

Photodynamic Therapy of Oral Cancer and Novel Liposomal Photosensitizers †
 , ,
, ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. 5-Aminolevulinic Acid
3. Methylene Blue
4. Porphyrin Photosensitizers
5. Foscan (Temoporfin; mTHPC)
6. Chlorin e6 and HPPH
7. Theranostics and Photodynamic Therapy
8. Targeting Cancer Cells
9. Novel Porphyrinoids with High In Vitro Cytotoxic Activity against Oral Cancer Cells
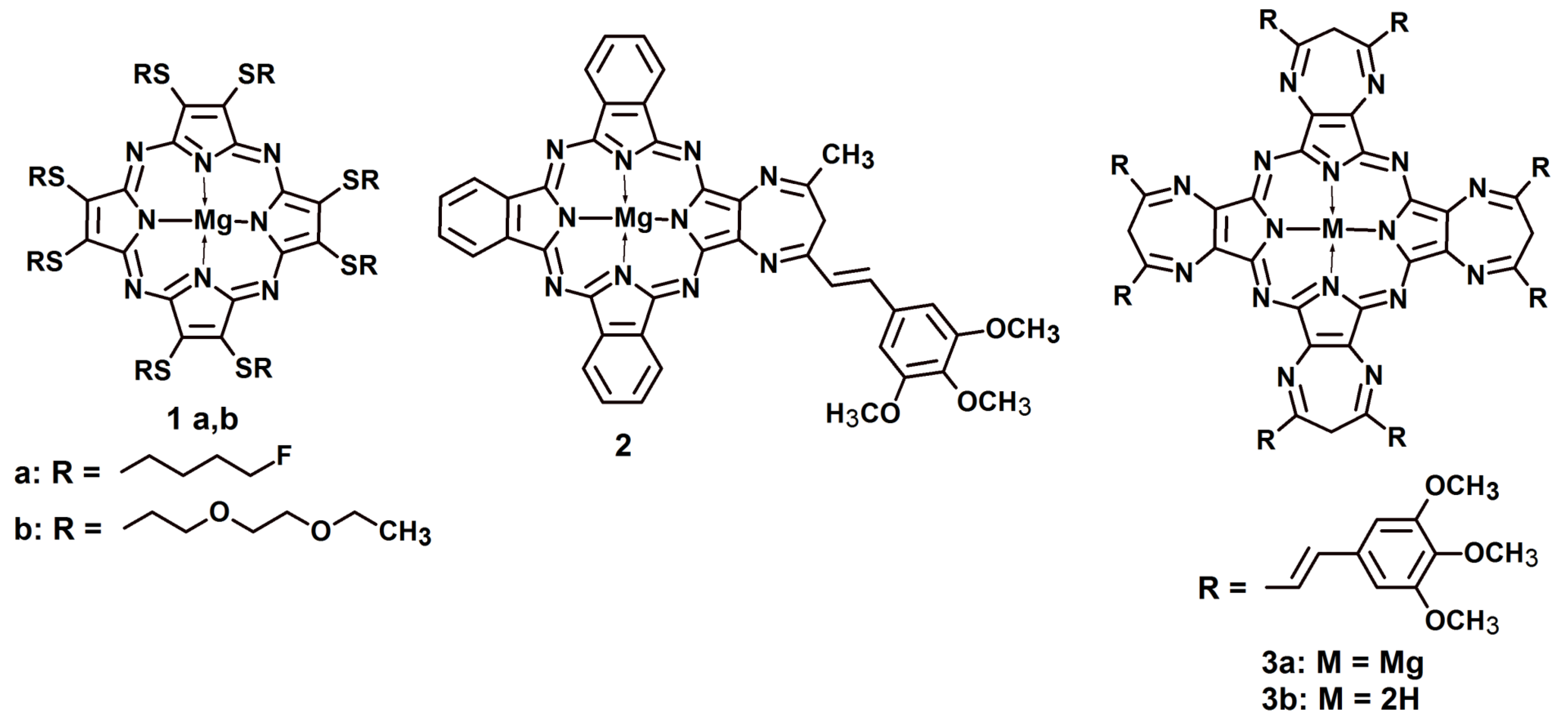
9.1. Sulfanyl Porphyrazines with Fluoroalkyl and Diether Chains
9.2. Porphyrazines and Tribenzoporphyrazine with Annulated Diazepine Rings
9.3. Potential Methods of Liposome Administration
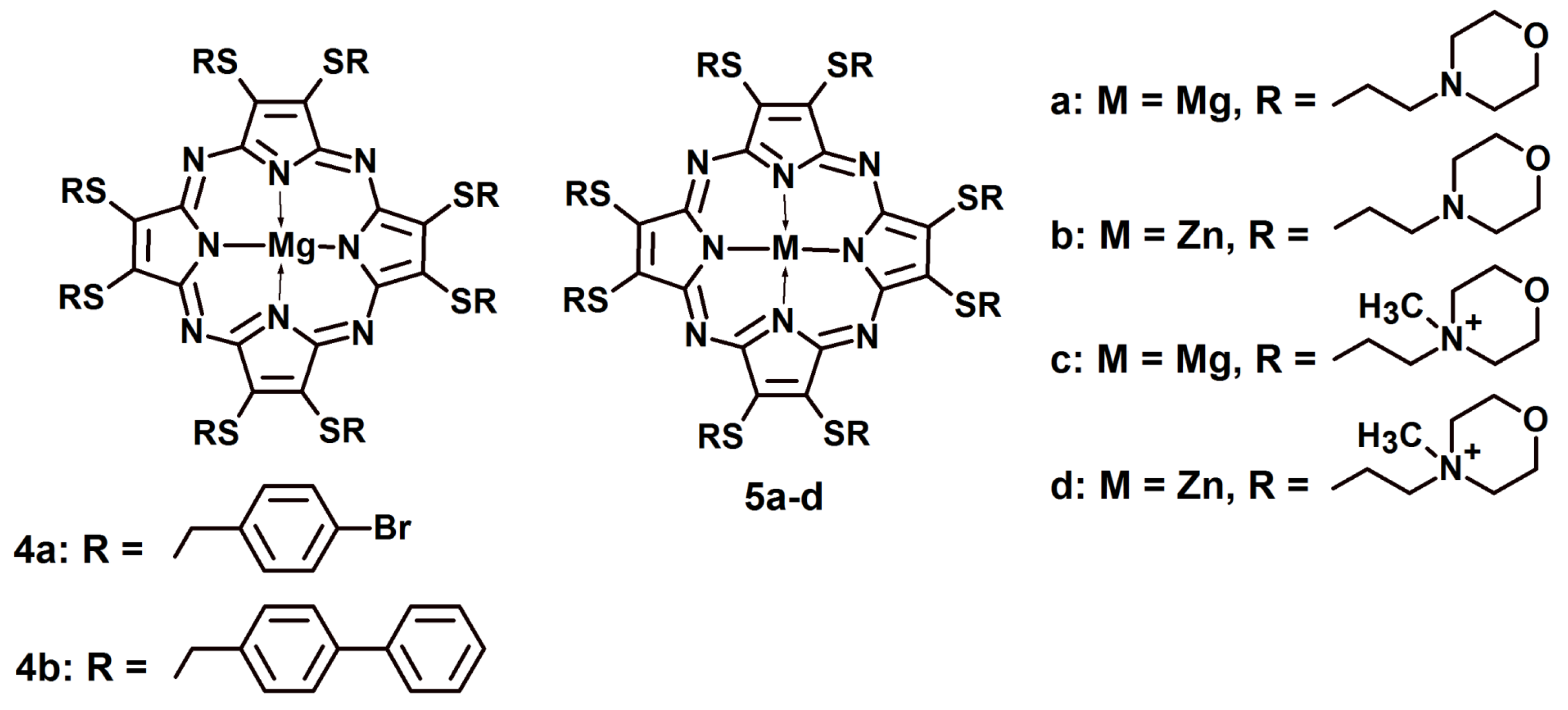
9.4. Sulfanyl Porphyrazines with 4-Bromobenzyl and 4-Biphenylylmethyl Substituents
9.5. Sulfanyl Porphyrazines with Morpholinoethyl and N-Methylmorpholinoethyl Substituents
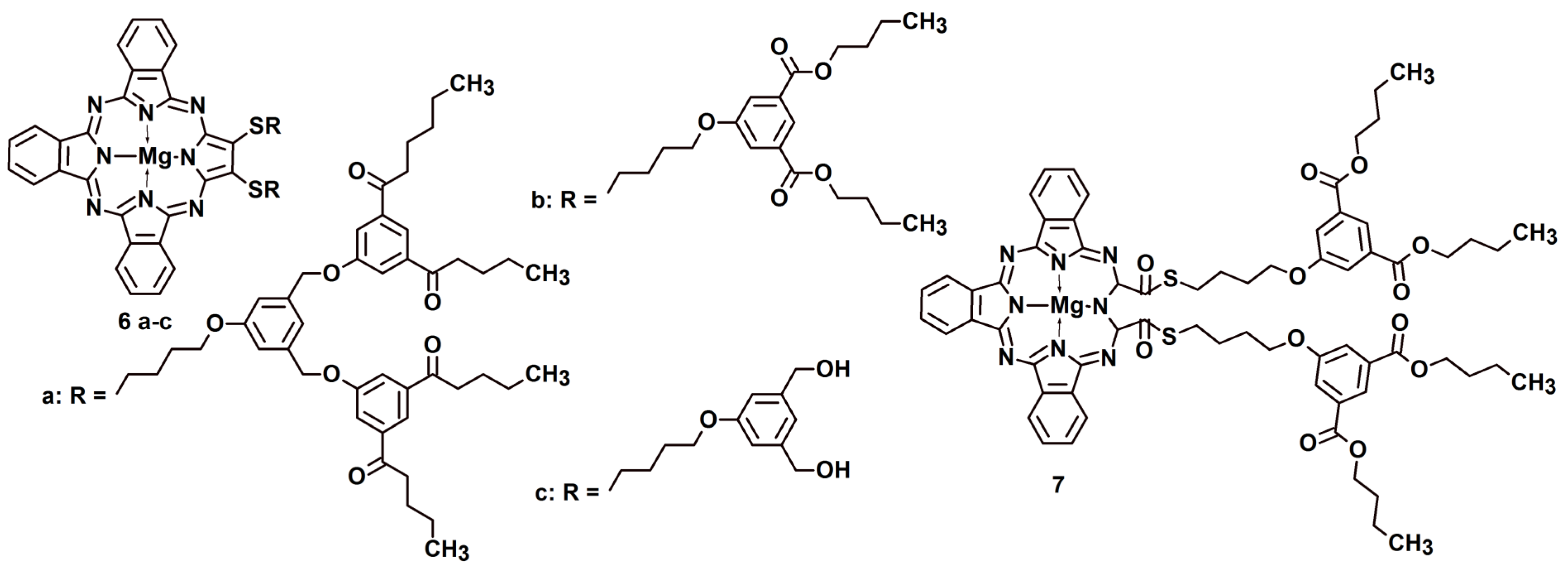
9.6. Sulfanyl Tribenzoporphyrazines with Dendrimeric Moieties
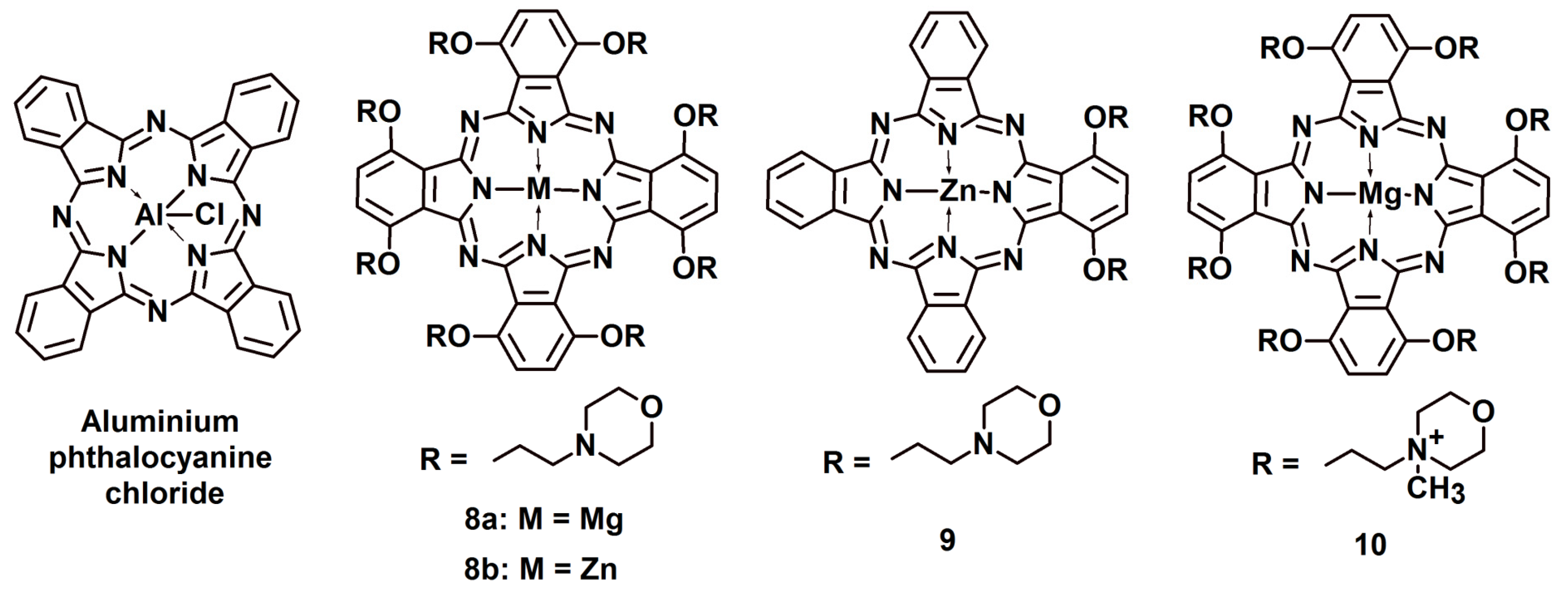
9.7. Phthalocyanines
9.8. Other Porphyrinoid Photosensitizers
10. Future Directions in the Photodynamic Therapy of Oral Cancer
10.1. Targeting Photosensitizers to Cancer Stem Cells
10.2. Upconversion Nanoparticles for Near-Infrared Irradiation of Tumors
10.3. Overcoming Tumor Hypoxia
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mouth and Oral Cancer Statistics. Available online: https://www.wcrf.org/cancer-trends/mouth-and-oral-cancer-statistics (accessed on 26 January 2023).
- Abrahamse, H.; Hamblin, M.R. New photosensitizers for photodynamic therapy. Biochem. J. 2016, 473, 347–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melissari, Z.; Sample, H.C.; Twamley, B.; Williams, R.M.; Senge, M.O. Synthesis and spectral properties of gem-dimethyl chlorin photosensitizers. Chemphotochem 2020, 4, 601–611. [Google Scholar] [CrossRef]
- Yao, Q.C.; Fan, J.L.; Long, S.R.; Zhao, X.Z.; Li, H.D.; Du, J.J.; Shao, K.; Peng, X.J. The concept and examples of type-III photosensitizers for cancer photodynamic therapy. Chem 2022, 8, 197–209. [Google Scholar] [CrossRef]
- Rak, J.; Kabesova, M.; Benes, J.; Pouckova, P.; Vetvicka, D. Advances in liposome-encapsulated phthalocyanines for photodynamic therapy. Life 2023, 13, 305. [Google Scholar] [CrossRef]
- Skupin-Mrugalska, P.; Sobotta, L.; Kucinska, M.; Murias, M.; Mielcarek, J.; Düzgüneş, N. Cellular changes, molecular pathways and the immune system following photodynamic treatment. Curr. Med. Chem. 2014, 21, 4059–4073. [Google Scholar] [CrossRef]
- Chen, H.M.; Liu, C.M.; Yang, H.; Chou, H.Y.; Chiang, C.P.; Kuo, M.Y. 5-aminolevulinic acid induce apoptosis via NF-kappaB/JNK pathway in human oral cancer Ca9-22 cells. J. Oral Pathol. Med. 2011, 40, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Ahn, M.Y.; Yoon, H.E.; Kwon, S.M.; Lee, J.; Min, S.K.; Kim, Y.C.; Ahn, S.G.; Yoon, J.H. Synthesized Pheophorbide a-mediated photodynamic therapy induced apoptosis and autophagy in human oral squamous carcinoma cells. J. Oral Pathol. Med. 2013, 42, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Alzeibak, R.; Mishchenko, T.A.; Shilyagina, N.Y. Targeting immunogenic cancer cell death by photodynamic therapy: Past, present and future. J. Immunother. Cancer 2021, 9, e001926. [Google Scholar] [CrossRef] [PubMed]
