
Electrospun Polyurethane Vascular Grafts for Cerebral Revascularization: A Pilot Study on Rats
 , , ,
, , , 
Abstract
:1. Introduction
2. Methods
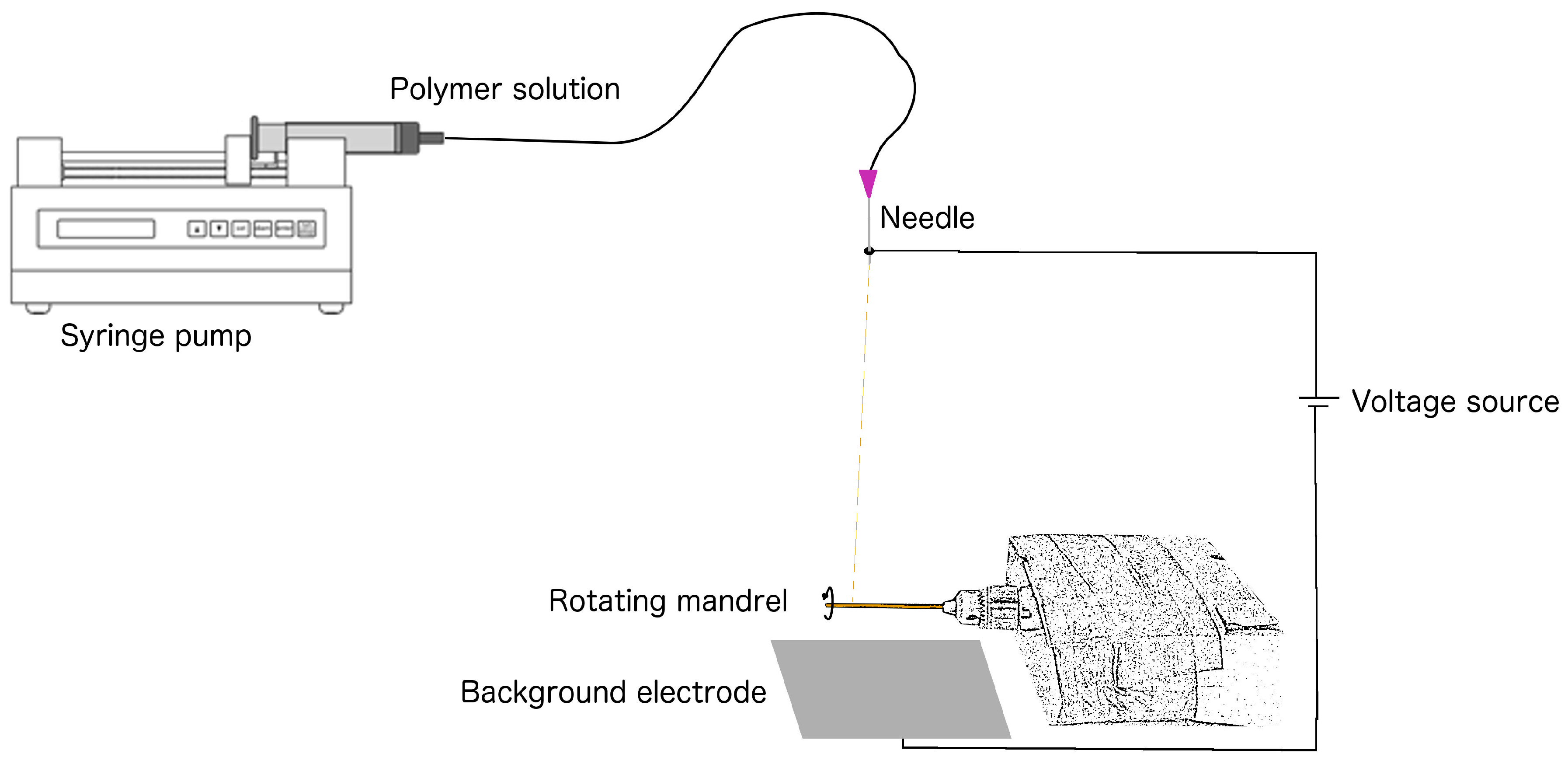
2.1. Graft Production: Polyurethane Solution and Electrospinning
2.2. SEM: ePU Graft Characterization
2.3. Animal Characterization and Grouping
2.4. Implantation of ePU Grafts
2.5. In Vivo Assessments over a 4-Month Period: Thrombosis
2.6. In Vivo Assessments after a 4-Month Period: Patency
2.7. Retrieval Surgery after 4-Month Period
2.8. Histological Assessments of Retrieved ePU Grafts: NIH and NE
2.9. Statistical Analyses
3. Results
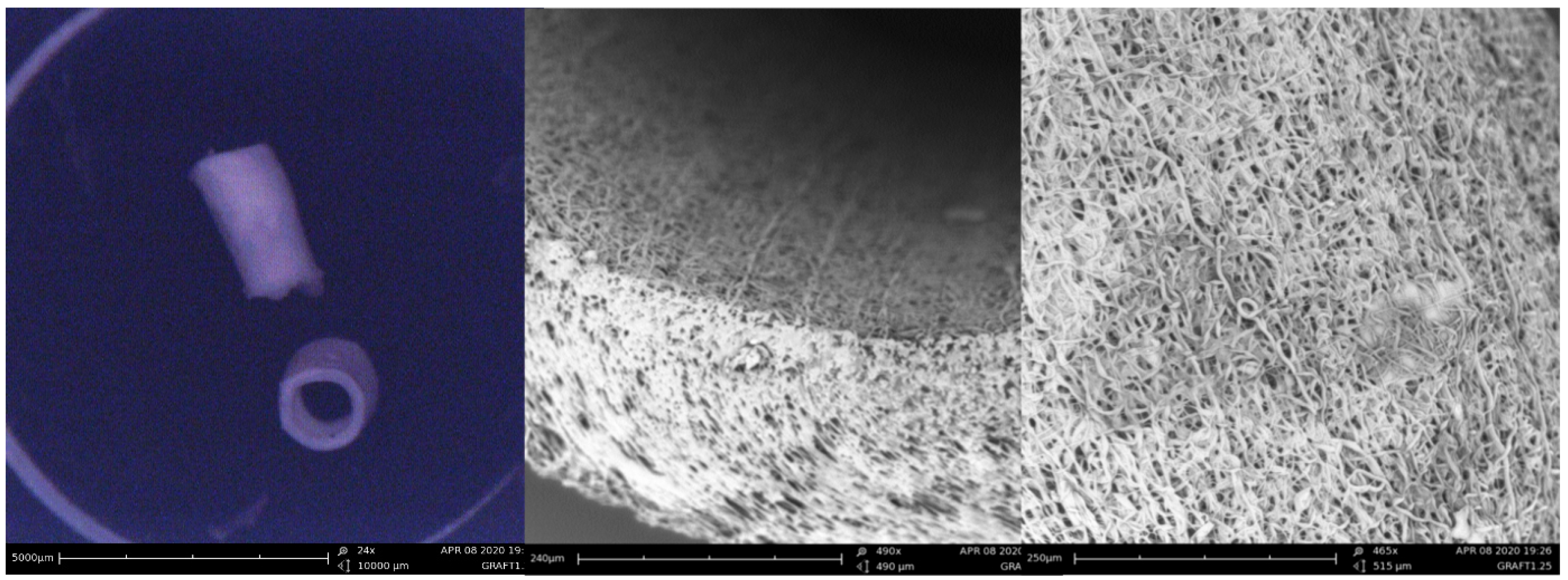
3.1. Pre-Implant Characterization: SEM
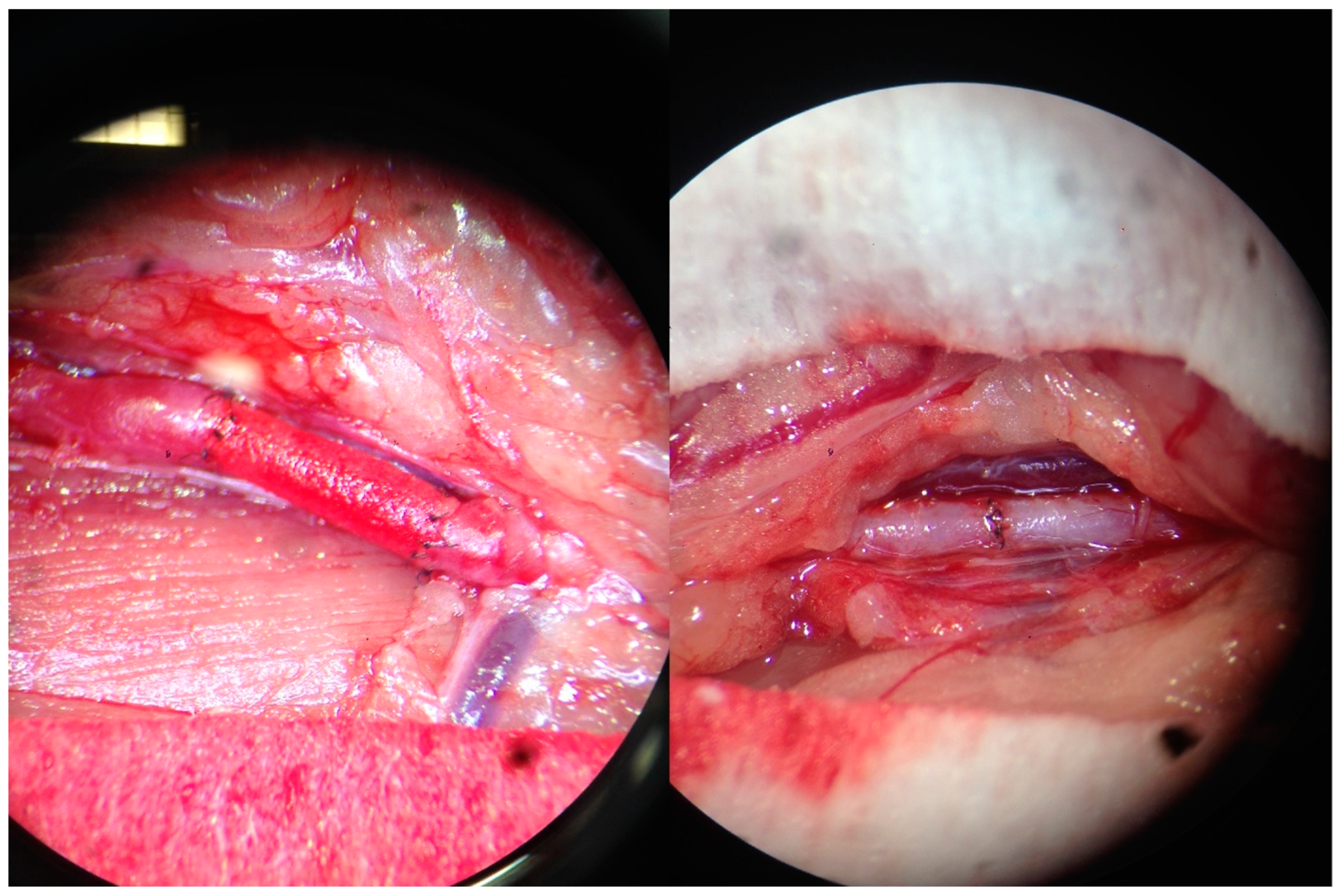
3.2. Implantation of ePU Grafts
3.3. In Vivo Assessments: Clinical Parameters of Thrombosis
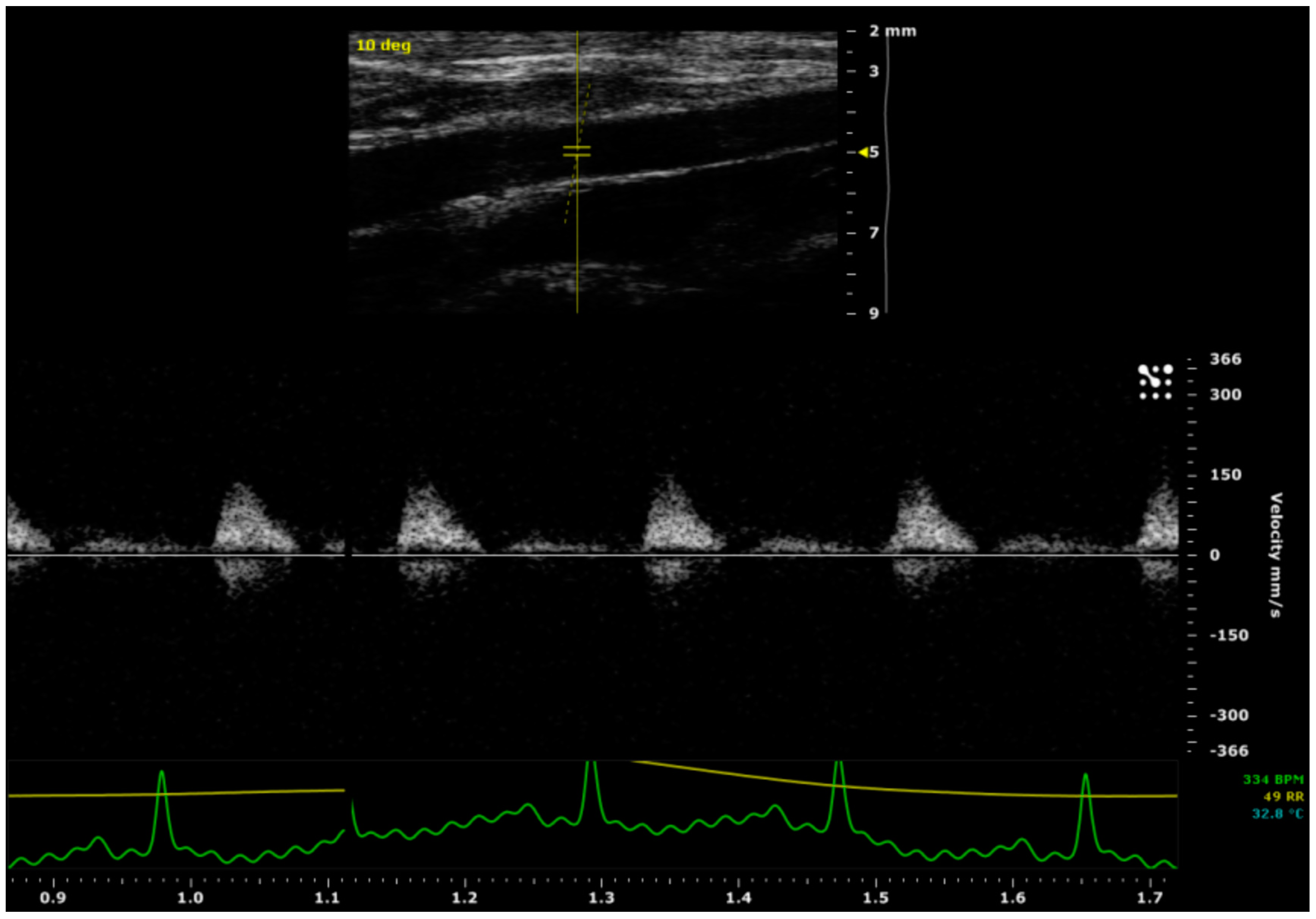
3.4. In Vivo Assessments: Patency on Ultrasound
3.5. Retrieval Surgery after a 4-Month Period
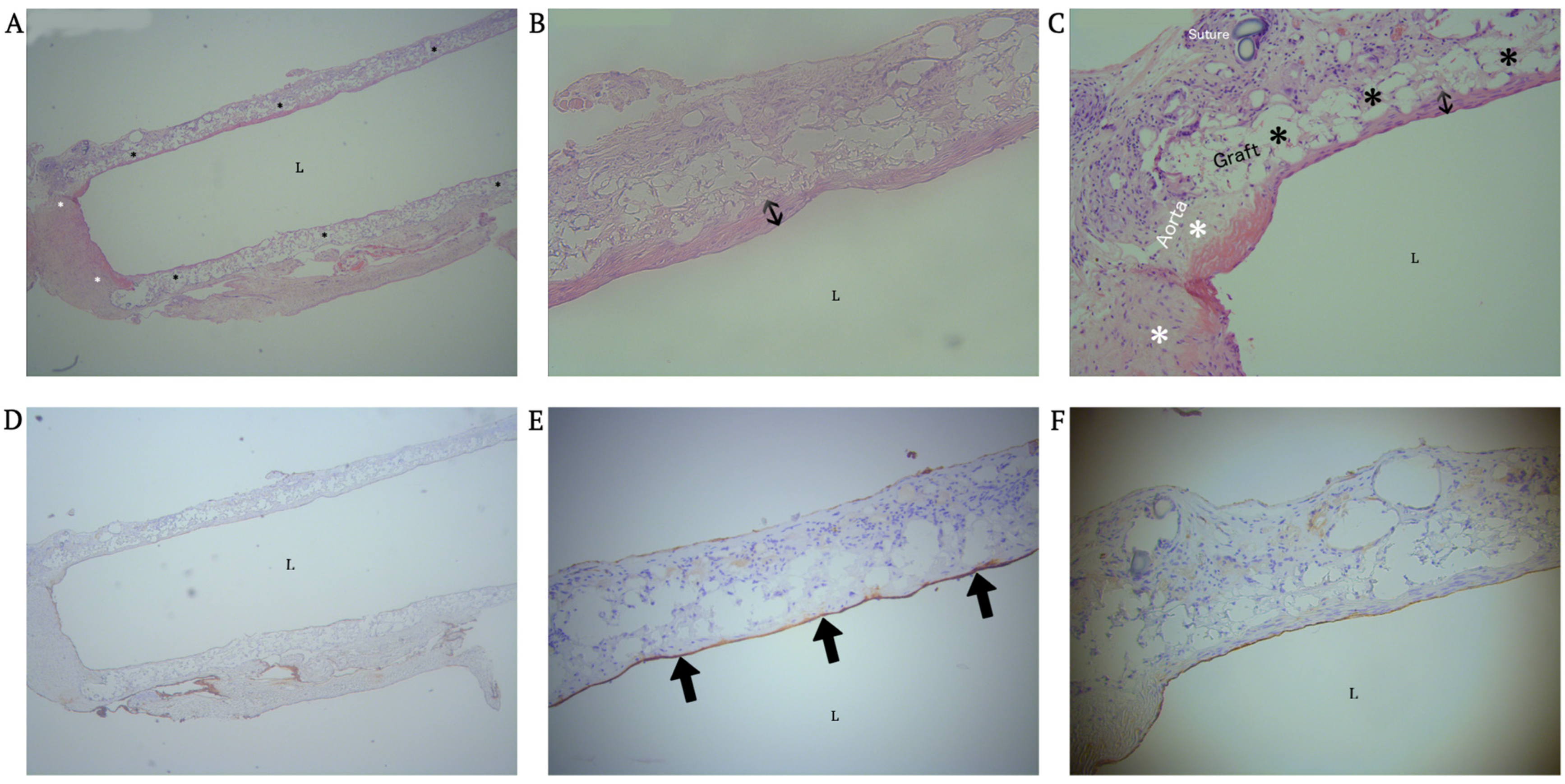
3.6. Histological Assessment: NIH and NE
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ePU | electrospun polyurethane |
| GSV | great saphenous vein |
| ID | inner diameter |
| IDps, IDpd, IDds, IDdd, ODps, ODpd, ODds and ODpd | inner/outer, proximal/distal diameters and systolic/diastolic diameters of graft/control aortas |
| NE | neo-endothalialization |
| NIH | neointimal hyperplasia |
| RA | radial artery |
| SEM | scanning electron microscopy |
References
- Charbel, F.; Amin-Hanjani, S. Decision making in cerebral revascularization surgery using intraoperative CBF measurements. In Cerebral Revascularization, 1st ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2011; p. 44. [Google Scholar]
- Liu, J.K.; Kan, P.; Karwande, S.V.; Couldwell, W.T. Conduits for cerebrovascular bypass and lessons learned from the cardiovascular experience. Neurosurg. Focus 2003, 14, e3. [Google Scholar] [CrossRef] [PubMed]
