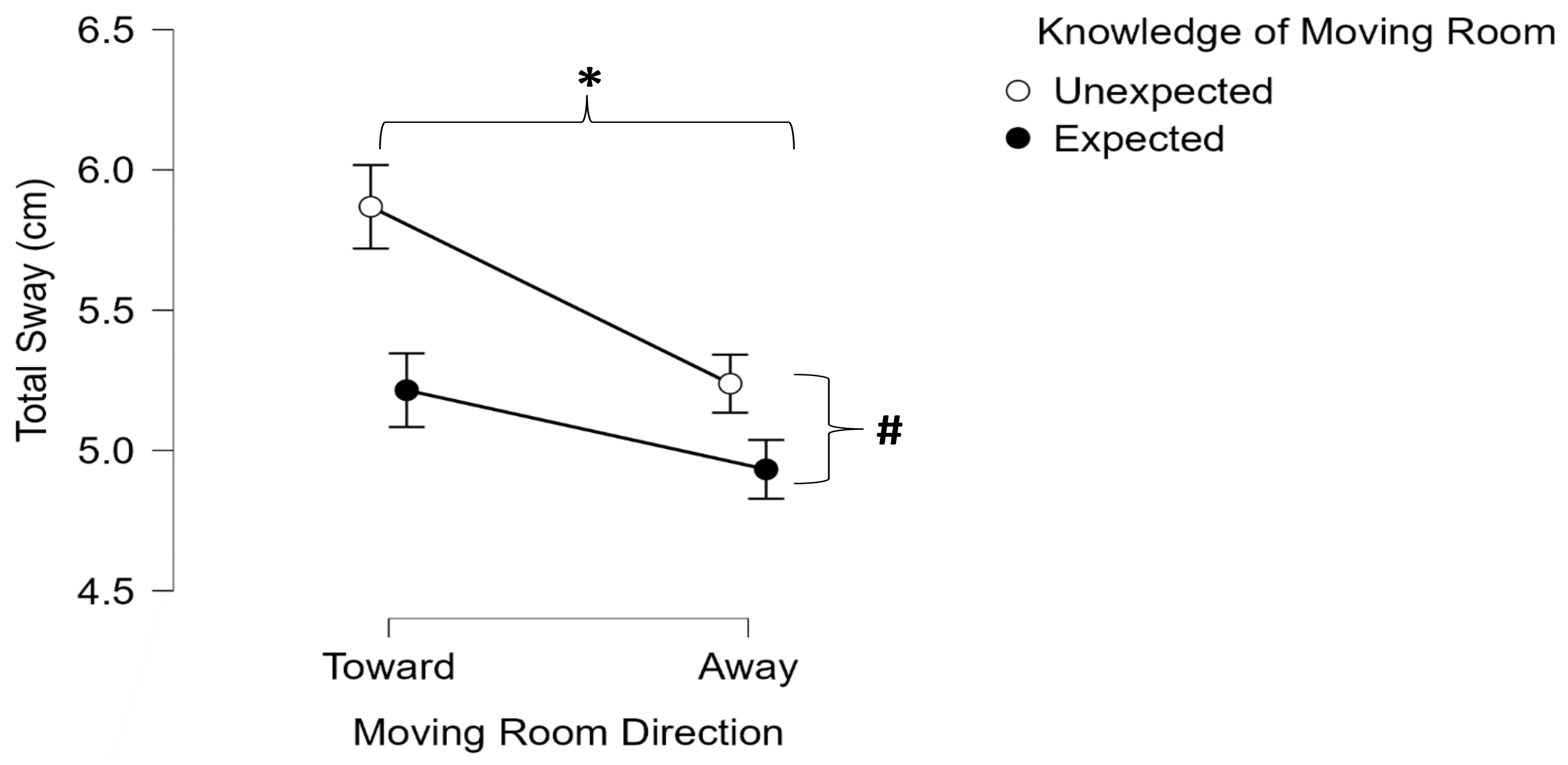
Total sway (F (1,29) = 15.448,
p < 0.001, ηp
2 = 0.348) (
Figure 3);
