
Peripheral T-Cell Lymphomas of the T Follicular Helper Type: Clinical, Pathological, and Genetic Attributes


Abstract
:1. Introduction
2. Angioimmunoblastic T-Cell Lymphoma
2.1. Epidemiology and Clinical Features
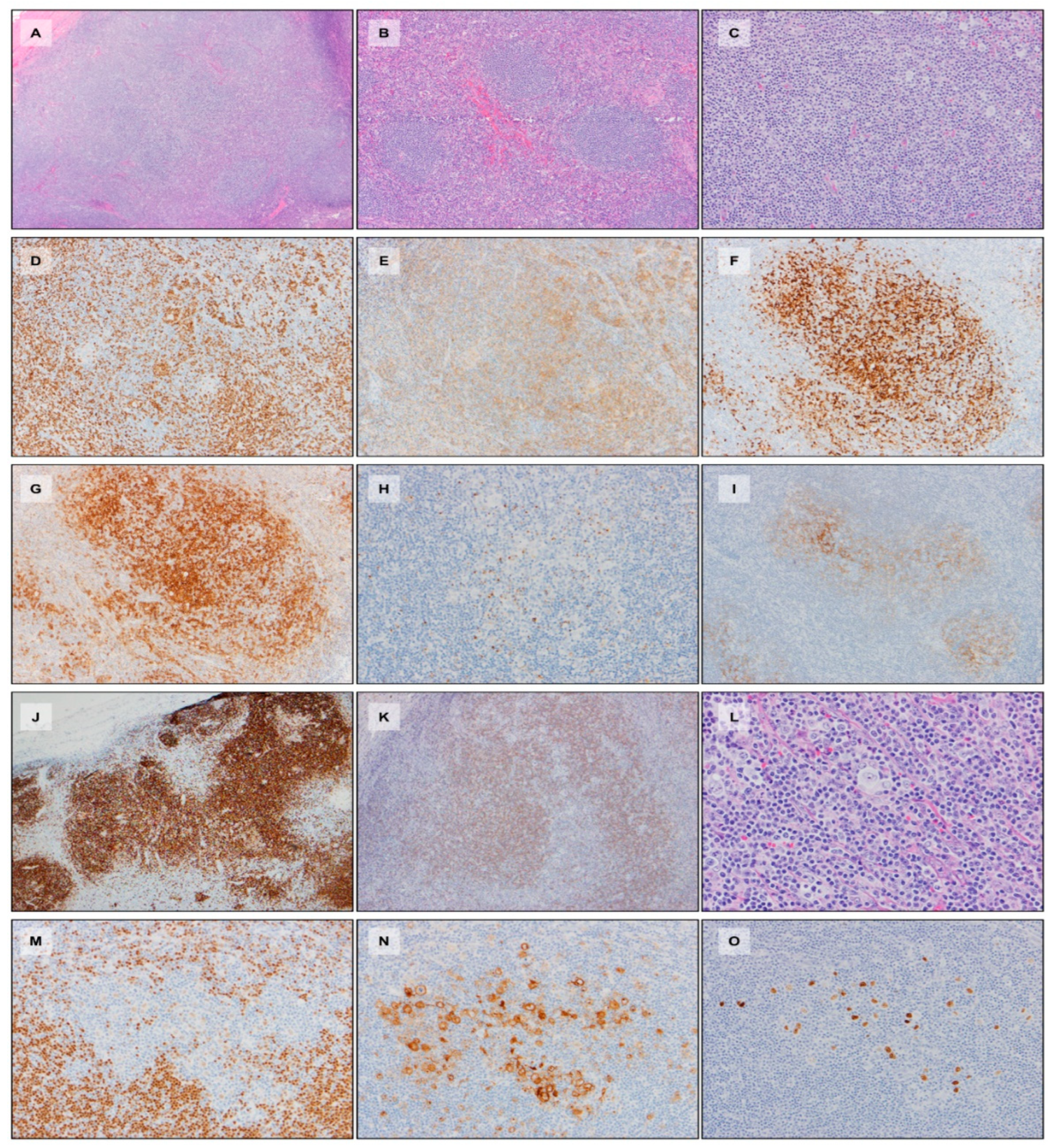
2.2. Morphology and Immunophenotype
2.3. EBV, B-Cell, and Plasma Cell Proliferations
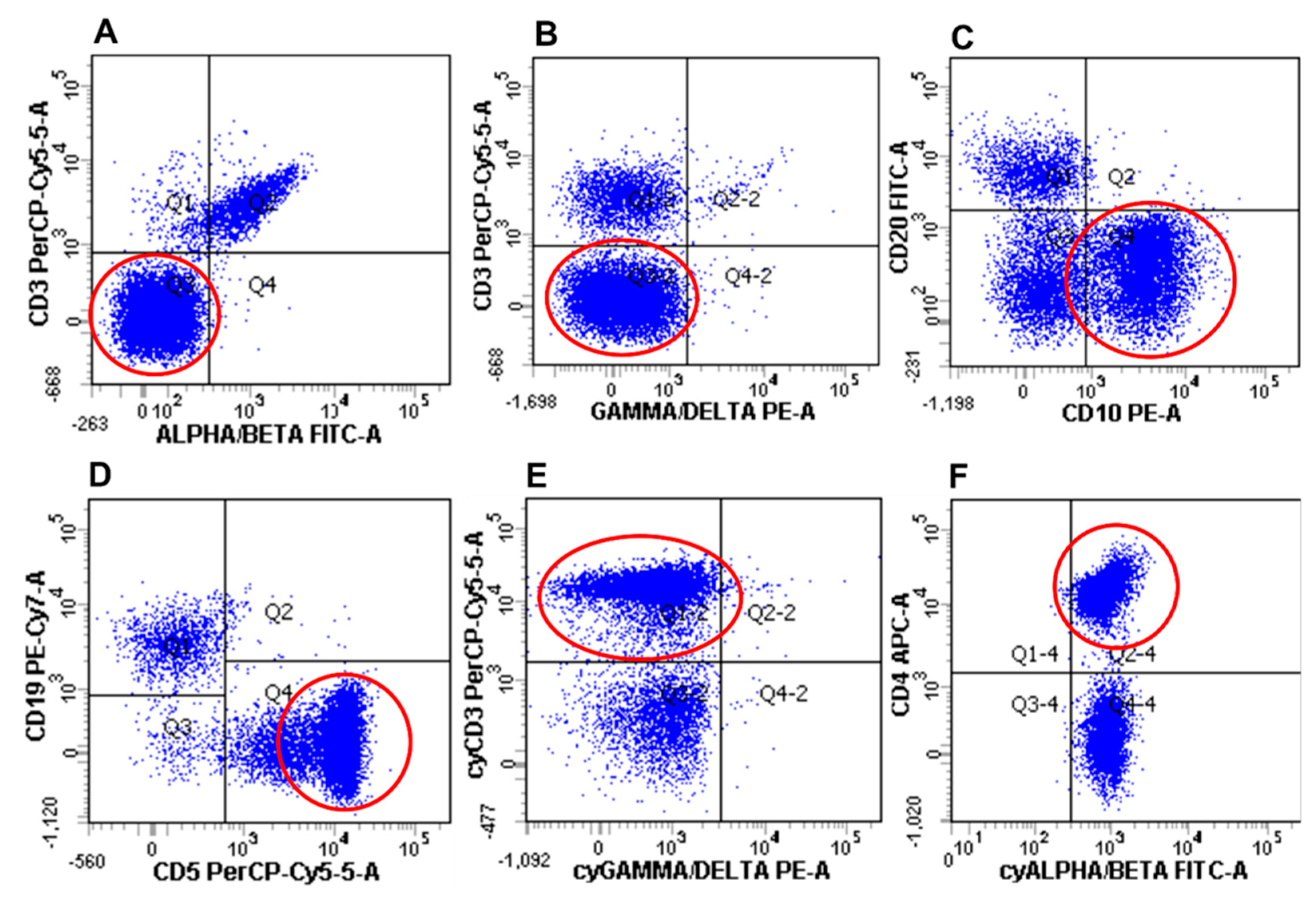
2.4. Flow Cytometry
2.5. Genetics
2.6. Differential Diagnoses
3. Follicular T-Cell Lymphoma
3.1. Epidemiology and Clinical Features
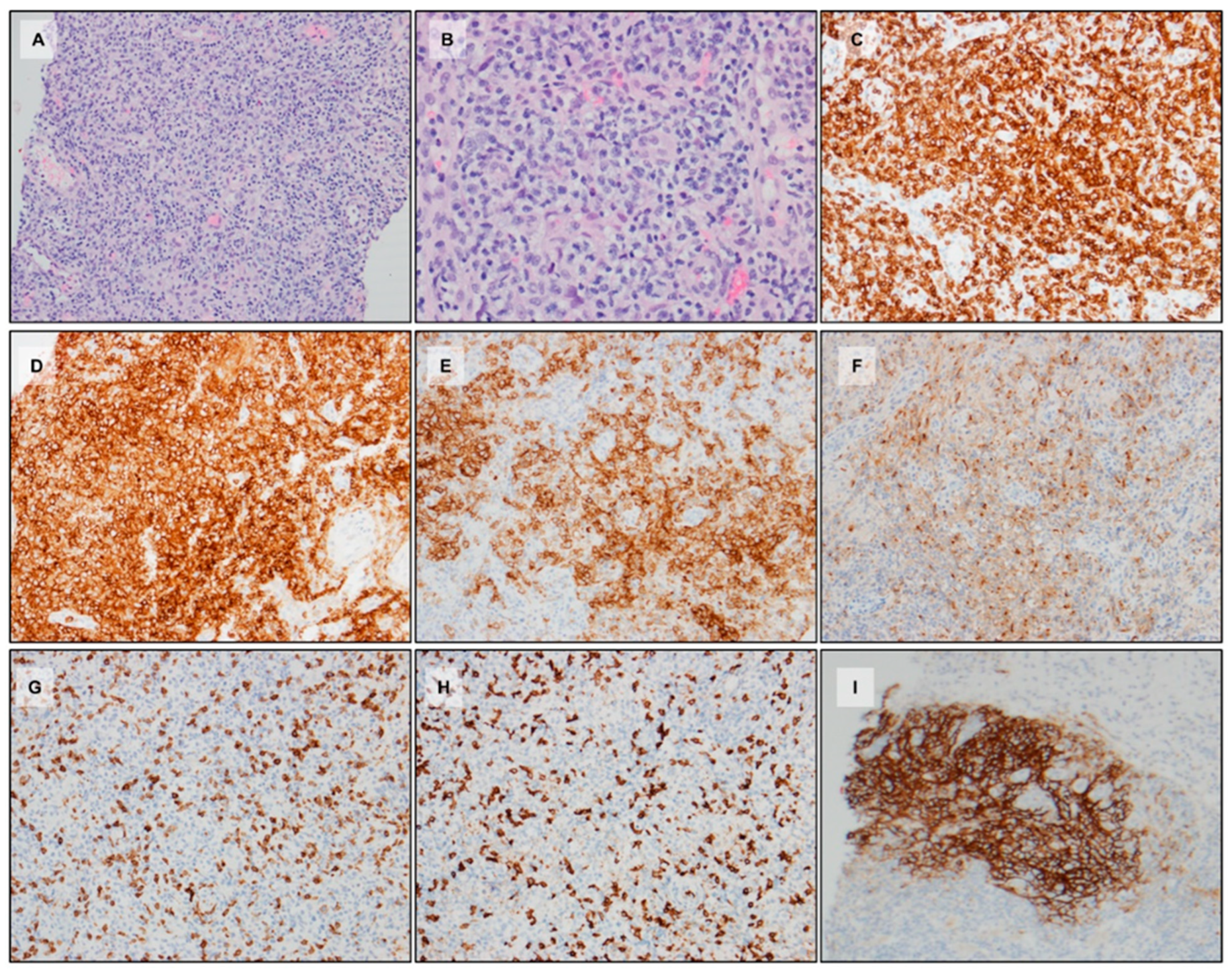
3.2. Morphology and Immunophenotype
3.3. Molecular Studies
3.4. Differential Diagnoses
4. Peripheral T-Cell Lymphoma with TFH Phenotype
5. G. Genetics of TFH Lymphomas
6. TFH Lymphomas, Clonal Hematopoiesis of Indeterminate Potential, and Myeloid Neoplasms
7. Treatment and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crotty, S. T follicular helper cell differentiation, function, and roles in disease. Immunity 2014, 41, 529–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crotty, S. A brief history of t cell help to b cells. Nat. Rev. Immunol. 2015, 15, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Goenka, R.; Barnett, L.G.; Silver, J.S.; O’Neill, P.J.; Hunter, C.A.; Cancro, M.P.; Laufer, T.M. Cutting edge: Dendritic cell-restricted antigen presentation initiates the follicular helper t cell program but cannot complete ultimate effector differentiation. J. Immunol. 2011, 187, 1091–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crotty, S. Follicular helper cd4 t cells (tfh). Annu. Rev. Immunol. 2011, 29, 621–663. [Google Scholar] [CrossRef]
- Crotty, S.; Johnston, R.J.; Schoenberger, S.P. Effectors and memories: Bcl-6 and blimp-1 in t and b lymphocyte differentiation. Nat. Immunol. 2010, 11, 114–120. [Google Scholar] [CrossRef]
- Crotty, S. T follicular helper cell biology: A decade of discovery and diseases. Immunity 2019, 50, 1132–1148. [Google Scholar] [CrossRef]
- Suan, D.; Nguyen, A.; Moran, I.; Bourne, K.; Hermes, J.R.; Arshi, M.; Hampton, H.R.; Tomura, M.; Miwa, Y.; Kelleher, A.D.; et al. T follicular helper cells have distinct modes of migration and molecular signatures in naive and memory immune responses. Immunity 2015, 42, 704–718. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Vinuesa, C.G. The elusive identity of t follicular helper cells. Trends Immunol. 2010, 31, 377–383. [Google Scholar] [CrossRef]
- Cubas, R.A.; Mudd, J.C.; Savoye, A.L.; Perreau, M.; van Grevenynghe, J.; Metcalf, T.; Connick, E.; Meditz, A.; Freeman, G.J.; Abesada-Terk, G., Jr.; et al. Inadequate t follicular cell help impairs b cell immunity during hiv infection. Nat. Med. 2013, 19, 494–499. [Google Scholar] [CrossRef] [Green Version]
- Simpson, N.; Gatenby, P.A.; Wilson, A.; Malik, S.; Fulcher, D.A.; Tangye, S.G.; Manku, H.; Vyse, T.J.; Roncador, G.; Huttley, G.A.; et al. Expansion of circulating t cells resembling follicular helper t cells is a fixed phenotype that identifies a subset of severe systemic lupus erythematosus. Arthritis Rheumatol. 2010, 62, 234–244. [Google Scholar] [CrossRef]
- Gu-Trantien, C.; Loi, S.; Garaud, S.; Equeter, C.; Libin, M.; de Wind, A.; Ravoet, M.; Le Buanec, H.; Sibille, C.; Manfouo-Foutsop, G.; et al. Cd4(+) follicular helper t cell infiltration predicts breast cancer survival. J. Clin. Investig. 2013, 123, 2873–2892. [Google Scholar] [CrossRef] [PubMed]
- Grogg, K.L.; Attygalle, A.D.; Macon, W.R.; Remstein, E.D.; Kurtin, P.J.; Dogan, A. Angioimmunoblastic t-cell lymphoma: A neoplasm of germinal-center t-helper cells? Blood 2005, 106, 1501–1502. [Google Scholar] [CrossRef] [PubMed]