- Archie, J.P. Carotid endarterectomy saphenous vein patch rupture revisited: Selective use on the basis of vein diameter. J. Vasc. Surg. 1996, 24, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, M.; Abel, N. Stroke and occlusive cerebrovascular disease. In Greenberg Handbook of Neurosurgery, 8th ed.; Thieme: New York, NY, USA, 2016; p. 1318. [Google Scholar]
- Eddleman, C.; Getch, C.; Bendok, B.; Batjer, H. Saphenous vein grafts for the high-flow cerebral revascularization. In Cerebral Revascularization, 1st ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2011; pp. 125–126. [Google Scholar]
- Surdell, D.L.; Hage, Z.A.; Eddleman, C.S.; Gupta, D.K.; Bendok, B.R.; Batjer, H.H. Revascularization for complex intracranial aneurysms. Neurosurg. Focus 2008, 24, E21. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, J.; Sasaki-Adams, D.; Abdulrauf, S. Radial artery harvesting for cerebral revascularization: Technical pearls. In Cerebral Revascularization, 1st ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2011; pp. 119–120. [Google Scholar]
- Kawashima, M.; Rhoton, A., Jr. Surgical anatomy of EC-IC bypass procedures. In Cerebral Revascularization, 1st ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2011; p. 66. [Google Scholar]
- Stegemann, J.P.; Kaszuba, S.N.; Rowe, S.L. Review: Advances in vascular tissue engineering using protein-based biomaterials. Tissue Eng. 2007, 13, 2601–2613. [Google Scholar] [CrossRef] [PubMed]
- Sankaran, K.K.; Subramanian, A.; Krishnan, U.M.; Sethuraman, S. Nanoarchitecture of scaffolds and endothelial cells in engineering small diameter vascular grafts. Biotechnol. J. 2015, 10, 96–108. [Google Scholar] [CrossRef]
- Sayers, R.D.; Raptis, S.; Berce, M.; Miller, J.H. Long-term results of femorotibial bypass with vein or polytetrafluoroethylene. Br. J. Surg. 1998, 85, 934–938. [Google Scholar] [CrossRef]
- Kucinska-Lipka, J.; Gubanska, I.; Janik, H.; Sienkiewicz, M. Fabrication of polyurethane and polyurethane based composite fibres by the electrospinning technique for soft tissue engineering of cardiovascular system. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 46, 166–176. [Google Scholar] [CrossRef]
- Xue, L.; Greisler, H.P. Biomaterials in the development and future of vascular grafts. J. Vasc. Surg. 2003, 37, 472–480. [Google Scholar] [CrossRef]
