
Can Slight Variations to Lateral Wedge Insoles Induce Significant Biomechanical Changes in Patients with Knee Osteoarthritis?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Equipment and Data Acquisition
2.3. Data Analysis
2.4. Statistical Analyses
3. Results
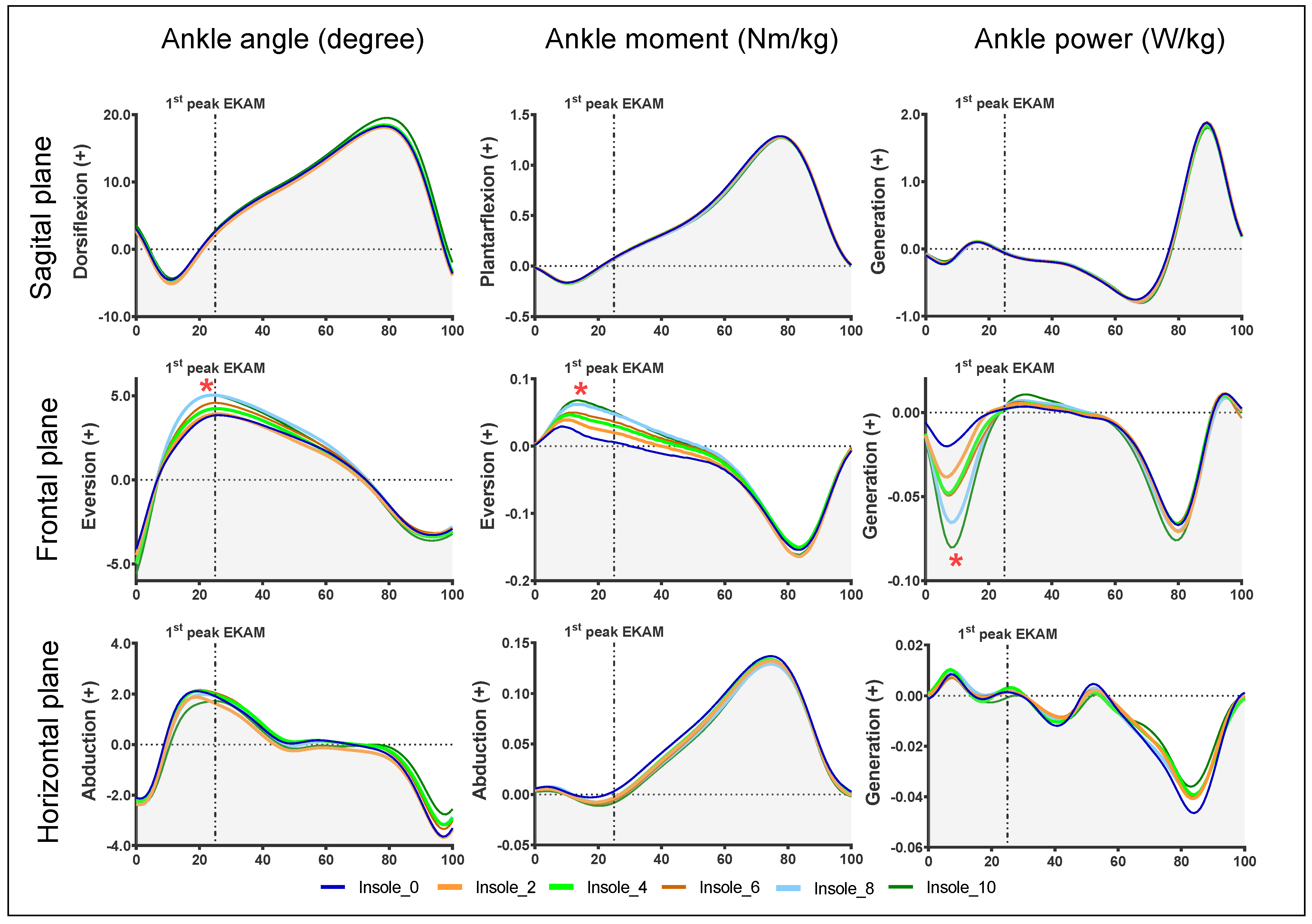
3.1. Ankle Biomechanical Parameters
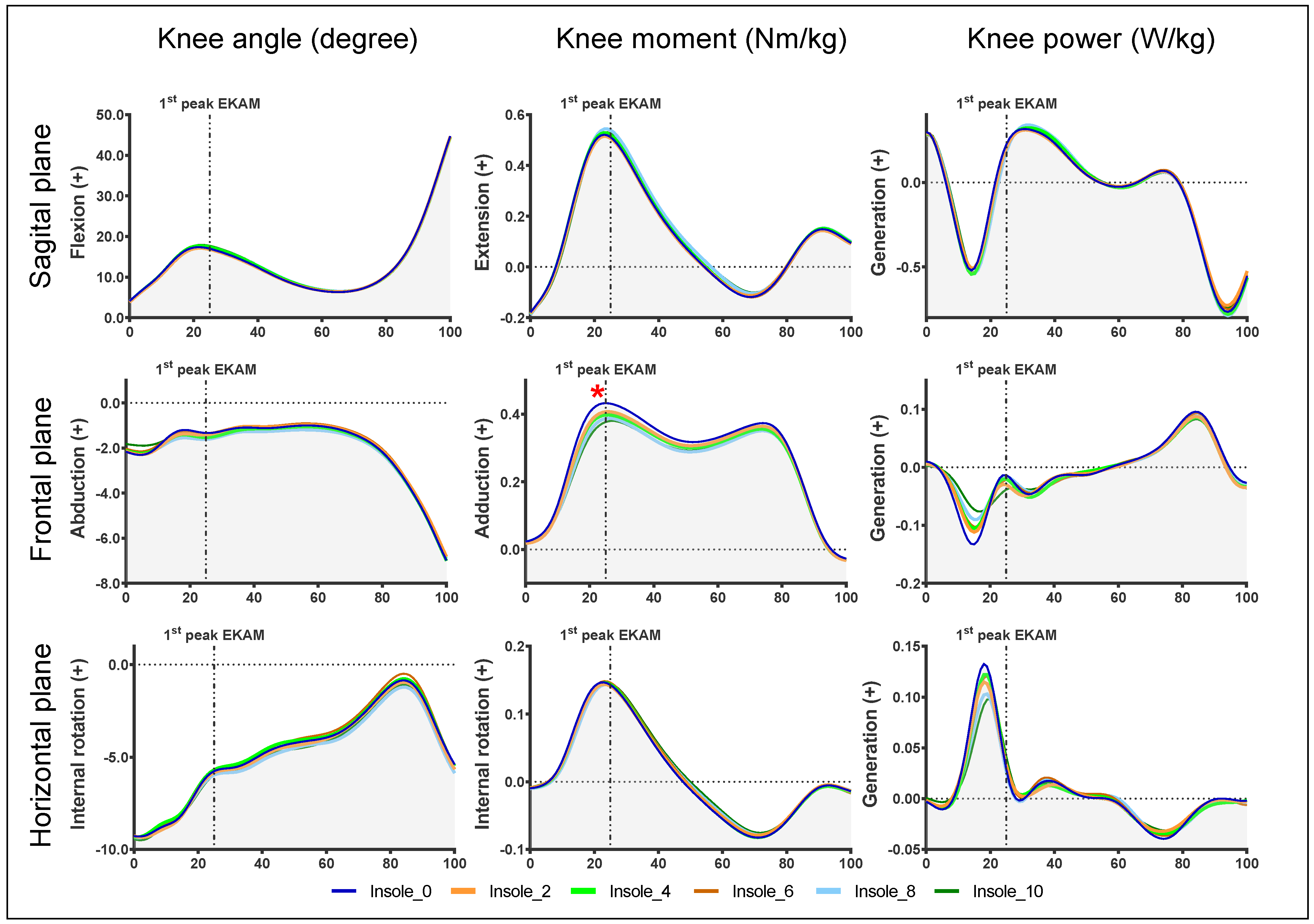
3.2. Knee Biomechanical Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Felson, D.T.; Zhang, Y.; Hannan, M.T.; Naimark, A.; Weissman, B.N.; Aliabadi, P.; Levy, D. The incidence and natural history of knee osteoarthritis in the elderly. The Framingham Osteoarthritis Study. Arthritis Rheum. 1995, 38, 1500–1505. [Google Scholar] [CrossRef]
- Buckley, J.G.; Scally, A.J.; Bhattacharjee, C. Living with Knee Osteoarthritis: The Positive Impact of Reducing the Knee Torque Induced When Sleeping Supine; A Randomised Clinical Trial. Biomechanics 2022, 2, 95–106. [Google Scholar] [CrossRef]
- Felson, D.T. Osteoarthritis as a disease of mechanics. Osteoarthr. Cartil./OARS Osteoarthr. Res. Soc. 2013, 21, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAlindon, T.E.; Bannuru, R.R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil./OARS Osteoarthr. Res. Soc. 2014, 22, 363–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, J.B.; Wong, D.X.; Jones, R.K.; Hill, C.L.; Thewlis, D. Lateral Wedge Insoles for Reducing Biomechanical Risk Factors for Medial Knee Osteoarthritis Progression: A Systematic Review and Meta-Analysis. Arthritis Care Res. 2016, 68, 936–951. [Google Scholar] [CrossRef] [Green Version]