- Konopka, K.; Goslinski, T. Photodynamic therapy in dentistry. J. Dent. Res. 2007, 86, 694–707. [Google Scholar] [CrossRef]
- Wooten, R.S.; Ahlquist, D.A.; Anderson, R.E.; Carpenter, H.A.; Pemberton, J.H.; Cortese, D.A.; Ilstrup, D.M. Localization of hematoporphyrin. Derivative to human colorectal cancer. Cancer 1989, 64, 1569–1576. [Google Scholar] [CrossRef]
- Dougherty, T.J.; Gomer, C.J.; Henderson, B.W.; Jori, G.; Kessel, D.; Korbelik, M.; Moan, J.; Peng, Q. Photodynamic therapy. J. Natl. Cancer Inst. 1998, 90, 889–905. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.J.; He, Y.Y.; Huang, C.G.; Huang, J.S.; Huang, Y.C.; An, J.Y.; Gu, Y.; Jiang, L.J. Pharmacokinetics, tissue distribution and photodynamic therapy efficacy of liposomal-delivered hypocrellin A, a potential photosensitizer for tumor therapy. Photochem. Photobiol. 1999, 70, 773–780. [Google Scholar] [CrossRef]
- Derycke, A.S.; de Witte, P.A. Liposomes for photodynamic therapy. Adv. Drug Deliv. Rev. 2004, 56, 17–30. [Google Scholar] [CrossRef]
- Biel, M.A. Photodynamic therapy in head and neck cancer. Curr. Oncol. Rep. 2002, 4, 87–96. [Google Scholar] [CrossRef]
- Fukuda, H.; Casas, A.; Batlle, A. Aminolevulinic acid: From its unique biological function to its star role in photodynamic therapy. Int. J. Biochem. Cell Biol. 2005, 37, 272–276. [Google Scholar] [CrossRef]
- Chen, Q.; Dan, H.; Tang, F.; Wang, J.; Li, X.; Cheng, J.; Zhao, H.; Zeng, X. Photodynamic therapy guidelines for the management of oral leucoplakia. Int. J. Oral Sci. 2019, 11, 14. [Google Scholar] [CrossRef]
- Wong, S.J.; Campbell, B.; Massey, B.; Lynch, D.P.; Cohen, E.E.W.; Blair, E.; Selle, R.; Shklovskaya, J.; Jovanovic, B.D.; Skripkauskas, S.; et al. A phase I trial of aminolevulinic acid-photodynamic therapy for treatment of oral leukoplakia. Oral Oncol. 2013, 49, 970–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubler, A.; Haase, T.; Rheinwald, M.; Barth, T.; Muhling, J. Treatment of oral leukoplakia by topical application of 5-aminolevulinic acid. Int. J. Oral Maxillofac. Surg. 1998, 27, 466–469. [Google Scholar] [CrossRef]
- Sieron, A.; Adamek, M.; Kawczyk-Krupka, A.; Mazur, S.; Ilewicz, L. Photodynamic therapy (PDT) using topically applied delta-aminolevulinic acid (ALA) for the treatment of oral leukoplakia. J. Oral Pathol. Med. 2003, 32, 330–336. [Google Scholar] [CrossRef]
- Chen, H.M.; Yu, C.H.; Tu, P.C.; Yeh, C.Y.; Tsai, T.; Chiang, C.P. Successful treatment of oral verrucous hyperplasia and oral leukoplakia with topical 5-aminolevulinic acid-mediated photodynamic therapy. Lasers Surg. Med. 2005, 37, 114–122. [Google Scholar] [CrossRef]
- Siddiqui, S.A.; Siddiqui, S.; Hussain, M.A.B.; Khan, S.; Liu, H.; Akhtar, K.; Hasan, S.A.; Ahmed, I.; Mallidi, S.; Khan, A.P.; et al. Clinical evaluation of a mobile, low-cost system for fluorescence guided photodynamic therapy of early oral cancer in India. Photodiagnosis Photodyn. Ther. 2022, 38, 102843. [Google Scholar] [CrossRef]