- De Leval, L.; Rickman, D.S.; Thielen, C.; Reynies, A.; Huang, Y.L.; Delsol, G.; Lamant, L.; Leroy, K.; Briere, J.; Molina, T.; et al. The gene expression profile of nodal peripheral t-cell lymphoma demonstrates a molecular link between angioimmunoblastic t-cell lymphoma (aitl) and follicular helper t (tfh) cells. Blood 2007, 109, 4952–4963. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Pinilla, S.M.; Atienza, L.; Murillo, C.; Perez-Rodriguez, A.; Montes-Moreno, S.; Roncador, G.; Perez-Seoane, C.; Dominguez, P.; Camacho, F.I.; Piris, M.A. Peripheral t-cell lymphoma with follicular t-cell markers. Am. J. Surg. Pathol. 2008, 32, 1787–1799. [Google Scholar] [CrossRef]
- Huang, Y.; Moreau, A.; Dupuis, J.; Streubel, B.; Petit, B.; Le Gouill, S.; Martin-Garcia, N.; Copie-Bergman, C.; Gaillard, F.; Qubaja, M.; et al. Peripheral t-cell lymphomas with a follicular growth pattern are derived from follicular helper t cells (tfh) and may show overlapping features with angioimmunoblastic t-cell lymphomas. Am. J. Surg. Pathol. 2009, 33, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Dobay, M.P.; Lemonnier, F.; Missiaglia, E.; Bastard, C.; Vallois, D.; Jais, J.P.; Scourzic, L.; Dupuy, A.; Fataccioli, V.; Pujals, A.; et al. Integrative clinicopathological and molecular analyses of angioimmunoblastic t-cell lymphoma and other nodal lymphomas of follicular helper t-cell origin. Haematologica 2017, 102, e148–e151. [Google Scholar] [CrossRef] [Green Version]
- Beltraminelli, H.; Leinweber, B.; Kerl, H.; Cerroni, L. Primary cutaneous cd4+ small-/medium-sized pleomorphic t-cell lymphoma: A cutaneous nodular proliferation of pleomorphic t lymphocytes of undetermined significance? A study of 136 cases. Am. J. Dermatopathol. 2009, 31, 317–322. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Arber, D.A.; Hasserjian, R.P.; Le Beau, M.M.; et al. Who Classification of Tumours of Haematopoietic and Lymphoid Tissues (Revised 4th Edition); International Agency for Research on Cancer: Lyon, France, 2017. [Google Scholar]
- Beltzung, F.; Ortonne, N.; Pelletier, L.; Beylot-Barry, M.; Ingen-Housz-Oro, S.; Franck, F.; Pereira, B.; Godfraind, C.; Delfau, M.H.; D’Incan, M.; et al. Primary cutaneous cd4+ small/medium t-cell lymphoproliferative disorders: A clinical, pathologic, and molecular study of 60 cases presenting with a single lesion: A multicenter study of the french cutaneous lymphoma study group. Am. J. Surg. Pathol. 2020, 44, 862–872. [Google Scholar] [CrossRef]
- Alikhan, M.; Song, J.Y.; Sohani, A.R.; Moroch, J.; Plonquet, A.; Duffield, A.S.; Borowitz, M.J.; Jiang, L.; Bueso-Ramos, C.; Inamdar, K.; et al. Peripheral t-cell lymphomas of follicular helper t-cell type frequently display an aberrant cd3(-/dim)cd4(+) population by flow cytometry: An important clue to the diagnosis of a hodgkin lymphoma mimic. Mod. Pathol. 2016, 29, 1173–1182. [Google Scholar] [CrossRef]
- Attygalle, A.; Al-Jehani, R.; Diss, T.C.; Munson, P.; Liu, H.; Du, M.Q.; Isaacson, P.G.; Dogan, A. Neoplastic t cells in angioimmunoblastic t-cell lymphoma express cd10. Blood 2002, 99, 627–633. [Google Scholar] [CrossRef] [Green Version]