- Hinman, R.S.; Bowles, K.A.; Metcalf, B.B.; Wrigley, T.V.; Bennell, K.L. Lateral wedge insoles for medial knee osteoarthritis: Effects on lower limb frontal plane biomechanics. Clin. Biomech. 2012, 27, 27–33. [Google Scholar] [CrossRef]
- Khosravi, M.; Babaee, T.; Daryabor, A.; Jalali, M. Effect of knee braces and insoles on clinical outcomes of individuals with medial knee osteoarthritis: A systematic review and meta-analysis. Assist. Technol. Off. J. RESNA 2021, 11, 1–17. [Google Scholar] [CrossRef]
- Telfer, S.; Lange, M.J.; Sudduth, A.S.M. Factors influencing knee adduction moment measurement: A systematic review and meta-regression analysis. Gait Posture 2017, 58, 333–339. [Google Scholar] [CrossRef]
- Kito, N.; Shinkoda, K.; Yamasaki, T.; Kanemura, N.; Anan, M.; Okanishi, N.; Ozawa, J.; Moriyama, H. Contribution of knee adduction moment impulse to pain and disability in Japanese women with medial knee osteoarthritis. Clin. Biomech. 2010, 25, 914–919. [Google Scholar] [CrossRef] [Green Version]
- Khosravi, M.; Arazpour, M.; Sharafat Vaziri, A. An evaluation of the use of a lateral wedged insole and a valgus knee brace in combination in subjects with medial compartment knee osteoarthritis (OA). Assist. Technol. Off. J. RESNA 2021, 33, 87–94. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Q.; Zhang, C. Ineffectiveness of lateral-wedge insoles on the improvement of pain and function for medial knee osteoarthritis: A meta-analysis of controlled randomized trials. Arch. Orthop. Trauma Surg. 2018, 138, 