- Yao, Y.L.; Wang, Y.F.; Li, C.X.; Wu, L.; Tang, G.Y. Management of oral leukoplakia by ablative fractional laser-assisted photodynamic therapy: A 3-year retrospective study of 48 patients. Lasers Surg. Med. 2022, 54, 682–687. [Google Scholar] [CrossRef]
- Gorsky, M.; Epstein, J.B. Oral lichen planus: Malignant transformation and human papilloma virus: A review of potential clinical implications. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 461–464. [Google Scholar] [CrossRef]
- Raghavendra Kini, D.N.; Saha, A. Therapeutic Management of Oral Lichen Planus: A Review for the Clinicians. World J. Dent. 2011, 2, 249–253. [Google Scholar] [CrossRef]
- Tardivo, J.P.; Del Giglio, A.; de Oliveira, C.S.; Gabrielli, D.S.; Junqueira, H.C.; Tada, D.B.; Severino, D.; de Fatima Turchiello, R.; Baptista, M.S. Methylene blue in photodynamic therapy: From basic mechanisms to clinical applications. Photodiagnosis Photodyn. Ther. 2005, 2, 175–191. [Google Scholar] [CrossRef]
- Aghahosseini, F.; Arbabi-Kalati, F.; Fashtami, L.A.; Djavid, G.E.; Fateh, M.; Beitollahi, J.M. Methylene blue-mediated photodynamic therapy: A possible alternative treatment for oral lichen planus. Lasers Surg. Med. 2006, 38, 33–38. [Google Scholar] [CrossRef]
- Sadaksharam, J.; Nayaki, K.P.; Selvam, N.P. Treatment of oral lichen planus with methylene blue mediated photodynamic therapy—A clinical study. Photodermatol. Photoimmunol. Photomed. 2012, 28, 97–101. [Google Scholar] [CrossRef]
- Bakhtiari, S.; Azari-Marhabi, S.; Mojahedi, S.M.; Namdari, M.; Rankohi, Z.E.; Jafari, S. Comparing clinical effects of photodynamic therapy as a novel method with topical corticosteroid for treatment of oral lichen planus. Photodiagnosis Photodyn. Ther. 2017, 20, 159–164. [Google Scholar] [CrossRef]
- Mostafa, D.; Moussa, E.; Alnouaem, M. Evaluation of photodynamic therapy in treatment of oral erosive lichen planus in comparison with topically applied corticosteroids. Photodiagnosis Photodyn. Ther. 2017, 19, 56–66. [Google Scholar] [CrossRef]
- Biel, M.A. Photodynamic therapy and the treatment of head and neck cancers. J. Clin. Laser Med. Surg. 1996, 14, 239–244. [Google Scholar] [CrossRef]
- Biel, M.A. Photodynamic therapy as an adjuvant intraoperative treatment of recurrent head and neck carcinomas. Arch. Otolaryngol. 1996, 122, 1261–1265. [Google Scholar] [CrossRef] [PubMed]
- Biel, M. Advances in photodynamic therapy for the treatment of head and neck cancers. Lasers Surg. Med. 2006, 38, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, H.; Tobita, T.; Ohba, S.; Uehara, M.; Asahina, I. Treatment outcome of Photofrin-based photodynamic therapy for T1 and T2 oral squamous cell carcinoma and dysplasia. Photodiagnosis Photodyn. Ther. 2013, 10, 229–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopper, C.; Kubler, A.; Lewis, H.; Tan, I.B.; Putnam, G. mTHPC-mediated photodynamic therapy for early oral squamous cell carcinoma. Int. J. Cancer 2004, 111, 138–146. [Google Scholar] [CrossRef]
