
DoseMRT: A Software Package for Individualised Monte Carlo Dose Calculations of Synchrotron-Generated Microbeam Radiation Therapy

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Simulation Configuration
2.1.1. Stage I: Synchrotron Radiation Production
2.1.2. Stage II: Dose Calculation
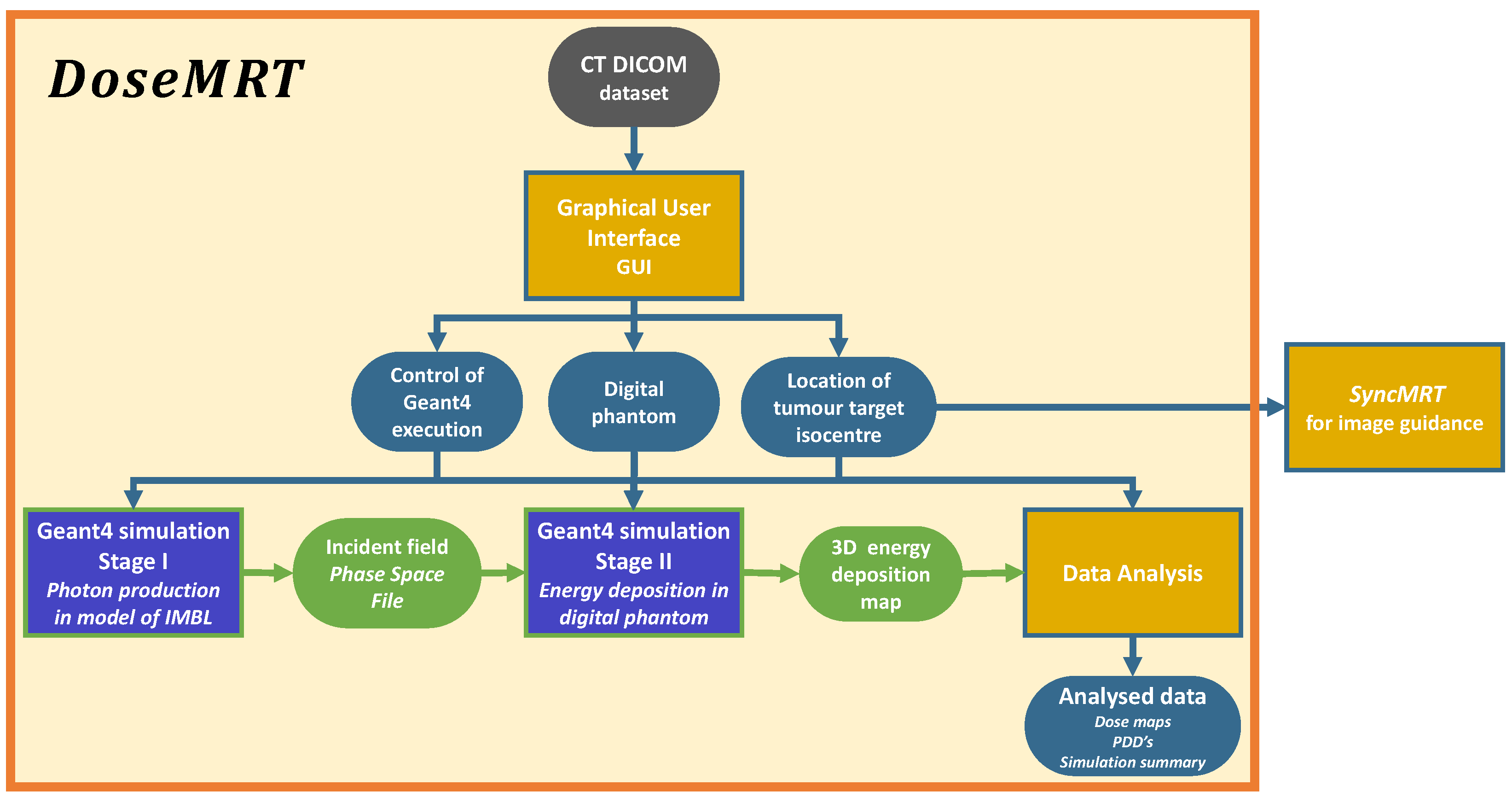
2.1.3. Graphical User Interface
- To implement the Geant4 simulation geometry based on the CT DICOM dataset.