1453–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, V.; Machado, L.; Vilaca, A.; Xara-Leite, F.; Roriz, P. Effects of tailored lateral wedge insoles on medial knee osteoarthritis based on biomechanical analysis: 12-week randomized controlled trial. Clin. Rehabil. 2021, 35, 1235–1246. [Google Scholar] [CrossRef]
- Ferreira, V.; Simoes, R.; Goncalves, R.S.; Machado, L.; Roriz, P. The optimal degree of lateral wedge insoles for reducing knee joint load: A systematic review and meta-analysis. Arch. Physiother. 2019, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.K.; Chapman, G.J.; Parkes, M.J.; Forsythe, L.; Felson, D.T. The effect of different types of insoles or shoe modifications on medial loading of the knee in persons with medial knee osteoarthritis: A randomised trial. J. Orthop. Res. 2015, 33, 1646–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tipnis, R.A.; Anloague, P.A.; Laubach, L.L.; Barrios, J.A. The dose-response relationship between lateral foot wedging and the reduction of knee adduction moment. Clin. Biomech. 2014, 29, 984–989. [Google Scholar] [CrossRef]
- Felson, D.T.; Parkes, M.; Carter, S.; Liu, A.; Callaghan, M.J.; Hodgson, R.; Bowes, M.; Jones, R.K. The Efficacy of a Lateral Wedge Insole for Painful Medial Knee Osteoarthritis After Prescreening: A Randomized Clinical Trial. Arthritis Rheumatol. 2019, 71, 908–915. [Google Scholar] [CrossRef]
- Jones, R.K.; Chapman, G.J.; Forsythe, L.; Parkes, M.J.; Felson, D.T. The relationship between reductions in knee loading and immediate pain response whilst wearing lateral wedged insoles in knee osteoarthritis. J. Orthop. Res. 2014, 32, 1147–1154. [Google Scholar] [CrossRef] [Green Version]