- Bisig, B.; Thielen, C.; Herens, C.; Gofflot, S.; Travert, M.; Delfau-Larue, M.H.; Boniver, J.; Gaulard, P.; de Leval, L. C-maf expression in angioimmunoblastic t-cell lymphoma reflects follicular helper t-cell derivation rather than oncogenesis. Histopathology 2012, 60, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Dorfman, D.M.; Brown, J.A.; Shahsafaei, A.; Freeman, G.J. Programmed death-1 (pd-1) is a marker of germinal center-associated t cells and angioimmunoblastic t-cell lymphoma. Am. J. Surg. Pathol. 2006, 30, 802–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roncador, G.; Garcia Verdes-Montenegro, J.F.; Tedoldi, S.; Paterson, J.C.; Klapper, W.; Ballabio, E.; Maestre, L.; Pileri, S.; Hansmann, M.L.; Piris, M.A.; et al. Expression of two markers of germinal center t cells (sap and pd-1) in angioimmunoblastic t-cell lymphoma. Haematologica 2007, 92, 1059–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basha, B.M.; Bryant, S.C.; Rech, K.L.; Feldman, A.L.; Vrana, J.A.; Shi, M.; Reed, K.A.; King, R.L. Application of a 5 marker panel to the routine diagnosis of peripheral t-cell lymphoma with t-follicular helper phenotype. Am. J. Surg. Pathol. 2019, 43, 1282–1290. [Google Scholar] [CrossRef]
- Dogan, A.; Attygalle, A.D.; Kyriakou, C. Angioimmunoblastic t-cell lymphoma. Br. J. Haematol. 2003, 121, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Piccaluga, P.P.; Agostinelli, C.; Califano, A.; Carbone, A.; Fantoni, L.; Ferrari, S.; Gazzola, A.; Gloghini, A.; Righi, S.; Rossi, M.; et al. Gene expression analysis of angioimmunoblastic lymphoma indicates derivation from t follicular helper cells and vascular endothelial growth factor deregulation. Cancer Res. 2007, 67, 10703–10710. [Google Scholar] [CrossRef] [Green Version]
- Piccaluga, P.P.; Fuligni, F.; De Leo, A.; Bertuzzi, C.; Rossi, M.; Bacci, F.; Sabattini, E.; Agostinelli, C.; Gazzola, A.; Laginestra, M.A.; et al. Molecular profiling improves classification and prognostication of nodal peripheral t-cell lymphomas: Results of a phase iii diagnostic accuracy study. J. Clin. Oncol. 2013, 31, 3019–3025. [Google Scholar] [CrossRef]
- Iqbal, J.; Wright, G.; Wang, C.; Rosenwald, A.; Gascoyne, R.D.; Weisenburger, D.D.; Greiner, T.C.; Smith, L.; Guo, S.; Wilcox, R.A.; et al. Gene expression signatures delineate biological and prognostic subgroups in peripheral t-cell lymphoma. Blood 2014, 123, 2915–2923. [Google Scholar] [CrossRef]
- Mourad, N.; Mounier, N.; Briere, J.; Raffoux, E.; Delmer, A.; Feller, A.; Meijer, C.J.; Emile, J.F.; Bouabdallah, R.; Bosly, A.; et al. Clinical, biologic, and pathologic features in 157 patients with angioimmunoblastic t-cell lymphoma treated within the groupe d’etude des lymphomes de l’adulte (gela) trials. Blood 2008, 111, 4463–4470. [Google Scholar] [CrossRef]
- Xie, Y.; Jaffe, E.S. How i diagnose angioimmunoblastic t-cell lymphoma. Am. J. Clin. Pathol. 2021, 156, 1–14. [Google Scholar] [CrossRef]
- De Leval, L.; Gisselbrecht, C.; Gaulard, P. Advances in the understanding and management of angioimmunoblastic t-cell lymphoma. Br. J. Haematol. 2010, 148, 673–689. [Google Scholar] [CrossRef] [PubMed]
- De Leval, L.; Parrens, M.; Le Bras, F.; Jais, J.P.; Fataccioli, V.; Martin, A.; Lamant, L.; Delarue, R.; Berger, F.; Arbion, F.; et al. Angioimmunoblastic t-cell lymphoma is the most common t-cell lymphoma in two distinct french information data sets. Haematologica 2015, 100, e361–e364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.U.; Chi, H.S.; Park, C.J.; Jang, S.; Seo, E.J.; Huh, J. Distinct features of angioimmunoblastic t-cell lymphoma with bone marrow involvement. Am. J. Clin. Pathol. 2009, 131, 640–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Federico, M.; Rudiger, T.; Bellei, M.; Nathwani, B.N.; Luminari, S.; Coiffier, B.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Savage, K.J.; et al. Clinicopathologic characteristics of angioimmunoblastic t-cell lymphoma: Analysis of the international peripheral t-cell lymphoma project. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 240–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lachenal, F.; Berger, F.; Ghesquieres, H.; Biron, P.; Hot, A.; Callet-Bauchu, E.; Chassagne, C.; Coiffier, B.; Durieu, I.; Rousset, H.; et al. Angioimmunoblastic t-cell lymphoma: Clinical and laboratory features at diagnosis in 77 patients. Medicine 2007, 86, 282–292. [Google Scholar] [CrossRef] [PubMed]
