
On the Optimal Whole-Body Vibration Protocol for Muscle Strength

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
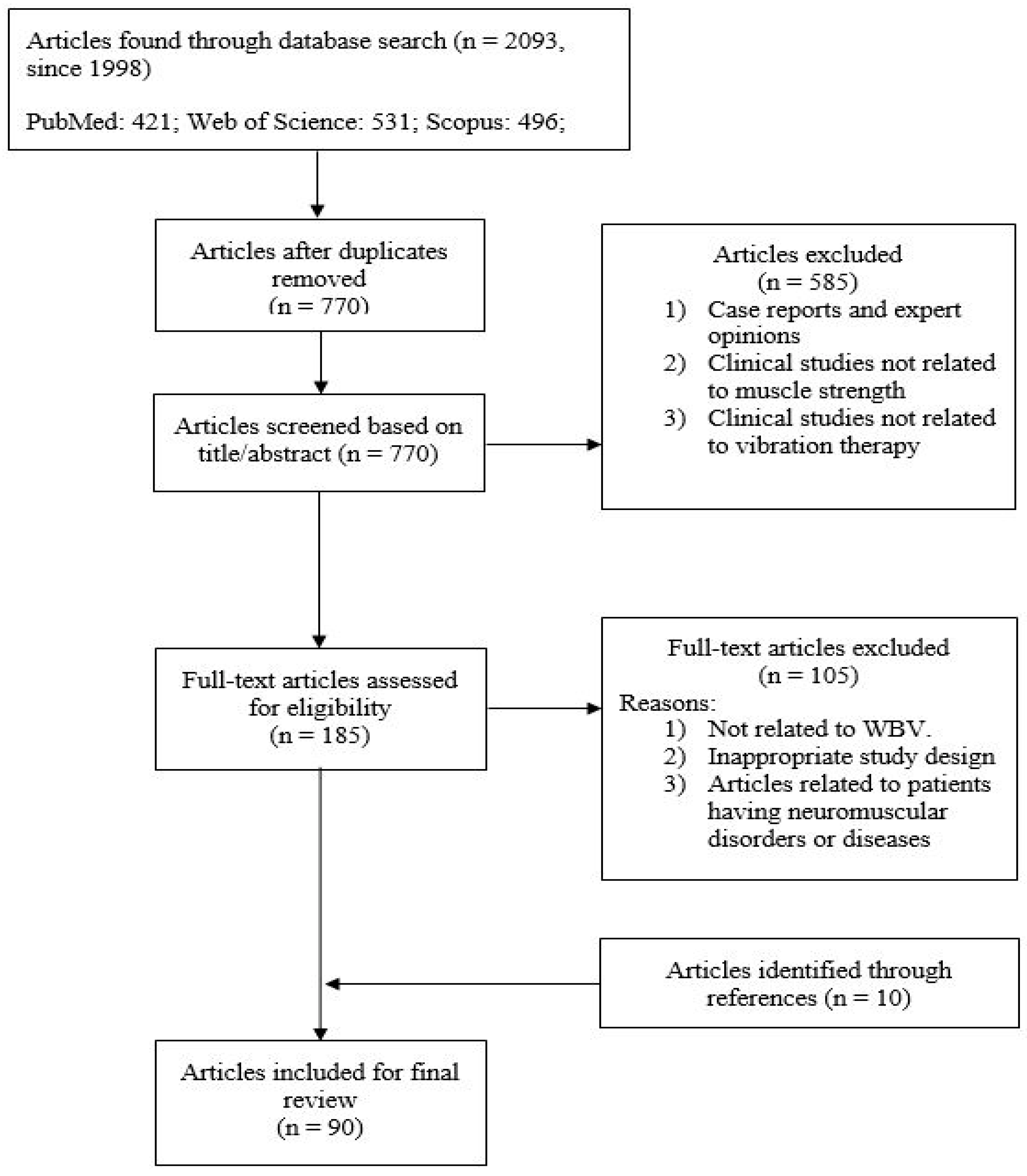
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Results of Literature Search
3. Results
3.1. Clinical Studies on Effects of Whole Body Vibration on Muscle in Standing Position
3.2. Clinical Studies on Effects of WBV on Muscle with Postures Other Than Standing
3.3. Adverse Effects of Vibration on Human Body
3.4. Optimal Vibration Protocol
4. Discussion
4.1. Optimal Vibration Protocol
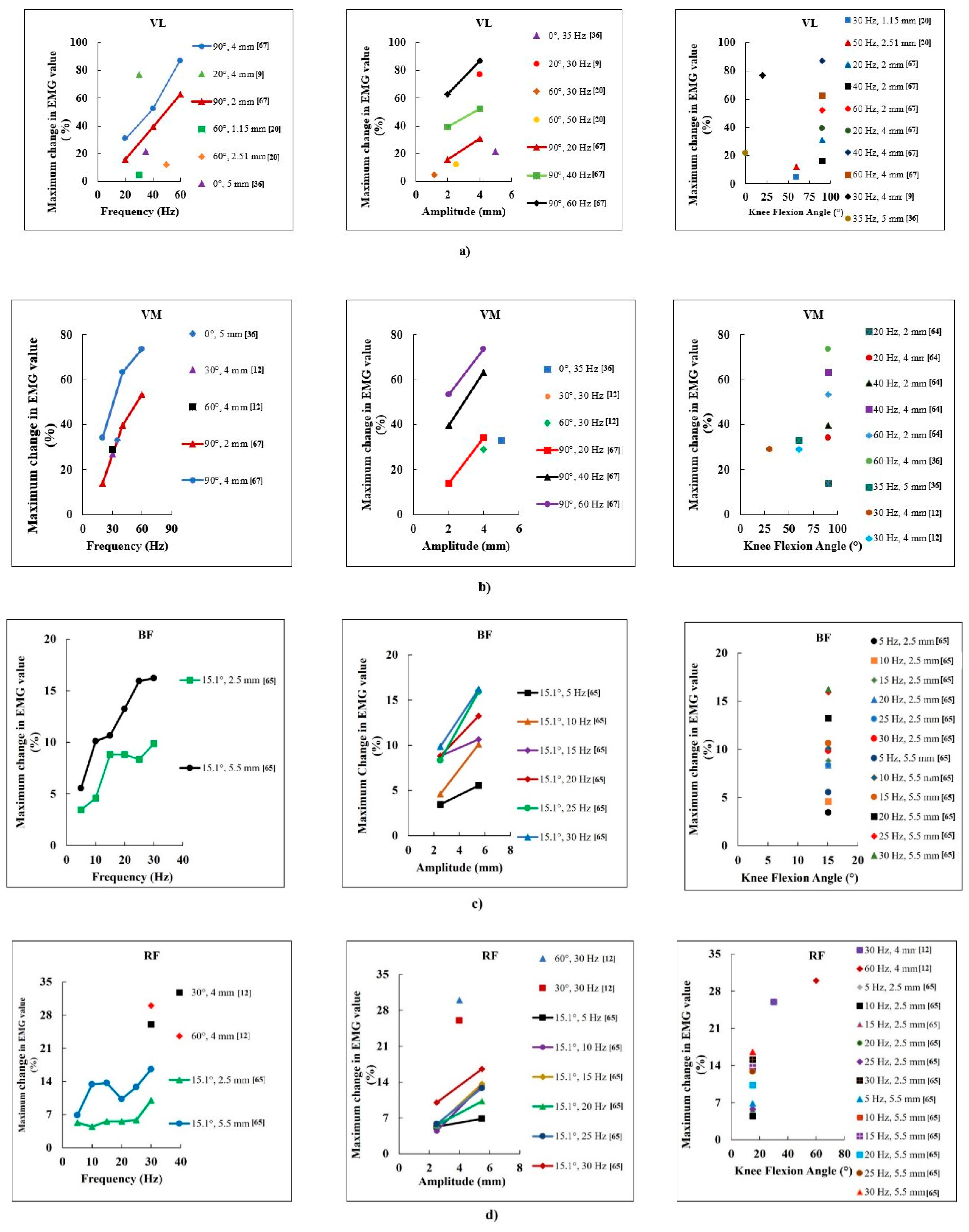
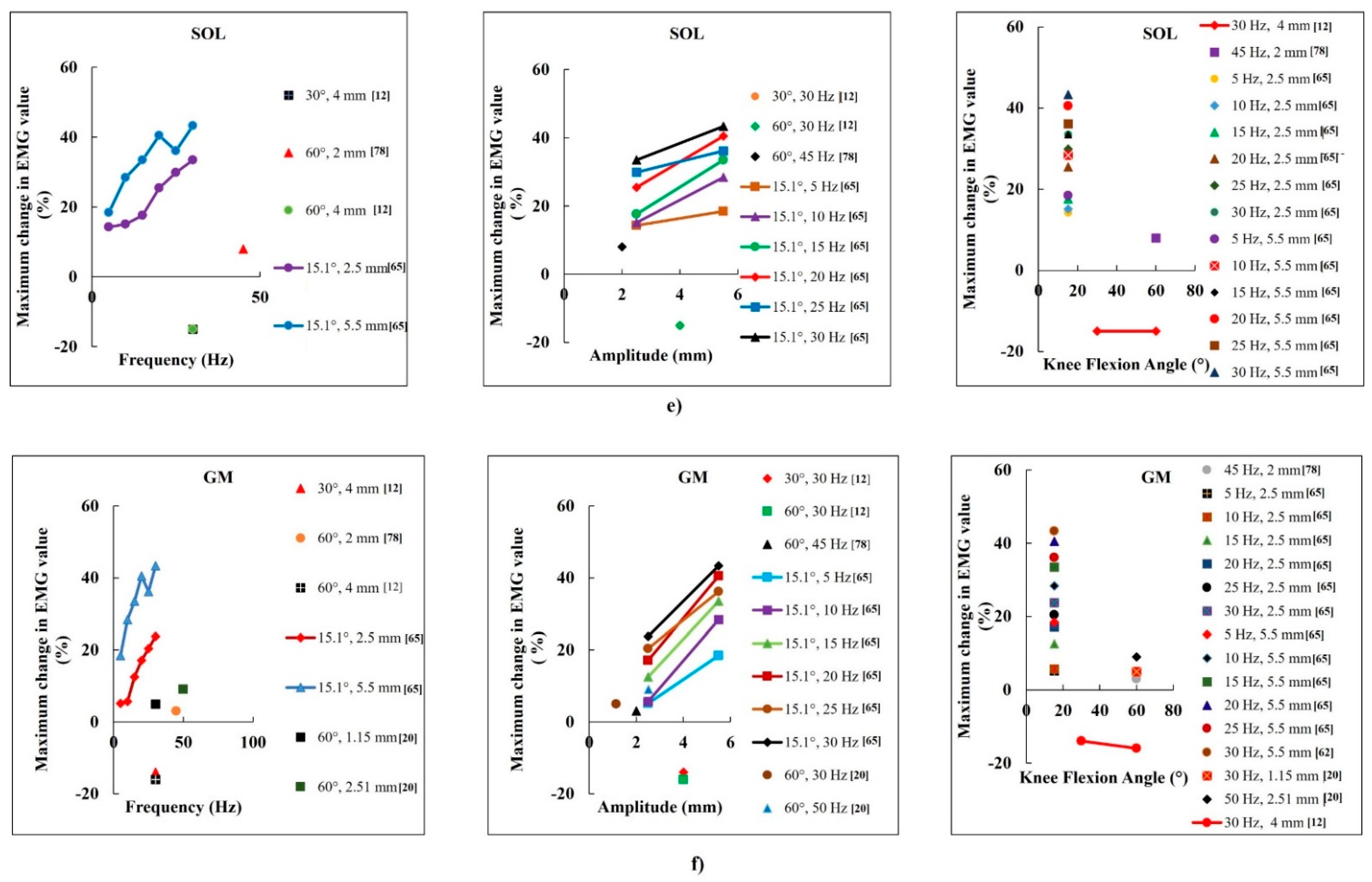
4.1.1. Optimal Vibration Frequency
4.1.2. Optimal Amplitude
4.1.3. Effects of Knee Flexion Angle
4.1.4. Effects of Posture and Muscle Type
4.1.5. Vibration Mode
4.2. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arora, N.K.; Sharma, S.; Saifi, S.; Sharma, S.; Arora, I.K. Effects of combined whole body vibration and resistance training on lower quadrants electromyographic activity, muscle strength and power in athletes. Foot 2021, 49, 101844. [Google Scholar] [CrossRef]
- Wu, S.; Ning, H.-T.; Xiao, S.-M.; Hu, M.-Y.; Wu, X.-Y.; Deng, H.-W.; Feng, H. Effects of vibration therapy on muscle mass, muscle strength and physical function in older adults with sarcopenia: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Ritzmann, R.; Kramer, A.; Gruber, M.; Gollhofer, A.; Taube, W. EMG activity during whole body vibration: Motion artifacts or stretch reflexes? Eur. J. Appl. Physiol. 2010, 110, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Masud, M.C.A.; Luk, H.Y.; Shen, C.L. Impact of Local Vibration Training on Neuromuscular Activity, Muscle Cell, and Muscle Strength: A Review. Crit. Rev. Biomed. Eng. 2022, 50, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Rigoni, I.; Bonci, T.; Bifulco, P.; Fratini, A. Characterisation of the transient mechanical response and the electromyographical activation of lower leg muscles in whole body vibration training. Sci. Rep. 2022, 12, 6232. [Google Scholar] [CrossRef]
- Pollock, R.D.; Woledge, R.; Martin, F.C.; Newham, D. Effects of whole body vibration on motor unit recruitment and threshold. J. Appl. Physiol. 2012, 112, 388–395. [Google Scholar] [CrossRef] [Green Version]
- Cardinale, C.; Bosco, M. The use of vibration as an exercise intervention. Exerc. Sport Sci. Rev. 2003, 31, 3–7. [Google Scholar] [CrossRef]
- Alizadeh-Meghrazi, M.; Masani, K.; Zariffa, J.; Sayenko, D.G.; Popovic, M.R.; Craven, B.C. Effect of whole-body vibration on lower-limb EMG activity in subjects with and without spinal cord injury. J. Spinal Cord Med. 2014, 37, 525–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abercromby, A.F.J.; Amonette, W.E.; Layne, C.S.; Mcfarlin, B.K.; Hinman, M.R.; Paloski, W.H. Vibration Exposure and Biodynamic Responses during Whole-Body Vibration Training. Med. Sci. Sports Exerc. 2007, 39, 1794–1800. [Google Scholar] [CrossRef]
