
Juvenile-Onset Non-Poikilodermatous CD8+CD56+ Mycosis Fungoides


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
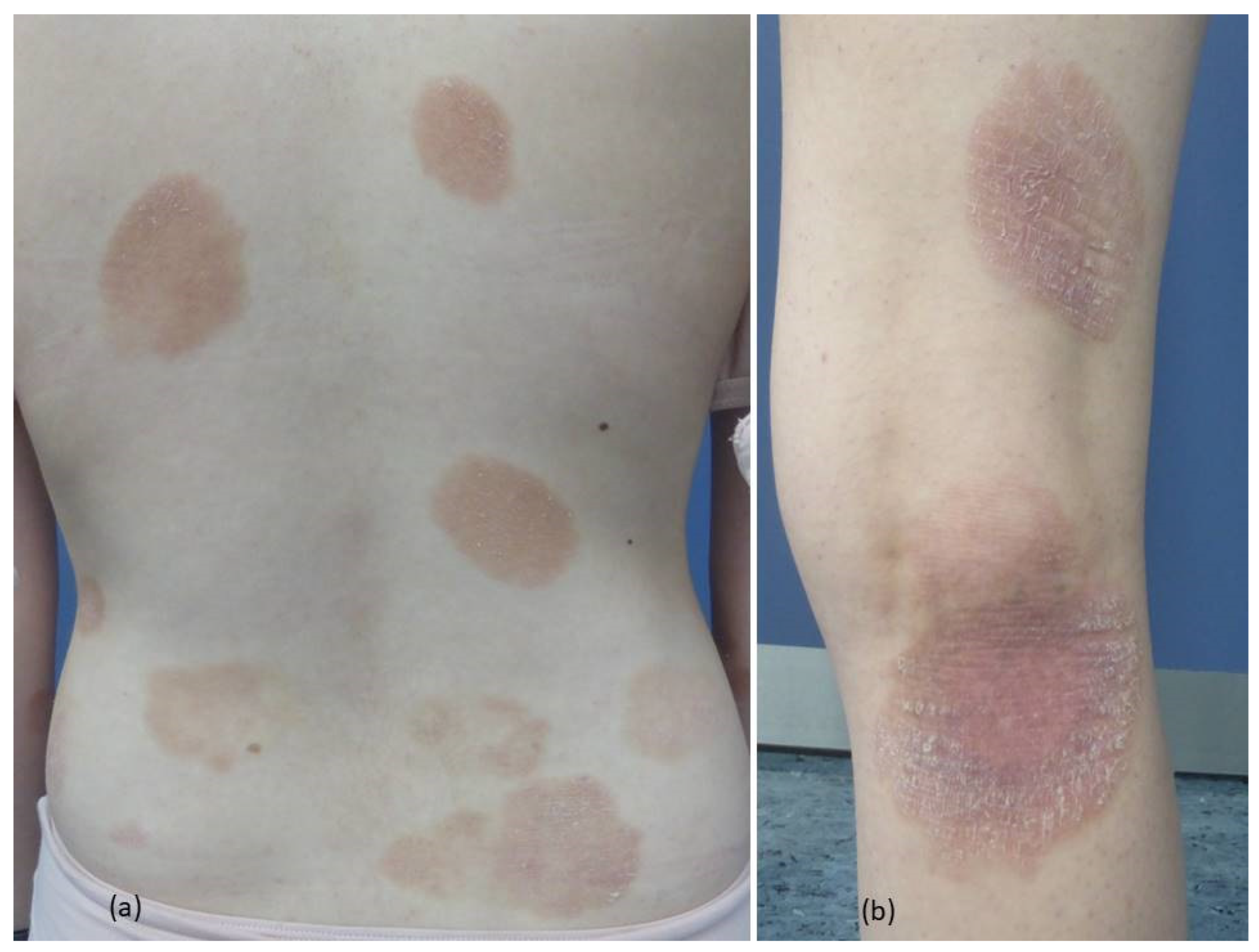
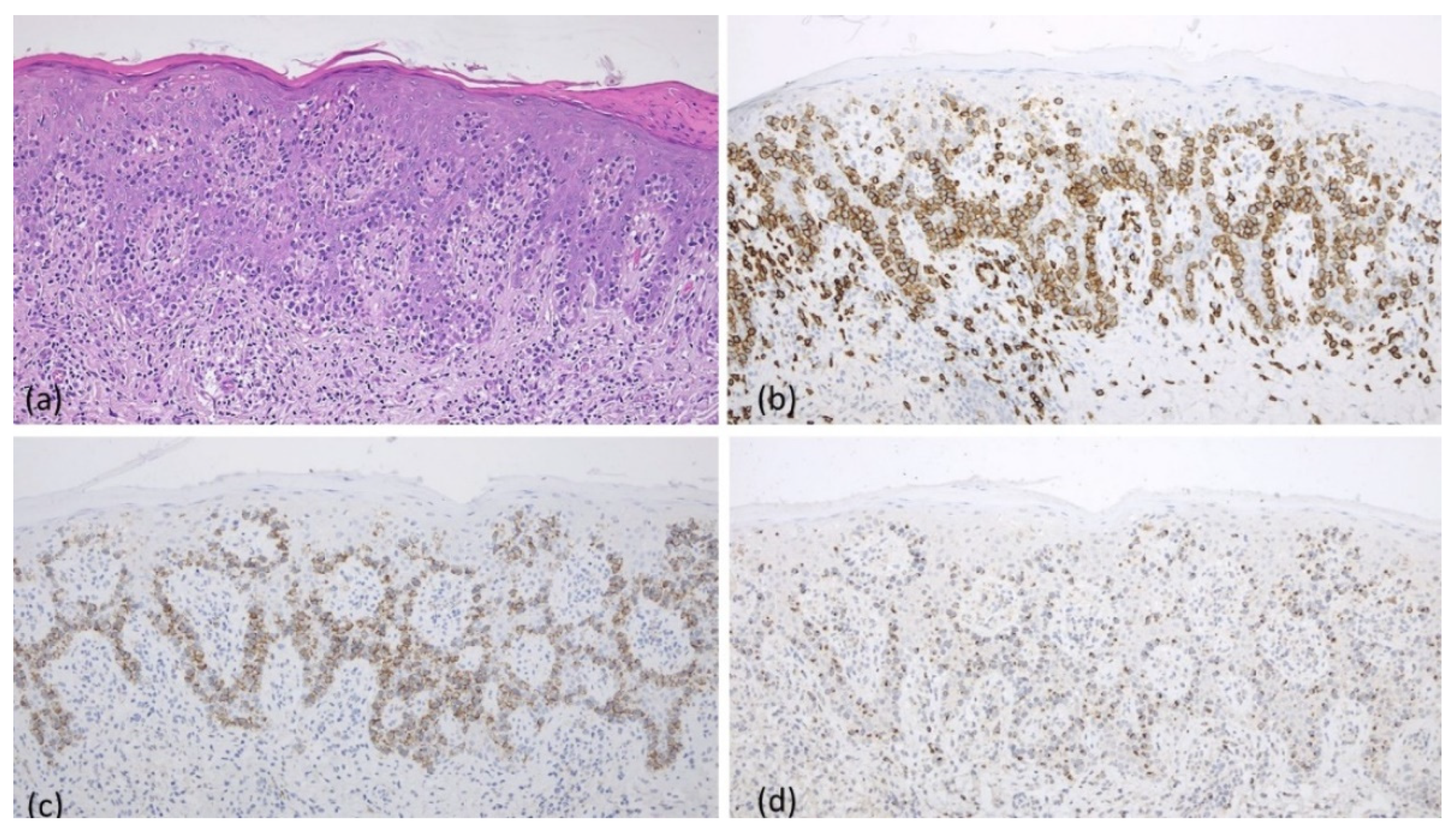
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wohlmuth-Wieser, I. Primary cutaneous T-cell lymphomas in childhood and adolescence. J. Dtsch. Dermatol. Ges. 2021, 19, 563–581. [Google Scholar] [CrossRef]
- Ben-Amitai, D.; Michael, D.; Feinmesser, M.; Hodak, E. Juvenile mycosis fungoides diagnosed before 18 years of age. Acta Derm. Venereol. 2003, 83, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Boulos, S.; Vaid, R.; Aladily, T.N.; Ivan, D.S.; Talpur, R.; Duvic, M. Clinical presentation, immunopathology, and treatment of juvenile-onset mycosis fungoides: A case series of 34 patients. J. Am. Acad. Dermatol. 2014, 71, 1117–1126. [Google Scholar] [CrossRef] [PubMed]
- Rovaris, M.; Colato, C.; Girolomoni, G. Pediatric CD8+/CD56+ mycosis fungoides with cytotoxic marker expression: A variant with indolent course. J. Cutan. Pathol. 2018, 45, 782–785. [Google Scholar] [CrossRef] [PubMed]
