
Radiation Treatment Timing and Dose Delivery: Effects on Bladder Cancer Cells in 3D in Vitro Culture
 , , , , , ,
, , , , , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Culture
2.2. Irradiator
2.3. Clonogenic Assay
2.4. Sphere Formation Assay
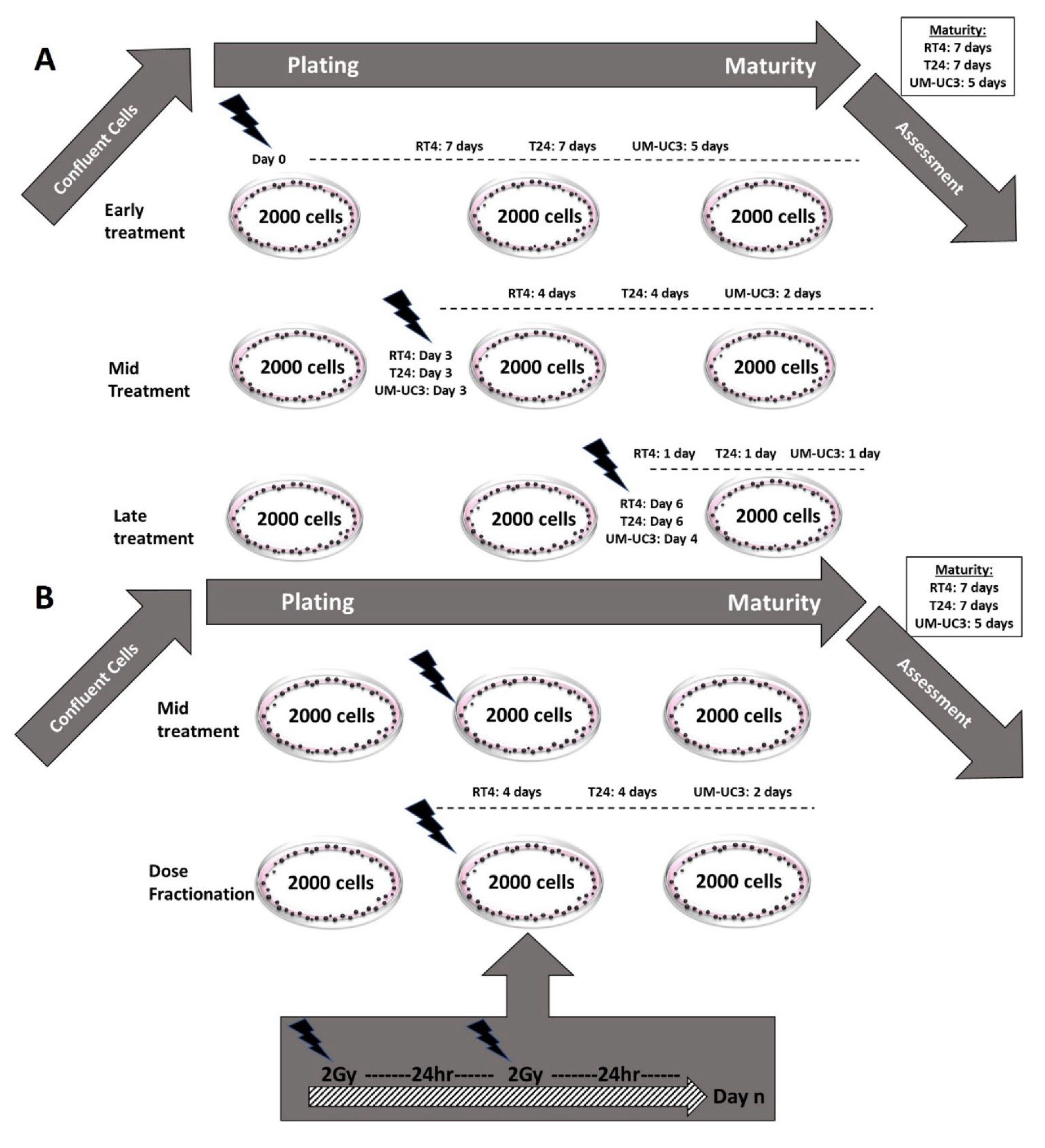
2.5. Sphere Irradiation
- −
- Early treatment: Cells were irradiated with a single dose (ranging between 0 and 10 Gy) immediately after embedding in Matrigel (day 0).
- −
- Late treatment: Spheres were irradiated with a single dose (ranging between 0 and 10 Gy) one day before ending the experiment. The experiment was ended at the specific maturity date for each cell line (Table 1)
- −
- Mid-treatment: Spheres were irradiated with a single dose (ranging between 0 and 10 Gy) halfway between plating and at the end of the experiment.
- −
- Dose fractionation (DF): Spheres were irradiated with a fractionated treatment that started the same day as the mid-treatment. The total dose (ranging between 0 and 10 Gy) was fractionated into 2 Gy/24 h.
2.6. Immunofluorescence and Confocal Microscopy Analysis
2.6.1. For Cells in 2D
2.6.2. For Spheres in 3D
2.7. Statistical Analysis
3. Results
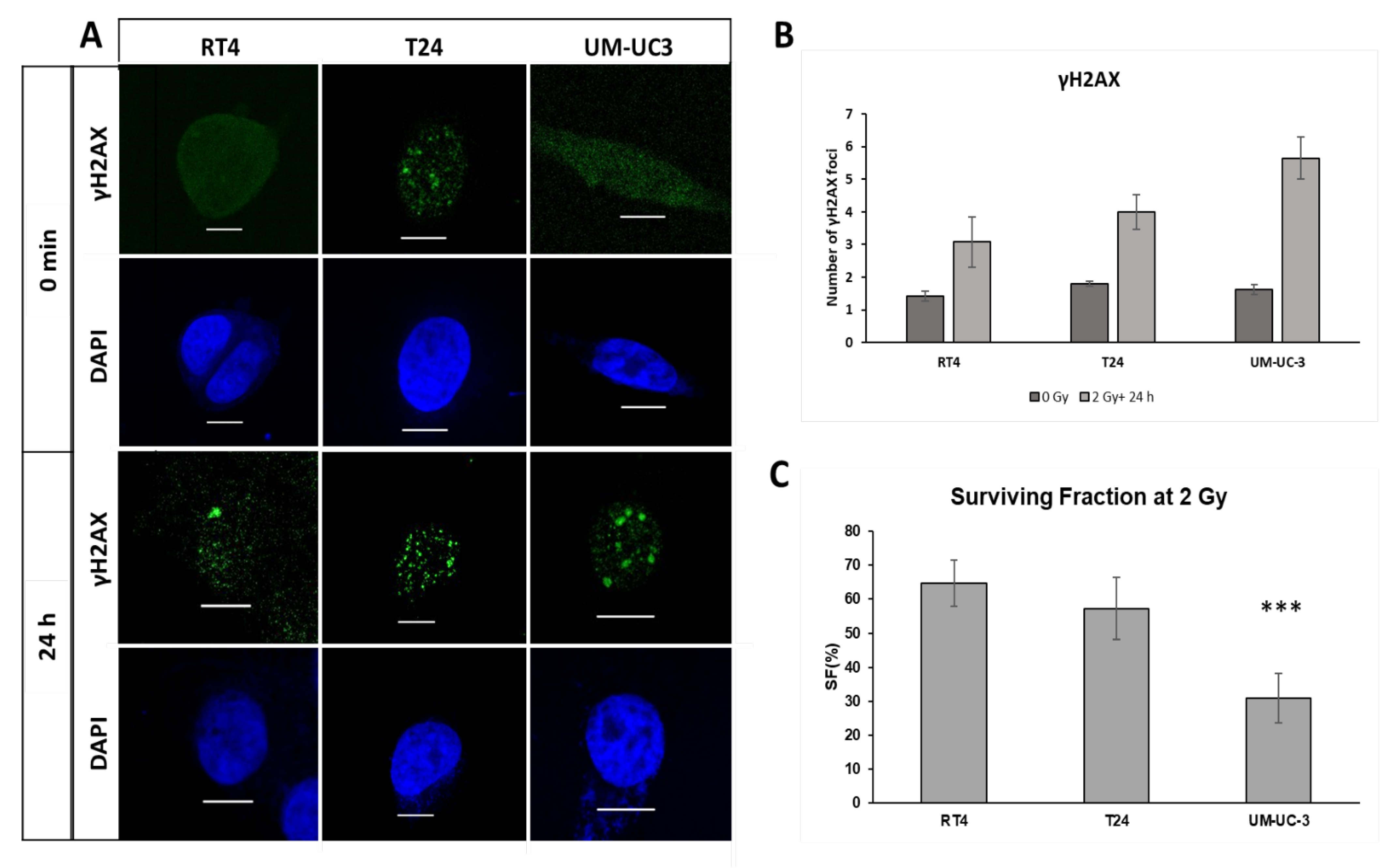
3.1. Radiosensitivity in 2D: Cell Survival and DNA DSB Repair
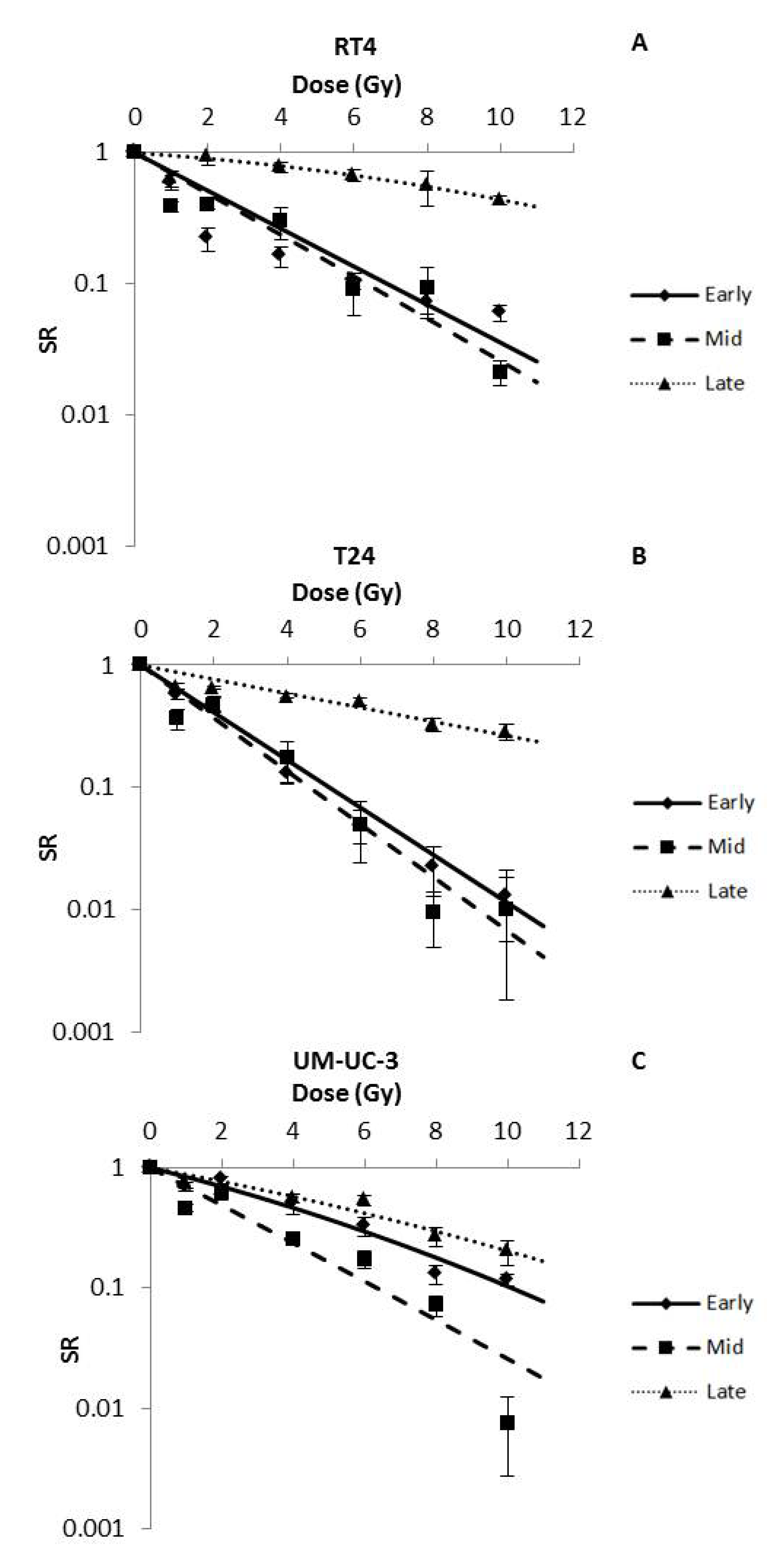
3.2. IR Dose and Timing Influence Sphere Numbers
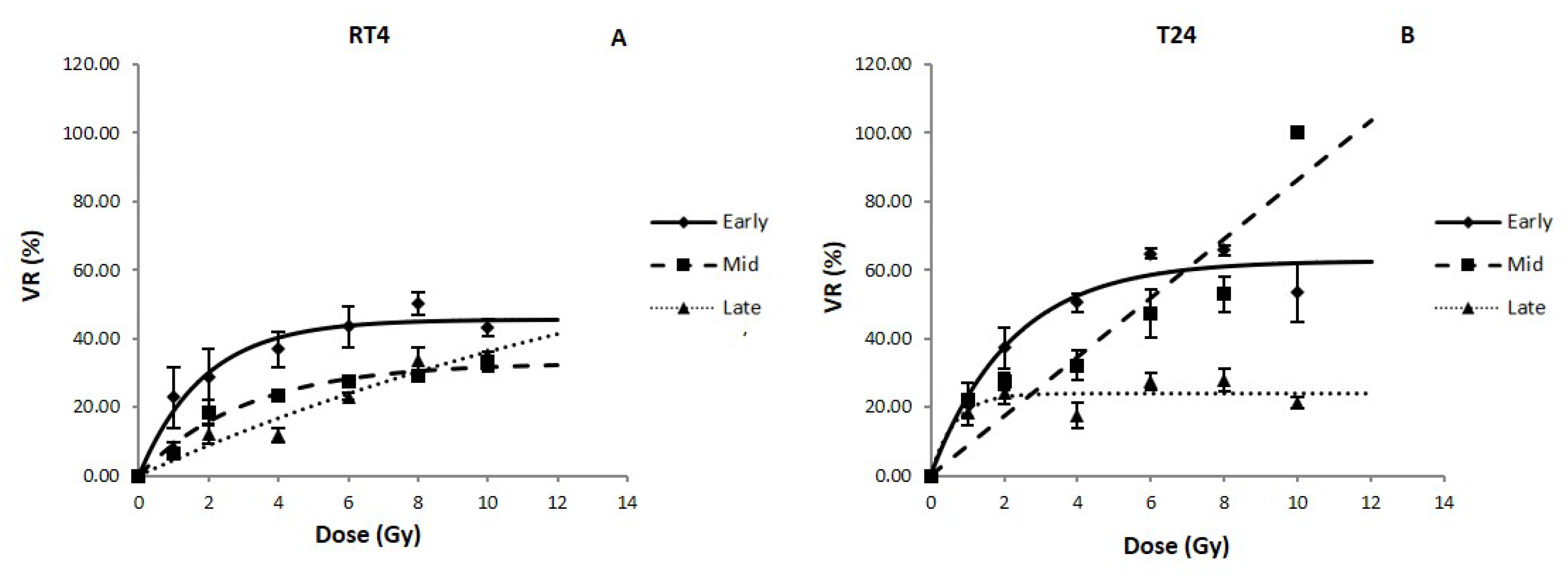
3.3. IR Time- and Dose-Dependent Effect on the Volume of Bladder Cancer Spheres
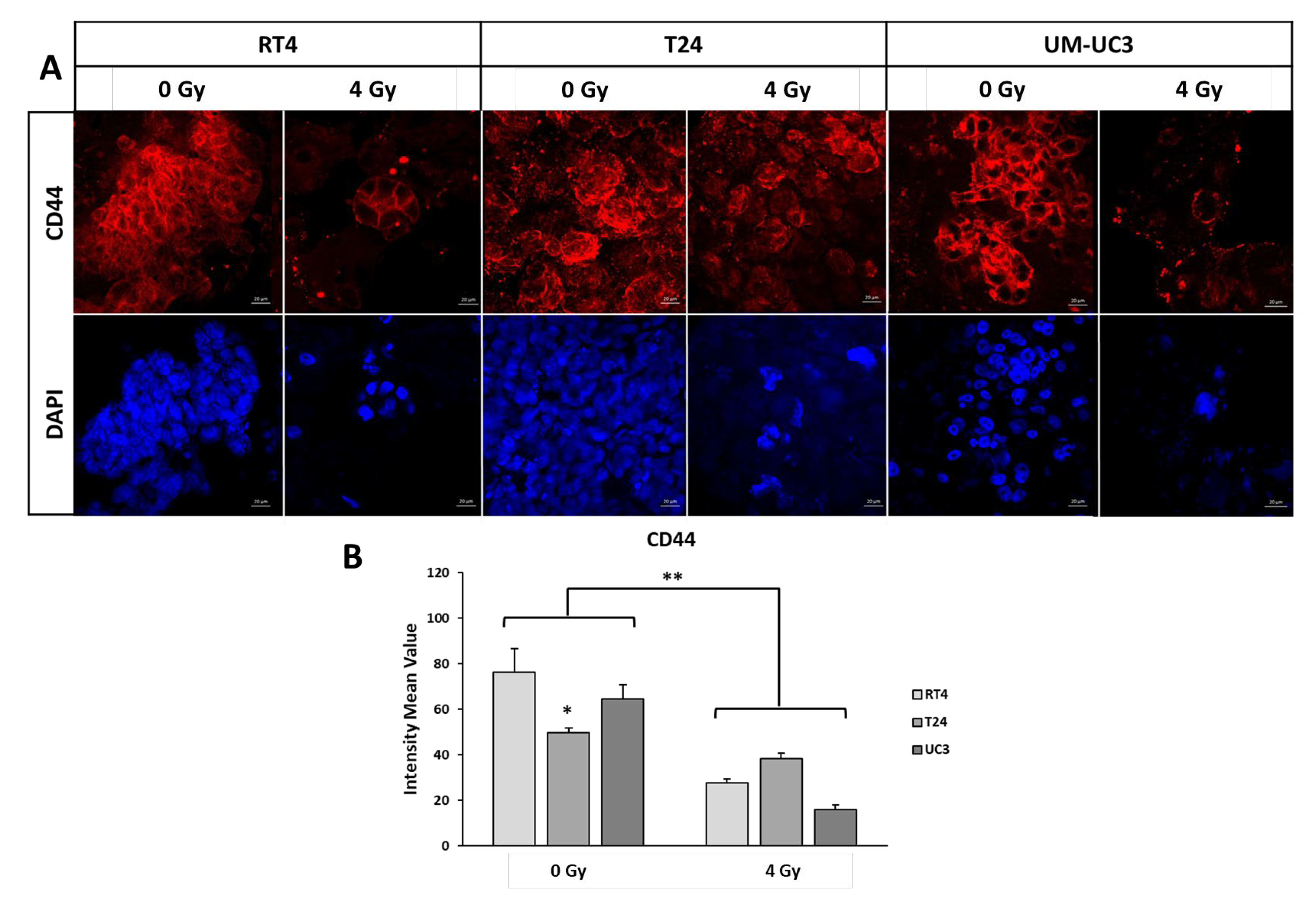
3.4. CD44 Results
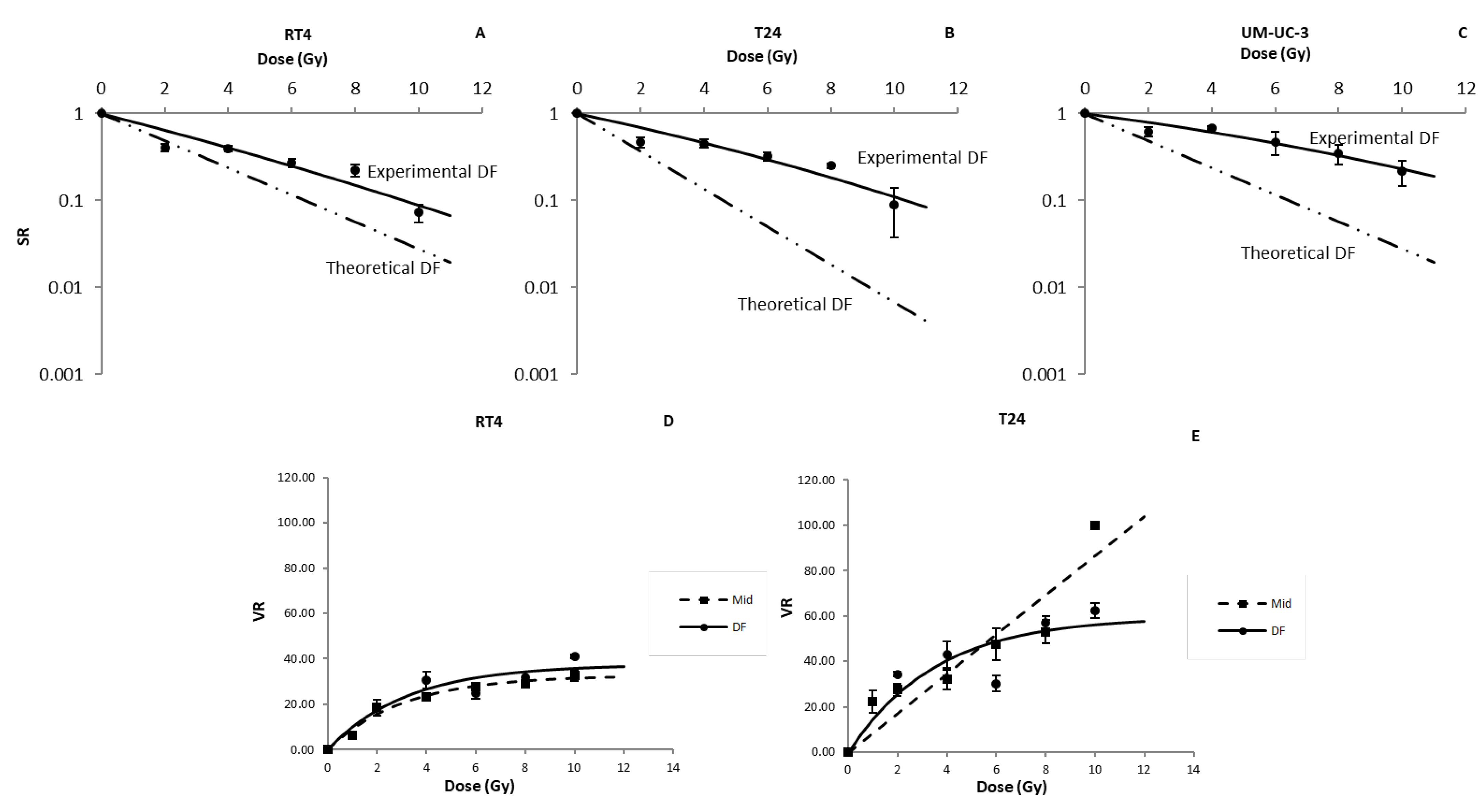
3.5. Dose Fractionation SR Results Are Not Compatible with the Predictions of the LQ Model
3.6. Differences between Pre- and Post-Plating IR
- −
- When treated before plating, RT4 cell line had a sensitivity comparable to early treatments (SR(2 Gy) values of 0.07 ± 0.05 for pre-plating IR vs. 0.07 ± 0.045 for early treatments, p-value < 0.05), while it was more sensitive than mid (SR(2 Gy) = 0.42 ± 0.04%) and late (SR(2 Gy) = 0.95 ± 0.014) treatment protocols.
- −
- T24 (SR(2 Gy) = 0.21 ± 0.03), when treated before plating, was more sensitive than all the post-plating treatments (SR(2 Gy) values of 0.49 ± 0.07, 0.47 ± 0.06 and 0.65 ± 0.02 for early, mid and late treatment protocols, respectively).
- −
- For UM-UC-3, cells irradiated pre-plating had SR values comparable to cells with late treatments, mainly at higher doses, with SR(8 Gy) values of 0.27 ± 0.06 and 0.27 ± 0.05 for pre-plating and late treatments, respectively.
4. Discussion
5. Conclusions
- The radio-response of the 3 bladder cancer cell lines, in terms of VR and SR, is very dependent on the timing of the treatment and the cells’ intrinsic sensitivity to both the treatment timing and dose.
- Current DF predictive models overestimate the sensitivity of the tested bladder cancer spheres.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Available online: https://gco.iarc.fr/today (accessed on 2 March 2022).
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Colquhoun, A.J.; Jones, G.D.D.; Moneef, M.A.L.; Bowman, K.J.; Kockelbergh, R.C.; Symonds, R.P.; Steward, W.P.; Mellon, J.K. Improving and Predicting Radiosensitivity in Muscle Invasive Bladder Cancer. J. Urol. 2003, 169, 1983–1992. [Google Scholar] [CrossRef]
