Author Contributions
Conceptualization, E.S. and A.R.B.; Data curation, A.L., E.S. and A.R.B.; Formal analysis, A.L. and E.S.; Investigation, A.L., E.S. and A.R.B.; Methodology, E.S. and A.R.B.; Project administration, A.L., E.S. and A.R.B.; Supervision, E.S. and A.R.B.; Validation, A.L., E.S. and A.R.B.; Writing—original draft, A.L.; Writing—review and editing, A.L., E.S. and A.R.B. All authors have read and agreed to the published version of the manuscript.
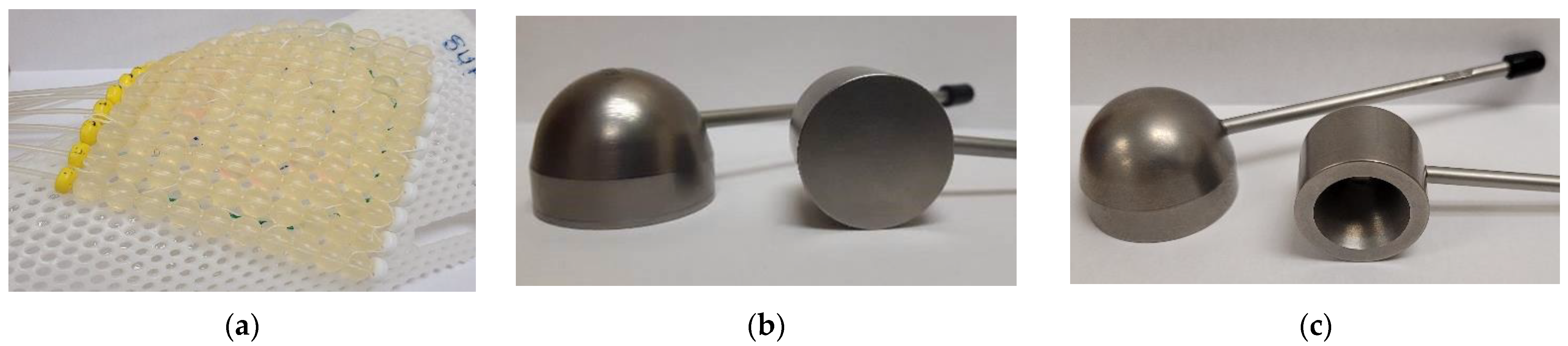
Figure 1.
Three common high dose rate (HDR) brachytherapy applicators. (a) A 10 catheter Freiburg flap applicator; (b) A horizontal 3 cm diameter (left) and horizontal 2 cm diameter (right) Valencia applicator; (c) A horizontal 3 cm diameter (left) and horizontal 2 cm diameter (right) Leipzig applicator.
Figure 1.
Three common high dose rate (HDR) brachytherapy applicators. (a) A 10 catheter Freiburg flap applicator; (b) A horizontal 3 cm diameter (left) and horizontal 2 cm diameter (right) Valencia applicator; (c) A horizontal 3 cm diameter (left) and horizontal 2 cm diameter (right) Leipzig applicator.
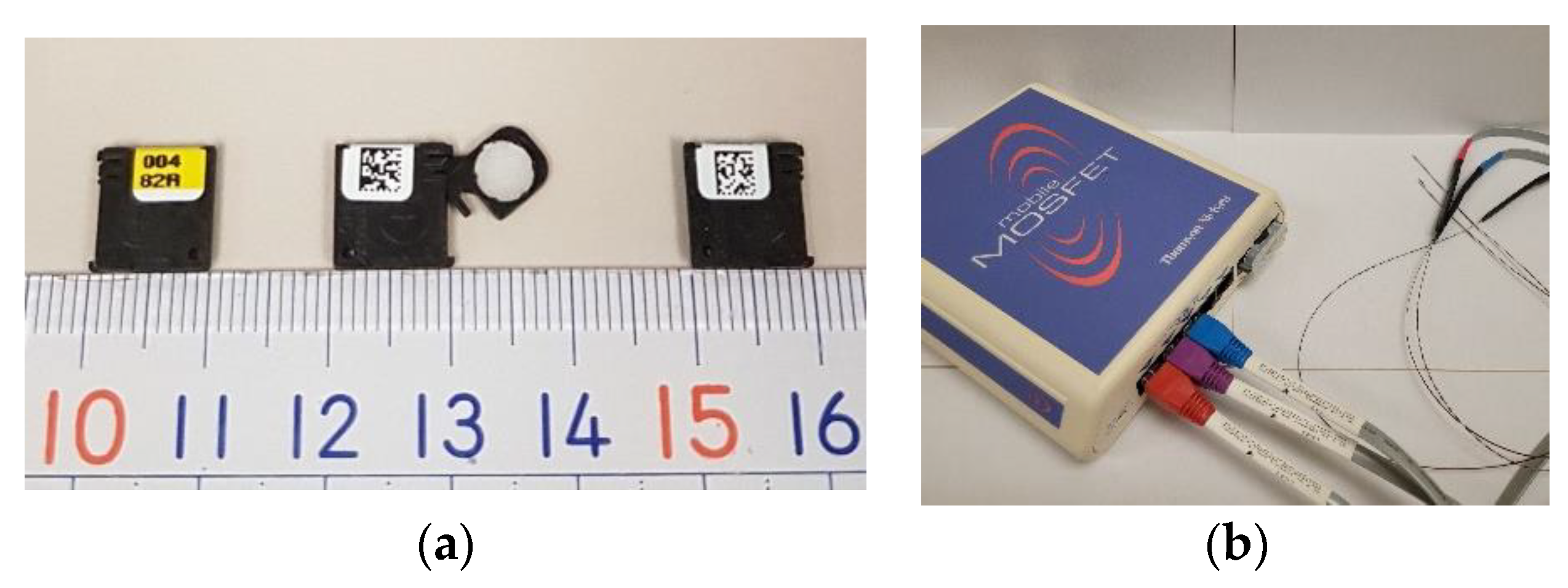
Figure 2.