- D’Cruz, A.K.; Robinson, M.H.; Biel, M.A. mTHPC-mediated photodynamic therapy in patients with advanced, incurable head and neck cancer: A multicenter study of 128 patients. Head Neck 2004, 26, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Kubler, A.C.; de Carpentier, J.; Hopper, C.; Leonard, A.G.; Putnam, G. Treatment of squamous cell carcinoma of the lip using Foscan-mediated photodynamic therapy. Int. J. Oral Maxillofac. Surg 2001, 30, 504–509. [Google Scholar] [CrossRef]
- Kubler, A.; Niziol, C.; Sidhu, M.; Dunne, A.; Werner, J.A. Analysis of cost effectiveness of photodynamic therapy with Foscan (Foscan-PDT) in comparison with palliative chemotherapy in patients with advanced head-neck tumors in Germany. Laryngorhinootologie 2005, 84, 725–732. [Google Scholar] [CrossRef]
- Karakullukçu, B.; van Oudenaarde, K.; Copper, M.P.; Klop, W.M.; van Veen, R.; Wildeman, M.; Bing Tan, I. Photodynamic therapy of early stage oral cavity and oropharynx neoplasms: An outcome analysis of 170 patients. Eur. Arch. Otorhinolaryngol. 2011, 268, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Copper, M.P.; Tan, I.B.; Oppelaar, H.; Ruevekamp, M.C.; Stewart, F.A. Meta-tetra(hydroxyphenyl)chlorin photodynamic therapy in early-stage squamous cell carcinoma of the head and neck. Arch. Otolaryngol. Head Neck Surg. 2003, 129, 709–711. [Google Scholar] [CrossRef] [Green Version]
- Jerjes, W.; Upile, T.; Radhi, H.; Hopper, C. Photodynamic therapy and end-stage tongue base cancer: Short communication. Head Neck Oncol. 2011, 3, 49. [Google Scholar] [CrossRef] [Green Version]
- Sobaniec, S.; Bernaczyk, P.; Pietruski, J.; Cholewa, M.; Skurska, A.; Dolinska, E.; Duraj, E.; Tokajuk, G.; Paniczko, A.; Olszewska, E.; et al. Clinical assessment of the efficacy of photodynamic therapy in the treatment of oral lichen planus. Lasers Med. Sci. 2013, 28, 311–316. [Google Scholar] [CrossRef] [Green Version]
- Rigual, N.; Shafirstein, G.; Cooper, M.T.; Baumann, H.; Bellnier, D.A.; Sunar, U.; Tracy, E.C.; Rohrbach, D.J.; Wilding, G.; Tan, W.; et al. Photodynamic therapy with 3-(1’-hexyloxyethyl) pyropheophorbide a for cancer of the oral cavity. Clin. Cancer Res. 2013, 19, 6605–6613. [Google Scholar] [CrossRef] [Green Version]
- Skupin-Mrugalska, P.; Zalewski, T.; Elvang, P.A.; Nowaczyk, G.; Czajkowski, M.; Piotrowska-Kempisty, H. Insight into theranostic nanovesicles prepared by thin lipid hydration and microfluidic method. Colloids Surf. B Biointerfaces 2021, 205, 111871. [Google Scholar] [CrossRef]
- Wang, D.; Fei, B.; Halig, L.V.; Qin, X.; Hu, Z.; Xu, H.; Wang, Y.A.; Chen, Z.; Kim, S.; Shin, D.M.; et al. Targeted iron-oxide nanoparticle for photodynamic therapy and imaging of head and neck cancer. ACS Nano 2014, 8, 6620–6632. [Google Scholar] [CrossRef]
- Liang, J.; Yang, B.; Zhou, X.; Han, Q.; Zou, J.; Cheng, L. Stimuli-responsive drug delivery systems for head and neck cancer therapy. Drug Deliv. 2021, 28, 272–284. [Google Scholar] [CrossRef]