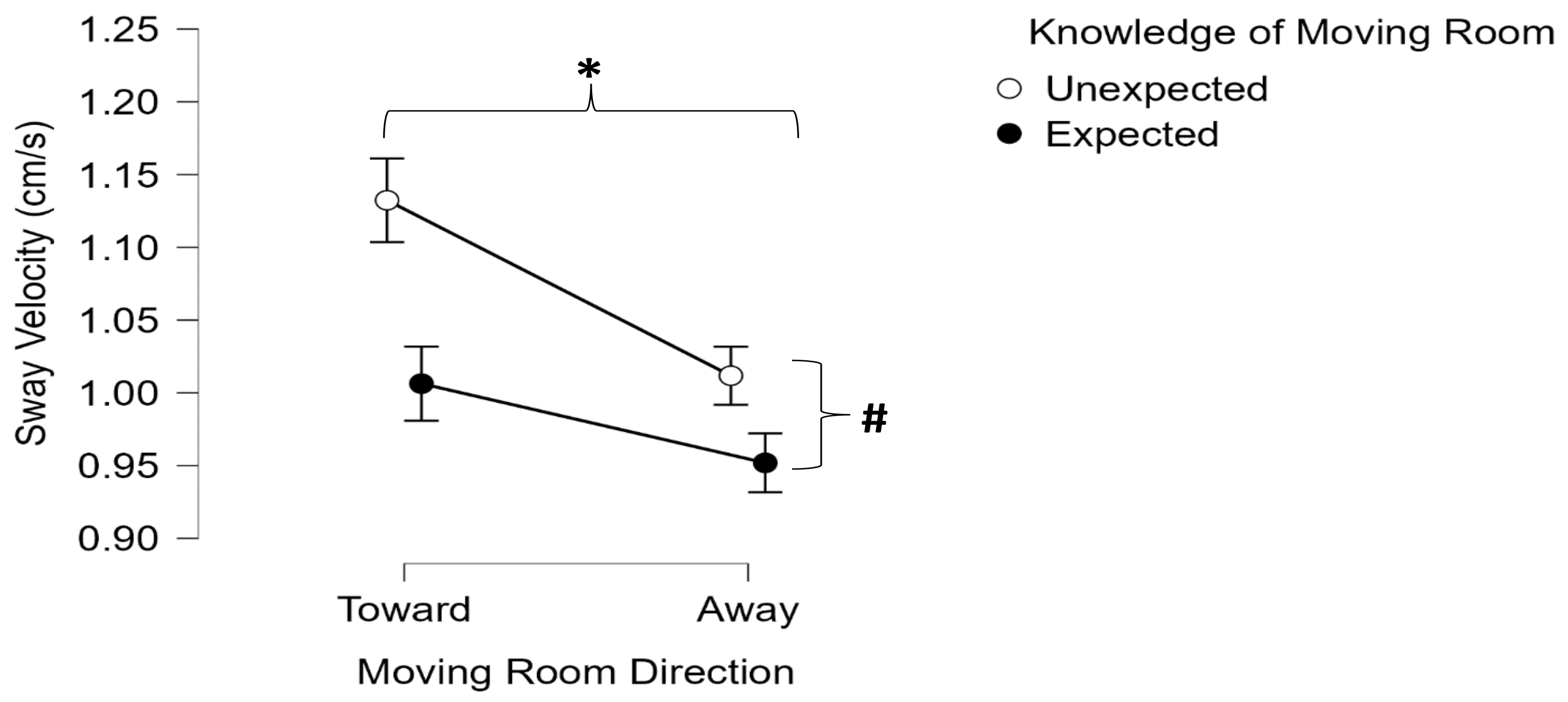
Sway velocity (F (1,29) = 15.071,
p < 0.001, ηp
2 = 0.342) (
Figure 4);