Optically-stimulated luminescence dosimeter (OSLD) and metal-oxide-semiconductor field-effect transistor (MOSFET) system. (a) A nanoDot TM shown to display its lot number face in closed position (left), QR code face in open position (middle), and QR code face in closed position (right); (b) An image of a mobileMOSFET single channel dosimeter system with three of the five channels connected.
Figure 2.
Optically-stimulated luminescence dosimeter (OSLD) and metal-oxide-semiconductor field-effect transistor (MOSFET) system. (a) A nanoDot TM shown to display its lot number face in closed position (left), QR code face in open position (middle), and QR code face in closed position (right); (b) An image of a mobileMOSFET single channel dosimeter system with three of the five channels connected.
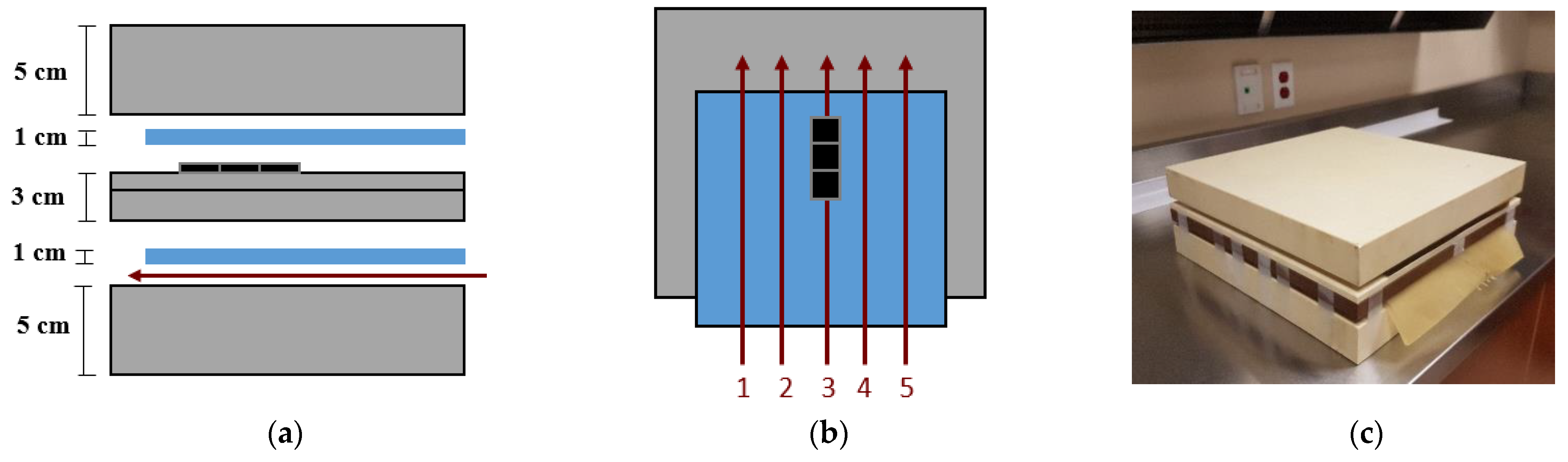
Figure 3.
Calibration set up. (a) A schematic interpretation of the calibration phantom in sagittal view. The slabs of solid water are represented by the grey blocks, and the superflab bolus is represented by the blue blocks. The OSLDs are represented by the black figures, and the catheters are the red arrows; (b) A top view schematic interpretation of the calibration phantom indicating the positions of catheters one to five. Three OSLDs are arranged, one on top of the other, in a superior, middle, and inferior position as shown in the image; (c) An image of the calibration phantom fully assembled.
Figure 3.
Calibration set up. (a) A schematic interpretation of the calibration phantom in sagittal view. The slabs of solid water are represented by the grey blocks, and the superflab bolus is represented by the blue blocks. The OSLDs are represented by the black figures, and the catheters are the red arrows; (b) A top view schematic interpretation of the calibration phantom indicating the positions of catheters one to five. Three OSLDs are arranged, one on top of the other, in a superior, middle, and inferior position as shown in the image; (c) An image of the calibration phantom fully assembled.
Figure 4.
Dose rate dependence phantom. The phantom used to test OSLD dependence on dose rate. An additional 8 cm of solid water was added to the middle of the phantom to provide a total source-to-OSLD distance of 12 cm, as shown in this image.
Figure 4.
Dose rate dependence phantom. The phantom used to test OSLD dependence on dose rate. An additional 8 cm of solid water was added to the middle of the phantom to provide a total source-to-OSLD distance of 12 cm, as shown in this image.
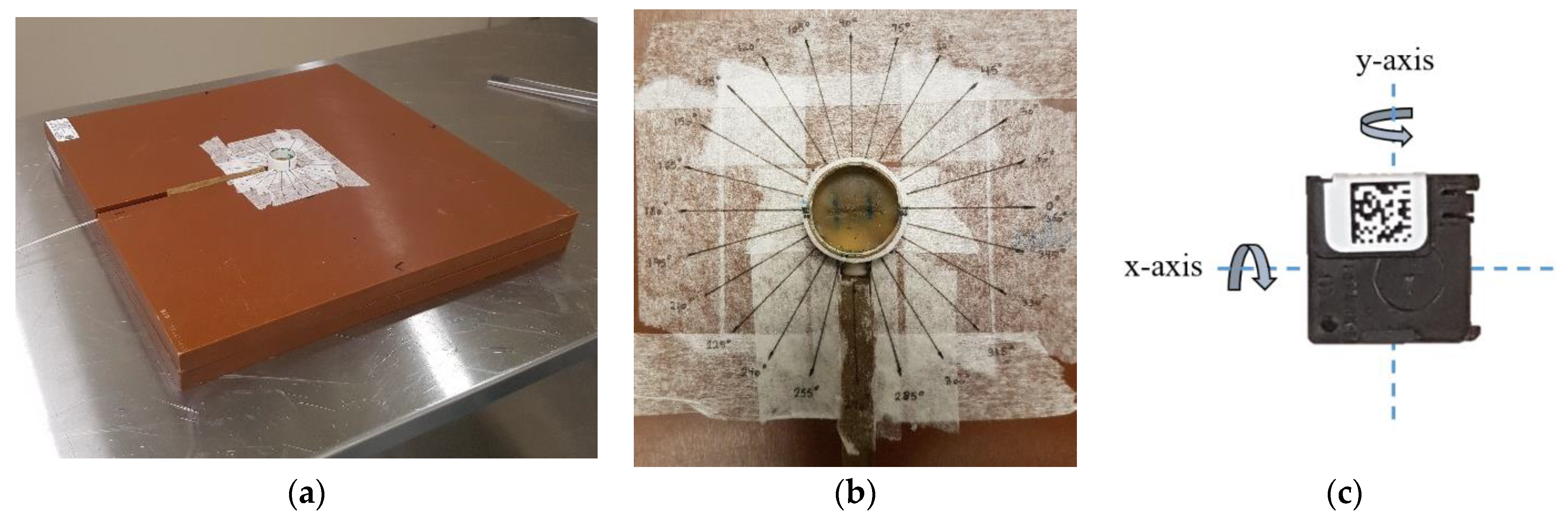
Figure 5.