- Hunt, M.A.; Takacs, J.; Krowchuk, N.M.; Hatfield, G.L.; Hinman, R.S.; Chang, R. Lateral wedges with and without custom arch support for people with medial knee osteoarthritis and pronated feet: An exploratory randomized crossover study. J. Foot Ankle Res. 2017, 10, 20. [Google Scholar] [CrossRef] [Green Version]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Cappozzo, A.; Catani, F.; Croce, U.D.; Leardini, A. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Ferreira, V.; Machado, L.; Vilaça, A.; Leite, F.X.; Roriz, P. Biomechanics performance in 30-s chair stand test in patients with medial knee osteoarthritis. Int. J. Hum. Factors Ergon. 2019, 6, 319–330. [Google Scholar] [CrossRef]
- Ferreira, V.; Machado, L.; Roriz, P. The effects on lower limbs kinematics of different lateral wedge insoles. J. Mech. Eng. Biomech. 2020, 4, 77–82. [Google Scholar] [CrossRef]
- Wen, C.; Cates, H.E.; Weinhandl, J.T.; Crouter, S.E.; Zhang, S. Knee biomechanics of patients with total knee replacement during downhill walking on different slopes. J. Sport Health Sci. 2022, 11, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Lewinson, R.T.; Worobets, J.T.; Stefanyshyn, D.J. Control conditions for footwear insole and orthotic research. Gait Posture 2016, 48, 99–105. [Google Scholar] [CrossRef]
- Documentation, C.-M.W. Visual3D Documentation. Available online: https://www.c-motion.com/v3dwiki/index.php?title=Visual3D_Documentation (accessed on 9 July 2022).
