
Treatment Strategies for Incisors of Children Affected by Molar Incisor Hypomineralization: A Narrative Review


Abstract
:1. Introduction
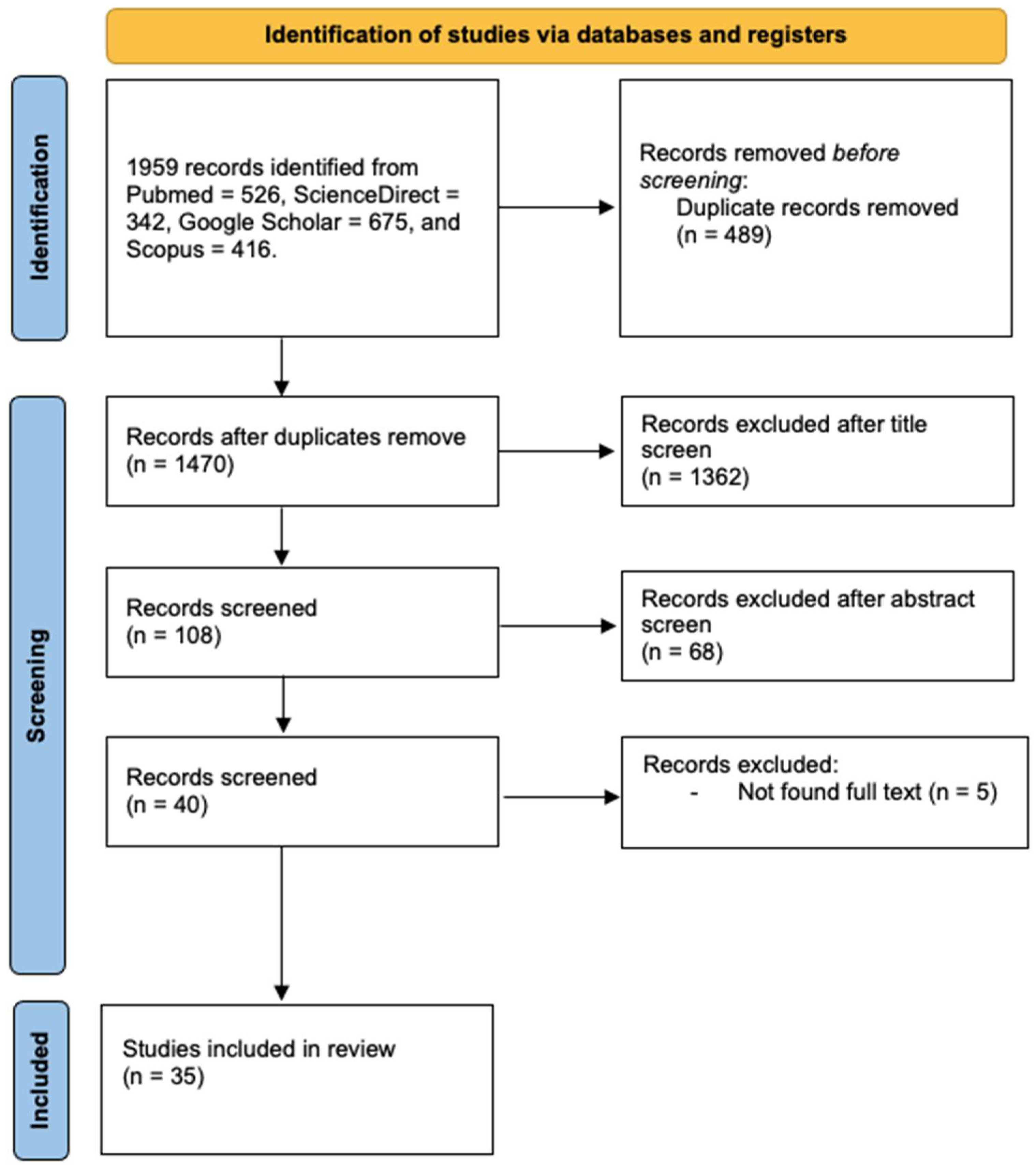
2. Search Strategy
3. Treatment Strategies for Incisors Affected by Molar Incisor Hypomineralization
3.1. Restorative and Aesthetic Approaches
3.2. Approaches to Increasing Mineral Content
3.3. Approaches to Relieving Hypersensitivity

{kind=link}
| Study Number | Authors | Publication Year | Study Type | Sample Size | Technique/Intervention | Outcome |
|---|---|---|---|---|---|---|
| 1 [49] | Attal et al. | 2014 | Case series | 5 patients/10 incisors | Resin infiltration | It is aesthetically promising, but caution is warranted due to the lack of long-term follow-up. |
| 2 [50] | Mazur et al. | 2018 | Retrospective study | 76 incisors | Resin infiltration | Enhances enamel aesthetics; visual and objective correlation observed. |
| 3 [51] | Brescia et al. | 2022 | Retrospective study | 33 patients/114 incisors (including fluorosis and trauma) | Resin infiltration | It is an effective treatment for mild MIH. |
| 4 [52] | Bhandari et al. | 2018 | Clinical trial | 22 incisors | Resin infiltration | Swift aesthetics for Grade I MIH; alternative before invasive procedures. |
| 5 [53] | Farias et al. | 2022 | Case report | 1 patient/1 incisor | Resin infiltration | Masks superficial white demarcated opacities; conservative, aesthetically effective treatment. |
| 6 [54] | Mabrouk et al. | 2020 | Case report | 1 patient/4 incisors | Resin infiltration | Minimally invasive technique eradicates white opacities effectively. |
| 7 [55] | Kim et al. | 2011 | Clinical trial | 12 patients/20 incisors | Resin infiltration | While the masking effect was effective in some, it was inadequate in others. |
| 8 [56] | Marouane and Chtioui | 2020 | Case report | 1 patient/2 incisors | Resin infiltration | Transillumination aids enamel infiltration treatment by assessing, confirming, and monitoring lesions. |
| 9 [57] | Giannetti et al. | 2018 | Case report | 1 patient/2 incisors | Resin infiltration | Deep infiltration can be performed to reach the limit of the lesion. |
| 10 [58] | Giannetti et al. | 2018 | Clinical trial | 17 patients/38 incisors | Resin infiltration | Superficial infiltration did not produce effective treatment in all cases. |
| 11 [38] | Warner et al. | 2022 | Clinical trial | 23 patients/29 incisors | Resin infiltration/microabrasion | Minimally invasive treatment is effective in reducing incisor opacities in children. |
| 12 [59] | Nogueira et al. | 2021 | Clinical trial | 51 patients/100 incisors | Resin infiltration with or without fluoride varnish and acid etching | Positively affected the structural integrity of the affected teeth by reducing the risk of enamel breakdown. |
| 13 [60] | Altan and Yilmaz | 2023 | Clinical trial | 37 patients/58 incisors | Resin infiltration | Micro-invasively effective treatment. |
| 14 [61] | Marouane and Manton | 2021 | Clinical trial | 17 patients/32 incisors | Resin infiltration | MIH lesion type and ethanol test predict time for infiltrating anterior teeth. |
| 15 [62] | Hasmun et al. | 2020 | Longitudinal interventional study | 103 patients | Resin infiltration/microabrasion/dental bleaching/composite resin restoration | Minimally invasive treatments can provide good clinical and psychosocial outcomes in children. |
| 16 [63] | ElBaz and Mahfouz | 2017 | Clinical trial | 20 patients/40 incisors | Resin infiltration/fluoride varnish | Resin infiltration is more successful at masking white opacities than fluoride varnish. |
| 17 [64] | Baroni et al. | 2019 | Case report | 1 patient/2 incisors | CPP-ACP/fluoride toothpaste/dental bleaching/composite resin restoration | Calcium phosphate may improve etching and bonding; bleaching reduces incisor defects pre-restoration. |