- Hazell, T.J.; Jakobi, J.M.; Kenno, K.A. The effects of whole-body vibration on upper- and lower-body EMG during static and dynamic contractions. Appl. Physiol. Nutr. Metab. 2007, 32, 1156–1163. [Google Scholar] [CrossRef]
- Cochrane, D.J.; Loram, I.D.; Stannard, S.R.; Rittweger, J. Changes in joint angle, muscle-tendon complex length, muscle contractile tissue displacement, and modulation of EMG activity during acute whole-body vibration. Muscle Nerve 2009, 40, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Ritzmann, R.; Gollhofer, A.; Kramer, A. The influence of vibration type, frequency, body position and additional load on the neuromuscular activity during whole body vibration. Eur. J. Appl. Physiol. 2012, 113, 1–11. [Google Scholar] [CrossRef]
- Lienhard, K.; Cabasson, A.; Meste, O.; Colson, S.S. Determination of the optimal parameters maximizing muscle activity of the lower limbs during vertical synchronous whole-body vibration. Eur. J. Appl. Physiol. 2014, 114, 1493–1501. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilzadeh, S.; Akpinar, M.; Polat, S.; Yildiz, A.; Oral, A. The effects of two different frequencies of whole-body vibration on knee extensors strength in healthy young volunteers: A randomized trial. J. Musculoskelet. Neuronal Interact. 2015, 15, 333–340. [Google Scholar] [CrossRef] [Green Version]
- Woo, H.J.; Yu, M.; Kwon, T.K. Effect of Whole Body Vibration Conditions on Lower Limb Muscles during Sling Exercise. Appl. Sci. 2022, 12, 1299. [Google Scholar] [CrossRef]
- Abercromby, A.F.J.; Amonette, W.E.; Layne, C.S.; Mcfarlin, B.K.; Hinman, M.R.; Paloski, W.H. Variation in Neuromuscular Responses during Acute Whole-Body Vibration Exercise. Med. Sci. Sports Exerc. 2007, 39, 1642–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avelar, N.C.; Ribeiro, V.G.; Mezêncio, B.; Fonseca, S.F.; Tossige-Gomes, R.; da Costa, S.J.; Szmuchrowski, L.; Gripp, F.; Coimbra, C.; Lacerda, A.C. Influence of the knee flexion on muscle activation and transmissibility during whole body vibration. J. Electromyogr. Kinesiol. 2013, 23, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Harijanto, C.; Lim, A.; Vogrin, S.; Duque, G. Does Whole-Body Vibration Training Have a Concurrent Effect on Bone and Muscle Health? A Systematic Review and Meta-Analysis. Gerontology 2021, 68, 601–611. [Google Scholar] [CrossRef]
- Bush, J.A.; Blog, G.L.; Kang, J.; Faigenbaum, A.D.; Ratamess, N.A. Effects of Quadriceps Strength After Static and Dynamic Whole-Body Vibration Exercise. J. Strength Cond. Res. 2015, 29, 1367–1377. [Google Scholar] [CrossRef]
- Marín, P.J.; Hazell, T.; García-Gutiérrez, M.T.; Cochrane, D.J. Acute unilateral leg vibration exercise improves contralateral neuromuscular performance. J. Musculoskelet. Neuronal Interact. 2014, 14, 58–67. [Google Scholar] [PubMed]
- Rønnestad, B.R. Acute Effects of Various Whole Body Vibration Frequencies on 1RM in Trained and Untrained Subjects. J. Strength Cond. Res. 2009, 23, 2068–2072. [Google Scholar] [CrossRef]