- Song, C.; Ran, J.; Wei, Z.; Wang, Y.; Chen, S.; Lin, L.; Zhang, G.; Cai, Y.; Han, W. Organic near-infrared-II nanophotosensitizer for safe cancer phototheranostics and improving immune microenvironment against metastatic tumor. ACS Appl. Mater. Interfaces 2021, 13, 3547–3558. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xie, D.; Pan, J.; Xia, C.; Fan, L.; Pu, Y.; Zhang, Q.; Ni, Y.H.; Wang, J.; Hu, Q. A near infrared light-triggered human serum albumin drug delivery system with coordination bonding of indocyanine green and cisplatin for targeting photochemistry therapy against oral squamous cell cancer. Biomater. Sci. 2019, 7, 5270–5282. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Wang, J.H.; Liu, Q.; Huang, H.; Chen, M.; Li, K.; Li, C.; Yu, X.F.; Chu, P.K. Rose-bengal-conjugated gold nanorods for in vivo photodynamic and photothermal oral cancer therapies. Biomaterials 2014, 35, 1954–1966. [Google Scholar] [CrossRef]
- Ren, S.; Cheng, X.; Chen, M.; Liu, C.; Zhao, P.; Huang, W.; He, J.; Zhou, Z.; Miao, L. Hypotoxic and rapidly metabolic PEG-PCL-C3-ICG nanoparticles for fluorescence-guided photothermal/photodynamic therapy against OSCC. ACS Appl. Mater. Interfaces 2017, 9, 31509–31518. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Shi, L.; Huang, Y.; Shen, L.; Peng, H.; Zhu, X.; Zhou, G. Nanoparticle delivery of Wnt-1 siRNA enhances photodynamic therapy by inhibiting epithelial-mesenchymal transition for oral cancer. Biomater. Sci. 2017, 5, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Günaydin, G.; Gedik, M.E.; Ayan, S. Photodynamic therapy-current limitations and novel approaches. Front. Chem. 2021, 9, 691697. [Google Scholar] [CrossRef] [PubMed]
- Jerjes, W.; Hamdoon, Z.; Hopper, C. Photodynamic therapy in the management of potentially malignant and malignant oral disorders. Head Neck Oncol. 2012, 4, 16. [Google Scholar] [CrossRef] [Green Version]
- Cerrati, E.W.; Nguyen, S.A.; Farrar, J.D.; Lentsch, E.J. The efficacy of photodynamic therapy in the treatment of oral squamous cell carcinoma: A meta-analysis. Ent-Ear Nose Throat 2015, 94, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Hinger, D.; Grafe, S.; Navarro, F.; Spingler, B.; Pandiarajan, D.; Walt, H.; Couffin, A.C.; Maake, C. Lipid nanoemulsions and liposomes improve photodynamic treatment efficacy and tolerance in CAL-33 tumor bearing nude mice. J. Nanobiotechnol. 2016, 14, 71. [Google Scholar] [CrossRef] [Green Version]
- Piskorz, J.; Skupin, P.; Lijewski, S.; Korpusinski, M.; Sciepura, M.; Konopka, K.; Sobiak, S.; Goslinski, T.; Mielcarek, J. Synthesis, physical-chemical properties and in vitro photodynamic activity against oral cancer cells of novel porphyrazines possessing fluoroalkylthio and dietherthio substituents. J. Fluor. Chem. 2012, 135, 265–271. [Google Scholar] [CrossRef]
- Piskorz, J.; Konopka, K.; Düzgüneş, N.; Gdaniec, Z.; Mielcarek, J.; Goslinski, T. Diazepinoporphyrazines containing peripheral styryl substituents and their promising nanomolar photodynamic activity against oral cancer cells in liposomal formulations. Chemmedchem 2014, 9, 1775–1782. [Google Scholar] [CrossRef]