- To select the treatment modality and treatment angle, identify the target isocentre from two orthogonal images, threshold all unique tissues, and apply treatment margins.
- Produce all files needed to execute the individual Geant4 dose calculation.
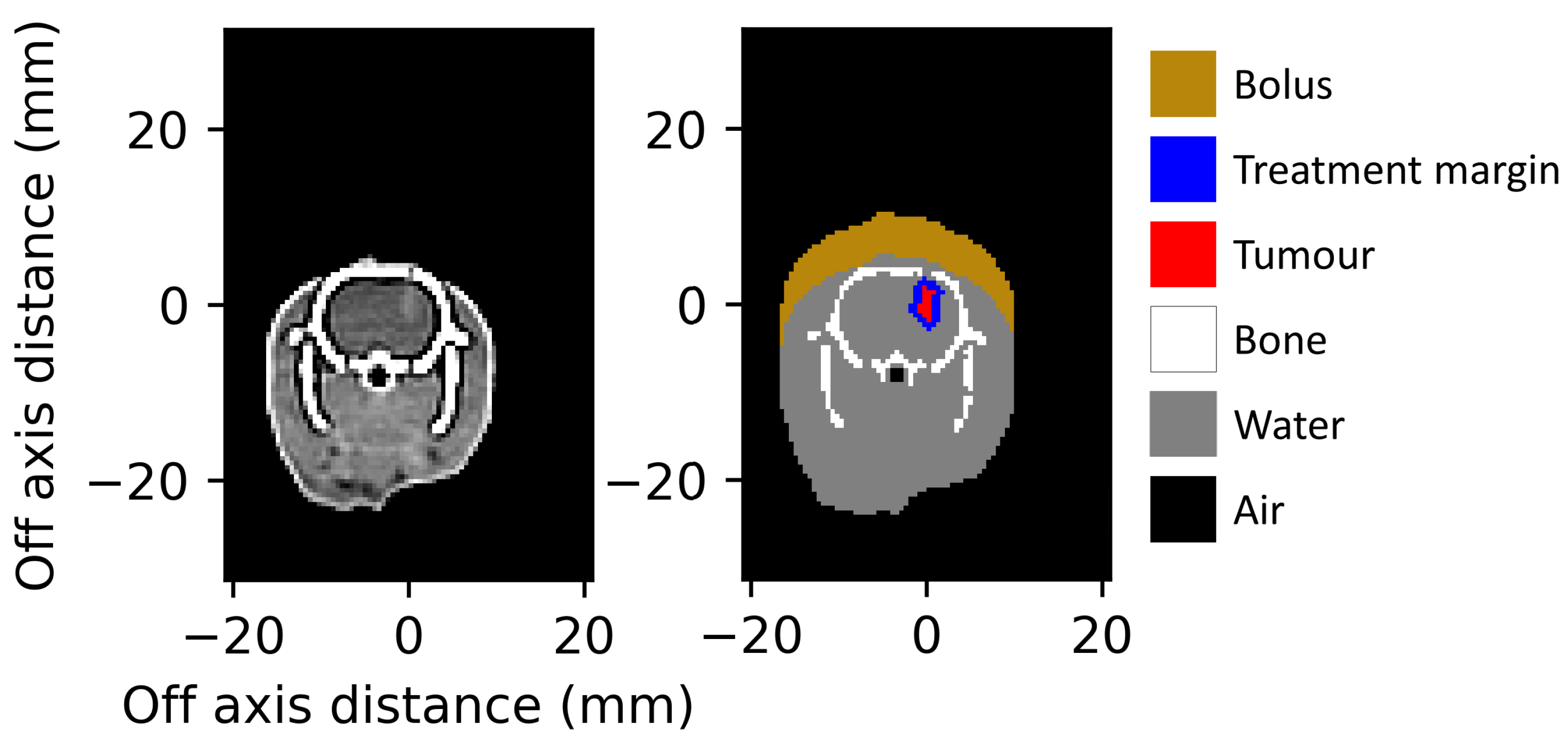
2.1.4. Tissue Segmentation
2.1.5. Alderson Radiation Therapy DICOM Conversion to Digital Phantoms
2.1.6. In Vivo Rat DICOM Conversion to Digital Phantoms
2.2. Experimental Dosimetry
2.2.1. Radiation Detectors
2.2.2. Phantom Dosimetry
2.3. In Vivo Animal Studies
2.3.1. Definition of Treatment Margin
2.3.2. Geant4 Dose Calculations
3. Results
3.1. Phantom Dosimetry
3.1.1. Validation of Broad Beam Geant4 Calculations in the Water Tank Phantom
3.1.2. Validation of Broad Beam Geant4 Calculations in the Alderson Radiation Therapy Phantom
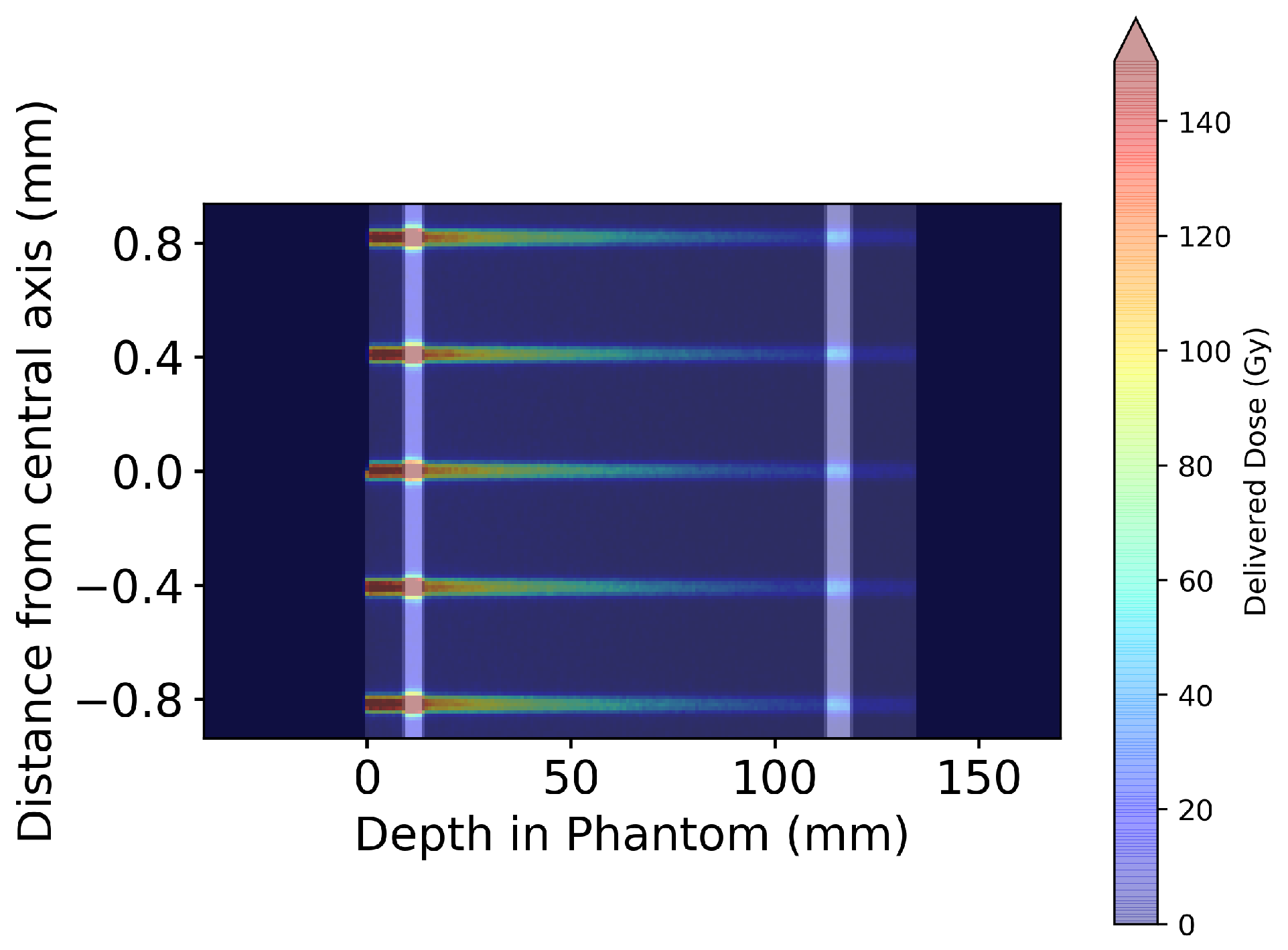
3.1.3. Validation of Microbeam Geant4 Calculations in the Alderson Radiation Therapy Phantom
3.2. In Vivo Treatment Simulations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Crosbie, J.C.; Anderson, R.L.; Rothkamm, K.; Restall, C.M.; Cann, L.; Ruwanpura, S.; Meachem, S.; Yagi, N.; Svalbe, I.; Lewis, R.A.; et al. Tumor Cell Response to Synchrotron Microbeam Radiation Therapy Differs Markedly From Cells in Normal Tissues. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, J.; Adam, J.F.; Crosbie, J.C.; Hall, C.J.; Lye, J.E.; McKinlay, J.; Pelliccia, D.; Pouzoulet, F.; Prezado, Y.; Stevenson, A.W.; et al. Preclinical radiotherapy at the Australian Synchrotron’s Imaging and Medical Beamline: Instrumentation, dosimetry and a small-animal feasibility study. J. Synchrotron Radiat. 2017, 24, 854–865. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.A.; Engels, E.; Petasecca, M.; Paino, J.; Tehei, M.; Corde, S.; Stevenson, A.; Hausermann, D.; Guatelli, S.; Rosenfeld, A.; et al. X-TREAM protocol for in vitro microbeam radiation therapy at the Australian Synchrotron. J. Appl. Phys. 2021, 129, 244902. [Google Scholar] [CrossRef]