- Zapatero, A.; Martin de Vidales, C.; Arellano, R.; Bocardo, G.; Pérez, M.; Ríos, P. Updated results of bladder-sparing trimodality approach for invasive bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2010, 28, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Shipley, W.U.; Zietman, A.L.; Kaufman, D.S.; Coen, J.J.; Sandler, H.M. Selective bladder preservation by trimodality therapy for patients with muscularis propria-invasive bladder cancer and who are cystectomy candidates—The Massachusetts General Hospital and Radiation Therapy Oncology Group experiences. Semin. Radiat. Oncol. 2005, 15, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Gakis, G.; Efstathiou, J.; Lerner, S.P.; Cookson, M.S.; Keegan, K.A.; Guru, K.A.; Shipley, W.U.; Heidenreich, A.; Schoenberg, M.P.; Sagaloswky, A.I.; et al. ICUD-EAU International Consultation on Bladder Cancer 2012: Radical Cystectomy and Bladder Preservation for Muscle-Invasive Urothelial Carcinoma of the Bladder. Eur. Urol. 2013, 63, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.S.; Lamb, B.W.; Kelly, J.D. Complications of Radical Cystectomy and Orthotopic Reconstruction. Adv. Urol. 2015, 2015, 323157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajab, N.F.; McKenna, D.J.; Diamond, J.; Williamson, K.; Hamilton, P.W.; McKelvey-Martin, V.J. Prediction of radiosensitivity in human bladder cell lines using nuclear chromatin phenotype. Cytom. Part A 2006, 69A, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Moneef, M.A.L.; Sherwood, B.T.; Bowman, K.J.; Kockelbergh, R.C.; Symonds, R.P.; Steward, W.P.; Mellon, J.K.; Jones, G.D.D. Measurements using the alkaline comet assay predict bladder cancer cell radiosensitivity. Br. J. Cancer 2003, 89, 2271–2276. [Google Scholar] [CrossRef] [Green Version]
- Hinata, N.; Shirakawa, T.; Zhang, Z.; Matsumoto, A.; Fujisawa, M.; Okada, H.; Kamidono, S.; Gotoh, A. Radiation induces p53-dependent cell apoptosis in bladder cancer cells with wild-type- p53 but not in p53-mutated bladder cancer cells. Urol. Res. 2003, 31, 387–396. [Google Scholar] [CrossRef]
- Ruiz de Almodovar, J.M.; Nunez, M.I.; McMillan, T.J.; Olea, N.; Mort, C.; Villalobos, M.; Pedraza, V.; Steel, G.G. Initial radiation-induced DNA damage in human tumour cell lines: A correlation with intrinsic cellular radiosensitivity. Br. J. Cancer 1994, 69, 457–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeggo, P.A.; Lobrich, M. DNA double-strand breaks: Their cellular and clinical impact? Oncogene 2007, 26, 7717–7719. [Google Scholar] [CrossRef]
- Joubert, A.; Foray, N. Intrinsic radiosensitivity and DNA double-strand breaks in human cells. Cancer Radiother. 2007, 11, 129–142. [Google Scholar] [CrossRef] [PubMed]
- Joubert, A.; Zimmerman, K.M.; Bencokova, Z.; Gastaldo, J.; Rénier, W.; Chavaudra, N.; Favaudon, V.; Arlett, C.; Foray, N. DNA double-strand break repair defects in syndromes associated with acute radiation response: At least two different assays to predict intrinsic radiosensitivity? Int. J. Radiat. Biol. 2008, 84, 107–125. [Google Scholar] [CrossRef]
- Puck, T.T.; Marcus, P.I. Action of x-rays on mammalian cells. J. Exp. Med. 1956, 103, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Fertil, B.; Malaise, E.P. Inherent cellular radiosensitivity as a basic concept for human tumor radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1981, 7, 621–629. [Google Scholar] [CrossRef]