- Abbott, W.M.; Vignati, J.J. Prosthetic grafts: When are they a reasonable alternative? Semin. Vasc. Surg. 1995, 8, 236–245. [Google Scholar]
- Li, D.; Xia, Y. Electrospinning of Nanofibers: Reinventing the Wheel? Adv. Mater. 2004, 16, 1151–1170. [Google Scholar] [CrossRef]
- Sill, T.J.; von Recum, H.A. Electrospinning: Applications in drug delivery and tissue engineering. Biomaterials 2008, 29, 1989–2006. [Google Scholar] [CrossRef] [PubMed]
- Uthamaraj, S.; Tefft, B.J.; Jana, S.; Hlinomaz, O.; Kalra, M.; Lerman, A.; Dragomir-Daescu, D.; Sandhu, G.S. Fabrication of Small Caliber Stent-grafts Using Electrospinning and Balloon Expandable Bare Metal Stents. J. Vis. Exp. 2016, 116, e54731. [Google Scholar] [CrossRef]
- Ercolani, E.; Del, G.C.; Bianco, A. Vascular tissue engineering of small-diameter blood vessels: Reviewing the electrospinning approach. J. Tissue Eng. Regen. Med. 2015, 9, 861–888. [Google Scholar] [CrossRef]
- Byrom, M.J.; Bannon, P.G.; White, G.H.; Ng, M.K. Animal models for the assessment of novel vascular conduits. J. Vasc. Surg. 2010, 52, 176–195. [Google Scholar] [CrossRef] [PubMed]
- Council, N.R. Guide for the Care and Use of Laboratory Animals, 8th ed.; The National Academic Press: Washington DC, USA, 2011. [Google Scholar]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. PLoS Biol. 2010, 8, e1000412. [Google Scholar] [CrossRef]
- Morton, D.; Hau, J. Welfare assesment and humane endpoints. In Handbook of Laboratory Animal Science, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2003; Volume 1, pp. 468–472. [Google Scholar]
- Grasl, C.; Bergmeister, H.; Stoiber, M.; Schima, H.; Weigel, G. Electrospun polyurethane vascular grafts: In vitro mechanical behavior and endothelial adhesion molecule expression. J. Biomed. Mater. Res. A 2010, 93, 716–723. [Google Scholar] [CrossRef]
- He, W.; Hu, Z.; Xu, A.; Liu, R.; Yin, H.; Wang, J.; Wang, S. The preparation and performance of a new polyurethane vascular prosthesis. Cell Biochem. Biophys. 2013, 66, 855–866. [Google Scholar] [CrossRef]