- Poole, C.M.; Day, L.R.; Rogers, P.A.; Crosbie, J.C. Synchrotron microbeam radiotherapy in a commercially available treatment planning system. Biomed. Phys. Eng. Express 2017, 3, 025001. [Google Scholar] [CrossRef]
- Donzelli, M.; Bräuer-Krisch, E.; Oelfke, U.; Wilkens, J.J.; Bartzsch, S. Hybrid dose calculation: A dose calculation algorithm for microbeam radiation therapy. Phys. Med. Biol. 2018, 63, 045013. [Google Scholar] [CrossRef]
- Day, L.R.J.; Donzelli, M.; Pellicioli, P.; Smyth, L.M.; Barnes, M.; Bartzsch, S.; Crosbie, J.C. A commercial treatment planning system with a hybrid dose calculation algorithm for synchrotron radiotherapy trials. Phys. Med. Biol. 2021, 66, 055016. [Google Scholar] [CrossRef]
- Debus, C.; Oelfke, U.; Bartzsch, S. A point kernel algorithm for microbeam radiation therapy. Phys. Med. Biol. 2017, 62, 8341. [Google Scholar] [CrossRef] [Green Version]
- Kraus, K.M.; Winter, J.; Zhang, Y.; Ahmed, M.; Combs, S.E.; Wilkens, J.J.; Bartzsch, S. Treatment planning study for microbeam radiotherapy using clinical patient data. Cancers 2022, 14, 685. [Google Scholar] [CrossRef]
- Martínez-Rovira, I.; Sempau, J.; Prezado, Y. Monte Carlo-based treatment planning system calculation engine for microbeam radiation therapy. Med. Phys. 2012, 39, 2829–2838. [Google Scholar] [CrossRef]
- Keshmiri, S.; Brocard, S.; Serduc, R.; Adam, J.F. A high-resolution dose calculation engine for X-ray microbeams radiation therapy. Med. Phys. 2022, 49, 3999–4017. [Google Scholar] [CrossRef]
- Agostinelli, S.; Allison, J.; Amako, K.a.; Apostolakis, J.; Araujo, H.; Arce, P.; Asai, M.; Axen, D.; Banerjee, S.; Barrand, G.; et al. GEANT4—A simulation toolkit. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrom. Detect. Assoc. Equip. 2003, 506, 250–303. [Google Scholar] [CrossRef] [Green Version]