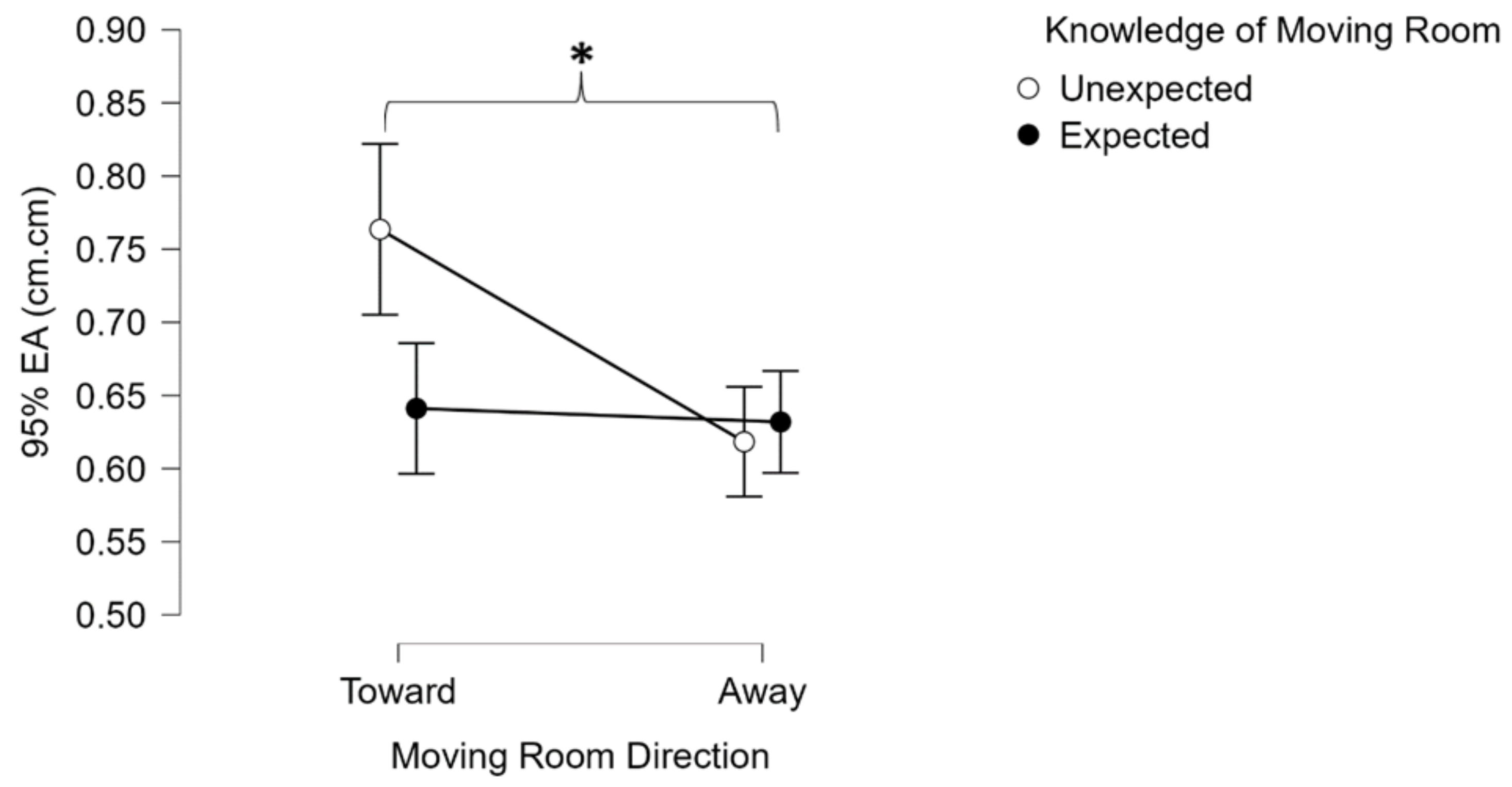
The 95% ellipsoid area (F (1,29) = 4.811,
p < 0.036, ηp
2 = 0.142) (
Figure 5).