- Torvinen, S.; Kannus, P.; Sievänen, H.; Jarvinen, T.A.; Pasanen, M.; Kontulainen, S.; Nenonen, A.; Järvinen, T.L.; Paakkala, T.; Järvinen, M.; et al. Effect of 8-Month Vertical Whole Body Vibration on Bone, Muscle Performance, and Body Balance: A Randomized Controlled Study. J. Bone Miner. Res. 2003, 18, 876–884. [Google Scholar] [CrossRef]
- Bemben, D.; Stark, C.; Taiar, R.; Bernardo-Filho, M. Relevance of Whole-Body Vibration Exercises on Muscle Strength/Power and Bone of Elderly Individuals. Dose-Response SAGE J. 2018, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alam, M.M.; Khan, A.A.; Farooq, M. Effect of whole-body vibration on neuromuscular performance: A literature review. Work 2018, 59, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Weng, C.; Liu, M.; Wang, Q.; Liu, L.; He, Y. Effect of whole-body vibration exercise on mobility, balance ability and general health status in frail elderly patients: A pilot randomized controlled trial. Clin. Rehabil. 2013, 28, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Yao, D.; Jakubowitz, E.; Ettinger, S.; Claassen, L.; Plaass, C.; Stukenborg-Colsman, C.; Daniilidis, K. Functional electrostimulation for drop foot treatment: Clinical outcome|Funktionelle Elektrostimulation zur Therapie des neurogenen Fallfußes: Klinisches Outcome. Orthopade 2016, 46, 227–233. [Google Scholar] [CrossRef]
- Surowiec, R.K.; Wang, H.; Nagelkirk, P.R.; Frame, J.W.; Dickin, D.C. The Effects of Whole-Body Vibration on the Wingate Test for Anaerobic Power When Applying Individualized Frequencies. J. Strength Cond. Res. 2014, 28, 2035–2041. [Google Scholar] [CrossRef] [Green Version]
- Siu, P.M.; Tam, B.T.; Chow, D.H.; Guo, J.-Y.; Huang, Y.-P.; Zheng, Y.-P.; Wong, S.H. Immediate Effects of 2 Different Whole-Body Vibration Frequencies on Muscle Peak Torque and Stiffness. Arch. Phys. Med. Rehabil. 2010, 91, 1608–1615. [Google Scholar] [CrossRef]
- Sitjà-Rabert, M.; Martínez-Zapata, M.J.; Fort-Vanmeerhaeghe, A.; Rey-Abella, F.; Romero-Rodriguez, D.; Bonfill, X. Whole body vibration for older persons: An open randomized, multicentre, parallel, clinical trial. BMC Geriatr. 2011, 11, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simão, A.P.; Mendonça, V.A.; Avelar, N.C.P.; da Fonseca, S.F.; Santos, J.M.; de Oliveira, A.C.C.; Tossige-Gomes, R.; Ribeiro, V.G.C.; Neves, C.D.C.; Balthazar, C.H.; et al. Whole Body Vibration Training on Muscle Strength and Brain-Derived Neurotrophic Factor Levels in Elderly Woman with Knee Osteoarthritis: A Randomized Clinical Trial Study. Front. Physiol. 2019, 10, 756. [Google Scholar] [CrossRef] [PubMed]
- Perchthaler, D.; Grau, S.; Hein, T. Evaluation of a Six-Week Whole-Body Vibration Intervention on Neuromuscular Performance in Older Adults. J. Strength Cond. Res. 2015, 29, 86–95. [Google Scholar] [CrossRef]
- Morel, D.S.; Marín, P.J.; Moreira-Marconi, E.; Dionello, C.F.; Bernardo-Filho, M. Can Whole-Body Vibration Exercises in Different Positions Change Muscular Activity of Upper Limbs? A Randomized Trial. Dose-Response 2018, 16, 1559325818804361. [Google Scholar] [CrossRef] [PubMed]
