Dear Editors: In 2016, Bessis and coworkers first reported Bier anemic spots, cyanosis, and urticaria-like eruption (BASCULE) syndrome [
1]. It is a chronic vasomotor dermatosis mainly affecting the lower limbs. Here we report a finding of circulating autoantibodies in a young female with BASCULE syndrome (
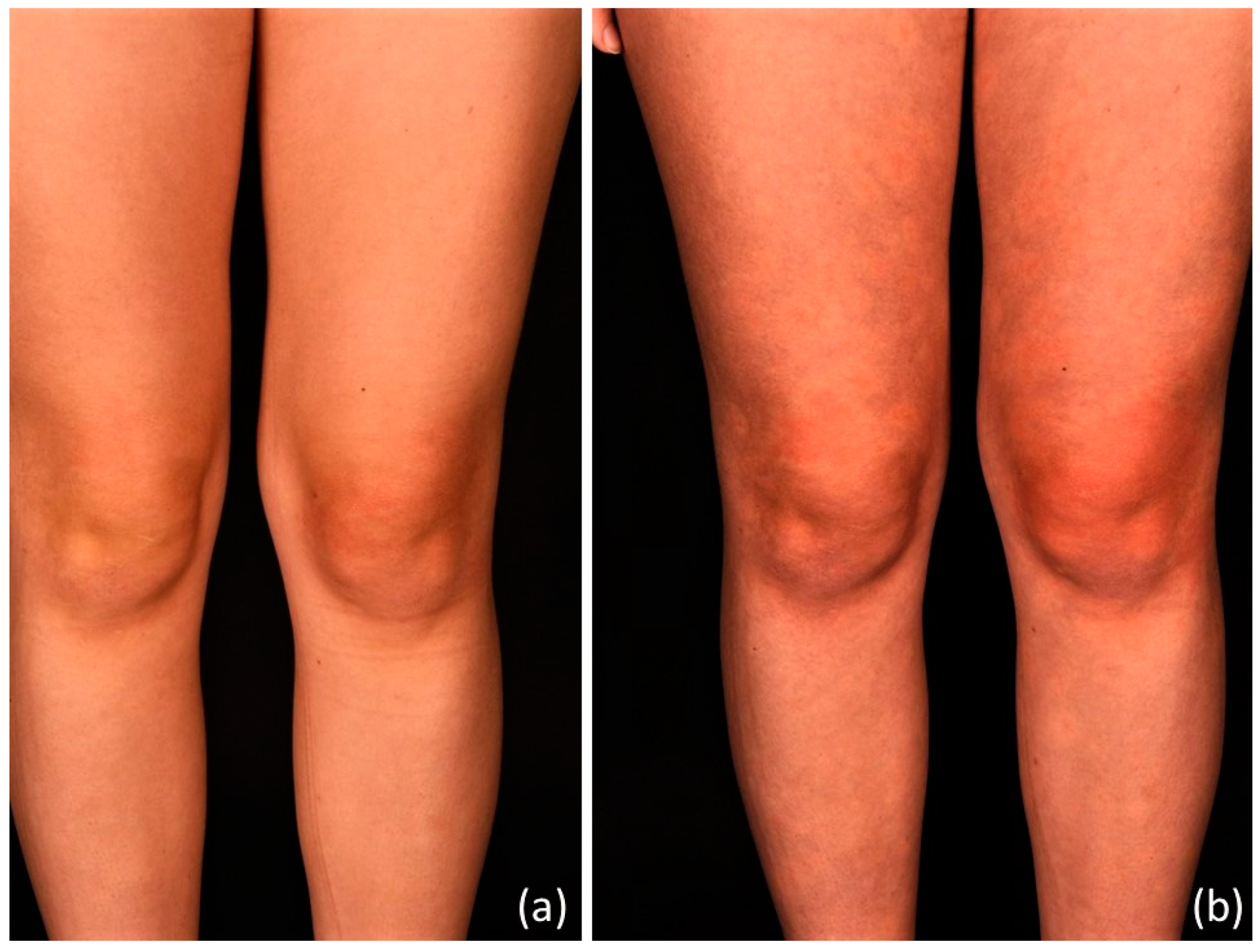
Figure 1).
An 18-year-old woman presented with a 6-month history of slightly itchy lesions on her lower limbs that always appeared while standing and resolved when sitting or lying down. No history of allergic conditions (e.g., atopic dermatitis, urticaria), recent infections, fever, Raynaud’s phenomenon, or arthralgia was established. On examination in supine position, her skin on both legs did not show any lesions. However, within a few minutes in standing position, she developed multiple anemic macules, in part with central erythema, slightly cyanotic macules, and urticarial plaques on both legs (
Figure 2).