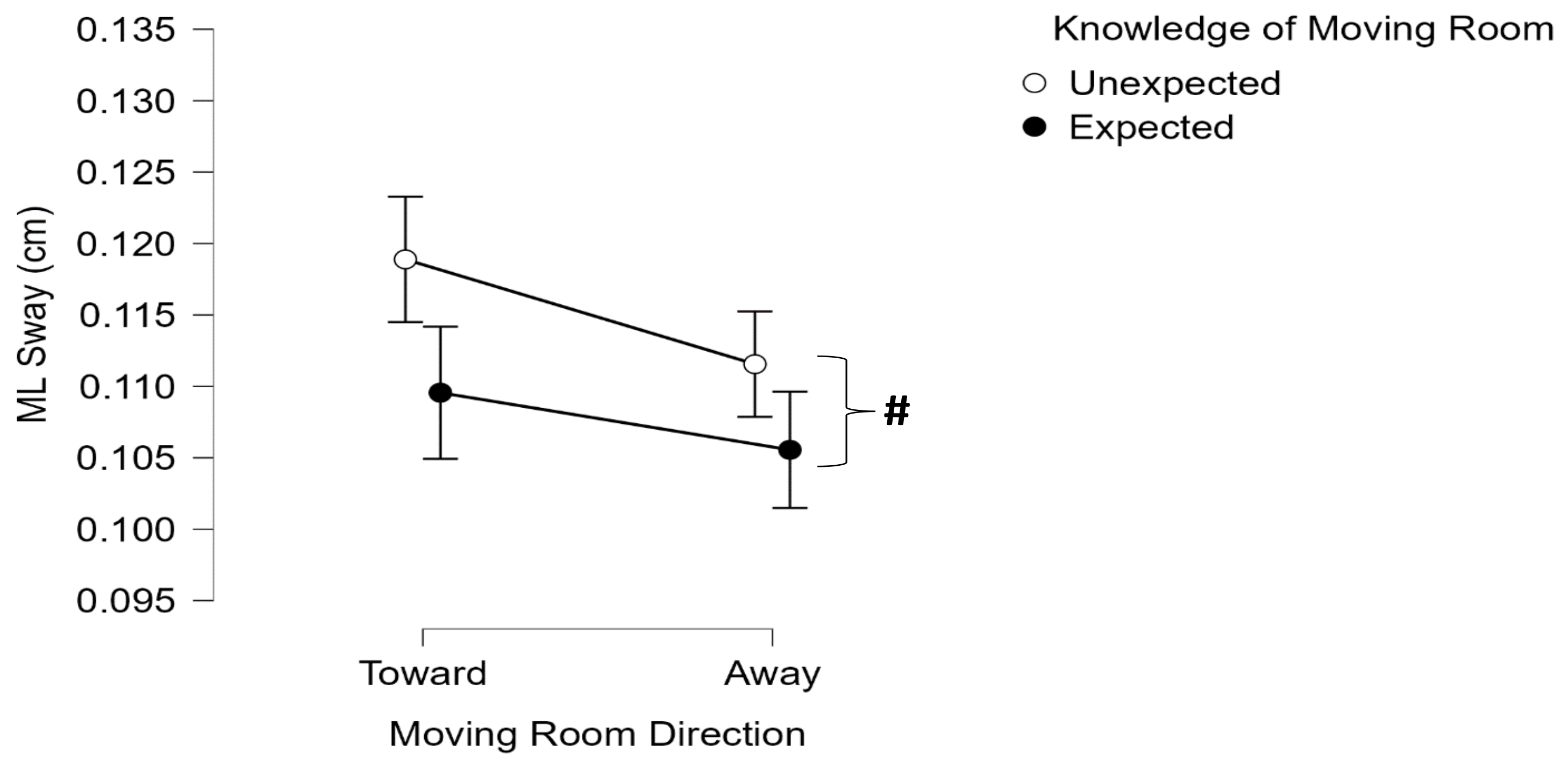
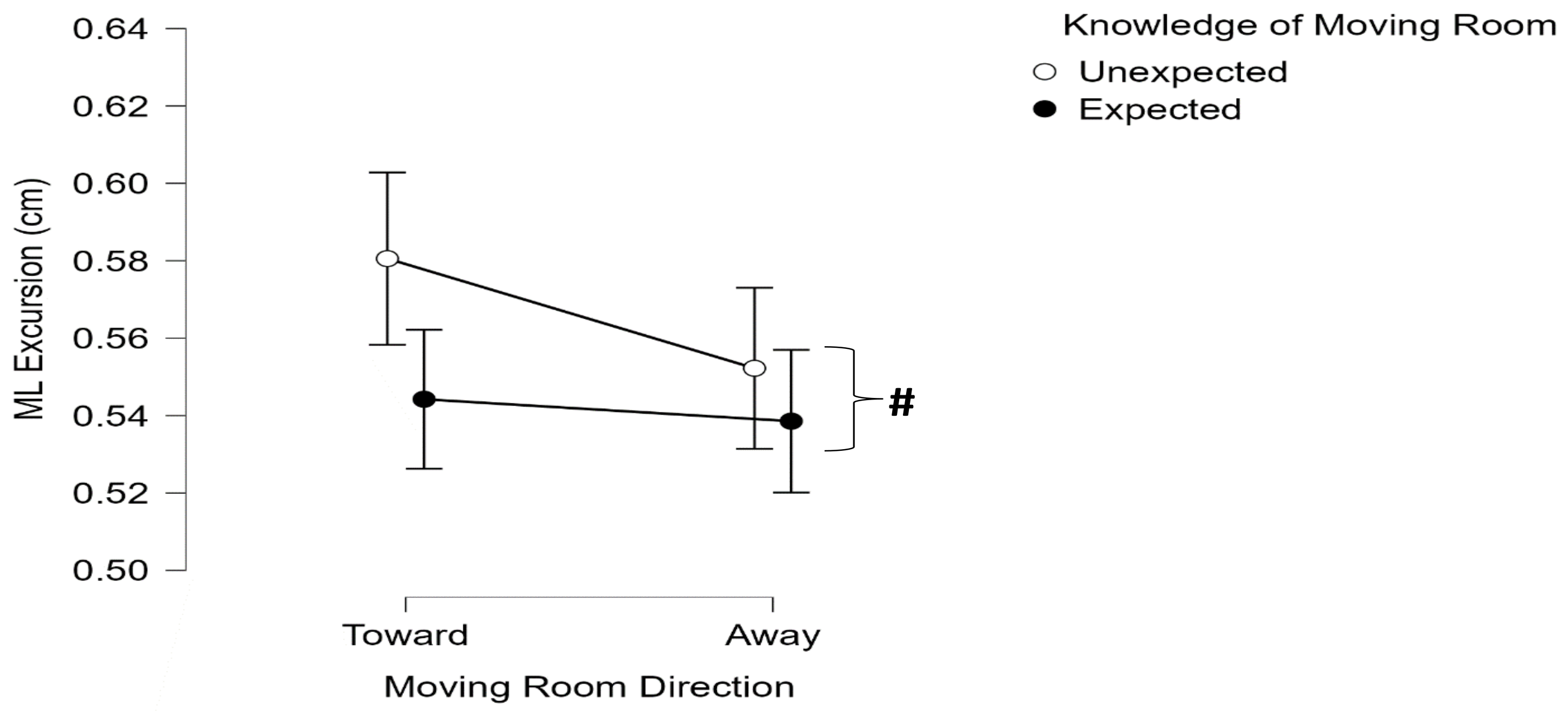
Significant differences between the two types of knowledge of the moving room were observed for the following variables:
The total sway (F (1,29) = 10.575,
p = 0.003, ηp
2 = 0.267) (
Figure 3);
Sway velocity (F (1,29) = 10.619,
p < 0.003, ηp
2 = 0.268) (
Figure 4);
Medial–lateral excursion (F (1,29) = 4.288,
p = 0.047, ηp
2 = 0.129) (
Figure 6);
Medial–lateral root mean square sway (F (1,29) = 6.591,
p = 0.016, ηp
2 = 0.185) (
Figure 7).
The pairwise comparisons of the significant main effect revealed that, for both the total sway and sway velocity, the room moving toward the participants induced greater postural sway than the room moving away (total sway; p < 0.001; 95% CI (0.219, 0.694); sway velocity; p < 0.001; 95% (0.041, 0.134); ellipsoid area; p = 0.036; 95% CI (0.005, 0.149)), and the unexpected moving room induced significantly greater postural sway than the expected moving rooms (total sway; p = 0.003; 95% CI (0.178, 0.781); sway velocity; p = 0.003; 95% CI (0.035, 0.151); medial–lateral excursion; p = 0.047; 95% CI (0.0003, 0.050); medial–lateral root mean square sway; p = 0.016; 95% CI (0.002, 0.014)).