- He, W.; Hu, Z.J.; Xu, A.W.; Yin, H.H.; Wang, J.S.; Ye, J.L.; Wang, S.M. Assessment of the mechanical properties and biocompatibility of a new electrospun polyurethane vascular prosthesis. Nan Fang Yi Ke Da Xue Xue Bao 2011, 31, 2006–2011. [Google Scholar]
- Wang, X.; Lin, P.; Yao, Q.; Chen, C. Development of small-diameter vascular grafts. World J. Surg. 2007, 31, 682–689. [Google Scholar] [CrossRef]
- Sell, S.A.; McClure, M.J.; Garg, K.; Wolfe, P.S.; Bowlin, G.L. Electrospinning of collagen/biopolymers for regenerative medicine and cardiovascular tissue engineering. Adv. Drug Deliv. Rev. 2009, 61, 1007–1019. [Google Scholar] [CrossRef] [PubMed]
- Konig, G.; McAllister, T.N.; Dusserre, N.; Garrido, S.A.; Iyican, C.; Marini, A.; Fiorillo, A.; Avila, H.; Wystrychowski, W.; Zagalski, K.; et al. Mechanical properties of completely autologous human tissue engineered blood vessels compared to human saphenous vein and mammary artery. Biomaterials 2009, 30, 1542–1550. [Google Scholar] [CrossRef] [PubMed]
- Donovan, D.L.; Schmidt, S.P.; Townshend, S.P.; Njus, G.O.; Sharp, W.V. Material and structural characterization of human saphenous vein. J. Vasc. Surg. 1990, 12, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Pillay, V.; Dott, C.; Choonara, Y.E.; Tyagi, C.; Tomar, L.; Kumar, P.; Toit, L.C.D.; Ndesendo, V.M.K. A Review of the Effect of Processing Variables on the Fabrication of Electrospun Nanofibers for Drug Delivery Applications. J. Nanomater. 2017, 2013, 789289. [Google Scholar] [CrossRef]
- Beachley, V.; Wen, X. Effect of electrospinning parameters on the nanofiber diameter and length. Mater. Sci. Eng. C Mater. Biol. Appl. 2009, 29, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Milleret, V.; Hefti, T.; Hall, H.; Vogel, V.; Eberli, D. Influence of the fiber diameter and surface roughness of electrospun vascular grafts on blood activation. Acta Biomater. 2012, 8, 4349–4356. [Google Scholar] [CrossRef] [PubMed]
- Beattie, D.; Davies, A. Graft maintenance and graft failure. In Emergency Vascular and Endovascular Surgical Practice, 2nd ed.; Barros, A., Chant, A., Eds.; Hodder Arnold: London, UK, 2017; pp. 197–199. [Google Scholar]