Angular dependence phantom. (a) The phantom used to test OSLD angular dependence. Two 2 cm solid water slabs were used, with the top slab having the machined circle in the center and canal for the catheter as shown in the image; (b) A close-up of the top of the angular dependence phantom to show OSLD placement within the superflab bolus as well as the marked angles used for the experiment; (c) A depiction of how the OSLD was rotated along its x-axis and y-axis.
Figure 5.
Angular dependence phantom. (a) The phantom used to test OSLD angular dependence. Two 2 cm solid water slabs were used, with the top slab having the machined circle in the center and canal for the catheter as shown in the image; (b) A close-up of the top of the angular dependence phantom to show OSLD placement within the superflab bolus as well as the marked angles used for the experiment; (c) A depiction of how the OSLD was rotated along its x-axis and y-axis.
Figure 6.
X-ray lightbox. Optical annealing set up with an array of 40 open OSLDs arranged on the surface of an X-ray lightbox.
Figure 6.
X-ray lightbox. Optical annealing set up with an array of 40 open OSLDs arranged on the surface of an X-ray lightbox.
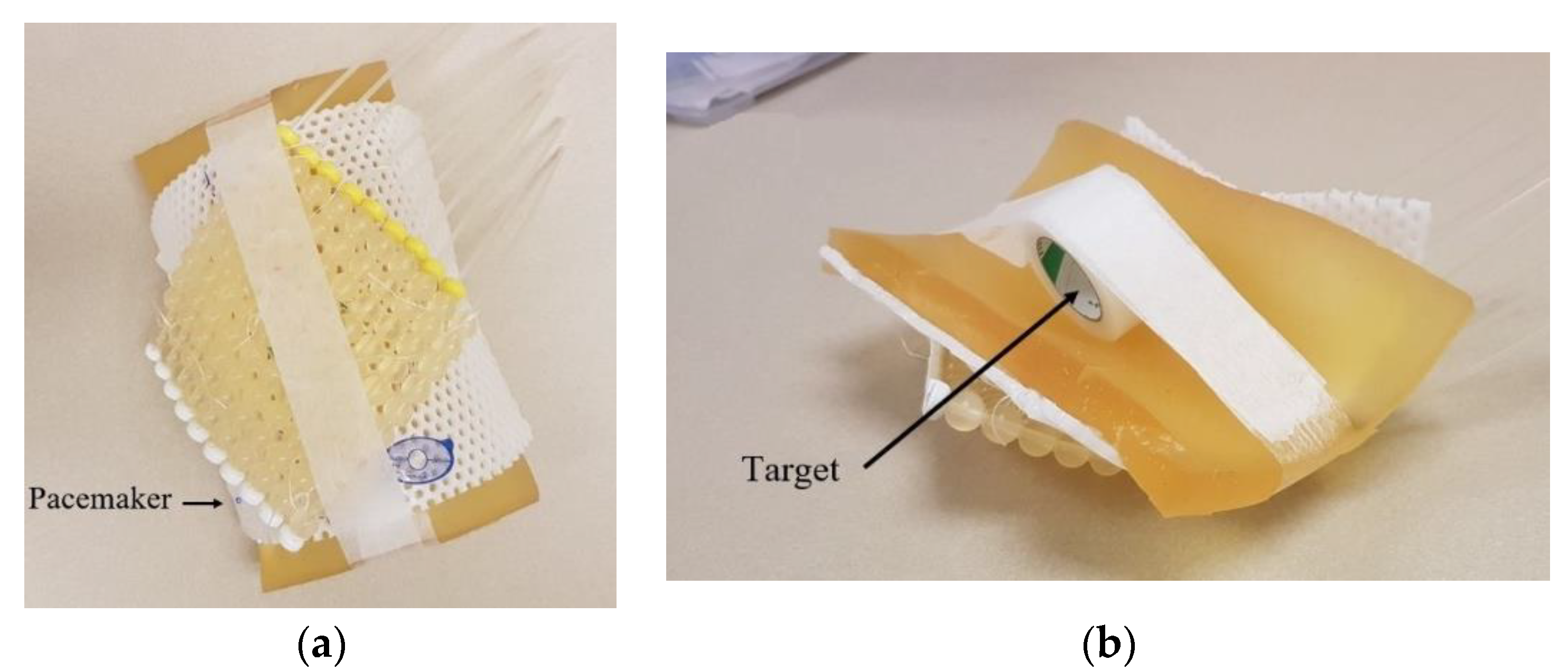
Figure 7.
The phantom used to test OSLDs using a Freiburg flap applicator. (a) Top view of the phantom indicating the position of the pacemaker; (b) Bottom view of phantom indicating the position of the target.
Figure 7.
The phantom used to test OSLDs using a Freiburg flap applicator. (a) Top view of the phantom indicating the position of the pacemaker; (b) Bottom view of phantom indicating the position of the target.