For subjective VR experience analyses (
Table 1), the repeated-measure ANOVA revealed a significant main effect between the SSQ responses of pre-test, post-unexpected, and post-expected sessions (F (2,58) = 5.524,
p = 0.006, ηp
2 = 0.160). Pairwise comparisons of significant main effects revealed that the post-expected SSQ responses were significantly greater than the pre-test SSQ responses but not greater than the post-unexpected SSQ responses. The average score for the PQ was 94.4, with a standard deviation of +/−12.21, a maximum score of 113, and a minimum score of 67. The average score for the pre-test BCS was 42.90, with a standard deviation of 12.72, a maximum of 67, and a minimum of 10 out of 80 possible points, with the average balance confidence score being 53.6%. The average score for the post-test (moving room trials) was 45.77, with a standard deviation of 12.40, a maximum of 72, and a minimum of 11 out of 80 possible points, with the average balance confidence score being 57.2%. The paired-sample
t-test revealed that pre- and post-test scores were strongly and positively correlated (
r = 0.943,
p < 0.001), and a significant difference was observed between pre- and post-test scores (
p = 0.001), where post-test scores were significantly higher than pre-test scores.
4. Discussion
The purpose of this study was to assess the postural stability behavior when exposed to a Vroom paradigm and the subjective experience of VR exposure. Evidence of the virtual moving room inducing postural perturbations that challenge the postural control system, especially when the moving room is unexpected and toward the individual, and increased balance confidence with realistic immersion in the VE and no adverse effects of simulator sickness was observed, suggesting the beneficial effects of the virtual moving room paradigm in postural stability and potential balance training.
4.1. Comparison of Moving Room Conditions
In the current study, the postural sway variables of total sway, sway velocity, and 95% ellipsoid area were significantly higher when the Vroom moved toward the participants than away from them, and the postural sway variables of total sway, sway velocity, and medial–lateral root mean square sway and excursions were significantly higher during unexpected trials than during the expected trials. These findings suggest decreased postural stability when the perturbations were unanticipated, and when the virtual moving room moved toward the participants.
The roles of CPRs and APRs are important to consider when comparing unexpected and expected perturbations. During unexpected perturbations, the individual’s postural control system is forced to respond to the unanticipated moving room perturbations, resulting in compensatory postural adjustments and higher postural sway than during expected perturbations [
24]. However, in expected perturbations, the individual’s postural control system anticipates the moving room perturbations, resulting in anticipatory postural adjustments and lower postural sway than in unexpected perturbations [
24,
25,
26,
27]. Thus, evidence of both CPRs and APRs was observed in the Vroom paradigm. These results are consistent with our previous findings on the impact of a virtual moving wall on postural stability [
6]. During unexpected conditions, without the knowledge of an upcoming virtual and visual perturbation, the CPRs work in response to the moving room, relying on the visual sensory information in a feedback loop mechanism to maintain postural stability. During the expected conditions, with the knowledge of an upcoming virtual and visual perturbation, the APRs work without greater reliance on the visual sensory information in a feed-forward loop mechanism to maintain postural stability. Unexpected trials were always conducted first to obtain “true” unexpected postural responses to the moving room perturbations followed by the expected trials, but the order in which participants experienced a virtual moving room moving toward or away from them was completely random to eliminate any learning effects.
Additionally, not only did the perturbation being unexpected or expected have an impact on postural control behavior, but the direction in which the virtual moving room was moving (toward or away from the participant) also played a role in the results of the postural sway variables. In the current study, the unexpected toward-moving room condition elicited significantly higher total sway and sway velocity than the other three conditions. It is well known that individuals tend to sway in the direction of the perturbation [
9]. It is also known the degree of the limits of stability (LOS) in the posterior direction (4.5 degrees from the vertical line of gravity) is less than in the anterior direction (8 degrees from the vertical line of gravity) [
28]. Therefore, one can interpret that when the virtual moving room perturbation is moving toward the individual, it prompts them to sway posteriorly, and subsequently, there is little room for error, which results in the individual needing to quickly shift their COM anteriorly to prevent their center of gravity (COG) from going outside of their BOS in the posterior direction, hence the significantly greater postural sway when the moving room is unexpectedly moving toward the individual than when moving away from the individual.