- Dallas, G.; Mavvidis, A.; Kirialanis, P.; Papouliakos, S. The effect of 8 weeks of whole body vibration training on static balance and explosive strength of lower limbs in physical education students. Acta Gymnica 2017, 47, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Dallas, G.; Savvathi, A.; Dallas, K.; Maridaki, M. The effect of 6-weeks whole body vibration on muscular performance on young non-competitive female artistic gymnasts. Sci. Gymnast. J. 2019, 11, 151–162. [Google Scholar]
- Da Silva-Grigoletto, M.E.; De Hoyo, M.; Sañudo, B.; Carrasco, L.; García-Manso, J.M. Determining the Optimal Whole-Body Vibration Dose–response Relationship for Muscle Performance. J. Strength Cond. Res. 2011, 25, 3326–3333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annino, G.; Iellamo, F.; Palazzo, F.; Fusco, A.; Lombardo, M.; Campoli, F.; Padua, E. Acute changes in neuromuscular activity in vertical jump and flexibility after exposure to whole body vibration. Medicine 2017, 96, e7629. [Google Scholar] [CrossRef] [PubMed]
- Bulhões, L.C.C.; Vieira, E.R.; Borges, D.T.; Melo, S.A.; Cavalcanti, R.L.; da Costa, K.S.A.; Gomes, S.R.A.; Macedo, L.D.B.; Brasileiro, J.S. Whole Body Vibration on the Neuromuscular Performance of Elderls: Randomized Controlled Trial. Phys. Occup. Ther. Geriatr. 2022, 1–14. [Google Scholar] [CrossRef]
- Tseng, S.-Y.; Ko, C.-P.; Tseng, C.-Y.; Huang, W.-C.; Lai, C.-L.; Wang, C.-H. Is 20 Hz Whole-Body Vibration Training Better for Older Individuals than 40 Hz? Int. J. Environ. Res. Public Health 2021, 18, 11942. [Google Scholar] [CrossRef] [PubMed]
- Law, T.D.; Clark, L.A.; Clark, B.C. Resistance Exercise to Prevent and Manage Sarcopenia and Dynapenia. Annu. Rev. Gerontol. Geriatr. 2016, 36, 205–228. [Google Scholar] [CrossRef] [Green Version]
- Wei, N.; Ng, G.Y.F. The effect of whole body vibration training on quadriceps voluntary activation level of people with age-related muscle loss (sarcopenia): A randomized pilot study. BMC Geriatr. 2018, 18, 240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosco, C.; Colli, R.; Introini, E.; Cardinale, M.; Tsarpela, O.; Madella, A.; Tihanyi, J.; Viru, A. Adaptive responses of human skeletal muscle to vibration exposure. Clin. Physiol. 1999, 19, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Goudarzian, M.; Ghavi, S.; Shariat, A.; Shirvani, H.; Rahimi, M. Effects of whole body vibration training and mental training on mobility, neuromuscular performance, and muscle strength in older men. J. Exerc. Rehabil. 2017, 13, 573–580. [Google Scholar] [CrossRef] [Green Version]