- Allison, J.; Amako, K.; Apostolakis, J.; Araujo, H.; Dubois, P.A.; Asai, M.; Barrand, G.; Capra, R.; Chauvie, S.; Chytracek, R.; et al. Geant4 developments and applications. IEEE Trans. Nucl. Sci. 2006, 53, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Allison, J.; Amako, K.; Apostolakis, J.; Arce, P.; Asai, M.; Aso, T.; Bagli, E.; Bagulya, A.; Banerjee, S.; Barrand, G.; et al. Recent developments in Geant4. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrom. Detect. Assoc. Equip. 2016, 835, 186–225. [Google Scholar] [CrossRef]
- Dipuglia, A.; Cameron, M.; Davis, J.A.; Cornelius, I.M.; Stevenson, A.W.; Rosenfeld, A.B.; Petasecca, M.; Corde, S.; Guatelli, S.; Lerch, M.L.F. Validation of a Monte Carlo simulation for Microbeam Radiation Therapy on the Imaging and Medical Beamline at the Australian Synchrotron. Sci. Rep. 2019, 9, 17696. [Google Scholar] [CrossRef] [Green Version]
- Large, M.; Malaroda, A.; Petasecca, M.; Rosenfeld, A.; Guatelli, S. Modelling ICRP110 adult reference voxel phantoms for dosimetric applications: Development of a new Geant4 advanced example. In Proceedings of the Journal of Physics: Conference Series; IOP Publishing: Bristol, UK, 2020; Volume 1662, p. 012021. [Google Scholar]
- Paino, J.; Barnes, M.; Engels, E.; Davis, J.; Guatelli, S.; de Veer, M.; Hall, C.; Häusermann, D.; Tehei, M.; Corde, S.; et al. Incorporating clinical imaging into the delivery of microbeam radiation therapy. Appl. Sci. 2021, 11, 9101. [Google Scholar] [CrossRef]
- Barnes, M.; Paino, J.; Day, L.; Butler, D.; Häusermann, D.; Pelliccia, D.; Crosbie, J. SyncMRT: A solution to image-guided synchrotron radiotherapy for quality assurance and pre-clinical trials. J. Synchrotron Radiat. 2022, 29, 1074–1084. [Google Scholar] [CrossRef]
- Geant4 Collaboration. Geant4, version 10.4; Physics Reference Manual; Geant4 Collaboration, 2020; Volume 9. [Google Scholar]
- Engels, E.; Li, N.; Davis, J.; Paino, J.; Cameron, M.; Dipuglia, A.; Vogel, S.; Valceski, M.; Khochaiche, A.; O’Keefe, A.; et al. Toward personalized synchrotron microbeam radiation therapy. Sci. Rep. 2020, 10, 8833. [Google Scholar] [CrossRef]