- Bergmeister, H.; Grasl, C.; Walter, I.; Plasenzotti, R.; Stoiber, M.; Schreiber, C.; Losert, U.; Weigel, G.; Schima, H. Electrospun small-diameter polyurethane vascular grafts: Ingrowth and differentiation of vascular-specific host cells. Artif. Organs 2012, 36, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Nieponice, A.; Soletti, L.; Guan, J.; Hong, Y.; Gharaibeh, B.; Maul, T.M.; Huard, J.; Wagner, W.R.; Vorp, D.A. In vivo assessment of a tissue-engineered vascular graft combining a biodegradable elastomeric scaffold and muscle-derived stem cells in a rat model. Tissue Eng. Part A 2010, 16, 1215–1223. [Google Scholar] [CrossRef]
- Waltham, M.; Harris, J. Intimal hyperplasia: The nemesis of cardiovascular intervention. ANZ J. Surg. 2004, 74, 719–720. [Google Scholar] [CrossRef]
- Zilla, P.; Bezuidenhout, D.; Human, P. Prosthetic vascular grafts: Wrong models, wrong questions and no healing. Biomaterials 2007, 28, 5009–5027. [Google Scholar] [CrossRef]
- Uttayarat, P.; Perets, A.; Li, M.; Pimton, P.; Stachelek, S.J.; Alferiev, I.; Composto, R.J.; Levy, R.J.; Lelkes, P.I. Micropatterning of three-dimensional electrospun polyurethane vascular grafts. Acta Biomater. 2010, 6, 4229–4237. [Google Scholar] [CrossRef]
- Bergmeister, H.; Schreiber, C.; Grasl, C.; Walter, I.; Plasenzotti, R.; Stoiber, M.; Bernhard, D.; Schima, H. Healing characteristics of electrospun polyurethane grafts with various porosities. Acta Biomater. 2013, 9, 6032–6040. [Google Scholar] [CrossRef] [PubMed]
- Rocco, K.A.; Maxfield, M.W.; Best, C.A.; Dean, E.W.; Breuer, C.K. In vivo applications of electrospun tissue-engineered vascular grafts: A review. Tissue Eng. Part B Rev. 2014, 20, 628–640. [Google Scholar] [CrossRef] [PubMed]
- Fukunishi, T.; Best, C.A.; Sugiura, T.; Shoji, T.; Yi, T.; Udelsman, B.; Ohst, D.; Ong, C.S.; Zhang, H.; Shinoka, T.; et al. Tissue-Engineered Small Diameter Arterial Vascular Grafts from Cell-Free Nanofiber PCL/Chitosan Scaffolds in a Sheep Model. PLoS ONE 2016, 11, e0158555. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Allen, R.A.; Wang, Y. Fast-degrading elastomer enables rapid remodeling of a cell-free synthetic graft into a neoartery. Nat. Med. 2012, 18, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Ma, Z.; Teo, W.E.; Dong, Y.X.; Robless, P.A.; Lim, T.C.; Ramakrishna, S. Tubular nanofiber scaffolds for tissue engineered small-diameter vascular grafts. J. Biomed. Mater. Res. A 2009, 90, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, F.; Narita, Y.; Yamawaki-Ogata, A.; Kanie, K.; Kato, R.; Satake, M.; Kaneko, H.; Oshima, H.; Usui, A.; Ueda, Y. Novel small-caliber vascular grafts with trimeric Peptide for acceleration of endothelialization. Ann. Thorac. Surg. 2012, 93, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Yi, T.; Shinoka, T.; Lee, Y.U.; Reneker, D.H.; Breuer, C.K.; Becker, M.L. Pilot Mouse Study of 1 mm Inner Diameter (ID) Vascular Graft Using Electrospun Poly(ester urea) Nanofibers. Adv. Healthc. Mater. 2016, 5, 2427–2436. [Google Scholar] [CrossRef]
- Qiu, X.; Lee, B.L.; Ning, X.; Murthy, N.; Dong, N.; Li, S. End-point immobilization of heparin on plasma-treated surface of electrospun polycarbonate-urethane vascular graft. Acta Biomater. 2017, 51, 138–147. [Google Scholar] [CrossRef]
- Janairo, R.R.; Zhu, Y.; Chen, T.; Li, S. Mucin covalently bonded to microfibers improves the patency of vascular grafts. Tissue Eng. Part A 2014, 20, 285–293. [Google Scholar] [CrossRef]
- Hashi, C.K.; Derugin, N.; Janairo, R.R.; Lee, R.; Schultz, D.; Lotz, J.; Li, S. Antithrombogenic modification of small-diameter microfibrous vascular grafts. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1621–1627. [Google Scholar] [CrossRef]
- Hashi, C.K.; Zhu, Y.; Yang, G.Y.; Young, W.L.; Hsiao, B.S.; Wang, K.; Chu, B.; Li, S. Antithrombogenic property of bone marrow mesenchymal stem cells in nanofibrous vascular grafts. Proc. Natl. Acad. Sci. USA 2007, 104, 11915–11920. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Li, X.; Yang, T.; Lu, T.; Du, P.; Jing, C.; Chen, Z.; Lin, F.; Zhao, G.; Zhao, L. Construction of spider silk protein small-caliber tissue engineering vascular grafts based on dynamic culture and its performance evaluation. J. Biomed. Mater. Res. A 2023, 111, 71–87. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, N.; Yoshida, T.; Oyama, K.; Naruse, D.; Tsutsui, M.; Kikuchi, Y.; Koga, D.; Kamiya, H. Polyvinyl alcohol coating prevents platelet adsorption and improves mechanical property of polycaprolactone-based small-caliber vascular graft. Front. Cardiovasc. Med. 2022, 9, 946899. [Google Scholar] [CrossRef] [PubMed]
- Ilanlou, S.; Khakbiz, M.; Amoabediny, G.; Mohammadi, J. Preclinical studies of acellular extracellular matrices as small-caliber vascular grafts. Tissue Cell 2019, 60, 25–32. [Google Scholar] [CrossRef]
- Abbott, W.M.; Callow, A.; Moore, W.; Rutherford, R.; Veith, F.; Weinberg, S. Evaluation and performance standards for arterial prostheses. J. Vasc. Surg. 1993, 17, 746–756. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention Group (N = 9) | Control Group (N = 9) | Significance of Difference (p-Value) | ||
|---|---|---|---|---|
| Proximal graft | ||||
| Diastole | ID | 1597 ± 365 | 1352 ± 150 | 0.083 |
| OD | 1956 ± 402 | 1683 ± 173 | 0.083 | |
| Systole | ID | 1754 ± 370 | 1474 ± 150 | 0.054 |
| OD | 2077 ± 399 | 1786 ± 182 | 0.066 | |
| Expansion (IDs-IDd) | 157 ± 75 | 123 ± 49 | 0.280 | |
| Vmax (mm/s) | 371 ± 505 | 250 ± 55 | 0.479 | |
| Mid graft | ||||
| Diastole | ID | 1378 ± 130 | / | / |
| OD | 1766 ± 149 | / | / | |
| Systole | ID | 1498 ± 150 | / | / |
| OD | 1826 ± 131 | / | / | |
| Expansion (IDs-IDd) | 121 ± 55 | / | / | |
| Vmax (mm/s) | 207 ± 110 | / | / | |
| Distal graft | ||||
| Diastole | ID | 1341 ± 201 | 1210 ± 227 | 0.231 |
| OD | 1716 ± 201 | 1523 ± 214 | 0.075 | |
| Systole | ID | 1445 ± 192 | 1324 ± 238 | 0.270 |
| OD | 1803 ± 188 | 1620 ± 211 | 0.079 | |
| Expansion (IDs-IDd) | 104 ± 64 | 114 ± 102 | 0.827 | |
| Vmax (mm/s) | 323 ± 469 | 264 ± 42 | 0.711 | |
| Prox-dist expansion | 52 ± 110 | 9 ± 75 | 0.353 | |
| Vmax decay (prox-dist, mms/s) | 49 ± 40 | −14 ± 39 | 0.010 | |