- Siegert, W.; Nerl, C.; Agthe, A.; Engelhard, M.; Brittinger, G.; Tiemann, M.; Lennert, K.; Huhn, D. Angioimmunoblastic lymphadenopathy (aild)-type t-cell lymphoma: Prognostic impact of clinical observations and laboratory findings at presentation. The kiel lymphoma study group. Ann. Oncol. 1995, 6, 659–664. [Google Scholar] [CrossRef]
- Dunleavy, K.; Wilson, W.H.; Jaffe, E.S. Angioimmunoblastic t cell lymphoma: Pathobiological insights and clinical implications. Curr. Opin. Hematol. 2007, 14, 348–353. [Google Scholar] [CrossRef]
- Anagnostopoulos, I.; Hummel, M.; Finn, T.; Tiemann, M.; Korbjuhn, P.; Dimmler, C.; Gatter, K.; Dallenbach, F.; Parwaresch, M.R.; Stein, H. Heterogeneous epstein-barr virus infection patterns in peripheral t-cell lymphoma of angioimmunoblastic lymphadenopathy type. Blood 1992, 80, 1804–1812. [Google Scholar] [CrossRef] [Green Version]
- Weiss, L.M.; Jaffe, E.S.; Liu, X.F.; Chen, Y.Y.; Shibata, D.; Medeiros, L.J. Detection and localization of epstein-barr viral genomes in angioimmunoblastic lymphadenopathy and angioimmunoblastic lymphadenopathy-like lymphoma. Blood 1992, 79, 1789–1795. [Google Scholar] [CrossRef] [Green Version]
- Pautier, P.; Devidas, A.; Delmer, A.; Dombret, H.; Sutton, L.; Zini, J.M.; Nedelec, G.; Molina, T.; Marolleau, J.P.; Brice, P. Angioimmunoblastic-like t-cell non hodgkin’s lymphoma: Outcome after chemotherapy in 33 patients and review of the literature. Leuk. Lymphoma 1999, 32, 545–552. [Google Scholar] [CrossRef]
- Attygalle, A.D.; Kyriakou, C.; Dupuis, J.; Grogg, K.L.; Diss, T.C.; Wotherspoon, A.C.; Chuang, S.S.; Cabecadas, J.; Isaacson, P.G.; Du, M.Q.; et al. Histologic evolution of angioimmunoblastic t-cell lymphoma in consecutive biopsies: Clinical correlation and insights into natural history and disease progression. Am. J. Surg. Pathol. 2007, 31, 1077–1088. [Google Scholar] [CrossRef]
- Ree, H.J.; Kadin, M.E.; Kikuchi, M.; Ko, Y.H.; Go, J.H.; Suzumiya, J.; Kim, D.S. Angioimmunoblastic lymphoma (aild-type t-cell lymphoma) with hyperplastic germinal centers. Am. J. Surg. Pathol. 1998, 22, 643–655. [Google Scholar] [CrossRef]
- Rodriguez-Justo, M.; Attygalle, A.D.; Munson, P.; Roncador, G.; Marafioti, T.; Piris, M.A. Angioimmunoblastic t-cell lymphoma with hyperplastic germinal centres: A neoplasia with origin in the outer zone of the germinal centre? Clinicopathological and immunohistochemical study of 10 cases with follicular t-cell markers. Mod. Pathol. 2009, 22, 753–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zettl, A.; Lee, S.S.; Rudiger, T.; Starostik, P.; Marino, M.; Kirchner, T.; Ott, M.; Muller-Hermelink, H.K.; Ott, G. Epstein-barr virus-associated b-cell lymphoproliferative disorders in angloimmunoblastic t-cell lymphoma and peripheral t-cell lymphoma, unspecified. Am. J. Clin. Pathol. 2002, 117, 368–379. [Google Scholar] [CrossRef] [PubMed]