- Neves, S.; Faneca, H.; Bertin, S.; Konopka, K.; Düzgüneş, N.; Pierrefite-Carle, V.; Simoes, S.; de Lima, M.C.P. Transferrin lipoplex-mediated suicide gene therapy of oral squamous cell carcinoma in an immunocompetent murine model and mechanisms involved in the antitumoral response. Cancer Gene Ther. 2009, 16, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.J.; Tian, L.L.; Zhang, R.; Dong, Z.L.; Wang, H.R.; Liu, Z. Collagenase-encapsulated pH-responsive nanoscale coordination polymers for tumor microenvironment modulation and enhancedphotodynamic nanomedicine. ACS Appl. Mater. Inter. 2018, 10, 43493–43502. [Google Scholar] [CrossRef] [PubMed]
- Kohli, A.G.; Kivimae, S.; Tiffany, M.R.; Szoka, F.C. Improving the distribution of Doxil (R) in the tumor matrix by depletion of tumor hyaluronan. J. Control Release 2014, 191, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Dolor, A.; Szoka, F.C. Digesting a path forward: The Uutility of collagenase tumor treatment for improved drug delivery. Mol. Pharmaceut. 2018, 15, 2069–2083. [Google Scholar] [CrossRef]
- Pandey, M.; Choudhury, H.; Ying, J.N.S.; Ling, J.F.S.; Ting, J.; Ting, J.S.S.; Hwen, I.K.Z.; Suen, H.W.; Kamar, H.S.S.; Gorain, B.; et al. Mucoadhesive nanocarriers as a promising strategy to enhance intracellular delivery against oral cavity carcinoma. Pharmaceutics 2022, 14, 795. [Google Scholar] [CrossRef]
- Alaei, S.; Omidian, H. Mucoadhesion and mechanical assessment of oral films. Eur. J. Pharm. Sci. 2021, 159, 105727. [Google Scholar] [CrossRef] [PubMed]
- Piskorz, J.; Lijewski, S.; Gierszewski, M.; Gorniak, K.; Sobotta, L.; Wicher, B.; Tykarska, E.; Duzgunes, N.; Konopka, K.; Sikorski, D.; et al. Sulfanyl porphyrazines: Molecular barrel-like self-assembly in crystals, optical properties and in vitro photodynamic activity towards cancer cells. Dyes Pigment. 2017, 136, 898–908. [Google Scholar] [CrossRef]
- Skupin-Mrugalska, P.; Koczorowski, T.; Szczolko, W.; Dlugaszewska, J.; Teubert, A.; Piotrowska-Kempisty, H.; Goslinski, T.; Sobotta, L. Cationic porphyrazines with morpholinoethyl substituents-Syntheses, optical properties, and photocytotoxicities. Dyes Pigment. 2022, 197, 109937. [Google Scholar] [CrossRef]
- Mlynarczyk, D.T.; Lijewski, S.; Falkowski, M.; Piskorz, J.; Szczolko, W.; Sobotta, L.; Stolarska, M.; Popenda, L.; Jurga, S.; Konopka, K.; et al. Dendrimeric sulfanyl porphyrazines: Synthesis, physico-chemical characterization, and biological activity for potential applications in photodynamic therapy. Chempluschem 2016, 81, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Mlynarczyk, D.T.; Piskorz, J.; Popenda, L.; Stolarska, M.; Szczolko, W.; Konopka, K.; Jurga, S.; Sobotta, L.; Mielcarek, J.; Düzgüneş, N.; et al. S-seco-porphyrazine as a new member of the seco-porphyrazine family-Synthesis, characterization and photocytotoxicity against cancer cells. Bioorg. Chem. 2020, 96, 103634. [Google Scholar] [CrossRef]
- Piskorz, J.; Mlynarczyk, D.T.; Szczolko, W.; Konopka, K.; Düzgüneş, N.; Mielcarek, J. Liposomal formulations of magnesium sulfanyl tribenzoporphyrazines for the photodynamic therapy of cancer. J. Inorg. Biochem. 2018, 184, 34–41. [Google Scholar] [CrossRef]