- Monteiro-Oliveira, B.B.; Coelho-Oliveira, A.C.; Paineiras-Domingos, L.L.; Sonza, A.; Sá-Caputo, D.D.C.D.; Bernardo-Filho, M. Use of surface electromyography to evaluate effects of whole-body vibration exercises on neuromuscular activation and muscle strength in the elderly: A systematic review. Disabil. Rehabil. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cristi-Montero, C.; Collado, P.S.; Márquez, S.; Garatachea, N.; Cuevas, M.J. Whole-body vibration training increases physical fitness measures without alteration of inflammatory markers in older adults. Eur. J. Sport Sci. 2013, 14, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.T.; Judge, S.; Malone, A.; Moynes, R.C.; Conviser, J.; Skinner, J.S. Effects of bioDensity Training and Power Plate Whole-Body Vibration on Strength, Balance, and Functional Independence in Older Adults. J. Aging Phys. Health Act. 2016, 24, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Hansson, T.; Magnusson, M.; Broman, H. Back muscle fatigue and seated whole body vibrations: An experimental study in man. Clin. Biomech. 1991, 6, 173–178. [Google Scholar] [CrossRef]
- Miller, R.M.; Heishman, A.D.; Freitas, E.; Bemben, M.G. Comparing the Acute Effects of Intermittent and Continuous Whole-Body Vibration Exposure on Neuromuscular and Functional Measures in Sarcopenia and Nonsarcopenic Elderly Women. Dose-Response 2018, 16, 1559325818797009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osawa, Y.; Oguma, Y.; Onishi, S. Effects of whole-body vibration training on bone-free lean body mass and muscle strength in young adults. J. Sports Sci. Med. 2011, 10, 97–104. [Google Scholar]
- Pujari, A.N.; Neilson, R.D.; Cardinale, M. Effects of different vibration frequencies, amplitudes and contraction levels on lower limb muscles during graded isometric contractions superimposed on whole body vibration stimulation. J. Rehabil. Assist. Technol. Eng. 2019, 6, 2055668319827466. [Google Scholar] [CrossRef] [Green Version]
- Osawa, Y.; Oguma, Y. Effects of resistance training with whole-body vibration on muscle fitness in untrained adults. Scand. J. Med. Sci. Sports 2011, 23, 84–95. [Google Scholar] [CrossRef]
- Krajnak, K.; Riley, D.A.; Wu, J.; Mcdowell, T.; Welcome, D.E.; Xu, X.S.; Dong, R.G. Frequency-dependent Effects of Vibration on Physiological Systems: Experiments with Animals and other Human Surrogates. Ind. Health 2012, 50, 343–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolan, A.J.; Govers, M.E.; Oliver, M.L. Effect of fatigue on muscle latency, muscle activation and perceived discomfort when exposed to whole-body vibration. Ergonomics 2021, 64, 1281–1296. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Martin, B.J. Contribution of the tonic vibration reflex to muscle stress and muscle fatigue. Scand. J. Work. Environ. Health 1993, 19, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, G. Human Body Vibration Exposure and its Measurement. J. Acoust. Soc. Am. 1983, 73, 2229. [Google Scholar] [CrossRef]
- Zhou, X.; Liu, Y.; Luo, M.; Zheng, S.; Yang, R.; Zhang, X. Overall and thermal comfort under different temperature, noise, and vibration exposures. Indoor Air 2022, 32, e12915. [Google Scholar] [CrossRef]
