
BRAF and MLH1 Analysis Algorithm for the Evaluation of Lynch Syndrome Risk in Colorectal Carcinoma Patients: Evidence-Based Data from the Analysis of 100 Consecutive Cases

 , , , ,
, , , ,  , , and
, , and
Abstract
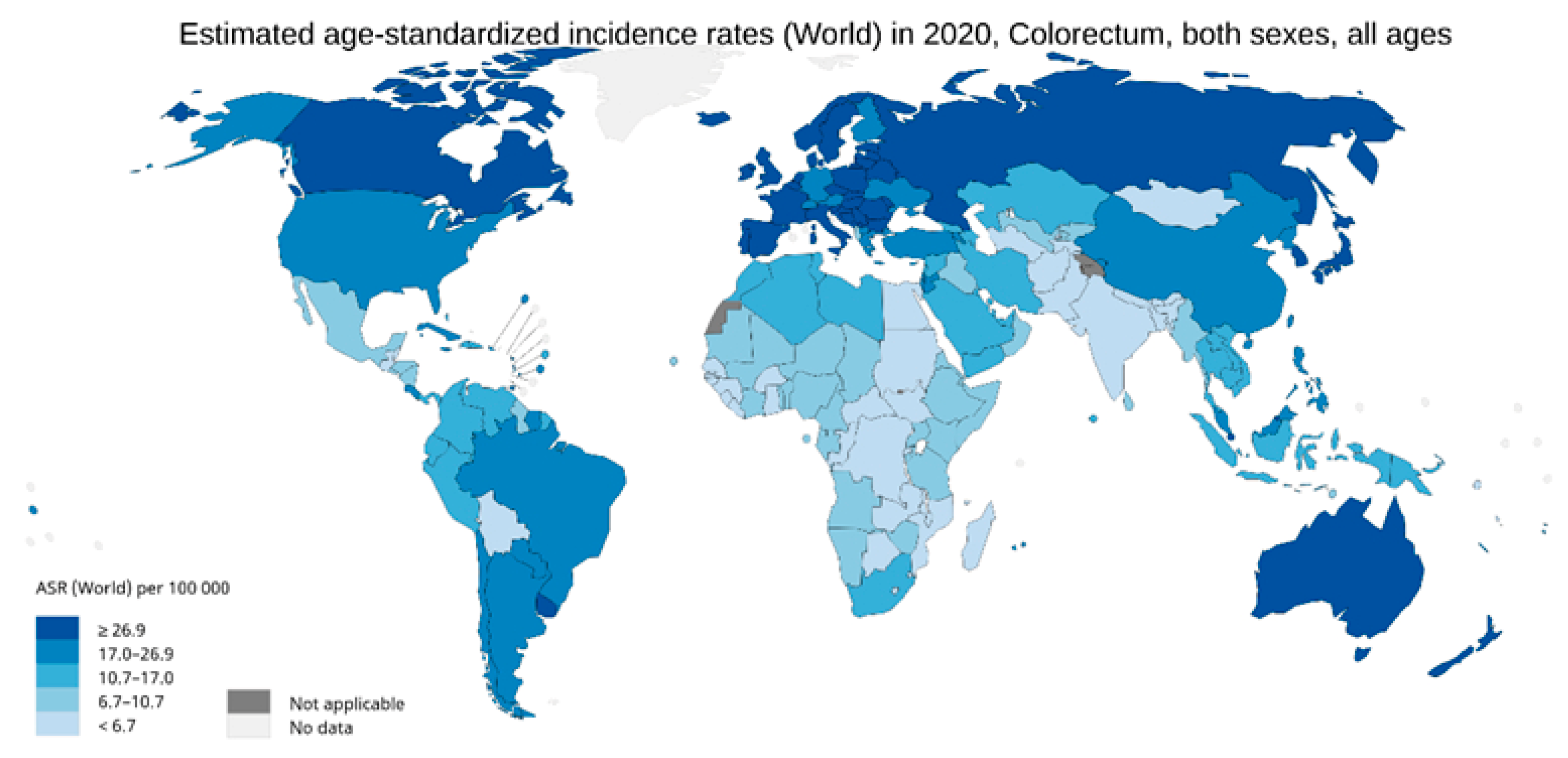
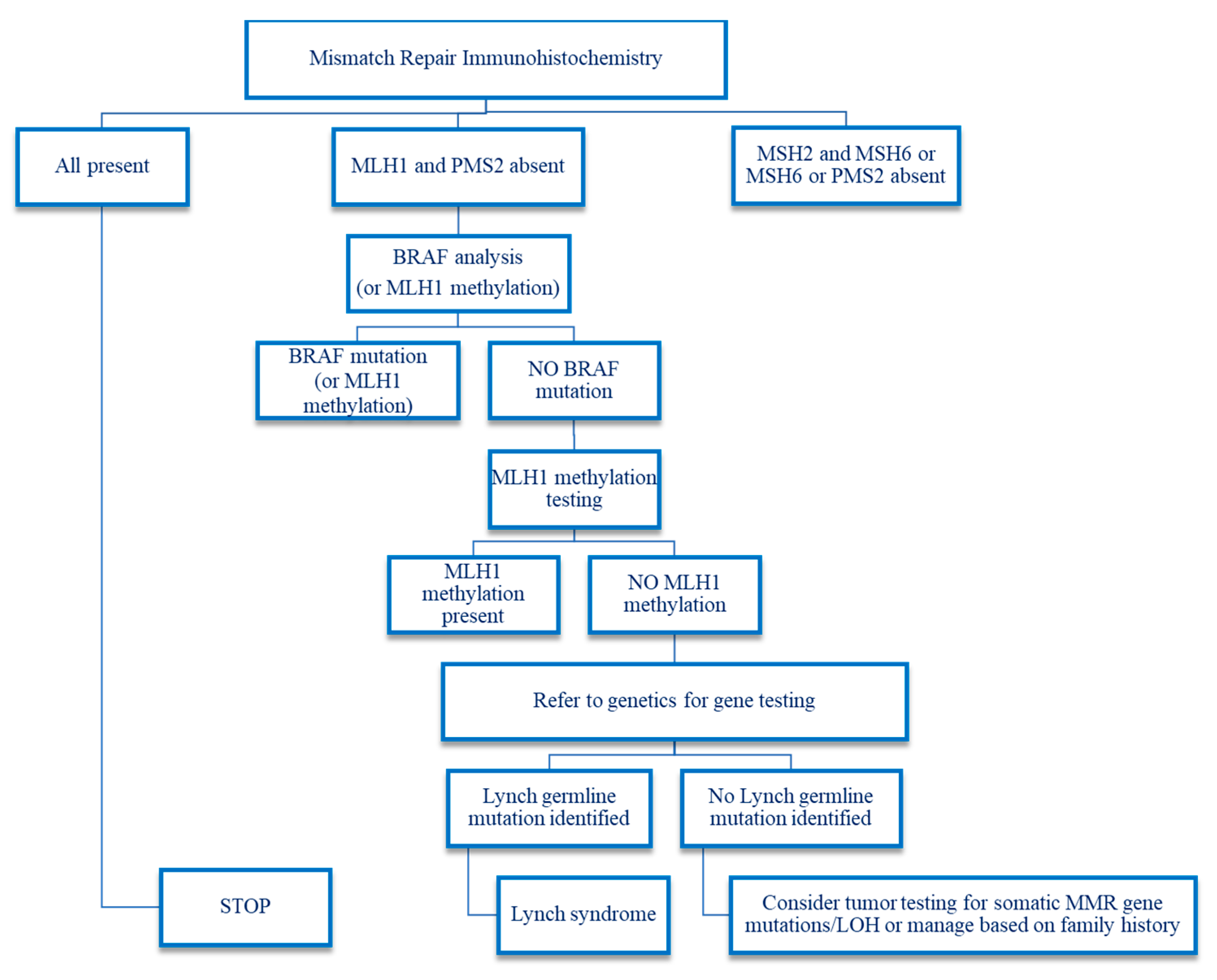
:1. Introduction
2. Materials and Methods
2.1. Case Selection