- Young, J.; Yee, M.; Kim, H.Y.; Cheung, J.; Chino, T.; Düzgüneş, N.; Konopka, K. Phototoxicity of liposomal Zn-and Al-phthalocyanine against cervical and oral squamous cell carcinoma cells in vitro. Med. Sci. Monit. Basic 2016, 22, 156–164. [Google Scholar] [CrossRef] [Green Version]
- Cheung, J.; Furukawa, D.; Pandez, R.; Yıldırım, M.; Frazier, A.; Piskorz, J.; Düzgüneş, N.; Konopka, K. Photocytotoxicity of liposomal zinc phthalocyanine in oral squamous cell carcinoma and pharyngeal carcinoma cells. Ther. Deliv. 2020, 11, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Skupin-Mrugalska, P.; Szczolko, W.; Gierlich, P.; Konopka, K.; Goslinski, T.; Mielcarek, J.; Düzgüneş, N. Physicochemical properties of liposome-incorporated 2-(morpholin-4-yl)ethoxy phthalocyanines and their photodynamic activity against oral cancer cells. J. Photoch. Photobio. A 2018, 353, 445–457. [Google Scholar] [CrossRef]
- Dlugaszewska, J.; Szczolko, W.; Koczorowski, T.; Skupin-Mrugalska, P.; Teubert, A.; Konopka, K.; Kucinska, M.; Murias, M.; Düzgüneş, N.; Mielcarek, J.; et al. Antimicrobial and anticancer photodynamic activity of a phthalocyanine photosensitizer with N-methyl morpholiniumethoxy substituents in non-peripheral positions. J. Inorg. Biochem. 2017, 172, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Janas, K.; Boniewska-Bernacka, E.; Dyrda, G.; Slota, R. Porphyrin and phthalocyanine photosensitizers designed for targeted photodynamic therapy of colorectal cancer. Bioorgan. Med. Chem. 2021, 30, 115926. [Google Scholar] [CrossRef] [PubMed]
- Santos, K.L.M.; Barros, R.M.; Lima, D.P.S.; Nunes, A.M.A.; Sato, M.R.; Faccio, R.; Damasceno, B.P.G.D.; Oshiro, J.A. Prospective application of phthalocyanines in the photodynamic therapy against microorganisms and tumor cells: A mini-review. Photodiagn. Photodyn. 2020, 32, 102032. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.P.; Babu, P.S.S.; Nair, S.A.; Ramakrishnan, S.; Ramaiah, D.; Chandrashekar, T.K.; Srinivasan, A.; Pillai, M.R. meso-Tetrakis(p-sulfonatophenyl)N-confused porphyrin tetrasodium salt: A potential sensitizer for photodynamic therapy. J. Med. Chem. 2012, 55, 5110–5120. [Google Scholar] [CrossRef] [PubMed]
- Chin, Y.; Lim, S.H.; Zorlu, Y.; Ahsen, V.; Kiew, L.V.; Chung, L.Y.; Dumoulin, F.; Lee, H.B. Improved photodynamic efficacy of Zn(II) phthalocyanines via glycerol substitution. PLoS ONE 2014, 9, e97894. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.; Bae, J.Y.; Son, H.K.; Lee, D.Y.; Park, G.; You, H.; Ko, H.; Kim, Y.C.; Kim, J. RUNX3 confers sensitivity to pheophorbide a-photodynamic therapy in human oral squamous cell carcinoma cell lines. Laser Med. Sci. 2015, 30, 499–507. [Google Scholar] [CrossRef]
- Chu, P.L.; Shihabuddeen, W.A.; Low, K.P.; Poon, D.J.J.; Ramaswamy, B.; Lang, Z.G.; Nei, W.L.; Chua, K.L.M.; Thong, P.S.P.; Soo, K.C.; et al. Vandetanib sensitizes head and neck squamous cell carcinoma to photodynamic therapy through modulation of EGFR-dependent DNA repair and the tumour microenvironment. Photodiagn. Photodyn. 2019, 27, 367–374. [Google Scholar] [CrossRef]