| Subject | Graft Length a (mm) | NIH Length (mm) | Graft Length/NIH Length (%) | NIH 1 b Anastomosis (µm) | NIH 2 b Anastomosis (µm) | NIH 3 b Anastomosis (µm) | NIH 4 b Anastomosis (µm) | NIH 5 c Mid Graft (µm) | NIH 6 c Mid Graft (µm) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 9.20 | 6.03 | 66% | 62 | 93 | 0 | 0 | 82 | 0 |
| 2 | 10.63 | 5.81 | 55% | 50 | 0 | 77 | 39 | 82 | 40 |
| 3 | 14.38 | 0.00 | 0% | 0 | 0 | 0 | 0 | 0 | 0 |
| 4 | 9.88 | 3.42 | 35% | 0 | 0 | 33 | 55 | 0 | 27 |
| 5 | 16.09 | 14.10 | 88% | 100 | 200 | 64 | 0 | 137 | 68 |
| 6 | 9.15 | 5.36 | 59% | 26 | 30 | 50 | 24 | 57 | 32 |
| 7 | 9.03 | 2.93 | 32% | 49 | 40 | 0 | 0 | 0 | 40 |
| 8 | 11.19 | 10.54 | 94% | 51 | 72 | 0 | 0 | 0 | 0 |
| Mean | 11.19 | 6.02 | 54% | 42 | 54 | 28 | 15 | 45 | 26 |
| Total | 35 d | Total | 35 d | ||||||
| SD | 2.48 | 4.16 | 29% | 31 | 64 | 30 | 21 | 49 | 23 |
| Total | 43 d | Total | 40 d |
| Subject | Graft Length (mm) | Endothelial Length (mm) | Endothelial Length/Graft Length (%) |
|---|---|---|---|
| 1 | 9.20 | 5 | 55% |
| 2 | 10.63 | 11 | 100% |
| 3 | 14.38 | 0 | 0% |
| 4 | 9.88 | 10 | 100% |
| 5 | 16.09 | 17 | 90% |
| 6 | 9.15 | 9 | 100% |
| 7 | 9.03 | 9 | 100% |
| 8 | 11.19 | 11 | 94% |
| Mean | 11.19 | 8.95 | 80% |
| SD | 2.48 | 4.64 | 40% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vergauwen, E.; Tubeeckx, M.R.L.; Houben, A.; Van Vlierberghe, S.; Demolder, M.; De Meyer, G.R.Y.; Pauwels, P.; Menovsky, T. Electrospun Polyurethane Vascular Grafts for Cerebral Revascularization: A Pilot Study on Rats. BioChem 2024, 4, 1-17. https://doi.org/10.3390/biochem4010001
Vergauwen E, Tubeeckx MRL, Houben A, Van Vlierberghe S, Demolder M, De Meyer GRY, Pauwels P, Menovsky T. Electrospun Polyurethane Vascular Grafts for Cerebral Revascularization: A Pilot Study on Rats. BioChem. 2024; 4(1):1-17. https://doi.org/10.3390/biochem4010001
Chicago/Turabian StyleVergauwen, Evelynn, Michiel R. L. Tubeeckx, Annemie Houben, Sandra Van Vlierberghe, Marc Demolder, Guido R. Y. De Meyer, Patrick Pauwels, and Tomas Menovsky. 2024. "Electrospun Polyurethane Vascular Grafts for Cerebral Revascularization: A Pilot Study on Rats" BioChem 4, no. 1: 1-17. https://doi.org/10.3390/biochem4010001