- Nicolae, A.; Pittaluga, S.; Venkataraman, G.; Vijnovich-Baron, A.; Xi, L.; Raffeld, M.; Jaffe, E.S. Peripheral t-cell lymphomas of follicular t-helper cell derivation with hodgkin/reed-sternberg cells of b-cell lineage: Both ebv-positive and ebv-negative variants exist. Am. J. Surg. Pathol. 2013, 37, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Willenbrock, K.; Brauninger, A.; Hansmann, M.L. Frequent occurrence of b-cell lymphomas in angioimmunoblastic t-cell lymphoma and proliferation of epstein-barr virus-infected cells in early cases. Br. J. Haematol. 2007, 138, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Balague, O.; Martinez, A.; Colomo, L.; Rosello, E.; Garcia, A.; Martinez-Bernal, M.; Palacin, A.; Fu, K.; Weisenburger, D.; Colomer, D.; et al. Epstein-barr virus negative clonal plasma cell proliferations and lymphomas in peripheral t-cell lymphomas: A phenomenon with distinctive clinicopathologic features. Am. J. Surg. Pathol. 2007, 31, 1310–1322. [Google Scholar] [CrossRef]
- Huppmann, A.R.; Roullet, M.R.; Raffeld, M.; Jaffe, E.S. Angioimmunoblastic t-cell lymphoma partially obscured by an epstein-barr virus-negative clonal plasma cell proliferation. J. Clin. Oncol. 2013, 31, e28–e30. [Google Scholar] [CrossRef] [Green Version]
- Serke, S.; van Lessen, A.; Hummel, M.; Szczepek, A.; Huhn, D.; Stein, H. Circulating cd4+ t lymphocytes with intracellular but no surface cd3 antigen in five of seven patients consecutively diagnosed with angioimmunoblastic t-cell lymphoma. Cytometry 2000, 42, 180–187. [Google Scholar] [CrossRef]
- Stacchini, A.; Demurtas, A.; Aliberti, S.; Francia di Celle, P.; Godio, L.; Palestro, G.; Novero, D. The usefulness of flow cytometric cd10 detection in the differential diagnosis of peripheral t-cell lymphomas. Am. J. Clin. Pathol. 2007, 128, 854–864. [Google Scholar] [CrossRef]
- Singh, A.; Schabath, R.; Ratei, R.; Stroux, A.; Klemke, C.D.; Nebe, T.; Florcken, A.; van Lessen, A.; Anagnostopoulos, I.; Dorken, B.; et al. Peripheral blood scd3(-) cd4(+) t cells: A useful diagnostic tool in angioimmunoblastic t cell lymphoma. Hematol. Oncol. 2014, 32, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Loghavi, S.; Wang, S.A.; Medeiros, L.J.; Jorgensen, J.L.; Li, X.; Xu-Monette, Z.Y.; Miranda, R.N.; Young, K.H. Immunophenotypic and diagnostic characterization of angioimmunoblastic t-cell lymphoma by advanced flow cytometric technology. Leuk. Lymphoma 2016, 57, 2804–2812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yabe, M.; Gao, Q.; Ozkaya, N.; Huet, S.; Lewis, N.; Pichardo, J.D.; Moskowitz, A.J.; Horwitz, S.M.; Dogan, A.; Roshal, M. Bright pd-1 expression by flow cytometry is a powerful tool for diagnosis and monitoring of angioimmunoblastic t-cell lymphoma. Blood Cancer J. 2020, 10, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintanilla-Martinez, L.; Fend, F.; Moguel, L.R.; Spilove, L.; Beaty, M.W.; Kingma, D.W.; Raffeld, M.; Jaffe, E.S. Peripheral t-cell lymphoma with reed-sternberg-like cells of b-cell phenotype and genotype associated with epstein-barr virus infection. Am. J. Surg. Pathol. 1999, 23, 1233–1240. [Google Scholar] [CrossRef]
- Hartmann, S.; Goncharova, O.; Portyanko, A.; Sabattini, E.; Meinel, J.; Kuppers, R.; Agostinelli, C.; Pileri, S.A.; Hansmann, M.L. Cd30 expression in neoplastic t cells of follicular t cell lymphoma is a helpful diagnostic tool in the differential diagnosis of hodgkin lymphoma. Mod. Pathol. 2019, 32, 37–47. [Google Scholar] [CrossRef]
- Van den Oord, J.J.; de Wolf-Peeters, C.; O’Connor, N.T.; de Vos, R.; Tricot, G.; Desmet, V.J. Nodular t-cell lymphoma. Report of a case studied with morphologic, immunohistochemical, and DNA hybridization techniques. Arch. Pathol. Lab. Med. 1988, 112, 133–138. [Google Scholar]
- Hu, S.; Young, K.H.; Konoplev, S.N.; Medeiros, L.J. Follicular t-cell lymphoma: A member of an emerging family of follicular helper t-cell derived t-cell lymphomas. Hum. Pathol. 2012, 43, 1789–1798. [Google Scholar] [CrossRef]