- Bodgi, L.; Foray, N. The nucleo-shuttling of the ATM protein as a basis for a novel theory of radiation response: Resolution of the linear-quadratic model. Int. J. Radiat. Biol. 2016, 92, 117–131. [Google Scholar] [CrossRef]
- Deschavanne, P.J.; Fertil, B. A review of human cell radiosensitivity in vitro. Int. J. Radiat. Oncol. Biol. Phys. 1996, 34, 251–266. [Google Scholar] [CrossRef]
- Fertil, B.; Reydellet, I.; Deschavanne, P.J. A benchmark of cell survival models using survival curves for human cells after completion of repair of potentially lethal damage. Radiat. Res. 1994, 138, 61–69. [Google Scholar] [CrossRef]
- Curtis, S.B. Mechanistic models. Basic Life Sci. 1991, 58, 367–382, discussion 382-366. [Google Scholar] [PubMed]
- Curtis, S.B. Lethal and potentially lethal lesions induced by radiation--a unified repair model. Radiat. Res. 1986, 106, 252–270. [Google Scholar] [CrossRef] [PubMed]
- Tobias, C.A. The repair-misrepair model in radiobiology: Comparison to other models. Radiat. Res. Suppl. 1985, 8, S77–S95. [Google Scholar] [CrossRef] [PubMed]
- Chadwick, K.H.; Leenhouts, H.P. A molecular theory of cell survival. Phys. Med. Biol. 1973, 13, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Bodgi, L.; Canet, A.; Pujo-Menjouet, L.; Lesne, A.; Victor, J.M.; Foray, N. Mathematical models of radiation action on living cells: From the target theory to the modern approaches. A historical and critical review. J. Biol. 2016, 394, 93–101. [Google Scholar] [CrossRef]
- Bentzen, S.M.; Christensen, J.J.; Overgaard, J.; Overgaard, M. Some methodological problems in estimating radiobiological parameters from clinical data. Alpha/beta ratios and electron RBE for cutaneous reactions in patients treated with postmastectomy radiotherapy. Acta Oncol. 1988, 27, 105–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahmad, H.F.; Cheaito, K.; Chalhoub, R.M.; Hadadeh, O.; Monzer, A.; Ballout, F.; El-Hajj, A.; Mukherji, D.; Liu, Y.-N.; Daoud, G.; et al. Sphere-Formation Assay: Three-Dimensional in vitro Culturing of Prostate Cancer Stem/Progenitor Sphere-Forming Cells. Front. Oncol. 2018, 8, 347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodgi, L.; Bahmad, H.F.; Araji, T.; Al Choboq, J.; Bou-Gharios, J.; Cheaito, K.; Zeidan, Y.H.; Eid, T.; Geara, F.; Abou-Kheir, W. Assessing Radiosensitivity of Bladder Cancer in vitro: A 2D vs. 3D Approach. Front. Oncol. 2019, 9, 153. [Google Scholar] [CrossRef] [Green Version]
- Azzi, J.; Waked, A.; Bou-Gharios, J.; Al Choboq, J.; Geara, F.; Bodgi, L.; Maalouf, M. Radiosensitizing Effect of Curcumin on Human Bladder Cancer Cell Lines: Impact on DNA Repair Mechanisms. Nutr. Cancer 2022, 74, 2207–2221. [Google Scholar] [CrossRef]
- Bou-Gharios, J.; Assi, S.; Bahmad, H.F.; Kharroubi, H.; Araji, T.; Chalhoub, R.M.; Ballout, F.; Harati, H.; Fares, Y.; Abou-Kheir, W. The potential use of tideglusib as an adjuvant radio-therapeutic treatment for glioblastoma multiforme cancer stem-like cells. Pharmacol. Rep. 2021, 73, 227–239. [Google Scholar] [CrossRef]
- Anderson, K.; Lutz, C.; Van Delft, F.W.; Bateman, C.M.; Guo, Y.; Colman, S.M.; Kempski, H.; Moorman, A.V.; Titley, I.; Swansbury, J.; et al. Genetic variegation of clonal architecture and propagating cells in leukaemia. Nature 2011, 469, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Codony-Servat, J.; Rosell, R. Cancer stem cells and immunoresistance: Clinical implications and solutions. Transl. Lung Cancer Res. 2015, 4, 689–703. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, H.; Okudela, K.; Yazawa, T.; Sato, H.; Shimoyamada, H. Cancer stem cell: Implications in cancer biology and therapy with special reference to lung cancer. Lung Cancer 2009, 66, 275–281. [Google Scholar] [CrossRef]