- Bonnet, D.; Dick, J.E. Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat. Med. 1997, 3, 730–737. [Google Scholar] [CrossRef]
- Al-Hajj, M.; Wicha, M.S.; Benito-Hernandez, A.; Morrison, S.J.; Clarke, M.F. Prospective identification of tumorigenic breast cancer cells. Proc. Natl. Acad. Sci. USA 2003, 100, 3983–3988. [Google Scholar] [CrossRef] [Green Version]
- Mackenzie, I.C. Growth of malignant oral epithelial stem cells after seeding into organotypical cultures of normal mucosa. J. Oral Pathol. Med. 2004, 33, 71–78. [Google Scholar] [CrossRef]
- Mannelli, G.; Gallo, O. Cancer stem cells hypothesis and stem cells in head and neck cancers. Cancer Treat. Rev. 2012, 38, 515–539. [Google Scholar] [CrossRef]
- Rodini, C.O.; Lopes, N.M.; Lara, V.S.; Mackenzie, I.C. Oral cancer stem cells-properties and consequences. J. Appl. Oral Sci. 2017, 25, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Elkashty, O.A.; Abu Elghanam, G.; Su, X.Y.; Liu, Y.N.; Chauvin, P.J.; Tran, S.D. Cancer stem cells enrichment with surface markers CD271 and CD44 in human head and neck squamous cell carcinomas. Carcinogenesis 2020, 41, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Güleryüz, B.; Ünal, U.; Gülsoy, M. Near infrared light activated upconversion nanoparticles (UCNP) based photodynamic therapy of prostate cancers: An in vitro study. Photodiagn. Photodyn. Ther. 2021, 36, 102616. [Google Scholar] [CrossRef]
- Chatterjee, D.K.; Yong, Z. Upconverting nanoparticles as nanotransducers for photodynamic therapy in cancer cells. Nanomedicine 2008, 3, 73–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawamura, T.; Tanaka, T.; Ishige, H.; Iizuka, M.; Murayama, Y.; Otsuji, E.; Ohkubo, A.; Ogura, S.I.; Yuasa, H. The effect of coatings on the affinity of lanthanide nanoparticles to MKN45 and HeLa cancer cells and improvement in photodynamic therapy Eeficiency. Int. J. Mol. Sci. 2015, 16, 22415–22424. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.Y.; Liao, M.L.; Hong, G.C.; Chang, W.W.; Chu, C.C. Near-infrared-triggered photodynamic therapy toward breast cancer cells using dendrimer-functionalized upconversion nanoparticles. Nanomaterials 2017, 7, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, Y.L.; Fu, L.H.; Li, C.Y.; Lin, J.; Huang, P. Conquering the hypoxia limitation for photodynamic therapy. Adv. Mater. 2021, 33, 202103978. [Google Scholar] [CrossRef]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Düzgüneş, N.; Piskorz, J.; Skupin-Mrugalska, P.; Yıldırım, M.; Sessevmez, M.; Cheung, J. Photodynamic Therapy of Oral Cancer and Novel Liposomal Photosensitizers. Oral 2023, 3, 276-294. https://doi.org/10.3390/oral3030023
Düzgüneş N, Piskorz J, Skupin-Mrugalska P, Yıldırım M, Sessevmez M, Cheung J. Photodynamic Therapy of Oral Cancer and Novel Liposomal Photosensitizers. Oral. 2023; 3(3):276-294. https://doi.org/10.3390/oral3030023
Chicago/Turabian StyleDüzgüneş, Nejat, Jaroslaw Piskorz, Paulina Skupin-Mrugalska, Metin Yıldırım, Melike Sessevmez, and Jennifer Cheung. 2023. "Photodynamic Therapy of Oral Cancer and Novel Liposomal Photosensitizers" Oral 3, no. 3: 276-294. https://doi.org/10.3390/oral3030023