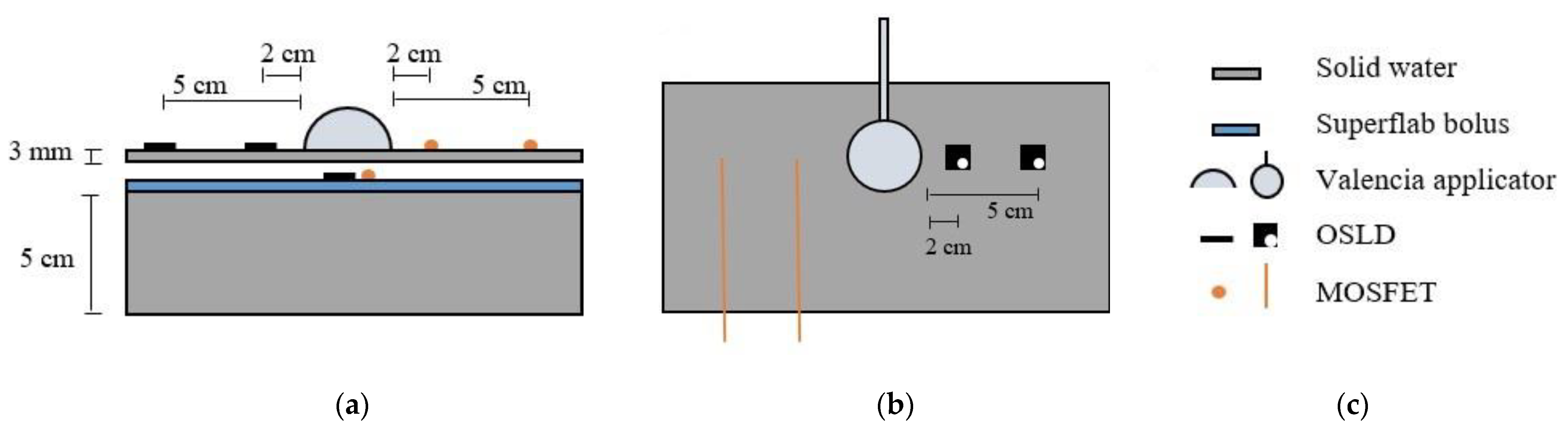
Figure 8.
An interpretation of the phantom used to test OSLDs using an H3 Valencia applicator. (a) Side view of the phantom indicating the positions of the Valencia, OSLDs, and MOSFETs; (b) Top view of phantom indicating the symmetric position of the OSLDs with the MOSFETs about the head of the Valencia; (c) A legend describing the components of the phantom depicted in (a,b).
Figure 8.
An interpretation of the phantom used to test OSLDs using an H3 Valencia applicator. (a) Side view of the phantom indicating the positions of the Valencia, OSLDs, and MOSFETs; (b) Top view of phantom indicating the symmetric position of the OSLDs with the MOSFETs about the head of the Valencia; (c) A legend describing the components of the phantom depicted in (a,b).
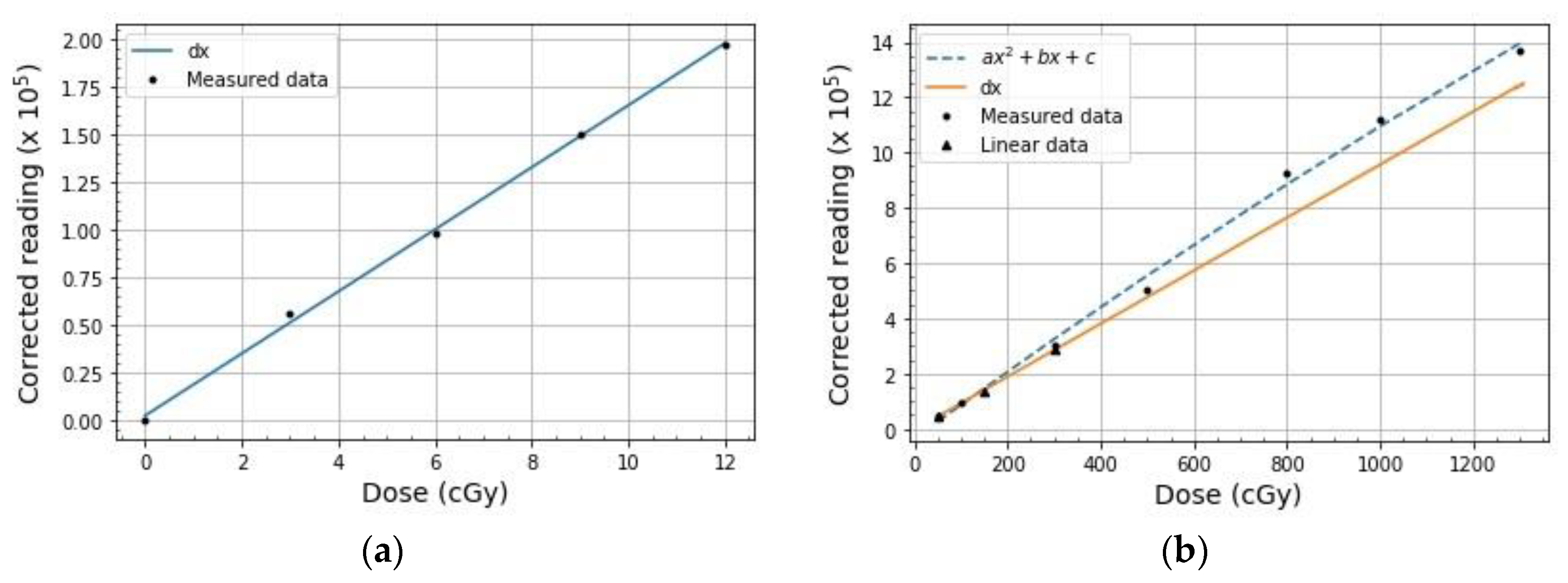
Figure 9.
Calibration results. (a) Low dose linear calibration curve where d = 0.163 ± 0.003; (b) The overlay of the high dose linear and non-linear calibration curves where a = (−1.01 ± 1.06) × 10−6, b = 0.012 ± 0.001, c = −0.35 ± 0.36, and d = (9.6 ± 0.2) × 10−3.
Figure 9.
Calibration results. (a) Low dose linear calibration curve where d = 0.163 ± 0.003; (b) The overlay of the high dose linear and non-linear calibration curves where a = (−1.01 ± 1.06) × 10−6, b = 0.012 ± 0.001, c = −0.35 ± 0.36, and d = (9.6 ± 0.2) × 10−3.
Figure 10.