- Poppe, H.; Kerstan, A.; Böckers, M.; Goebeler, M.; Geissinger, E.; Rosenwald, A.; Hamm, H. Childhood mycosis fungoides with a CD8+ CD56+ cytotoxic immunophenotype. J. Cutan. Pathol. 2015, 42, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Santonja, C.; Sánchez-García, F.J.; Rodríguez-Rodríguez, R.N.; Manso, R.; Requena, L.; Gil-Mateo, M.D.P.; Rodríguez-Pinilla, S.M. Double CD4/CD8-Positive, Nonpoikilodermic Mycosis Fungoides Expressing CD56 in a Young Man. Am. J. Dermatopathol. 2022, 44, 936–939. [Google Scholar] [CrossRef] [PubMed]
- Kempf, W.; Kazakov, D.V.; Broekaert, S.M.; Metze, D. Pediatric CD8⁺CD56⁺ non-poikilodermatous mycosis fungoides: Case report and review of the literature. Am. J. Dermatopathol. 2014, 36, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Shiomi, T.; Monobe, Y.; Kuwabara, C.; Hayashi, H.; Yamamoto, T.; Sadahira, Y. Poikilodermatous mycosis fungoides with a CD8+ CD56+ immunophenotype: A case report and literature review. J. Cutan. Pathol. 2013, 40, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Park, M.Y.; Hwang, S.; Kim, J.; Almurayshid, A.I.; Yoon, S.O.; Oh, S.H. Rare case of CD8+ CD56+ cytotoxic variant of mycosis fungoides clinically presenting with a combination of hypopigmentation and poikiloderma. Int. J. Dermatol. 2020, 59, e374–e376. [Google Scholar] [CrossRef] [PubMed]