- Livingstone, J.; Stevenson, A.W.; Butler, D.J.; Häusermann, D.; Adam, J.F. Characterization of a synthetic single crystal diamond detector for dosimetry in spatially fractionated synchrotron X-ray fields. Med. Phys. 2016, 43, 4283–4293. [Google Scholar] [CrossRef]
- Stevenson, A.W.; Crosbie, J.C.; Hall, C.J.; Livingstone, J.; Lye, J.E. Quantitative characterisation of the X-ray beam at the Australian Synchrotron Imaging and Medical Beamline (IMBL). J. Synchrotron Radiat. 2016, 24, 110–141. [Google Scholar] [CrossRef]
- Van Rossum, G.; Drake, F.L. Python 3 Reference Manual; CreateSpace: Scotts Valley, CA, USA, 2009. [Google Scholar]
- ICRP. Adult Reference Computational Phantoms; ICRP Publication 110, Annals of ICRP; ICRP: Amsterdam, The Netherlands, 2009; Volume 39, p. 1. [Google Scholar]
- Geant4 Collaboration. Book for Application Developers; Geant4 Collaboration, 2019; Volume 10, pp. 5–12. Available online: http://geant4-userdoc.web.cern.ch/geant4-userdoc/UsersGuides/ForApplicationDeveloper/BackupVersions (accessed on 1 February 2023).
- Pal, N.R.; Pal, S.K. A review on image segmentation techniques. Pattern Recognit. 1993, 26, 1277–1294. [Google Scholar] [CrossRef]
- IAEA. Absorbed Dose Determination in External Beam Radiotherapy: An International Code of Practice for Dosimetry Based on Standards of Absorbed Dose to Water; Technical Report Series No. 398; Vienna International Atomic Energy Agency: Vienna, Austria, 2000. [Google Scholar]
- Patallo, I.S.; Carter, R.; Maughan, D.; Nisbet, A.; Schettino, G.; Subiel, A. Evaluation of a micro ionization chamber for dosimetric measurements in image-guided preclinical irradiation platforms. Phys. Med. Biol. 2021, 66, 245012. [Google Scholar] [CrossRef] [PubMed]
- Andreo, P.; Huq, M.S.; Westermark, M.; Song, H.; Tilikidis, A.; DeWerd, L.; Shortt, K. Protocols for the dosimetry of high-energy photon and electron beams: A comparison of the IAEA TRS-398 and previous international Codes of Practice. Phys. Med. Biol. 2002, 47, 3033. [Google Scholar] [CrossRef]