| 18 [65] | Mastroberardino et al. | 2012 | Case report | 1 patient/4 incisors | CPP-ACP/dental bleaching | The combined use of CPP-ACP and hydrogen peroxide is successful in treating white opacities without the need for invasive treatment. |
| 19 [66] | Vieira et al. | 2023 | Case report | 1 patient/2 incisors | Dental bleaching/microabrasion/composite resin restoration | The initial use of minimally invasive techniques contributes to the final treatment being as conservative as possible. |
| 20 [67] | Pessôa et al. | 2018 | Case report | 1 patient/4 incisors | Microabrasion/composite veneers | Adequate aesthetics were achieved after the conservative approach. |
| 21 [69] | Prud’homme et al. | 2017 | Case series | 3 patients/9 incisors | Microabrasion/resin infiltration/etch–bleach–seal technique | A non-invasive approach to the treatment of anterior yellow-brown opacities, but definitive aesthetic success may not be achieved. |
| 22 [70] | Bhandari et al. | 2019 | Clinical trial | 43 incisors | Microabrasion/CPP-ACP | Microabrasion and remineralizing agent enhance aesthetics of white opacities over time. |
| 23 [71] | Costa et al. | 2021 | Case report | 1 patient/4 incisors | Microabrasion/dental bleaching | A minimally invasive combination—microabrasion and low-concentration gel with light—enhanced aesthetics. |
| 24 [72] | Hasmun et al. | 2018 | Retrospective study | 93 children | Microabrasion with or without composite resin restoration | Minimally invasive dental treatment to reduce the visibility of enamel opacities in MIH can have a positive impact on children’s wellbeing. |
| 25 [75] | Sezer and Kargül | 2022 | Clinical trial | 53 patients/401 incisors | CaGP/CPP-ACFP/fluoride toothpaste | The use of two mineral-containing agents also improved lesions in hypomineralized anterior teeth with demarcated opacities. |
| 26 [76] | Sezer et al. | 2022 | Clinical trial | 22 patients/167 incisors | CaGP/CPP-ACFP | CPP-ACFP and CaGP had a positive effect on decreasing hypomineralization in MIH-affected enamel for a three-month period. |
| 27 [77] | Restrepo et al. | 2016 | Clinical trial | 51 patients/51 incisors | Fluoride varnish/home care | Fluoride varnish application was not effective in remineralization of the lesions. |
| 28 [78] | Singh et al. | 2021 | Clinical trial | 30 patients | CPP-ACP/fluoride varnish | Both agents are equally effective in providing remineralization. |
| 29 [79] | Singh et al. | 2021 | Clinical trial | 10 incisors | Self-assembling peptide | The agent may be an alternative, viable, preventive treatment option for remineralization of hypomineralized lesions. |
| 30 [80] | Biondi et al. | 2017 | Clinical trial | 55 patients/92 incisors | Fluoride varnish with or without tricalcium phosphate or CPP-ACP | Success in the treatment of lesions increases by adding remineralization agents to fluoride varnish. |
| 31 [81] | Solinas et al. | 2021 | Case report | 1 patient/4 incisors | Hydroxyapatite-based paste | The agent improves aesthetics and also eliminates hypersensitivity. |
| 32 [86] | Muniz et al. | 2020 | Clinical trial | 66 patients/99 incisors | Laser/fluoride varnish | Low-level laser therapy desensitizes teeth with MIH, and its combination with fluoride increases its effectiveness. |
| 33 [87] | Ozgül et al. | 2013 | Clinical trial | 33 patients/92 incisors | Ozone/fluoride varnish/CPP-ACP/CPP-ACFP | CPP-ACP paste was found to be more effective, and ozone therapy prolonged the effect of CPP-ACP paste. |
| 34 [88] | da Silva et al. | 2022 | Case report | 1 patient/5 incisors | Low-level laser therapy | Low-level laser therapy is indicated for the treatment of hypersensitivity and improving oral-health-related quality of life. |