Dose linearity results. The relationship between OSLD response and absorbed dose. For each data point, a single OSLD was irradiated, kept in the dark for a minimum of 10 min, and then readout. The solid orange line represents OSLD linear response to dose. Meanwhile, the blue dashed curve models the data obtained from this experiment and is described by Equation (1).
Figure 10.
Dose linearity results. The relationship between OSLD response and absorbed dose. For each data point, a single OSLD was irradiated, kept in the dark for a minimum of 10 min, and then readout. The solid orange line represents OSLD linear response to dose. Meanwhile, the blue dashed curve models the data obtained from this experiment and is described by Equation (1).
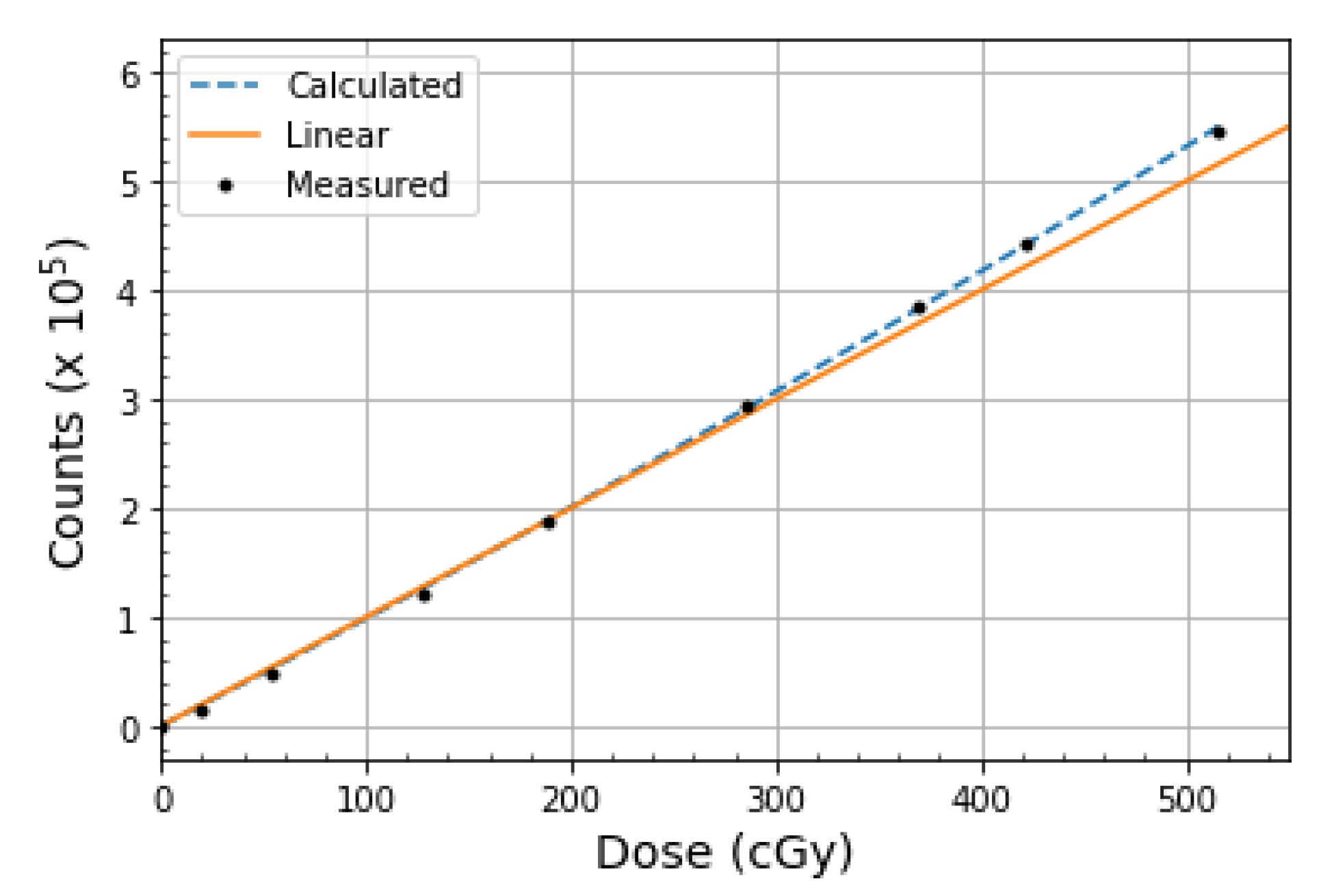
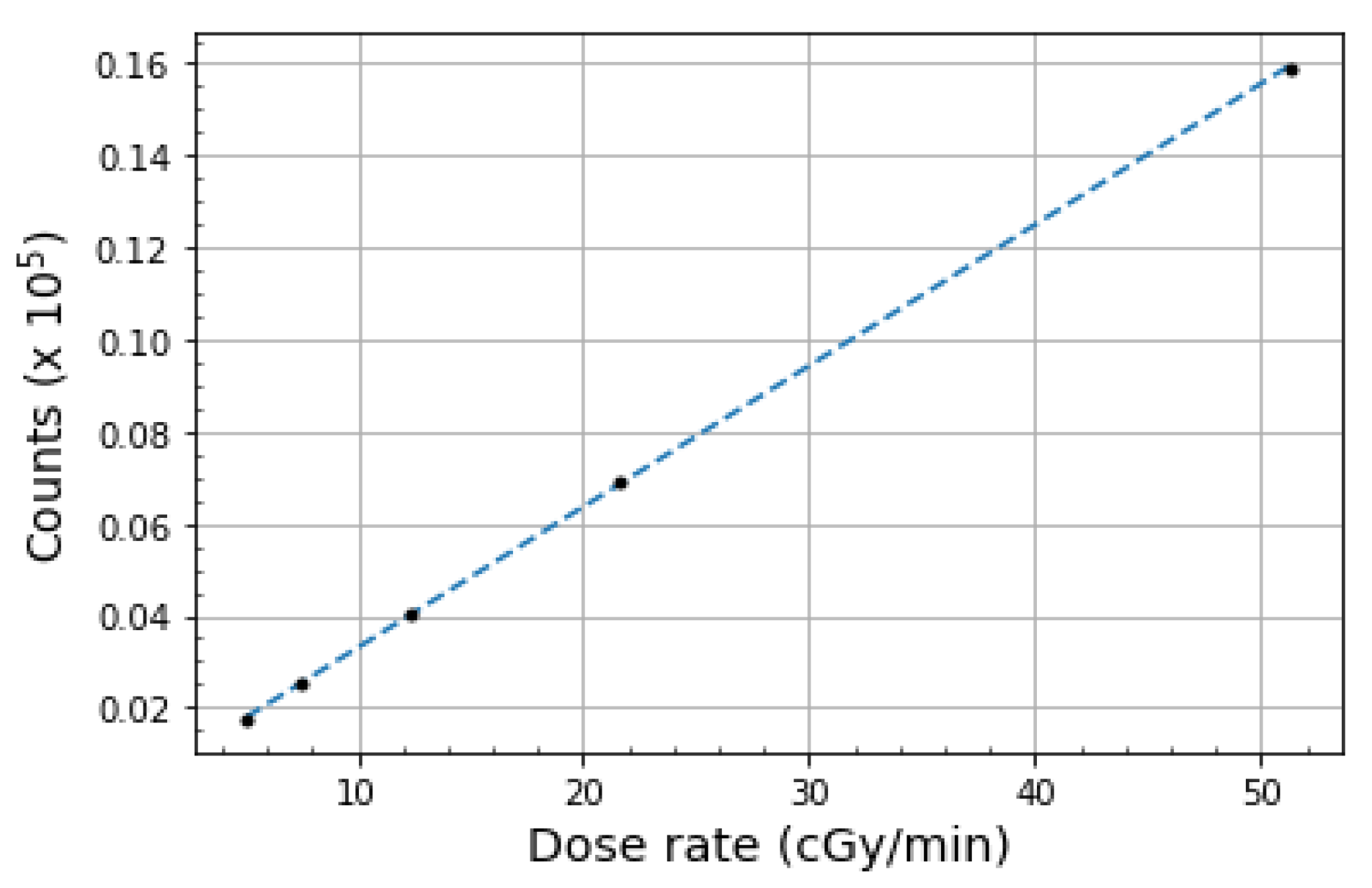
Figure 11.
Dose rate dependence results. The relationship between OSLD counts and absorbed dose with varying dose rates. The data can be modeled by Equation (2), which is represented by the dashed line.
Figure 11.
Dose rate dependence results. The relationship between OSLD counts and absorbed dose with varying dose rates. The data can be modeled by Equation (2), which is represented by the dashed line.
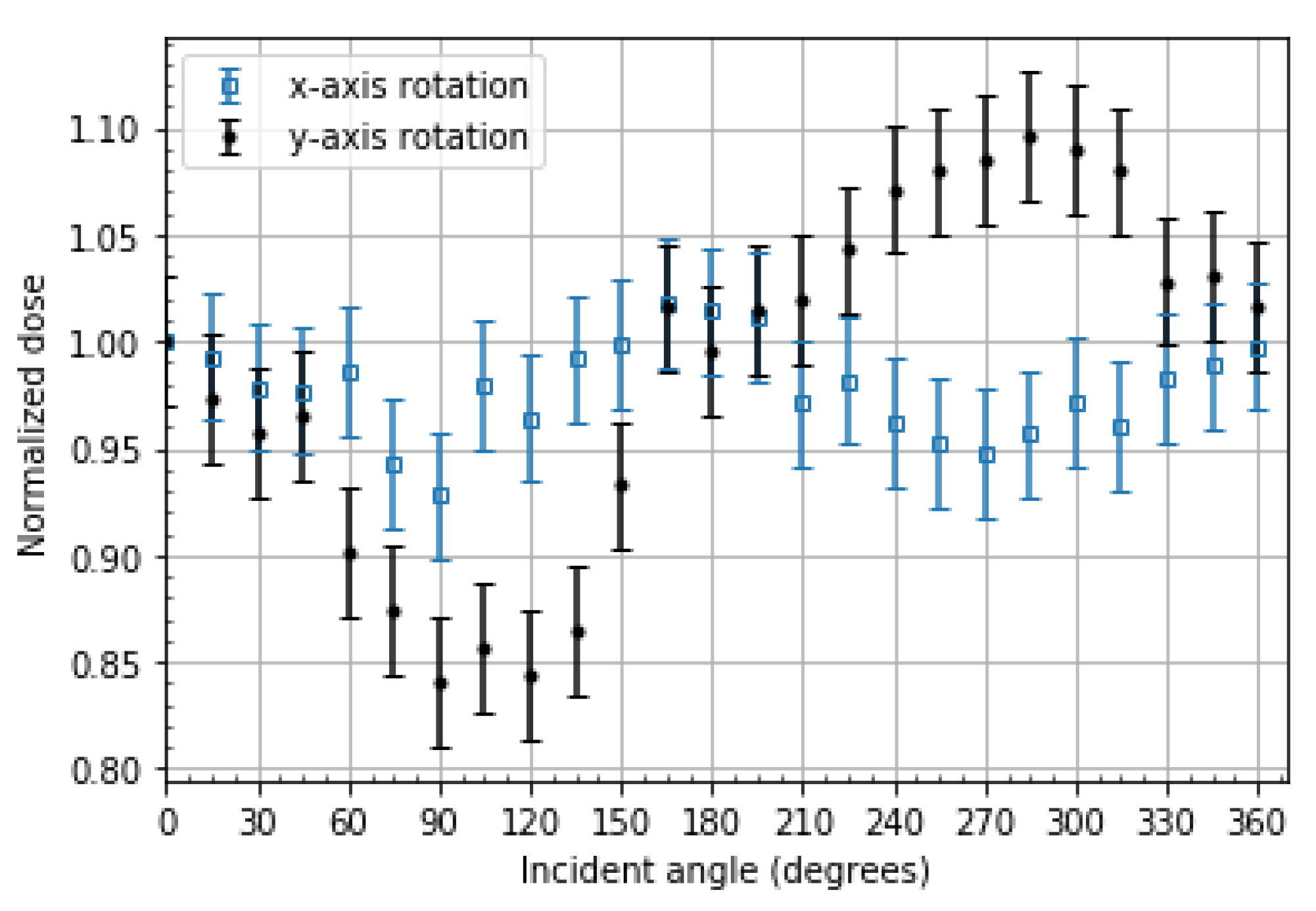
Figure 12.