- Kat, C.-J.; Jooste, J.S.; Grant, C.C.; Becker, P.J.; Els, P.S. Cardiovascular response to whole-body vibration on an automobile seat. Ergonomics 2021, 64, 1405–1415. [Google Scholar] [CrossRef]
- Carlucci, F.; Felici, F.; Piccinini, A.; Haxhi, J.; Sacchetti, M. Individual Optimal Frequency in Whole-Body Vibration. J. Strength Cond. Res. 2016, 30, 3503–3511. [Google Scholar] [CrossRef]
- Wei, N.; Pang, M.Y.C.; Ng, S.S.; Ng, G.Y. Optimal frequency/time combination of whole body vibration training for developing physical performance of people with sarcopenia: A randomized controlled trial. Clin. Rehabil. 2017, 31, 1313–1321. [Google Scholar] [CrossRef]
- Petit, P.-D.; Pensini, M.; Tessaro, J.; Desnuelle, C.; Legros, P.; Colson, S.S. Optimal whole-body vibration settings for muscle strength and power enhancement in human knee extensors. J. Electromyogr. Kinesiol. 2010, 20, 1186–1195. [Google Scholar] [CrossRef]
- Curry, B.D.; Govindaraju, S.R.; Bain, J.L.; Zhang, L.L.; Yan, J.-G.; Matloub, H.S.; Riley, D.A. Evidence for frequency-dependent arterial damage in vibrated rat tails. Anat. Rec. Part A Discov. Mol. Cell. Evol. Biol. 2005, 284, 511–521. [Google Scholar] [CrossRef]
- Bovenzi, M.; D’Agostin, F.; Rui, F.; Negro, C. A longitudinal study of finger systolic blood pressure and exposure to hand-transmitted vibration. Int. Arch. Occup. Environ. Health 2007, 81, 613–623. [Google Scholar] [CrossRef]
- Bovenzi, M. Exposure-response relationship in the hand-arm vibration syndrome: An overview of current epidemiology research. Int. Arch. Occup. Environ. Health 1998, 71, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, M.; Lim, J. Electromyography activity of vastus lateralis muscle during whole-body vibrations of different frequencies. J. Strength Cond. Res. 2003, 17, 621–624. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.D.; Woledge, R.C.; Mills, K.R.; Martin, F.C.; Newham, D.J. Muscle activity and acceleration during whole body vibration: Effect of frequency and amplitude. Clin. Biomech. 2010, 25, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.-W.; Chou, L.-W.; Chen, W.-H.; Shiang, T.-Y.; Liu, C. Dual-frequency whole body vibration enhances vertical jumping and change-of-direction ability in rugby players. J. Sport Health Sci. 2015, 6, 346–351. [Google Scholar] [CrossRef] [Green Version]
- Perchthaler, D.; Horstmann, T.; Grau, S. Variations in neuromuscular activity of thigh muscles during whole-body vibration in consideration of different biomechanical variables. J. Sports Sci. Med. 2013, 12, 439–446. [Google Scholar]
- Krol, P.; Piecha, M.; Slomka, K.; Sobota, G.; Polak, A.; Juras, G. The effect of whole-body vibration frequency and amplitude on the myoelectric activity of vastus medialis and vastus lateralis. J. Sports Sci. Med. 2011, 10, 169–174. [Google Scholar]
- Chen, B.; Dong, Y.; Guo, J.; Zheng, Y.; Zhang, J.; Wang, X. Effects of Whole-Body Vibration on Lumbar-Abdominal Muscles Activation in Healthy Young Adults: A Pilot Study. Med. Sci. Monit. 2019, 25, 1945–1951. [Google Scholar] [CrossRef]