- Wu, C.-T.; Lin, W.-Y.; Chang, Y.-H.; Chen, W.-C.; Chen, M.-F. Impact of CD44 expression on radiation response for bladder cancer. J. Cancer 2017, 8, 1137–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, M.; Fojo, T.; Bates, S. Tumour stem cells and drug resistance. Nat. Rev. Cancer 2005, 5, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, L.N.; Chow, E.K.-H. Mechanisms of chemoresistance in cancer stem cells. Clin. Transl. Med. 2013, 2, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnenberg, V.S.; Donnenberg, A.D. Multiple drug resistance in cancer revisited: The cancer stem cell hypothesis. J. Clin. Pharmacol. 2005, 45, 872–877. [Google Scholar] [CrossRef]
- Abou-Kheir, W.G.; Hynes, P.G.; Martin, P.L.; Pierce, R.; Kelly, K. Characterizing the contribution of stem/progenitor cells to tumorigenesis in the Pten-/-TP53-/- prostate cancer model. Stem Cells 2010, 28, 2129–2140. [Google Scholar] [CrossRef]
- Mouhieddine, T.H.; Nokkari, A.; Itani, M.M.; Chamaa, F.; Bahmad, H.; Monzer, A.; El-Merahbi, R.; Daoud, G.; Eid, A.; Kobeissy, F.H.; et al. Metformin and Ara-a Effectively Suppress Brain Cancer by Targeting Cancer Stem/Progenitor Cells. Front. Neurosci. 2015, 9, 442. [Google Scholar] [CrossRef] [Green Version]
- Morrison, B.J.; Steel, J.C.; Morris, J.C. Sphere Culture of Murine Lung Cancer Cell Lines Are Enriched with Cancer Initiating Cells. PLoS ONE 2012, 7, e49752. [Google Scholar] [CrossRef]
- Abou-Kheir, W.; Hynes, P.G.; Martin, P.; Yin, J.J.; Liu, Y.N.; Seng, V.; Lake, R.; Spurrier, J.; Kelly, K. Self-renewing Pten-/-TP53-/- protospheres produce metastatic adenocarcinoma cell lines with multipotent progenitor activity. PLoS ONE 2011, 6, e26112. [Google Scholar] [CrossRef]
- Riedl, A.; Schlederer, M.; Pudelko, K.; Stadler, M.; Walter, S.; Unterleuthner, D.; Unger, C.; Kramer, N.; Hengstschlager, M.; Kenner, L.; et al. Comparison of cancer cells in 2D vs 3D culture reveals differences in AKT-mTOR-S6K signaling and drug responses. J. Cell Sci. 2017, 130, 203–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bissell, M.J. Goodbye flat biology—Time for the 3rd and the 4th dimensions. J. Cell Sci. 2017, 130, 3–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sart, S.; Tomasi, R.F.X.; Amselem, G.; Baroud, C.N. Multiscale cytometry and regulation of 3D cell cultures on a chip. Nat. Commun. 2017, 8, 469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, T.; Sopko, N.A.; Kates, M.; Liu, X.; Joice, G.; McConkey, D.J.; Bivalacqua, T.J. Impact of spheroid culture on molecular and functional characteristics of bladder cancer cell lines. Oncol. Lett. 2019, 18, 4923–4929. [Google Scholar] [CrossRef] [Green Version]
- Amaral, R.L.; Miranda, M.; Marcato, P.D.; Swiech, K. Comparative analysis of 3D bladder tumor spheroids obtained by forced floating and hanging drop methods for drug screening. Front. Physiol. 2017, 8, 605. [Google Scholar] [CrossRef] [Green Version]
- Pereira, P.M.R.; Berisha, N.; Bhupathiraju, N.; Fernandes, R.; Tomé, J.P.C.; Drain, C.M. Cancer cell spheroids are a better screen for the photodynamic efficiency of glycosylated photosensitizers. PLoS ONE 2017, 12, e0177737. [Google Scholar] [CrossRef]