- Sawada, Y.; Sugita, K.; Kabashima, R.; Hino, R.; Nakamura, M.; Koga, C.; Tokura, Y. CD8+ CD56+ mycosis fungoides with an indolent clinical behaviour: Case report and literature review. Acta Derm. Venereol. 2010, 90, 525–526. [Google Scholar] [CrossRef] [PubMed]
- Menni, S.; Piccinno, R.; Crosti, L.; Berti, E. Parapsoriasis in two children: A clinical, immunophenotypic, and immunogenotypic study. Pediatr. Dermatol. 1994, 11, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.M.; Lim, D.J.; Won, C.H.; Chang, S.E.; Lee, M.W.; Lee, W.J. Mycosis Fungoides in Children and Adolescents: A Systematic Review. JAMA Dermatol. 2021, 157, 431–438. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gambichler, T.; Thiele, A.; Merz, H.; Susok, L.; Boms, S. Juvenile-Onset Non-Poikilodermatous CD8+CD56+ Mycosis Fungoides. Dermato 2024, 4, 1-4. https://doi.org/10.3390/dermato4010001
Gambichler T, Thiele A, Merz H, Susok L, Boms S. Juvenile-Onset Non-Poikilodermatous CD8+CD56+ Mycosis Fungoides. Dermato. 2024; 4(1):1-4. https://doi.org/10.3390/dermato4010001
Chicago/Turabian StyleGambichler, Thilo, Andrea Thiele, Hartmut Merz, Laura Susok, and Stefanie Boms. 2024. "Juvenile-Onset Non-Poikilodermatous CD8+CD56+ Mycosis Fungoides" Dermato 4, no. 1: 1-4. https://doi.org/10.3390/dermato4010001