- Sawilowsky, S. New Effect Size Rules of Thumb. J. Mod. Appl. Stat. Methods 2009, 8, 597–599. [Google Scholar] [CrossRef]
- Chapman, G.J.; Parkes, M.J.; Forsythe, L.; Felson, D.T.; Jones, R.K. Ankle motion influences the external knee adduction moment and may predict who will respond to lateral wedge insoles?: An ancillary analysis from the SILK trial. Osteoarthr. Cartil./OARS Osteoarthr. Res. Soc. 2015, 23, 1316–1322. [Google Scholar] [CrossRef] [Green Version]
- Tse, C.T.F.; Ryan, M.B.; Hunt, M.A. Influence of foot posture on immediate biomechanical responses during walking to variable-stiffness supported lateral wedge insole designs. Gait Posture 2020, 81, 21–26. [Google Scholar] [CrossRef]
- Santilli, V.; Frascarelli, M.A.; Paoloni, M.; Frascarelli, F.; Camerota, F.; De Natale, L.; De Santis, F. Peroneus longus muscle activation pattern during gait cycle in athletes affected by functional ankle instability: A surface electromyographic study. Am. J. Sports Med. 2005, 33, 1183–1187. [Google Scholar] [CrossRef]
- Reeves, J.; Jones, R.; Liu, A.; Bent, L.; Plater, E.; Nester, C. A systematic review of the effect of footwear, foot orthoses and taping on lower limb muscle activity during walking and running. Prosthet. Orthot. Int. 2019, 43, 576–596. [Google Scholar] [CrossRef]
- Ludwig, O.; Kelm, J.; Frohlich, M. The influence of insoles with a peroneal pressure point on the electromyographic activity of tibialis anterior and peroneus longus during gait. J. Foot Ankle Res. 2016, 9, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatfield, G.L.; Cochrane, C.K.; Takacs, J.; Krowchuk, N.M.; Chang, R.; Hinman, R.S.; Hunt, M.A. Knee and ankle biomechanics with lateral wedges with and without a custom arch support in those with medial knee osteoarthritis and flat feet. J. Orthop. Res. 2016, 34, 1597–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, C.C.; Lee, Y.J.; Chen, B.; Aruin, A.S. Immediate and short-term effects of wearing a single textured insole on symmetry of stance and gait in healthy adults. Gait Posture 2016, 49, 190–195. [Google Scholar] [CrossRef]
- Jin, L. The Influence of Different Footwear Insole Stiffness on Center of Pressure and Ankle Kinematics during Walking: A Case Report. Biomechanics 2022, 2, 205–212. [Google Scholar] [CrossRef]
- Shaw, K.E.; Charlton, J.M.; Perry, C.K.L.; de Vries, C.M.; Redekopp, M.J.; White, J.A.; Hunt, M.A. The effects of shoe-worn insoles on gait biomechanics in people with knee osteoarthritis: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 238–253. [Google Scholar] [CrossRef] [Green Version]
- Kluge, F.; Krinner, S.; Lochmann, M.; Eskofier, B.M. Speed dependent effects of laterally wedged insoles on gait biomechanics in healthy subjects. Gait Posture 2017, 55, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Maly, M.R.; Culham, E.G.; Costigan, P.A. Static and dynamic biomechanics of foot orthoses in people with medial compartment knee osteoarthritis. Clin. Biomech. 2002, 17, 603–610. [Google Scholar] [CrossRef]
- Sawada, T.; Tanimoto, K.; Tokuda, K.; Iwamoto, Y.; Ogata, Y.; Anan, M.; Takahashi, M.; Kito, N.; Shinkoda, K. Rear foot kinematics when wearing lateral wedge insoles and foot alignment influence the effect of knee adduction moment for medial knee osteoarthritis. Gait Posture 2017, 57, 177–181. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Minimum | Maximum | Mean | Standard Deviation | |