- Mann, H.B.; Whitney, D.R. On a Test of Whether one of Two Random Variables is Stochastically Larger than the Other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Wilcoxon, F. Individual Comparisons by Ranking Methods. Biom. Bull. 1945, 1, 80–83. [Google Scholar] [CrossRef]
- Kruskal, W.H.; Wallis, W.A. Use of Ranks in One-Criterion Variance Analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Coleman, T.; Li, Y. An Interior Trust Region Approach for Nonlinear Minimization Subject to Bounds. SIAM J. Optim. 1996, 6, 418–445. [Google Scholar] [CrossRef]
- Burger, M.; Oosterlinck, W.; Konety, B.; Chang, S.; Gudjonsson, S.; Pruthi, R.; Soloway, M.; Solsona, E.; Sved, P.; Babjuk, M.; et al. ICUD-EAU International Consultation on Bladder Cancer 2012: Non–Muscle-Invasive Urothelial Carcinoma of the Bladder. Eur. Urol. 2013, 63, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Selph, S.S.; Buckley, D.I.; Gustafson, K.S.; Griffin, J.C.; Grusing, S.E.; Gore, J.L. Treatment of muscle-invasive bladder cancer: A systematic review. Cancer 2016, 122, 842–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carillo, V.; Cozzarini, C.; Rancati, T.; Avuzzi, B.; Botti, A.; Borca, V.C.; Cattari, G.; Civardi, F.; Esposti, C.D.; Franco, P.; et al. Relationships between bladder dose–volume/surface histograms and acute urinary toxicity after radiotherapy for prostate cancer. Radiother. Oncol. 2014, 111, 100–105. [Google Scholar] [CrossRef]
- Feuerstein, M.A.; Goenka, A. Quality of Life Outcomes for Bladder Cancer Patients Undergoing Bladder Preservation with Radiotherapy. Curr. Urol. Rep. 2015, 16, 75. [Google Scholar] [CrossRef]
- Koga, F.; Kihara, K. Selective bladder preservation with curative intent for muscle-invasive bladder cancer: A contemporary review. Int. J. Urol. 2012, 19, 388–401. [Google Scholar] [CrossRef]
- Majewski, W.; Tarnawski, R. Acute and Late Toxicity in Radical Radiotherapy for Bladder Cancer. Clin. Oncol. 2009, 21, 598–609. [Google Scholar] [CrossRef]
- Milosevic, M.; Gospodarowicz, M.; Zietman, A.; Abbas, F.; Haustermans, K.; Moonen, L.; Rödel, C.; Schoenberg, M.; Shipley, W. Radiotherapy for Bladder Cancer. Urology 2007, 69, 80–92. [Google Scholar] [CrossRef] [Green Version]
- Ott, O.J.; Rödel, C.; Weiss, C.; Wittlinger, M.; St. Krause, F.; Dunst, J.; Fietkau, R.; Sauer, R. Radiochemotherapy for Bladder Cancer. Clin. Oncol. 2009, 21, 557–565. [Google Scholar] [CrossRef]
- Sengeløv, L.; Von der Maase, H. Radiotherapy in bladder cancer. Radiother. Oncol. 1999, 52, 1–14. [Google Scholar] [CrossRef]
- Zhang, S.; Yu, Y.-H.; Zhang, Y.; Qu, W.; Li, J. Radiotherapy in muscle-invasive bladder cancer: The latest research progress and clinical application. Am. J. Cancer Res. 2015, 5, 854–868. [Google Scholar]
- Pettiford, J.; Rashid, S.; Balyimez, A.; Radivoyevitch, T.; Koshkin, V.S.; Lindner, D.J.; Parker, Y.; Day, M.L.; Day, K.C.; Tomlins, S.; et al. Identification of gene expression determinants of radiosensitivity in bladder cancer (BC) cell lines. J. Clin. Oncol. 2018, 36, e16507. [Google Scholar] [CrossRef]
- Peters, L.J. The ESTRO Regaud lecture Inherent radio sensitivity of tumor and normal tissue cells as a predictor of human tumor response. Radiother. Oncol. 1990, 17, 177–190. [Google Scholar] [CrossRef]