| 35 [89] | Paschoal et al. | 2021 | Case report | 1 patient/3 incisors | Diode laser/fluoride varnish | Diode laser and fluoride varnish reduce hypersensitivity and increase oral-health-related quality of life. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weerheijm, K.L.; Jalevik, B.; Alaluusua, S. Molar-incisor hypomineralisation. Caries Res. 2001, 35, 390–391. [Google Scholar] [CrossRef]
- Babajko, S.; Jedeon, K.; Houari, S.; Loiodice, S.; Berdal, A. Disruption of Steroid Axis, a New Paradigm for Molar Incisor Hypomineralization (MIH). Front. Physiol. 2017, 8, 343. [Google Scholar] [CrossRef]
- Sezer, B.; Çarıkçıoğlu, B.; Kargül, B. Dental age and tooth development in children with molar-incisor hypomineralization: A case-control study. Arch. Oral Biol. 2022, 134, 105325. [Google Scholar] [CrossRef] [PubMed]
- Şen Yavuz, B.; Sezer, B.; Kaya, R.; Tuğcu, N.; Kargül, B. Is there an association between molar incisor hypomineralization and developmental dental anomalies? A case-control study. BMC Oral Health 2023, 23, 776. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Elhennawy, K.; Reda, S.; Bekes, K.; Manton, D.J.; Krois, J. Global burden of molar incisor hypomineralization. J. Dent. 2018, 68, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Dong, B.; Yu, D.; Ren, Q.; Sun, Y. The prevalence of molar incisor hypomineralization: Evidence from 70 studies. Int. J. Paediatr. Dent. 2018, 28, 170–179. [Google Scholar] [CrossRef]
- Lopes, L.B.; Machado, V.; Mascarenhas, P.; Mendes, J.J.; Botelho, J. The prevalence of molar-incisor hypomineralization: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 22405. [Google Scholar] [CrossRef] [PubMed]
- Sezer, B. Does the scientific literature provide sufficient information on incisors affected by molar incisor hypomineralisation? Eur. Arch. Paediatr. Dent. 2023, 24, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Juárez-López, M.L.A.; Salazar-Treto, L.V.; Hernández-Monjaraz, B.; Molina-Frechero, N. Etiological Factors of Molar Incisor Hypomineralization: A Systematic Review and Meta-Analysis. Dent. J. 2023, 11, 111. [Google Scholar] [CrossRef] [PubMed]
- Alhowaish, L.; Baidas, L.; Aldhubaiban, M.; Bello, L.L.; Al-Hammad, N. Etiology of Molar-Incisor Hypomineralization (MIH): A Cross-Sectional Study of Saudi Children. Children 2021, 8, 466. [Google Scholar] [CrossRef]
- Ilczuk-Rypuła, D.; Zalewska, M.; Pietraszewska, D.; Dybek, A.; Nitecka-Buchta, A.; Postek-Stefańska, L. Prevalence and Possible Etiological Factors of Molar-Incisor Hypomineralization (MIH) in Population of Silesian Children in Poland: A Pilot Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 8697. [Google Scholar] [CrossRef]
- Alzahrani, A.Y.; Alamoudi, N.M.H.; El Meligy, O.A.E.S. Contemporary Understanding of the Etiology and Management of Molar Incisor Hypomineralization: A Literature Review. Dent. J. 2023, 11, 157. [Google Scholar] [CrossRef] [PubMed]
- Hoberg, C.; Klein, C.; Klein, D.; Meller, C. Perinatal hypoxia and the risk of severe Molar-Incisor Hypomineralisation (MIH): A retrospective analysis of the pH value of umbilical arterial blood after birth. Eur. Arch. Paediatr. Dent. 2022, 23, 109–115. [Google Scholar] [CrossRef]
- Garot, E.; Rouas, P.; Somani, C.; Taylor, G.D.; Wong, F.; Lygidakis, N.A. An update of the aetiological factors involved in molar incisor hypomineralisation (MIH): A systematic review and meta-analysis. Eur. Arch. Paediatr. Dent. 2022, 23, 23–38. [Google Scholar] [CrossRef]
- Wuollet, E.; Laisi, S.; Salmela, E.; Ess, A.; Alaluusua, S. Molar-incisor hypomineralization and the association with childhood illnesses and antibiotics in a group of Finnish children. Acta Odontol. Scand. 2016, 74, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Głódkowska, N.; Emerich, K. The impact of environmental air pollution on the prevalence of molar incisor hypomineralization in schoolchildren: A cross-sectional study. Adv. Clin. Exp. Med. 2020, 29, 1469–1477. [Google Scholar] [CrossRef] [PubMed]