A punch biopsy taken from an urticaria-like lesion revealed nonspecific lymphohistiocytic infiltrates surrounding the vessels of the upper dermis. Giemsa stain and CD117 immunohistochemistry did not show an increased number of mast cells, as would be characteristic for urticaria. The patient was referred to a cardiologist and neurologist in order to exclude postural orthostatic tachycardia syndrome (POTS) and other forms of orthostatic intolerance. Heart rate, blood pressure, electrocardiogram, and echocardiogram were normal. However, a Schellong test revealed mild orthostatic hypotension. Pilocarpine iontopheresis did not provoke skin lesions. Laboratory parameters such as complete blood count, liver enzymes, serum creatinine, diaminooxidase, serum tryptase, serum IgE, eosinophilic cationic protein, thyroid autoantibodies, and extractable nuclear antigen (ENA) antibodies were within the normal limits. However, indirect immunofluorescence detected elevated antinuclear antibodies (ANA, with a titer of 1:640, normal range < 1:80). In addition, anti-dense fine speckled 70 (DFS70) antibodies were also positive. Taken together, a diagnosis of BASCULE syndrome associated with elevated ANAs was made. Three months later, the ANA titer was increased at 1:1280 and anti-DFS70 antibodies were again detected. In contrast to a recent case report [
2], high-dose antihistamine medication (Bilastine, Fexofenadine) did not lead to significant improvements and neither did the wearing of compression stockings.
Since the first description by Bessis et al. [
1] 18 patients with BASCULE syndrome have been described [
3]. Clinically, postural urticarial represent a condition very similar to BASCULE [
4]. BASCULE syndrome is characterized by an impressive, easy-to-provoke pathology that can be associated with POTS and orthostatic dysregulation [
3]. Characteristically, cutaneous symptoms of BASCULE syndrome occur few minutes after assuming a standing position and disappear spontaneously when lying or sitting down. All reported patients with BASCULE syndrome were under 20 years old and to this date, abnormal laboratory test results including for autoantibodies have not been described [
1,
2,
3,
4]. El Nemmon et al. [
3], recently reported a 13-year-old boy with BASCULE syndrome and one-year history of Raynaud’s phenomenon without elevated ANA titer. It has been suggested that the transient skin lesions characteristic for BASCULE syndrome represent a benign vasomotor disorder, such as stasis-induced exaggerated vasoconstrictive responses of arterioles to tissue hypoxia, lack of venoarteriolar reflexes in dermal ascending arterioles, and/or paradoxical reactions to hypoxia.
In the present case, we observed a clearly elevated ANA titer with positive anti-DFS70 antibodies without clinical evidence for typically associated symptoms of systemic autoimmune rheumatic diseases (SARD). In adults with increased ANA titers, detection of anti-DFS70 antibodies may help to exclude SARDs, since these typically do not occur. In pediatric patients, however, anti-DFS70 antibodies can also be detected in rare cases of systemic sclerosis and systemic lupus erythematosus. Notably, these auto-antibodies have a remarkably high frequency in children with localized scleroderma, juvenile dermatomyositis, and uveitis [
5]. Moreover, anti-DFS70 antibodies are significantly associated with atopic dermatitis and may result in misdiagnosis of SARDs [
6]. However, whether the detection of circulating antibodies in a patient with BASCULE syndrome represents a mere coincidence or hints to an association remains, at present, unclear. Systematic screening for autoantibodies in patients with BASCULE syndrome may help to answer this question, thereby shedding lights.
Author Contributions
Conceptualization, T.G.; methodology, T.G.; investigation, T.G., M.B., R.S., C.H.S. and N.A.R.; writing—original draft preparation, T.G.; visualization, T.G., M.B. and N.A.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This case study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from the patient presented.
Data Availability Statement
Not applicable.
Conflicts of Interest
T.G. has received speakers and/or advisory board honoraria from BMS, Sanofi-Genzyme, MSD, Novartis Pharma, Roche, Abbvie, Almirall, Janssen, Lilly, Pfizer, Pierre Fabre, Merck-Serono, outside the submitted work. The other authors have no conflict of interest to declare.
References
- Bessis, D.; Jeziorski, É.; Rigau, V.; Pralong, P.; Pallure, V. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: A new entity? Br. J. Dermatol. 2016, 175, 218–220. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, L.; Dvorakova, V.; Browne, F.; Irvine, A.D. High-dose bilastine for the treatment of BASCULE syndrome. Clin. Exp. Dermatol. 2021, 46, 357–358. [Google Scholar] [CrossRef] [PubMed]
- El Nemnom, P.; Lauwerys, B.; Marot, L.; Tennstedt, D.; Dekeuleneer, V. Bier anemic spots, cyanosis, and urticaria-like eruption (BASCULE) syndrome: Report of two new cases and literature review. Pediatr. Dermatol. 2020, 37, 864–867. [Google Scholar] [CrossRef] [PubMed]
- Hirohata, A.; Yamaoka, T.; Hayashi, M.; Murota, H.; Tani, M.; Katayama, I. Unique case of postural cholinergic urticaria induced by a standing position. Clin. Exp. Dermatol. 2016, 41, 439–440. [Google Scholar] [CrossRef] [PubMed]
- Schmeling, H.; Mahler, M.; Levy, D.M.; Moore, K.; Stevens, A.M.; Wick, J.; McMillan, J.D.; Horneff, G.; Assassi, S.; Charles, J.; et al. Autoantibodies to Dense Fine Speckles in Pediatric Diseases and Controls. J. Rheumatol. 2015, 42, 2419–2426. [Google Scholar] [CrossRef]
- Santler B, Wimmer L, Schlueter B, Ehrchen J. Anti-DFS70 antibodies are associated with atopic dermatitis and can cause misdiagnosis of connective tissue disease. J. Dtsch. Dermatol. Ges. 2023, 21, 464–470. [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



{kind=link}
{kind=link}