- Brengues, M.; Lapierre, A.; Bourgier, C.; Pèlegrin, A.; Özsahin, M.; Azria, D. T lymphocytes to predict radiation-induced late effects in normal tissues. Expert Rev. Mol. Diagn. 2017, 17, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, I. Application of radiogenomics in radiation oncology. J. Radiat. Cancer Res. 2017, 8, 74–76. [Google Scholar] [CrossRef]
- Azimzadeh, O.; Tapio, S. Proteomics approaches to investigate cancer radiotherapy outcome: Slow train coming. Transl. Cancer Res. 2017, 6, S779–S788. [Google Scholar] [CrossRef]
- Vogin, G.; Bodgi, L.; Canet, A.; Pereira, S.; Gillet-Daubin, J.; Foray, N. OC-0221: High-performance radiosensitivity assay to predict post radiation overreactions. Radiother. Oncol. 2017, 123, S110–S111. [Google Scholar] [CrossRef]
- Granzotto, A.; Benadjaoud, M.A.; Vogin, G.; Devic, C.; Ferlazzo, M.L.; Bodgi, L.; Pereira, S.; Sonzogni, L.; Forcheron, F.; Viau, M.; et al. Influence of Nucleoshuttling of the ATM Protein in the Healthy Tissues Response to Radiation Therapy: Toward a Molecular Classification of Human Radiosensitivity. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 450–460. [Google Scholar] [CrossRef]
- Ferlazzo, M.L.; Bourguignon, M.; Foray, N. Functional Assays for Individual Radiosensitivity: A Critical Review. Semin. Radiat. Oncol. 2017, 27, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Barendsen, G.W. Dose fractionation, dose rate and iso-effect relationships for normal tissue responses. Int. J. Radiat. Oncol. Biol. Phys. 1982, 8, 1981–1997. [Google Scholar] [CrossRef]
- Ellis, F. The relationship of biological effect to dose-time fractionation factors in radiotherapy. Curr. Top. Radiat. Res. 1965, 4, 357–397. [Google Scholar]
- Suit, H.; Wette, R. Radiation dose fractionation and tumour control probability. Radiat. Res. 1966, 29, 267–281. [Google Scholar] [CrossRef] [PubMed]
- Goodwin Jinesh, G.; Daniel Levi, W.; Ashish, M.K. Bladder Cancer Stem Cells: Biological and Therapeutic Perspectives. Curr. Stem Cell Res. Ther. 2014, 9, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Seifert, H.-H.; Meyer, A.; Cronauer, M.V.; Hatina, J.; Müller, M.; Rieder, H.; Hoffmann, M.J.; Ackermann, R.; Schulz, W.A. A new and reliable culture system for superficial low-grade urothelial carcinoma of the bladder. World J. Urol. 2007, 25, 297–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overgaard, J.; Horsman, M.R. Modification of hypoxia induced radioresistance in tumors by the use of oxygen and sensitizers. Semin. Radiat. Oncol. 1996, 6, 10–21. [Google Scholar] [CrossRef]
- Rich, J.N. Cancer Stem Cells in Radiation Resistance. Cancer Res. 2007, 67, 8980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DelNero, P.; Lane, M.; Verbridge, S.S.; Kwee, B.; Kermani, P.; Hempstead, B.; Stroock, A.; Fischbach, C. 3D culture broadly regulates tumor cell hypoxia response and angiogenesis via pro-inflammatory pathways. Biomaterials 2015, 55, 110–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thames, H.D.; Wither, H.R.; Peters, L.J.; Fletcher, G. Changes in early and late radiation responses with altered dose fractionation: Implications for dose-survival relationships. Int. J. Radiat. Oncol. Biol. Phys. 1982, 8, 219–226. [Google Scholar] [CrossRef]
- Jones, B.; Dale, R.G.; Deehan, C.; Hopkins, K.I.; Morgan, D.A. The role of biologically effective dose (BED) in clinical oncology. Clin. Oncol. 2001, 13, 71–81. [Google Scholar]