- Sakakibara, A.; Suzuki, Y.; Kato, H.; Yamamoto, K.; Sakata-Yanagimoto, M.; Ishikawa, Y.; Furukawa, K.; Shimada, K.; Kohno, K.; Nakamura, S.; et al. Follicular t-cell lymphoma mimicking lymphocyte-rich classic hodgkin lymphoma: A case report of a diagnostic pitfall. J. Clin. Exp. Hematop. JCEH 2021, 61, 97–101. [Google Scholar] [CrossRef]
- Moroch, J.; Copie-Bergman, C.; de Leval, L.; Plonquet, A.; Martin-Garcia, N.; Delfau-Larue, M.H.; Molinier-Frenkel, V.; Belhadj, K.; Haioun, C.; Audouin, J.; et al. Follicular peripheral t-cell lymphoma expands the spectrum of classical hodgkin lymphoma mimics. Am. J. Surg. Pathol. 2012, 36, 1636–1646. [Google Scholar] [CrossRef]
- Rodriguez, M.; Alonso-Alonso, R.; Tomas-Roca, L.; Rodriguez-Pinilla, S.M.; Manso-Alonso, R.; Cereceda, L.; Borregon, J.; Villaescusa, T.; Cordoba, R.; Sanchez-Beato, M.; et al. Peripheral t-cell lymphoma: Molecular profiling recognizes subclasses and identifies prognostic markers. Blood Adv. 2021, 5, 5588–5598. [Google Scholar] [CrossRef]
- Manso, R.; Gonzalez-Rincon, J.; Rodriguez-Justo, M.; Roncador, G.; Gomez, S.; Sanchez-Beato, M.; Piris, M.A.; Rodriguez-Pinilla, S.M. Overlap at the molecular and immunohistochemical levels between angioimmunoblastic t-cell lymphoma and a subgroup of peripheral t-cell lymphomas without specific morphological features. Oncotarget 2018, 9, 16124–16133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostinelli, C.; Hartmann, S.; Klapper, W.; Korkolopoulou, P.; Righi, S.; Marafioti, T.; Piccaluga, P.P.; Patsouris, E.; Hansmann, M.L.; Lennert, K.; et al. Peripheral t cell lymphomas with follicular t helper phenotype: A new basket or a distinct entity? Revising karl lennert’s personal archive. Histopathology 2011, 59, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Attygalle, A.D. Nodal t-cell lymphomas with a t-follicular helper cell phenotype. Diagn. Histopathol. 2018, 24, 227–236. [Google Scholar] [CrossRef]
- Cairns, R.A.; Iqbal, J.; Lemonnier, F.; Kucuk, C.; de Leval, L.; Jais, J.P.; Parrens, M.; Martin, A.; Xerri, L.; Brousset, P.; et al. Idh2 mutations are frequent in angioimmunoblastic t-cell lymphoma. Blood 2012, 119, 1901–1903. [Google Scholar] [CrossRef] [Green Version]
- Heavican, T.B.; Bouska, A.; Yu, J.; Lone, W.; Amador, C.; Gong, Q.; Zhang, W.; Li, Y.; Dave, B.J.; Nairismagi, M.L.; et al. Genetic drivers of oncogenic pathways in molecular subgroups of peripheral t-cell lymphoma. Blood 2019, 133, 1664–1676. [Google Scholar] [CrossRef] [Green Version]
- Lemonnier, F.; Couronne, L.; Parrens, M.; Jais, J.P.; Travert, M.; Lamant, L.; Tournillac, O.; Rousset, T.; Fabiani, B.; Cairns, R.A.; et al. Recurrent tet2 mutations in peripheral t-cell lymphomas correlate with tfh-like features and adverse clinical parameters. Blood 2012, 120, 1466–1469. [Google Scholar] [CrossRef] [Green Version]
- Sakata-Yanagimoto, M.; Enami, T.; Yoshida, K.; Shiraishi, Y.; Ishii, R.; Miyake, Y.; Muto, H.; Tsuyama, N.; Sato-Otsubo, A.; Okuno, Y.; et al. Somatic rhoa mutation in angioimmunoblastic t cell lymphoma. Nat. Genet. 2014, 46, 171–175. [Google Scholar] [CrossRef]
- Yoon, S.E.; Cho, J.; Kim, Y.J.; Ko, Y.H.; Park, W.Y.; Kim, S.J.; Kim, W.S. Comprehensive analysis of clinical, pathological, and genomic characteristics of follicular helper t-cell derived lymphomas. Exp. Hematol. Oncol. 2021, 10, 33. [Google Scholar] [CrossRef]
- Ondrejka, S.L.; Grzywacz, B.; Bodo, J.; Makishima, H.; Polprasert, C.; Said, J.W.; Przychodzen, B.; Maciejewski, J.P.; Hsi, E.D. Angioimmunoblastic t-cell lymphomas with the rhoa p.Gly17val mutation have classic clinical and pathologic features. Am. J. Surg. Pathol. 2016, 40, 335–341. [Google Scholar] [CrossRef]