- Elzein, R.; Chouery, E.; Abdel-Sater, F.; Bacho, R.; Ayoub, F. Relation between molar-incisor hypomineralization (MIH) occurrence and war pollutants in bombarded regions: Epidemiological pilot study in Lebanon. Niger. J. Clin. Pract. 2021, 24, 1808–1813. [Google Scholar] [CrossRef]
- Jedeon, K.; De la Dure-Molla, M.; Brookes, S.J.; Loiodice, S.; Marciano, C.; Kirkham, J.; Canivenc-Lavier, M.-C.; Boudalia, S.; Bergès, R.; Harada, H.; et al. Enamel defects reflect perinatal exposure to bisphenol A. Am. J. Pathol. 2013, 183, 108–118. [Google Scholar] [CrossRef]
- Elzein, R.; Abdel-Sater, F.; Mehawej, C.; Jalkh, N.; Ayoub, F.; Chouery, E. Identification by whole-exome sequencing of new single-nucleotide polymorphisms associated with molar-incisor hypomineralisation among the Lebanese population. Eur. Arch. Paediatr. Dent. 2022, 23, 919–928. [Google Scholar] [CrossRef]
- Teixeira, R.J.P.B.; Andrade, N.S.; Queiroz, L.C.C.; Mendes, F.M.; Moura, M.S.; Moura, L.F.A.D.; Lima, M.D.M. Exploring the association between genetic and environmental factors and molar incisor hypomineralization: Evidence from a twin study. Int. J. Paediatr. Dent. 2018, 28, 198–206. [Google Scholar] [CrossRef]
- Hočevar, L.; Kovač, J.; Podkrajšek, K.T.; Battelino, S.; Pavlič, A. The possible influence of genetic aetiological factors on molar-incisor hypomineralisation. Arch. Oral Biol. 2020, 118, 104848. [Google Scholar] [CrossRef]
- Bussaneli, D.G.; Restrepo, M.; Fragelli, C.M.B.; Santos-Pinto, L.; Jeremias, F.; Cordeiro, R.C.L.; Bezamat, M.; Vieira, A.R.; Scarel-Caminaga, R.M. Genes Regulating Immune Response and Amelogenesis Interact in Increasing the Susceptibility to Molar-Incisor Hypomineralization. Caries Res. 2019, 53, 217–227. [Google Scholar] [CrossRef]
- Pang, L.; Li, X.; Wang, K.; Tao, Y.; Cui, T.; Xu, Q.; Lin, H. Interactions with the aquaporin 5 gene increase the susceptibility to molar-incisor hypomineralization. Arch. Oral Biol. 2020, 111, 104637. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.R. On the genetics contribution to molar incisor hypomineralization. Int. J. Paediatr. Dent. 2019, 29, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Sezer, B.; Tuğcu, N.; Çalışkan, C.; Durmuş, B.; Kargül, B. İstanbul’da yaşayan bir grup çocuğun büyük azı-kesici hipomineralizasyonu gözlenen dişlerinde lezyon dağılım ve karakteristiklerinin değerlendirilmesi. 7tepe Klin. 2023, 19, 10–16. [Google Scholar]
- Rodd, H.D.; Graham, A.; Tajmehr, N.; Timms, L.; Hasmun, N. Molar Incisor Hypomineralisation: Current Knowledge and Practice. Int. Dent. J. 2021, 71, 285–291. [Google Scholar] [CrossRef]
- Bastos-Bitencourt, N.A.; Mosquim, V.; Zabeu, G.S.; Rios, D.; Ishikiriama, S.K.; Wang, L. MIH-Affected Teeth: Clinical Challenges from Diagnosis to Restorative Management. Int. J. Periodontics Restor. Dent. 2022, 42, 225–231. [Google Scholar] [CrossRef]
- Lygidakis, N.A.; Wong, F.; Jälevik, B.; Vierrou, A.M.; Alaluusua, S.; Espelid, I. Best Clinical Practice Guidance for clinicians dealing with children presenting with Molar-Incisor-Hypomineralisation (MIH): An EAPD Policy Document. Eur. Arch. Paediatr. Dent. 2010, 11, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Ghanim, A.; Elfrink, M.; Weerheijm, K.; Mariño, R.; Manton, D. A practical method for use in epidemiological studies on enamel hypomineralisation. Eur. Arch. Paediatr. Dent. 2015, 16, 235–246. [Google Scholar] [CrossRef]
- Durmus, B.; Sezer, B.; Tugcu, N.; Caliskan, C.; Bekiroglu, N.; Kargul, B. Two-Year Survival of High-Viscosity Glass Ionomer in Children with Molar Incisor Hypomineralization. Med. Princ. Pract. 2021, 30, 73–79. [Google Scholar] [CrossRef]
- Somani, C.; Taylor, G.D.; Garot, E.; Rouas, P.; Lygidakis, N.A.; Wong, F.S.L. An update of treatment modalities in children and adolescents with teeth affected by molar incisor hypomineralisation (MIH): A systematic review. Eur. Arch. Paediatr. Dent. 2022, 23, 39–64. [Google Scholar] [CrossRef]