- Fournier, P.; Crosbie, J.C.; Cornelius, I.; Berkvens, P.; Donzelli, M.; Clavel, A.H.; Rosenfeld, A.B.; Petasecca, M.; Lerch, M.L.F.; Bräuer-Krisch, E. Absorbed dose-to-water protocol applied to synchrotron-generated x-rays at very high dose rates. Phys. Med. Biol. 2016, 61, N349–N361. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.; Petasecca, M.; Cullen, A.; Paino, J.; Archer, J.; Rosenfeld, A.; Lerch, M. X-Tream dosimetry of synchrotron radiation with the PTW microDiamond. J. Instrum. 2019, 14, 10037. [Google Scholar] [CrossRef]
- Livingstone, J.; Stevenson, A.W.; Häusermann, D.; Adam, J.F. Experimental optimisation of the X-ray energy in microbeam radiation therapy. Phys. Med. 2018, 45, 156–161. [Google Scholar] [CrossRef] [Green Version]
- Vinogradov, A.; Zorev, N.; Kozhevnikov, I.; Yakushkin, I. Phenomenon of total external reflection of x rays. Zh. Eksp. Teor. Fiz. 1985, 89, 2124–2132. [Google Scholar]
- Fournier, P.; Cornelius, I.; Donzelli, M.; Requardt, H.; Nemoz, C.; Petasecca, M.; Bräuer-Krisch, E.; Rosenfeld, A.; Lerch, M. X-Tream quality assurance in synchrotron X-ray microbeam radiation therapy. J. Synchrotron Radiat. 2016, 23, 1180–1190. [Google Scholar] [CrossRef] [Green Version]
- Butler, D.J.; Beveridge, T.; Lehmann, J.; Oliver, C.P.; Stevenson, A.W.; Livingstone, J. Spatial response of synthetic microDiamond and diode detectors measured with kilovoltage synchrotron radiation. Med. Phys. 2018, 45, 943–952. [Google Scholar] [CrossRef] [Green Version]
- Butson, M.J.; Cheung, T.; Peter, K. Weak energy dependence of EBT gafchromic film dose response in the 50 kVp–10 MVp X-ray range. Appl. Radiat. Isot. 2006, 64, 60–62. [Google Scholar] [CrossRef]
- Rink, A.; Vitkin, I.A.; Jaffray, D.A. Energy dependence (to) of radiochromic films assessed using a real-time optical dosimeter. Med. Phys. 2007, 34, 458–463. [Google Scholar] [CrossRef]
- Mentzel, F.; Paino, J.; Barnes, M.; Cameron, M.; Corde, S.; Engels, E.; Kröninger, K.; Lerch, M.; Nackenhorst, O.; Rosenfeld, A.; et al. Accurate and fast deep learning dose prediction for a preclinical microbeam radiation therapy study using low-statistics Monte Carlo simulations. arXiv 2022, arXiv:2212.05659. [Google Scholar] [CrossRef]