- Steinhilber, J.; Mederake, M.; Bonzheim, I.; Serinsoz-Linke, E.; Muller, I.; Fallier-Becker, P.; Lemonnier, F.; Gaulard, P.; Fend, F.; Quintanilla-Martinez, L. The pathological features of angioimmunoblastic t-cell lymphomas with idh2(r172) mutations. Mod. Pathol. 2019, 32, 1123–1134. [Google Scholar] [CrossRef]
- Attygalle, A.D.; Feldman, A.L.; Dogan, A. Itk/syk translocation in angioimmunoblastic t-cell lymphoma. Am. J. Surg. Pathol. 2013, 37, 1456–1457. [Google Scholar] [CrossRef] [PubMed]
- Streubel, B.; Vinatzer, U.; Willheim, M.; Raderer, M.; Chott, A. Novel t(5;9)(q33;q22) fuses itk to syk in unspecified peripheral t-cell lymphoma. Leukemia 2006, 20, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Genovese, G.; Kahler, A.K.; Handsaker, R.E.; Lindberg, J.; Rose, S.A.; Bakhoum, S.F.; Chambert, K.; Mick, E.; Neale, B.M.; Fromer, M.; et al. Clonal hematopoiesis and blood-cancer risk inferred from blood DNA sequence. N. Engl. J. Med. 2014, 371, 2477–2487. [Google Scholar] [CrossRef] [Green Version]
- Jaiswal, S.; Fontanillas, P.; Flannick, J.; Manning, A.; Grauman, P.V.; Mar, B.G.; Lindsley, R.C.; Mermel, C.H.; Burtt, N.; Chavez, A.; et al. Age-related clonal hematopoiesis associated with adverse outcomes. N. Engl. J. Med. 2014, 371, 2488–2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Wahab, O.; Mullally, A.; Hedvat, C.; Garcia-Manero, G.; Patel, J.; Wadleigh, M.; Malinge, S.; Yao, J.; Kilpivaara, O.; Bhat, R.; et al. Genetic characterization of tet1, tet2, and tet3 alterations in myeloid malignancies. Blood 2009, 114, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Ley, T.J.; Ding, L.; Walter, M.J.; McLellan, M.D.; Lamprecht, T.; Larson, D.E.; Kandoth, C.; Payton, J.E.; Baty, J.; Welch, J.; et al. Dnmt3a mutations in acute myeloid leukemia. N. Engl. J. Med. 2010, 363, 2424–2433. [Google Scholar] [CrossRef] [Green Version]
- Papaemmanuil, E.; Gerstung, M.; Malcovati, L.; Tauro, S.; Gundem, G.; Van Loo, P.; Yoon, C.J.; Ellis, P.; Wedge, D.C.; Pellagatti, A.; et al. Clinical and biological implications of driver mutations in myelodysplastic syndromes. Blood 2013, 122, 3616–3627; quiz 3699. [Google Scholar] [CrossRef]
- Yao, W.Q.; Wu, F.; Zhang, W.; Chuang, S.S.; Thompson, J.S.; Chen, Z.; Zhang, S.W.; Clipson, A.; Wang, M.; Liu, H.; et al. Angioimmunoblastic t-cell lymphoma contains multiple clonal t-cell populations derived from a common tet2 mutant progenitor cell. J. Pathol. 2020, 250, 346–357. [Google Scholar] [CrossRef] [Green Version]
- Tiacci, E.; Venanzi, A.; Ascani, S.; Marra, A.; Cardinali, V.; Martino, G.; Codoni, V.; Schiavoni, G.; Martelli, M.P.; Falini, B. High-risk clonal hematopoiesis as the origin of aitl and npm1-mutated aml. N. Engl. J. Med. 2018, 379, 981–984. [Google Scholar] [CrossRef]
- Lewis, N.E.; Petrova-Drus, K.; Huet, S.; Epstein-Peterson, Z.D.; Gao, Q.; Sigler, A.E.; Baik, J.; Ozkaya, N.; Moskowitz, A.J.; Kumar, A.; et al. Clonal hematopoiesis in angioimmunoblastic t-cell lymphoma with divergent evolution to myeloid neoplasms. Blood Adv. 2020, 4, 2261–2271. [Google Scholar] [CrossRef]
- Cheng, S.; Zhang, W.; Inghirami, G.; Tam, W. Mutation analysis links angioimmunoblastic t-cell lymphoma to clonal hematopoiesis and smoking. Elife 2021, 10, e66395. [Google Scholar] [CrossRef] [PubMed]