Angular dependence results. The radiation sensitivity of OSLDs as a function of the incident angle of 192Ir gamma rays normalized to 0°. For both axes of rotation, the incident angle of 0° corresponds to the QR code face of the OSLD, 90° to the thin edge of the OSLD case, 180° to the OSLD lot number face, and 270° to the thick edge of the OSLD case. The error bars represent a standard deviation of four OSLD readouts.
Figure 12.
Angular dependence results. The radiation sensitivity of OSLDs as a function of the incident angle of 192Ir gamma rays normalized to 0°. For both axes of rotation, the incident angle of 0° corresponds to the QR code face of the OSLD, 90° to the thin edge of the OSLD case, 180° to the OSLD lot number face, and 270° to the thick edge of the OSLD case. The error bars represent a standard deviation of four OSLD readouts.
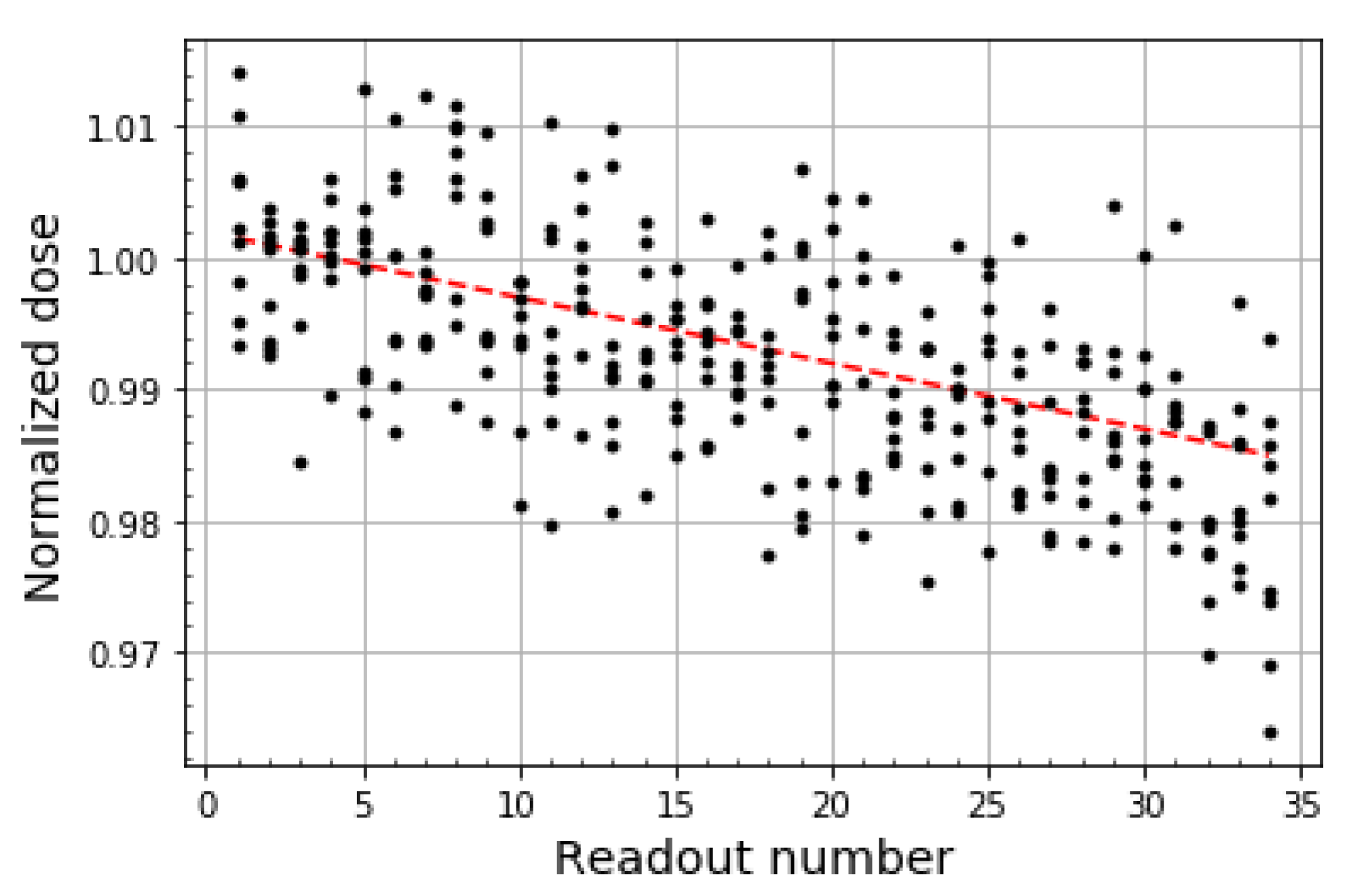
Figure 13.
Readout depletion results. The depletion of OSLD signal with consecutive readouts. The data from all nine irradiated OSLDs is overlayed, and the red dashed line represents the linear regression applied to the data, which has an intercept of 1.002, a slope of −0.0005/readout, and a standard deviation of the residuals of 0.00675.
Figure 13.
Readout depletion results. The depletion of OSLD signal with consecutive readouts. The data from all nine irradiated OSLDs is overlayed, and the red dashed line represents the linear regression applied to the data, which has an intercept of 1.002, a slope of −0.0005/readout, and a standard deviation of the residuals of 0.00675.