- Lygidakis, N.A.; Garot, E.; Somani, C.; Taylor, G.D.; Rouas, P.; Wong, F.S.L. Best clinical practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH): An updated European Academy of Paediatric Dentistry policy document. Eur. Arch. Paediatr. Dent. 2022, 23, 3–21. [Google Scholar] [CrossRef]
- Weber, K.R.; Wierichs, R.J.; Meyer-Lueckel, H.; Flury, S. Restoration of teeth affected by molar-incisor hypomineralisation: A systematic review. Swiss Dent. J. 2021, 131, 988–997. [Google Scholar]
- Davidovich, E.; Dagon, S.; Tamari, I.; Etinger, M.; Mijiritsky, E. An Innovative Treatment Approach Using Digital Workflow and CAD-CAM Part 2: The Restoration of Molar Incisor Hypomineralization in Children. Int. J. Environ. Res. Public Health 2020, 17, 1499. [Google Scholar] [CrossRef]
- Moulis, E.; Barthélemi, S.; Delsol, L. Orthodontic treatment of children with class II division 1 with severe MIH involving first permanent molars extractions: A case report. Int. Orthod. 2020, 18, 885–894. [Google Scholar] [CrossRef]
- Tugcu, N.; Sezer, B.; Caliskan, C.; Durmus, B.; Kargul, B. Changes in oral health-related quality of life after treatment of molar incisor hypomineralisation using Glass Hybrid Restorations. J. Pak. Med. Assoc. 2022, 72, 1977–1982. [Google Scholar]
- Dincer, E. Why do I have white spots on my front teeth? J. Mich. Dent. Assoc. 2009, 91, 40–43. [Google Scholar]
- Warner, C.; Hasmun, N.N.; Elcock, C.; Lawson, J.A.; Vettore, M.V.; Rodd, H.D. Making white spots disappear! Do minimally invasive treatments improve incisor opacities in children with molar-incisor hypomineralisation? Int. J. Paediatr. Dent. 2022, 32, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Puleio, F.; Fiorillo, L.; Gorassini, F.; Iandolo, A.; Meto, A.; D’Amico, C.; Cervino, G.; Pinizzotto, M.; Bruno, G.; Portelli, M.; et al. Systematic Review on White Spot Lesions Treatments. Eur. J. Dent. 2022, 16, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Richter, A.E.; Arruda, A.O.; Peters, M.C.; Sohn, W. Incidence of caries lesions among patients treated with comprehensive orthodontics. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Cazzolla, A.P.; De Franco, A.R.; Lacaita, M.; Lacarbonara, V. Efficacy of 4-year treatment of icon infiltration resin on postorthodontic white spot lesions. BMJ Case Rep. 2018, 2018, bcr2018225639. [Google Scholar] [CrossRef]
- Puleio, F.; Di Spirito, F.; Lo Giudice, G.; Pantaleo, G.; Rizzo, D.; Lo Giudice, R. Long-Term Chromatic Durability of White Spot Lesions through Employment of Infiltration Resin Treatment. Medicina 2023, 59, 749. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, R.; Lipari, F.; Puleio, F.; Alibrandi, A.; Lo Giudice, F.; Tamà, C.; Sazonova, E.; Lo Giudice, G. Spectrophotometric Evaluation of Enamel Color Variation Using Infiltration Resin Treatment of White Spot Lesions at One Year Follow-Up. Dent. J. 2020, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.N.; Fine, C.M.; Newton, M.N.; Kabani, F.; Muzzin, K.B.; Reed, K.M. Resin Infiltration Therapy: A micro-invasive treatment approach for white spot lesions. J. Dent. Hyg. 2021, 95, 31–35. [Google Scholar] [PubMed]
- Elhennawy, K.; Manton, D.J.; Crombie, F.; Zaslansky, P.; Radlanski, R.J.; Jost-Brinkmann, P.G.; Schwendicke, F. Structural, mechanical and chemical evaluation of molar-incisor hypomineralization- affected enamel: A systematic review. Arch. Oral Biol. 2017, 83, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Gambetta-Tessini, K.; Mariño, R.; Ghanim, A.; Adams, G.G.; Manton, D.J. Validation of quantitative light-induced fluorescence-digital in the quantification of demarcated hypomineralized lesions of enamel. J. Investig. Clin. Dent. 2017, 8, e12259. [Google Scholar] [CrossRef]