- Mulvey, E.; Ruan, J. Biomarker-driven management strategies for peripheral t cell lymphoma. J. Hematol. Oncol. 2020, 13, 59. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, S.; O’Connor, O.A.; Pro, B.; Illidge, T.; Fanale, M.; Advani, R.; Bartlett, N.L.; Christensen, J.H.; Morschhauser, F.; Domingo-Domenech, E.; et al. Brentuximab vedotin with chemotherapy for cd30-positive peripheral t-cell lymphoma (echelon-2): A global, double-blind, randomised, phase 3 trial. Lancet 2019, 393, 229–240. [Google Scholar] [CrossRef] [Green Version]
- Bachy, E.; Camus, V.; Thieblemont, C.; Sibon, D.; Casasnovas, R.O.; Ysebaert, L.; Damaj, G.; Guidez, S.; Pica, G.M.; Kim, W.S.; et al. Romidepsin plus chop versus chop in patients with previously untreated peripheral t-cell lymphoma: Results of the ro-chop phase iii study (conducted by lysa). J. Clin. Oncol. 2022, 40, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Ghione, P.; Faruque, P.; Mehta-Shah, N.; Seshan, V.; Ozkaya, N.; Bhaskar, S.; Yeung, J.; Spinner, M.A.; Lunning, M.; Inghirami, G.; et al. T follicular helper phenotype predicts response to histone deacetylase inhibitors in relapsed/refractory peripheral t-cell lymphoma. Blood Adv. 2020, 4, 4640–4647. [Google Scholar] [CrossRef]
- Ma, H.; O’Connor, O.A.; Marchi, E. New directions in treating peripheral t-cell lymphomas (ptcl): Leveraging epigenetic modifiers alone and in combination. Expert Rev. Hematol. 2019, 12, 137–146. [Google Scholar] [CrossRef]
- Ma, H.; O’Connor, O.A.; Marchi, E. Management of angioimmunoblastic t-cell lymphoma (aitl) and other t follicular helper cell lymphomas (tfh ptcl). Semin. Hematol. 2021, 58, 95–102. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Angioimmunoblastic T-Cell Lymphoma and Other Nodal Lymphomas of T Follicular Helper (TFH) Cell Origin |
|---|
| Angioimmunoblastic T-cell lymphoma |
| Follicular T-cell lymphoma |
| Nodal peripheral T-cell lymphoma with the TFH phenotype |
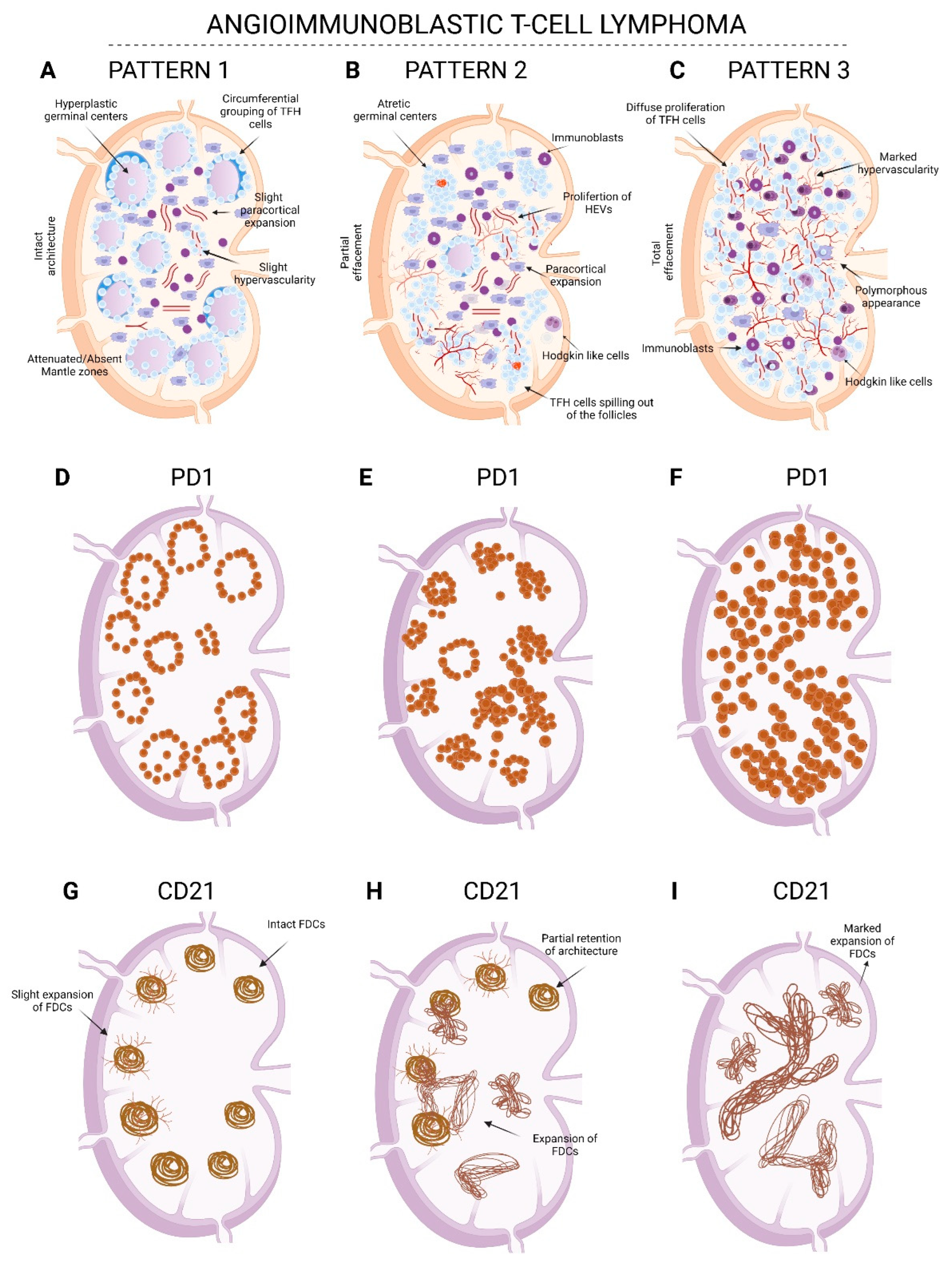
| Pattern 1 | Pattern 2 | Pattern 3 | |
|---|---|---|---|
| Architecture | Preserved | Partially effaced | Totally effaced |
| Follicles | Hyperplastic germinal centers Absent/attenuated mantle zones | Atretic/regressed Castleman-like follicles | Absent or occasional compressed follicles seen at the periphery (especially highlighted with a CD20 stain) |
| Paracortex | Focal areas of paracortical expansion and perifollicular polymorphous infiltrate focal slight increase in HEVs | Areas with polymorphous infiltration with immunoblasts and Hodgkin’s-like cells Proliferation of HEVs in the expanded areas | Marked polymorphous diffuse infiltration with immunoblasts and Hodgkin’s-like cells Marked proliferation of HEVs |
| TFH cell | Perifollicular with occasional paracortical clustering | Paracortical aggregates spilling out of follicles with grouping around HEVs | Diffuse proliferation of TFH cells with grouping around HEVs |
| FDC meshworks (CD21 or CD23 IHC) | Intact with slight branching out | Partially intact with areas demonstrating expansion and encircling of HEVs | Marked expansion with encircling around HEVs |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ganapathi, K.A.; Karner, K.H.; Menon, M.P. Peripheral T-Cell Lymphomas of the T Follicular Helper Type: Clinical, Pathological, and Genetic Attributes. Hemato 2022, 3, 268-286. https://doi.org/10.3390/hemato3010020
Ganapathi KA, Karner KH, Menon MP. Peripheral T-Cell Lymphomas of the T Follicular Helper Type: Clinical, Pathological, and Genetic Attributes. Hemato. 2022; 3(1):268-286. https://doi.org/10.3390/hemato3010020
Chicago/Turabian StyleGanapathi, Karthik A., Kristin H. Karner, and Madhu P. Menon. 2022. "Peripheral T-Cell Lymphomas of the T Follicular Helper Type: Clinical, Pathological, and Genetic Attributes" Hemato 3, no. 1: 268-286. https://doi.org/10.3390/hemato3010020