- Mentzel, F.; Barnes, M.; Kröninger, K.; Lerch, M.; Nackenhorst, O.; Paino, J.; Rosenfeld, A.; Saraswati, A.; Tsoi, A.C.; Weingarten, J.; et al. A step towards treatment planning for microbeam radiation therapy: Fast peak and valley dose predictions with 3D U-Nets. arXiv 2022, arXiv:2211.11193. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section 3 | Simulation Histories | Phantom Voxels | Scoring Voxels | RAM Usage | CPU Hours | Real Time |
|---|---|---|---|---|---|---|
| Section 3.1.2, BB Phantom | 60 × 10 6 | 7.5 × 10 6 | 7.5 × 10 6 | 650 MB | 2 h | 6 min |
| Section 3.1.3, MB Phantom | 7.5 × 10 9 | 7.5 × 10 6 | 1.1 × 10 6 | 610 MB | 50 h | 7 min |
| Section 3.2, MB in vivo | 750 × 10 6 | 2.5 × 10 6 | 0.7 × 10 6 | 550 MB | 13 h | 6 min |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paino, J.; Cameron, M.; Large, M.; Barnes, M.; Engels, E.; Vogel, S.; Tehei, M.; Corde, S.; Guatelli, S.; Rosenfeld, A.; et al. DoseMRT: A Software Package for Individualised Monte Carlo Dose Calculations of Synchrotron-Generated Microbeam Radiation Therapy. Radiation 2023, 3, 123-137. https://doi.org/10.3390/radiation3020011
Paino J, Cameron M, Large M, Barnes M, Engels E, Vogel S, Tehei M, Corde S, Guatelli S, Rosenfeld A, et al. DoseMRT: A Software Package for Individualised Monte Carlo Dose Calculations of Synchrotron-Generated Microbeam Radiation Therapy. Radiation. 2023; 3(2):123-137. https://doi.org/10.3390/radiation3020011
Chicago/Turabian StylePaino, Jason, Matthew Cameron, Matthew Large, Micah Barnes, Elette Engels, Sarah Vogel, Moeava Tehei, Stéphanie Corde, Susanna Guatelli, Anatoly Rosenfeld, and et al. 2023. "DoseMRT: A Software Package for Individualised Monte Carlo Dose Calculations of Synchrotron-Generated Microbeam Radiation Therapy" Radiation 3, no. 2: 123-137. https://doi.org/10.3390/radiation3020011