- Maalouf, M.; Granzotto, A.; Devic, C.; Bodgi, L.; Ferlazzo, M.; Peaucelle, C.; Bajard, M.; Giraud, J.Y.; Balosso, J.; Hérault, J.; et al. Influence of Linear Energy Transfer on the Nucleo-shuttling of the ATM Protein: A Novel Biological Interpretation Relevant for Particles and Radiation. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 709–718. [Google Scholar] [CrossRef]
- Pos, F.J.; Hart, G.; Schneider, C.; Sminia, P. Radical radiotherapy for invasive bladder cancer: What dose and fractionation schedule to choose? Int. J. Radiat. Oncol. 2006, 64, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Chamie, K.; Litwin Mark, S.; Bassett Jeffrey, C.; Daskivich Timothy, J.; Lai, J.; Hanley Jan, M.; Konety Badrinath, R.; Saigal Christopher, S. Recurrence of high-risk bladder cancer: A population-based analysis. Cancer 2013, 119, 3219–3227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huddart, R.; McDonald, F.; Hafeez, S.; Warren-Oseni, K.; Taylor, H.; Thompson, A.; Khoo, V.; Harris, V.; McNair, H.; Mohammed, K.; et al. Phase I dose-escalated image-guided adaptive bladder radiotherapy study: Results of first dose cohort (68Gy). J. Clin. Oncol. 2014, 32, 291. [Google Scholar] [CrossRef]
- Murthy, V.; Masodkar, R.; Kalyani, N.; Mahantshetty, U.; Bakshi, G.; Prakash, G.; Joshi, A.; Prabhash, K.; Ghonge, S.; Shrivastava, S. Clinical Outcomes with Dose-Escalated Adaptive Radiation Therapy for Urinary Bladder Cancer: A Prospective Study. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 60–66. [Google Scholar] [CrossRef]
- Fennema, E.; Rivron, N.; Rouwkema, J.; Van Blitterswijk, C.; De Boer, J. Spheroid culture as a tool for creating 3D complex tissues. Trends Biotechnol. 2013, 31, 108–115. [Google Scholar] [CrossRef]
- El Chediak, A.; Shamseddine, A.; Bodgi, L.; Obeid, J.-P.; Geara, F.; Zeidan, Y.H. Optimizing tumor immune response through combination of radiation and immunotherapy. Med. Oncol. 2017, 34, 165. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell Line | Tissue | Disease | Age | Sphere Maturity |
|---|---|---|---|---|
| RT4 | Urinary bladder | Transitional cell papilloma | 63 years | Day 7 |
| UM-UC-3 | Urinary bladder | Transitional cell carcinoma | - | Day 5 |
| T24 | Urinary bladder | Transitional cell carcinoma | 81 years | Day7 |
| Assay | Dose | Treatment Delivery | Endpoint | Equation | |
|---|---|---|---|---|---|
| 2D | Clonogenic Assay | 2 Gy | Single dose, delayed plating | Surviving Fraction | |
| Immunofluorescence: anti-γH2AX | 2 Gy | Single dose | Number of foci 24 h after irradiation | NA | |
| 3D | Spheres assay | 0, 2, 4, 6, 8 and 10 Gy | Single dose: early, mid and late treatment protocols (Figure 1) | SR: Sphere Ratio | |
| VR: Volume Reduction | |||||
| 0, 2, 4, 6, 8 and 10 Gy | Factionated treatment: 2 Gy every 24 h mid treatment protocol (Figure 1) | SR: Sphere Ratio | |||
| VR: Volume Reduction | |||||
| Immunofluorescence: anti-CD44 | 4 Gy | Single dose, early treatment | CD44 expression | NA |
| Condition | α (95% CI) | β (95% CI) | R2 | |
|---|---|---|---|---|
| RT4 | Early | 0.3328 (0.2556, 0.41) | 0 | 0.8 |
| Mid | 0.3572 (0.0815, 0.6328) | 0.0007994 (−0.03194, 0.03354) | 0.92 | |
| Late | 0.04105 (0.019, 0.063) | 0.004094 (0.0014, 0.0067) | 0.99 | |
| DF | 0.2132 (−0.03186, 0.4583) | 0.002836 (−0.02621, 0.03188) | 0.9 | |
| T24 | Early | 0.4772 (0.4525, 0.5) | 0 | 0.99 |
| Mid | 0.4999 (0.2068, 0.7931) | 0 (−0.032, 0.033) | 0.96 | |
| Late | 0.1328 (0.1098, 0.1558) | 0 | 0.9 | |