- Chung, P.; Liu, C.; Wang, H.; Liu, Y.; Chuang, L.; Shiang, T.-Y. Various performance-enhancing effects from the same intensity of whole-body vibration training. J. Sport Health Sci. 2016, 6, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Stania, M.; Król, P.; Sobota, G.; Polak, A.; Bacik, B.; Juras, G. The effect of the training with the different combinations of frequency and peak-to-peak vibration displacement of whole-body vibration on the strength of knee flexors and extensors. Biol. Sport 2017, 34, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Machado, A.; García-López, D.; González-Gallego, J.; Garatachea, N. Whole-body vibration training increases muscle strength and mass in older women: A randomized-controlled trial. Scand. J. Med. Sci. Sports 2009, 20, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Vibration, M. Shock—Evaluation of Human Exposure To Whole-Body Vibration—Part 1: General Requirements; International Organization for Standardization, ISO: Geneva, Switzerland, 1997. [Google Scholar]
- Da Silva, M.E.; Nunez, V.M.; Vaamonde, D.; Fernandez, J.M.; Poblador, M.S.; Garcia-Manso, J.M.; Lancho, J.L. Effects of different frequences of whole body vibration on muscular performance. Biol. Sport 2006, 23, 267. [Google Scholar]
- Games, K.E.; Sefton, J.M.; Wilson, A.E. Whole-Body Vibration and Blood Flow and Muscle Oxygenation: A Meta-Analysis. J. Athl. Train. 2015, 50, 542–549. [Google Scholar] [CrossRef] [Green Version]
- Chadefaux, D.; Moorhead, A.P.; Marzaroli, P.; Marelli, S.; Marchetti, E.; Tarabini, M. Vibration transmissibility and apparent mass changes from vertical whole-body vibration exposure during stationary and propelled walking. Appl. Ergon. 2020, 90, 103283. [Google Scholar] [CrossRef] [PubMed]
- Zaidell, L.N.; Pollock, R.D.; James, D.C.; Bowtell, J.L.; Newham, D.J.; Sumners, D.P.; Mileva, K.N. Lower body acceleration and muscular responses to rotational and vertical whole-body vibration at different frequencies and amplitudes. Dose-Response 2019, 17, 1559325818819946. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Finlayson, M.; Bethoux, F.; Su, X.; Dillon, L.; Maldonado, H.M. Effects of controlled whole-body vibration training in improving fall risk factors among individuals with multiple sclerosis: A pilot study. Disabil. Rehabil. 2018, 40, 553–560. [Google Scholar] [CrossRef]
- Harwood, B.; Scherer, J.; Brown, R.E.; Cornett, K.M.D.; Kenno, K.A.; Jakobi, J.M. Neuromuscular responses of the plantar flexors to whole-body vibration. Scand. J. Med. Sci. Sports 2016, 27, 1569–1575. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, J.; Osugi, T.; Yamazaki, M.; Takakuwa, M. Effect of a combination of whole body vibration exercise and squat training on body balance, muscle power, and walking ability in the elderly. Ther. Clin. Risk Manag. 2014, 10, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rees, S.S.; Murphy, A.J.; Watsford, M.L. Effects of Whole-Body Vibration Exercise on Lower-Extremity Muscle Strength and Power in an Older Population: A Randomized Clinical Trial. Phys. Ther. 2008, 88, 462–470. [Google Scholar] [CrossRef] [Green Version]