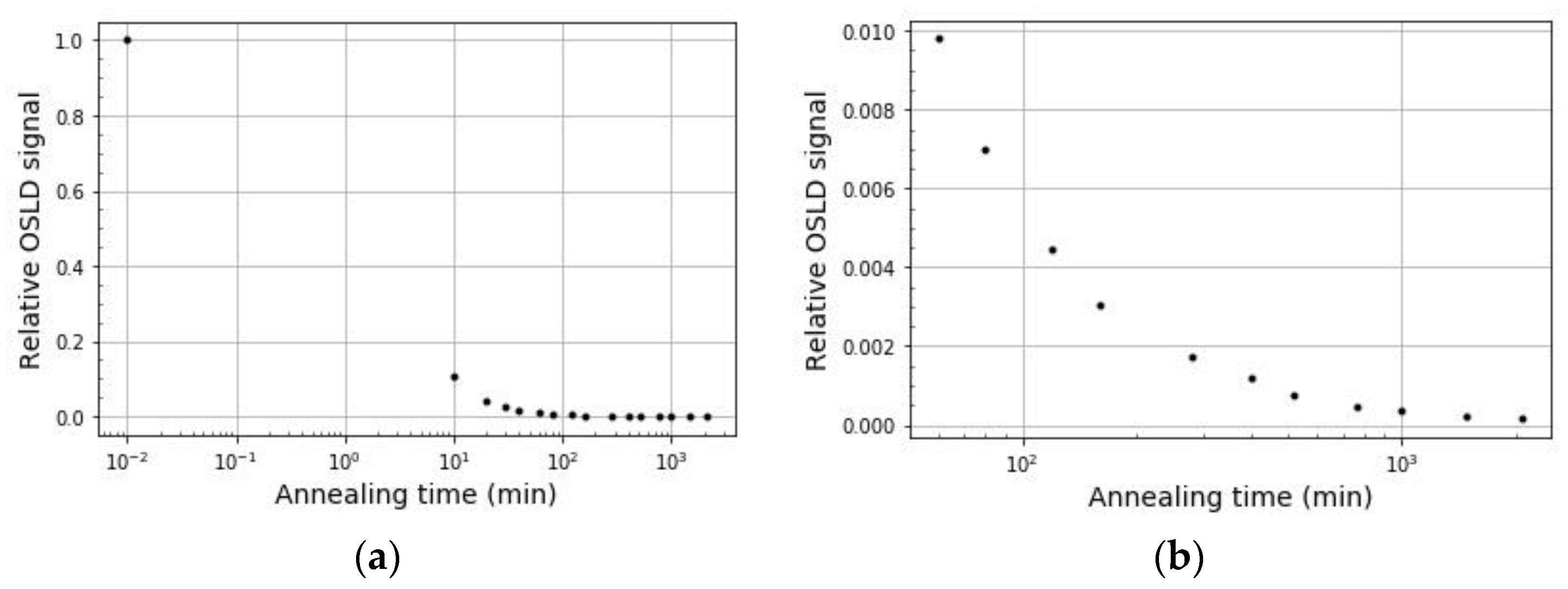
Figure 14.
Optical annealing results. (a) Reduction of OSLD signal with 2080 min of illumination exposure; (b) Reduction in OSLD signal from 60 min to 2080 min of illumination exposure.
Figure 14.
Optical annealing results. (a) Reduction of OSLD signal with 2080 min of illumination exposure; (b) Reduction in OSLD signal from 60 min to 2080 min of illumination exposure.
Table 1.
Calibration levels. Dose levels used to build each calibration curve.
Table 1.
Calibration levels. Dose levels used to build each calibration curve.
| Calibration Type | Dose Range (cGy) | Doses Used to Build the Curve (cGy) |
|---|
| Low dose (linear) | 0–10 | 0, 3, 6, 9, 12 |
| High dose (linear) | 10–300 | 50, 150, 300 |
| High dose (non-linear) | >300 | 50, 100, 300, 500, 800, 1000, 1300 |
Table 2.
Calibration validation. This table displays the calibration validation results for all three curves.
Table 2.
Calibration validation. This table displays the calibration validation results for all three curves.
| Calibration Curve | Validation Dose (cGy) | Measured Dose (cGy) | % Difference from Calibration Curve |
|---|
| Low dose (linear) | 10 | 10.23 | 2.3 |
| 10 | 9.998 | 1.2 |
| High dose (linear) | 200 | 203.0 | 1.5 |
| 200 | 203.8 | 1.9 |
| High dose (non-linear) | 400 | 402.8 | 0.070 |
| 650 | 637.7 | 1.9 |
| 900 | 912.6 | 1.4 |
Table 3.
Theoretical comparison. This table compares the dose rate between the measurements made and the theoretical calculations.
Table 3.
Theoretical comparison. This table compares the dose rate between the measurements made and the theoretical calculations.
| Distance (cm) | Average Counts Normalized | Inverse-Square | % Difference |
|---|
| 4 | 1.00 | 1.00 | - |
| 6 | 0.436 | 0.444 | 1.8 |
| 8 | 0.252 | 0.250 | 0.8 |
| 10 | 0.157 | 0.160 | 1.9 |
| 12 | 0.110 | 0.111 | 0.9 |
Table 4.
Freiburg flap measurements. This table displays the results of the Freiburg flap applicator end-to-end test.
Table 4.
Freiburg flap measurements. This table displays the results of the Freiburg flap applicator end-to-end test.
| Measurement Site | Measured OSLD Dose (cGy) | TPS Dose (cGy) | OSLD/TPS % Difference | OSLD/Lead % Difference |
|---|
| Target | 132.3 | 135 | 2.0 | - |
| Pacemaker | 38.40 | 40.3 | 4.7 | - |
| Pacemaker (with lead) | 37.42 | - | - | 2.6 |
Table 5.
Valencia target measurements. Target dose measurement with H3 Valencia. A dose of 600 cGy was delivered to the target.
Table 5.
Valencia target measurements. Target dose measurement with H3 Valencia. A dose of 600 cGy was delivered to the target.
| Measurement Site | Measured OSLD Dose (cGy) | Measured MOSFET Dose (cGy) | OSLD/MOSFET % Difference |
|---|
| Target | 599.5 | 602 | 0.42 |
Table 6.
Valencia OAR and surface measurements. OAR and surface dose measurements with H3 Valencia. A dose of 600 cGy was delivered to the target.
Table 6.
Valencia OAR and surface measurements. OAR and surface dose measurements with H3 Valencia. A dose of 600 cGy was delivered to the target.
| Measurement Site | Measured OSLD Dose (cGy) | Measured MOSFET Dose (cGy) | OSLD/MOSFET % Difference |
|---|
| OAR | 11.15 | 11.4 | 2.17 |
| OAR (with lead) | 7.861 | 9.36 | 16.0 |
| Surface | 4.946 | 5.57 | 11.2 |

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}