| DF | 0.176 (−0.03008, 0.3821) | 0.004437 (−0.01999, 0.02886) | 0.9 | |
| UC3 | Early | 0.1682 (0.03079, 0.3057) | 0.005847 (−0.01048, 0.02217) | 0.95 |
| Mid | 0.3572 (0.0815, 0.6328) | 0.0007994 (−0.03194, 0.03354) | 0.92 | |
| Late | 0.1238 (0.01556, 0.232) | 0.003527 (−0.009326, 0.01638) | 0.94 | |
| DF | 0.1061 (−0.001762, 0.214) | 0.004011 (−0.008775, 0.0168) | 0.94 |
| Condition | VRmax (CI 95%) | e (CI 95%) | R2 | |
|---|---|---|---|---|
| RT4 | Early | 45.62 (39.75, 51.49) | 0.5378 (0.2835, 0.7922) | 0.97 |
| Mid | 32.73 (27.55, 37.92) | 0.326 (0.1809, 0.471) | 0.98 | |
| Late | 88.94 (−136, 313.9) | 0.05236 (−0.1112, 0.2159) | 0.94 | |
| DF | 37.69 (21.43, 53.94) | 0.3101 (−0.07377, 0.6939) | 0.9 | |
| T24 | Early | 62.56 (52.29, 72.83) | 0.4551 (0.2019, 0.7083) | 0.96 |
| Mid | 2.06 × 104 (−1.138 × 107, 1.142 × 107) | 0.000421 (−0.233, 0.2338) | 0.88 | |
| Late | 23.9 (18.93, 28.87) | 1.566 (−0.5936, 3.725) | 0.85 | |
| DF | 59.42 (19.33, 99.52) | 0.2845 (−0.233, 0.8021) | 0.81 |
| RT4 | T-24 | UM-UC3 | ||||
|---|---|---|---|---|---|---|
| 2D Assays | Clonogenic Assay SF (2 Gy) | 64.8 ± 7% | 57 ± 9% | 31 ± 7.3% | ||
| Residual γH2AX foci (2 Gy) | 3 ± 0.8 foci | 4 ± 0.5 foci | 5.7 ± 0.6 foci | |||
| Sphere Ratio | Early Treatment | SR(2 Gy) | 0.22 ± 0.04 | 0.49 ± 0.07 | 0.79 ± 0.05 | |
| SR(8 Gy) | 0.07 ± 0.01 | 0.02 ± 0.01 | 0.13 ± 0.02 | |||
| Mid Treatment | SR(2 Gy) | 0.41 ± 0.04 | 0.47 ± 0.06 | 0.62 ± 0.08 | ||
| SR(8 Gy) | 0.09 ± 0.05 | 0.01 ± 0.00 | 0.07 ± 0.015 | |||
| Late Treatment | SR(2 Gy) | 0.41 ± 0.04 | 0.65 ± 0.02 | 0.66 ± 0.07 | ||
| SR(8 Gy) | 0.56 ± 0.05 | 0.33 ± 0.04 | 0.27 ± 0.05 | |||
| DF treatment | SR(2 Gy) | 0.41 ± 0.04 | 0.47± 0.07 | 0.62 ± 0.08 | ||
| SR(8 Gy) | 0.22 ± 0.04 | 0.25 ± 0.016 | 35 ± 0.09 | |||
| Volume Reduction | Early Treatment | SR(2 Gy) | 28 ±8.4% | 37.25 ± 6% | Not applicable | |
| SR(8 Gy) | 50 ± 3.3% | 65 ± 1.5% | Not applicable | |||
| Mid Treatment | SR(2 Gy) | 18.5±3.5% | 27.5 ± 2.6% | Not applicable | ||
| SR(8 Gy) | 29.1 ± 0.26% | 52.9 ± 5.2% | Not applicable | |||
| Late Treatment | SR(2 Gy) | 12.1 ± 3.5% | 24.2 ± 3% | Not applicable | ||
| SR(8 Gy) | 33.5 ± 3.9% | 28 ± 3% | Not applicable | |||
| DF Treatment | SR(2 Gy) | 18.5 ± 3.5% | 27.5 ± 2.6% | Not applicable | ||
| SR(8 Gy) | 31.8 ± 2.6% | 57 ± 2.8% | Not applicable | |||
| CD44 Expression | 0 Gy | 76 ± 10% | 50 ± 2% | 64 ± 6% | ||
| 4 Gy | 36 ± 2.4% | 76.8 ± 5% | 24.5 ± 3% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bodgi, L.; Al-Choboq, J.; Araji, T.; Bou-Gharios, J.; Azzi, J.; Challita, R.; Feghaly, C.; Bahmad, H.F.; Eid, T.; Geara, F.; et al. Radiation Treatment Timing and Dose Delivery: Effects on Bladder Cancer Cells in 3D in Vitro Culture. Radiation 2022, 2, 318-337. https://doi.org/10.3390/radiation2040025
Bodgi L, Al-Choboq J, Araji T, Bou-Gharios J, Azzi J, Challita R, Feghaly C, Bahmad HF, Eid T, Geara F, et al. Radiation Treatment Timing and Dose Delivery: Effects on Bladder Cancer Cells in 3D in Vitro Culture. Radiation. 2022; 2(4):318-337. https://doi.org/10.3390/radiation2040025
Chicago/Turabian StyleBodgi, Larry, Joelle Al-Choboq, Tarek Araji, Jolie Bou-Gharios, Joyce Azzi, Rafka Challita, Charbel Feghaly, Hisham F. Bahmad, Toufic Eid, Fady Geara, and et al. 2022. "Radiation Treatment Timing and Dose Delivery: Effects on Bladder Cancer Cells in 3D in Vitro Culture" Radiation 2, no. 4: 318-337. https://doi.org/10.3390/radiation2040025