- Crombie, F.A.; Manton, D.J.; Palamara, J.E.; Zalizniak, I.; Cochrane, N.J.; Reynolds, E.C. Characterisation of developmentally hypomineralised human enamel. J. Dent. 2013, 41, 611–618. [Google Scholar] [CrossRef]
- Fagrell, T.G.; Salmon, P.; Melin, L.; Norén, J.G. Onset of molar incisor hypomineralization (MIH). Swed. Dent. J. 2013, 37, 61–70. [Google Scholar] [PubMed]
- Attal, J.P.; Atlan, A.; Denis, M.; Vennat, E.; Tirlet, G. White spots on enamel: Treatment protocol by superficial or deep infiltration (part 2). Int. Orthod. 2014, 12, 1–31. [Google Scholar] [CrossRef]
- Mazur, M.; Westland, S.; Guerra, F.; Corridore, D.; Vichi, M.; Maruotti, A.; Nardi, G.M.; Ottolenghi, L. Objective and subjective aesthetic performance of icon® treatment for enamel hypomineralization lesions in young adolescents: A retrospective single center study. J. Dent. 2018, 68, 104–108. [Google Scholar] [CrossRef]
- Brescia, A.V.; Montesani, L.; Fusaroli, D.; Docimo, R.; Di Gennaro, G. Management of Enamel Defects with Resin Infiltration Techniques: Two Years Follow Up Retrospective Study. Children 2022, 9, 1365. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, R.; Thakur, S.; Singhal, P.; Chauhan, D.; Jayam, C.; Jain, T. Concealment effect of resin infiltration on incisor of Grade I molar incisor hypomineralization patients: An in vivo study. J. Conserv. Dent. 2018, 21, 450–454. [Google Scholar] [CrossRef]
- Farias, J.O.; Cunha, M.C.A.; Martins, V.L.; Mathias, P. Microinvasive esthetic approach for deep enamel white spot lesion. Dent. Res. J. 2022, 19, 29. [Google Scholar]
- Mabrouk, R.; Yahia, S.; Oueslati, A.; Frih, N. Erosion infiltration in the management of molar-incisor hypomineralization (MIH) defects. Case Rep. Dent. 2020, 2020, 8888256. [Google Scholar] [CrossRef]
- Kim, S.; Kim, E.Y.; Jeong, T.S.; Kim, J.W. The evaluation of resin infiltration for masking labial enamel white spot lesions. Int. J. Paediatr. Dent. 2011, 21, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Marouane, O.; Chtioui, F. Transillumination-aided infiltration: A diagnostic concept for treating enamel opacities. J. Esthet. Restor. Dent. 2020, 32, 451–456. [Google Scholar] [CrossRef]
- Giannetti, L.; Murri Dello Diago, A.; Corciolani, E.; Spinas, E. Deep infiltration for the treatment of hypomineralized enamel lesions in a patient with molar incisor hypomineralization: A clinical case. J. Biol. Regul. Homeost. Agents 2018, 32, 751–754. [Google Scholar]
- Giannetti, L.; Murri Dello Diago, A.; Silingardi, G.; Spinas, E. Superficial infiltration to treat white hypomineralized defects of enamel: Clinical trial with 12-month follow-up. J. Biol. Regul. Homeost. Agents 2018, 32, 1335–1338. [Google Scholar]
- Nogueira, V.K.C.; Soares, I.P.M.; Fragelli, C.M.B.; Boldieri, T.; Manton, D.J.; Bussaneli, D.G.; Cordeiro, R.d.C.L. Structural integrity of MIH-affected teeth after treatment with fluoride varnish or resin infiltration: An 18-Month randomized clinical trial. J. Dent. 2021, 105, 103570. [Google Scholar] [CrossRef]
- Altan, H.; Yilmaz, R.E. Clinical evaluation of resin infiltration treatment masking effect on hypomineralised enamel surfaces. BMC Oral Health 2023, 23, 444. [Google Scholar] [CrossRef]
- Marouane, O.; Manton, D.J. The influence of lesion characteristics on application time of an infiltrate applied to MIH lesions on anterior teeth: An exploratory in vivo pilot study. J. Dent. 2021, 115, 103814. [Google Scholar] [CrossRef]
- Hasmun, N.; Vettore, M.V.; Lawson, J.A.; Elcock, C.; Zaitoun, H.; Rodd, H.D. Determinants of children’s oral health-related quality of life following aesthetic treatment of enamel opacities. J. Dent. 2020, 98, 103372. [Google Scholar] [CrossRef]
- ElBaz, G.A.; Mahfouz, S.M. Efficacy of two different treatment modalities on masking white spot lesions in children with molar incisor hypo-mineralization. Egypt. Dent. J. 2017, 63, 2147–2154. [Google Scholar] [CrossRef]