- Yung, M.; Lang, A.E.; Stobart, J.; Kociolek, A.M.; Milosavljevic, S.; Trask, C. The combined fatigue effects of sequential exposure to seated whole body vibration and physical, mental, or concurrent work demands. PLoS ONE 2017, 12, e0188468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osawa, Y.; Oguma, Y. Effects of whole-body vibration on resistance training for untrained adults. J. Sports Sci. Med. 2011, 10, 328–337. [Google Scholar]
- Blottner, D.; Salanova, M.; Püttmann, B.; Schiffl, G.; Felsenberg, D.; Buehring, B.; Rittweger, J.; Buehring, B.; Rittweger, J. Human skeletal muscle structure and function preserved by vibration muscle exercise following 55 days of bed rest. Eur. J. Appl. Physiol. 2006, 97, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Azizan, A.; Fard, M.; Azari, M.F.; Benediktsdóttir, B.; Arnardóttir, E.S.; Jazar, R.; Maeda, S. The influence of vibration on seated human drowsiness. Ind. Health 2016, 54, 296–307. [Google Scholar] [CrossRef] [Green Version]
- Beard, G.F.; Griffin, M.J. Discomfort during lateral acceleration: Influence of seat cushion and backrest. Appl. Ergon. 2013, 44, 588–594. [Google Scholar] [CrossRef] [Green Version]
- Azizan, M.A.; Fard, M.; Azari, M.F. Characterization of the effects of vibration on seated driver alertness. Nonlinear Eng. 2014, 3, 163–168. [Google Scholar] [CrossRef]
- Basri, B.; Griffin, M. Predicting discomfort from whole-body vertical vibration when sitting with an inclined backrest. Appl. Ergon. 2013, 44, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.; Griffin, M.J. Motion sickness with combined fore-aft and pitch oscillation: Effect of phase and the visual scene. Aviat. Space Environ. Med. 2009, 80, 946–954. [Google Scholar] [CrossRef] [PubMed]
- Satou, Y.; Ando, H.; Nakiri, M.; Nagatomi, K.; Yamaguchi, Y.; Hoshiko, M.; Tsuji, Y.; Muramoto, J.; Mori, M.; Hara, K.; et al. Effects of Short-Term Exposure to Whole-Body Vibration on Wakefulness Level. Ind. Health 2007, 45, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, J.A.; Griffin, M. Motion Sickness from Combined Lateral and Roll Oscillation: Effect of Varying Phase Relationships. Aviat. Space Environ. Med. 2007, 78, 944–950. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Masud, A.; Shen, C.-L.; Chyu, M.-C. On the Optimal Whole-Body Vibration Protocol for Muscle Strength. Biomechanics 2022, 2, 547-561. https://doi.org/10.3390/biomechanics2040043
Al Masud A, Shen C-L, Chyu M-C. On the Optimal Whole-Body Vibration Protocol for Muscle Strength. Biomechanics. 2022; 2(4):547-561. https://doi.org/10.3390/biomechanics2040043
Chicago/Turabian StyleAl Masud, Abdullah, Chwan-Li Shen, and Ming-Chien Chyu. 2022. "On the Optimal Whole-Body Vibration Protocol for Muscle Strength" Biomechanics 2, no. 4: 547-561. https://doi.org/10.3390/biomechanics2040043