|---|---|---|---|---|
| Age (years) | 45.0 | 78 | 61.6 | 8.4 |
| Height | 1.38 | 1.77 | 1.6 | 0.01 |
| Body mass index | 20.8 | 35.5 | 29.3 | 5.1 |
| (n = 38) | 0° Insole | 2° Insole | 4° Insole | 6° Insole | 8° Insole | 10° Insole |
|---|---|---|---|---|---|---|
| Peak ankle eversion [°] | 4.4 (±3.1) | 4.5 (±3.1) | 4.8 (±3.0) | 5.1 (±2.9) | 5.5 (±3.0) | 5.5 (±3.1) |
| p-values | 1.000 | 1.000 | 0.105 | 0.001 | 0.009 | |
| Cohen’s d | 0.052 | 0.136 | 0.232 | 0.374 | 0.364 | |
| Ankle eversion at 1st peak EKAM [°] | 3.8 (±3.1) | 3.9 (±3.0) | 4.3 (±3.0) | 4.6 (±3.0) | 5.0 (±3.1) | 4.9 (±3.3) |
| p-values | 1.000 | 1.000 | 0.087 | 0.000 | 0.018 | |
| Cohen’s d | 0.043 | 0.158 | 0.253 | 0.400 | 0.357 | |
| Peak ankle eversion moment [Nm/kg] | 0.052 (±0.039) | 0.061 (±0.038) | 0.066 (±0.040) | 0.074 (±0.044) | 0.080 (±0.039) | 0.087 (±0.044) |
| p-values | 0.197 | 0.696 | 0.043 | 0.000 | 0.000 | |
| Cohen’s d | 0.234 | 0.354 | 0.529 * | 0.718 * | 0.842 ** | |
| Ankle eversion moment at 1st peak EKAM [Nm/kg] | 0.020 (±0.065) | 0.032 (±0.062) | 0.041 (±0.058) | 0.050 (±0.062) | 0.058 (±0.056) | 0.060 (±0.067) |
| p-values | 0.104 | 0.000 | 0.000 | 0.000 | 0.000 | |
| Cohen’s d | 0.189 | 0.341 | 0.472 | 0.626 * | 0.606 * | |
| Peak ankle power absorption (frontal plane) [W/kg] | −0.097 (±0.055) | −0.113 (±0.064) | −0.109 (±0.062) | −0.114 (±0.069) | −0.122 (±0.064) | −0.138 (±0.072) |
| p-values | 0.173 | 0.357 | 0.222 | 0.004 | 0.000 | |
| Cohen’s d | 0.268 | 0.205 | 0.272 | 0.419 | 0.640 * | |
| 1st Peak EKAM [Nm/kg] | 0.452 (±0.183) | 0.428 (±0.181) | 0.421 (±0.182) | 0.424 (±0.189) | 0.410 (±0.183) | 0.402 (±0.182) |
| p-values | 0.005 | 0.000 | 0.000 | 0.000 | 0.000 | |
| Cohen’s d | 0.131 | 0.170 | 0.151 | 0.230 | 0.274 | |
| KAAI [Nm/kgxs] | 0.196 (±0.104) | 0.188 (±0.107) | 0.183 (±0.097) | 0.185 (±0.100) | 0.177 (±0.097) | 0.177 (±0.100) |
| p-values | 0.531 | 0.109 | 0.077 | 0.001 | 0.000 | |
| Cohen’s d | 0.076 | 0.129 | 0.108 | 0.189 | 0.186 | |
| Time to 1st peak EKAM [s] | 0.184 (±0.058) | 0.194 (±0.061) | 0.195 (±0.063) | 0.199 (±0.065) | 0.197 (±0.062) | 0.202 (±0.064) |
| p-values | 0.060 | 0.115 | 0.037 | 0.001 | 0.000 | |
| Cohen’s d | 0.168 | 0.182 | 0.244 | 0.217 | 0.295 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, V.; Machado, L.; Vilaça, A.; Xará-Leite, F.; Roriz, P. Can Slight Variations to Lateral Wedge Insoles Induce Significant Biomechanical Changes in Patients with Knee Osteoarthritis? Biomechanics 2022, 2, 342-351. https://doi.org/10.3390/biomechanics2030027
Ferreira V, Machado L, Vilaça A, Xará-Leite F, Roriz P. Can Slight Variations to Lateral Wedge Insoles Induce Significant Biomechanical Changes in Patients with Knee Osteoarthritis? Biomechanics. 2022; 2(3):342-351. https://doi.org/10.3390/biomechanics2030027
Chicago/Turabian StyleFerreira, Vitor, Leandro Machado, Adélio Vilaça, Francisco Xará-Leite, and Paulo Roriz. 2022. "Can Slight Variations to Lateral Wedge Insoles Induce Significant Biomechanical Changes in Patients with Knee Osteoarthritis?" Biomechanics 2, no. 3: 342-351. https://doi.org/10.3390/biomechanics2030027