- Baroni, C.; Mazzoni, A.; Breschi, L. Molar incisor hypomineralization: Supplementary, restorative, orthodontic, and esthetic long-term treatment. Quintessence Int. 2019, 50, 412–417. [Google Scholar] [PubMed]
- Mastroberardino, S.; Campus, G.; Strohmenger, L.; Villa, A.; Cagetti, M.G. An Innovative Approach to Treat Incisors Hypomineralization (MIH): A Combined Use of Casein Phosphopeptide-Amorphous Calcium Phosphate and Hydrogen Peroxide—A Case Report. Case Rep. Dent. 2012, 2012, 379593. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.; Emerenciano, N.G.; Moda, M.D.; Silva, Ú.; Fagundes, T.C.; Danelon, M.; Cunha, R.F. Treatment of Molar-incisor Hypomineralization: A Case Report of 11-year Clinical Follow-up. Oper. Dent. 2023, 48, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Pessôa, C.P.; Pion, L.; Reyes, A.; Matos, R.; Alencar, C.F.; Novaes, T.F.; Braga, M.M. Conservative approach for molar-incisor hypomineralization: A case report and 7-year follow-up. Gen. Dent. 2018, 66, e1–e4. [Google Scholar]
- Wright, J.T. The etch-bleach-seal technique for managing stained enamel defects in young permanent incisors. Pediatr. Dent. 2002, 24, 249–252. [Google Scholar]
- Prud’homme, T.; Hyon, I.; Dajean Trutaud, S.; Lopez Cazaux, S. Different applicabilities of the etch-bleach-seal technique for treating opacities on permanent incisor damage by molar incisor hypomineralisation in three young patients. BMJ Case Rep. 2017, 2017, bcr2017221442. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, R.; Thakur, S.; Singhal, P.; Chauhan, D.; Jayam, C.; Jain, T. In Vivo Comparative Evaluation of Esthetics after Microabrasion and Microabrasion followed by Casein Phosphopeptide-Amorphous Calcium Fluoride Phosphate on Molar Incisor Hypomineralization-Affected Incisors. Contemp. Clin. Dent. 2019, 10, 9–15. [Google Scholar] [CrossRef]
- Costa, J.L.S.G.; Nogueira, B.R.; de Oliveira Junior, O.B.; Pretel, H. Association of microabrasion and tooth whitening with LED/laser system in the treatment of incisor hypomineralization: 3-year follow-up. Photodiagnosis Photodyn. Ther. 2021, 33, 102197. [Google Scholar] [CrossRef] [PubMed]
- Hasmun, N.; Lawson, J.; Vettore, M.V.; Elcock, C.; Zaitoun, H.; Rodd, H. Change in Oral Health-Related Quality of Life Following Minimally Invasive Aesthetic Treatment for Children with Molar Incisor Hypomineralisation: A Prospective Study. Dent. J. 2018, 6, 61. [Google Scholar] [CrossRef] [PubMed]
- Sezer, B.; Kargül, B. Current Remineralizing Agents in Caries Management. Turk. Klin. J. Dent. Sci. 2020, 26, 472–486. [Google Scholar] [CrossRef]
- Sezer, B.; Kargül, B. Remineralization Effectiveness of Toothpastes and Mousses in Molar-Incisor Hypomineralization. In Diş Macun ve Kremleri, 1st ed.; Arslantunalı Tağtekin, D., Ed.; Türkiye Klinikleri: Ankara, Turkey, 2020; pp. 136–142. [Google Scholar]
- Sezer, B.; Kargul, B. Effect of Remineralization Agents on Molar-Incisor Hypomineralization-Affected Incisors: A Randomized Controlled Clinical Trial. J. Clin. Pediatr. Dent. 2022, 46, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Sezer, B.; Tuğcu, N.; Calışkan, C.; Durmuş, B.; Kupets, T.; Bekiroğlu, N.; Kargül, B.; Bourgeois, D. Effect of casein phosphopeptide amorphous calcium fluoride phosphate and calcium glycerophosphate on incisors with molar-incisor hypomineralization: A cross-over, randomized clinical trial. Biomed. Mater. Eng. 2022, 33, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, M.; Jeremias, F.; Santos-Pinto, L.; Cordeiro, R.C.; Zuanon, A.C. Effect of Fluoride Varnish on Enamel Remineralization in Anterior Teeth with Molar Incisor Hypomineralization. J. Clin. Pediatr. Dent. 2016, 40, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; Goyal, A.; Gauba, K.; Rathore, M. A Comparative Evaluation of CPP-ACP Cream and Fluoride Varnish in Remineralization of MIH-affected Teeth Using Laser Fluorescence. Pediatr. Dent. 2021, 4, 117–121. [Google Scholar]