Our similar previous study involved the assessment of postural stability when the front wall of a virtual room alone moved toward the participants unexpectedly and expectedly [
6]. In the current study, medial–lateral and anterior–posterior excursions were higher than the values reported in the previous study, indicating greater postural instability in the current study when considering COP excursions. Factors such as the visual perturbation changing from a virtual moving wall in the previous study to an actual moving room, and the use of a different force platform should be considered when comparing the results from the two studies. With the previous study using a virtual moving wall [
6], through which only the central vision was manipulated, individuals might rely more on their peripheral vision as the two side walls of the virtual room remained stationary. However, in the current study, both the front wall and the two side virtual walls moved toward and away from the participants, through which not only the participants’ central vision but also their peripheral vision were manipulated, which could be additional reasons for an increase in postural instability. Based on the findings from the current study, a virtual moving room paradigm can be used to induce postural perturbations that challenge the postural control system even in healthy adults. Although this postural control behavior is based on acute exposure to the virtual moving room, the effects during chronic exposure and subsequent postural control adaptations are still unknown and offer more opportunities for further research.
While these findings offer insights into the impact of the novel Vroom paradigm on postural control responses, they merely reflect responses to a virtual and visual perturbation to the postural control system. These responses are not indicative of physical postural perturbations, as observed in treadmill-based PBBT. However, the inclusion of the Vroom paradigm in traditional balance measures such as Berg’s balance test or computerized dynamic posturography tools such as the sensory organization test can aid in the further understanding and assessment of the postural control system.
4.2. Subjective VR Experience
The surveys conducted revealed that the participants felt a strong sense of immersion, experienced little simulator sickness, and had greater balance confidence after exposure to the virtual environments. The PQ scores in the current study (94.4 ± 12.21) were similar to previously reported PQ scores (98.11 ± 15.78) [
22], suggesting that the individuals had a successful perception and realistic immersion in the exposed VE. The BCS was used to test the participants’ perception of their balance confidence. The BCS was previously validated on healthy young adults, with their scores ranging from 34% to 79.6%, with a mean score of 56 ± 12.5% [
23]. The total score obtained by summing the responses to all questions (maximum 80) was expressed as a percentage ranging from 0 to 100, with 0 reflecting “not confident at all” and 100 reflecting “extremely confident”. In the current study, the scores ranged from 10 to 67 with a mean score of 42.9 (53.6%) for the pre-test and from 11 to 72 with a mean score of 45.77 (57.2%) for the post-test. These findings suggest that the unexpected and expected visual perturbations resulted in the participants’ balance confidence increasing significantly compared with their pre-test scores, providing evidence that the virtual moving room paradigm can potentially be used as a postural stability and balance training tool. More specifically, it supports the hypothesis that balance confidence would increase after being exposed to the virtual and visual perturbations challenging the postural control system. However, these findings are only based on acute exposure, and long-term adaptations to the virtual moving room are still unknown. Finally, the findings from the SSQ revealed that the post-expected scores were significantly higher than the pre-test scores, also supporting previous research [
29]. This suggests that the longer the duration one remains in a VE, the more likely the experience of simulator sickness, but the mean scores for all conditions were significantly lower than five, suggesting that no adverse effects of simulator sickness due to the virtual moving room paradigm.
4.3. Limitations and Future Research
There are many potential limitations to consider with this study. First, the study was conducted on healthy individuals with no pre-existing clinical conditions that can impact postural control behavior. Hence, the Vroom paradigm might produce different results among elderly or clinical populations. Additionally, future studies using the Vroom paradigm in such populations should enforce caution as there is a risk for falls and simulator sickness. Another limitation to consider is that the preset order of unexpected and expected trials could potentially induce a learning effect in the moving room. However, if the expected trials were to be conducted first, there would be no true unexpected trials. To minimize any such undue effects, in both unexpected and expected trials, the participants did not know the moving direction of the virtual moving room and the order in which the direction was randomized. Another limitation to consider is the preset velocity of the Vroom, as faster or slower velocities could cause different postural stability behaviors. However, this velocity was chosen based on several preliminary testing trials. Finally, all the observed findings in the current study are due to acute exposure to the VE, the HMD, and the virtual moving room paradigm; hence, the results should be interpreted with caution, and more research on chronic exposure is warranted to assess any postural control adaptations and learning. Future studies like the current one should provide varying instructions on where to focus (internally or externally) to determine if external focus is the reason for increased postural stability with the HMD compared to no HMD. Future research on this topic should include biomechanical and cognitive measures such as 3D motion capture, electromyography (EMG) and electromyography (EEG), eye tracking, and tests of individuals performing various types of sensorimotor tasks [
30], in both general and clinical populations to better understand the postural control system during the Vroom paradigm.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}