- Singh, S.K.; Rathore, M.; Goyal, A. Assesment of Remineralization of Hypomineralized Enamel Lesions Using Self-Assembling Peptide Using Laser Fluorescence- A Pilot Study. Saudi J. Oral Dent. Res. 2021, 6, 498–501. [Google Scholar]
- Biondi, A.M.; Cortese, S.G.; Babino, L.; Fridman, D.E. Comparison of Mineral Density in Molar Incisor Hypomineralization applying fluoride varnishes and casein phosphopeptide-amorphous calcium phosphate. Acta Odontol. Latinoam. 2017, 30, 118–123. [Google Scholar]
- Solinas, G.; Grabesu, V.; Lattari, M.; Strinna, R.; Arnould, N.; Amodeo, A.A. Management of a Hypomineralisation of the Enamel by Applying a Remineraliser Based on Zinc Hydroxyapatite (microRepair). Case Rep. Dent. 2021, 2021, 5291858. [Google Scholar] [CrossRef]
- Linner, T.; Khazaei, Y.; Bücher, K.; Pfisterer, J.; Hickel, R.; Kühnisch, J. Hypersensitivity in teeth affected by molar-incisor hypomineralization (MIH). Sci. Rep. 2021, 11, 17922. [Google Scholar] [CrossRef] [PubMed]
- Raposo, F.; de Carvalho Rodrigues, A.C.; Lia, É.N.; Leal, S.C. Prevalence of Hypersensitivity in Teeth Affected by Molar-Incisor Hypomineralization (MIH). Caries Res. 2019, 53, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Sobral, A.P.T.; Santos, E.M.; Aranha, A.C.; Soares, P.V.; Moriyama, C.M.; Gonçalves, M.L.L.; Ribeiro, R.A.; Motta, L.J.; Horliana, A.C.R.T.; Fernandes, K.P.S.; et al. The control of pain due to dentin hypersensitivity in individuals with molar-incisor hypomineralisation: A protocol for a randomised controlled clinical trial. BMJ Open 2021, 11, e044653. [Google Scholar] [CrossRef]
- Oyedele, T.A.; Folayan, M.O.; Adekoya-Sofowora, C.A.; Oziegbe, E.O. Co-morbidities associated with molar-incisor hypomineralisation in 8- to 16-year-old pupils in Ile-Ife, Nigeria. BMC Oral Health 2015, 15, 37. [Google Scholar] [CrossRef] [PubMed]
- Muniz, R.S.C.; Carvalho, C.N.; Aranha, A.C.C.; Dias, F.M.C.S.; Ferreira, M.C. Efficacy of low-level laser therapy associated with fluoride therapy for the desensitisation of molar-incisor hypomineralisation: Randomised clinical trial. Int. J. Paediatr. Dent. 2020, 30, 323–333. [Google Scholar] [CrossRef]
- Ozgül, B.M.; Saat, S.; Sönmez, H.; Oz, F.T. Clinical evaluation of desensitizing treatment for incisor teeth affected by molar-incisor hypomineralization. J. Clin. Pediatr. Dent. 2013, 38, 101–105. [Google Scholar] [CrossRef] [PubMed]
- da Silva, F.G.; de Almeida, S.B.; de Campos, P.H.; Abrantes, R.M.; de Oliveira, A.V.A.; Guaré, R.O.; Diniz, M.B. Low-Level Laser Therapy for Management of Hypersensitivity in Molar-Incisor Hypomineralization and Oral Health-Related Quality of Life: Case Report. J. Clin. Pediatr. Dent. 2022, 46, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Paschoal, M.A.B.; Costa, H.E.; Santos-Pinto, L.; Ferreira, M.C. Photobiomodulation therapy for hypersensitivity associated with molar-incisor hypomineralization: A case report. Gen. Dent. 2021, 69, 50–53. [Google Scholar]
- Lygidakis, N.A. Treatment modalities in children with teeth affected by molar-incisor enamel hypomineralisation (MIH): A systematic review. Eur. Arch. Paediatr. Dent. 2010, 11, 65–74. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sezer, B.; Çarıkçıoğlu, B. Treatment Strategies for Incisors of Children Affected by Molar Incisor Hypomineralization: A Narrative Review. Oral 2024, 4, 74-89. https://doi.org/10.3390/oral4010007
Sezer B, Çarıkçıoğlu B. Treatment Strategies for Incisors of Children Affected by Molar Incisor Hypomineralization: A Narrative Review. Oral. 2024; 4(1):74-89. https://doi.org/10.3390/oral4010007
Chicago/Turabian StyleSezer, Berkant, and Burak Çarıkçıoğlu. 2024. "Treatment Strategies for Incisors of Children Affected by Molar Incisor Hypomineralization: A Narrative Review" Oral 4, no. 1: 74-89. https://doi.org/10.3390/oral4010007