2.2. DNA Extraction and Quantification
2.3. BRAF Analysis
2.4. MLH1 Promoter Methylation Analysis
3. Results
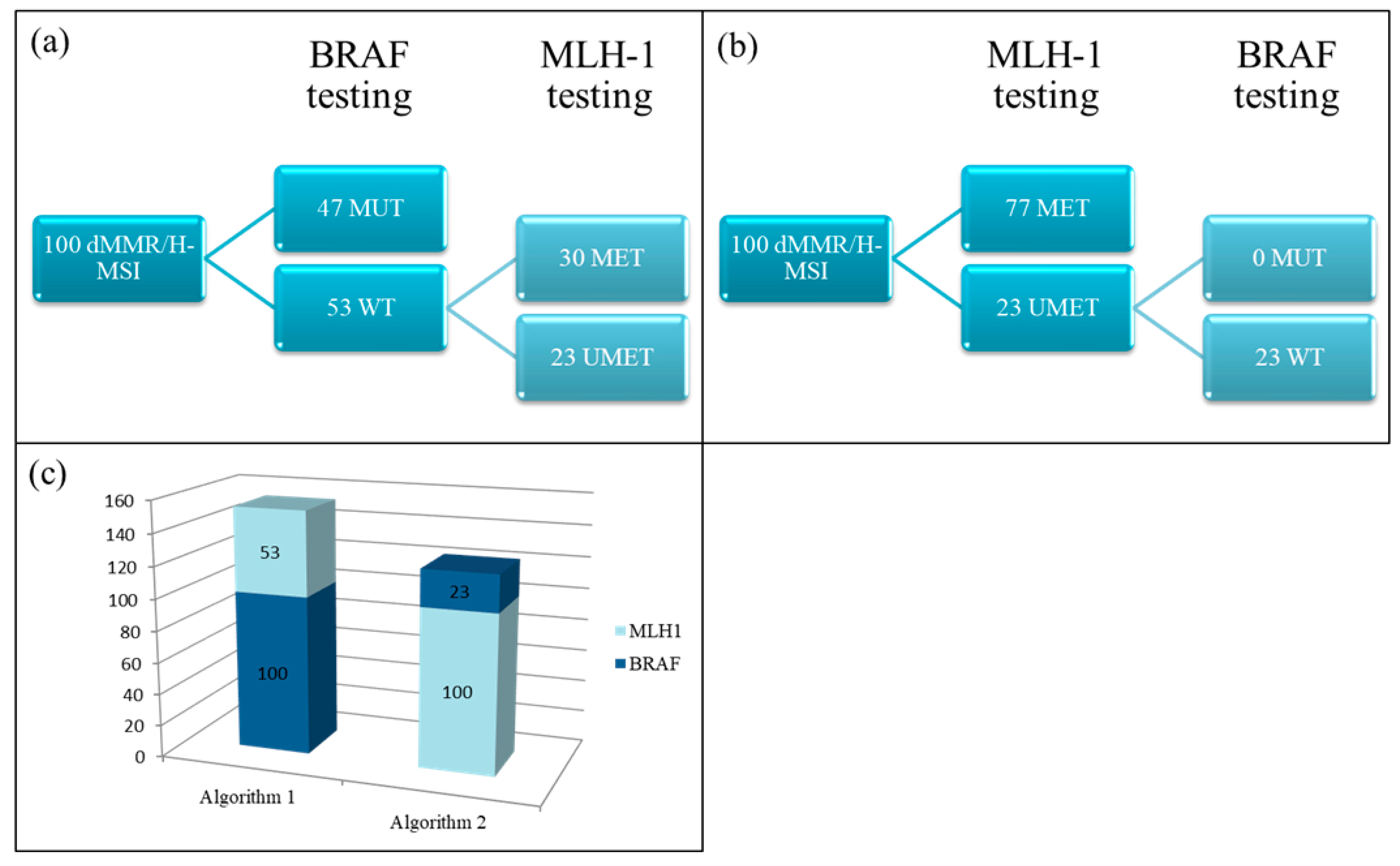
3.1. BRAF Analysis
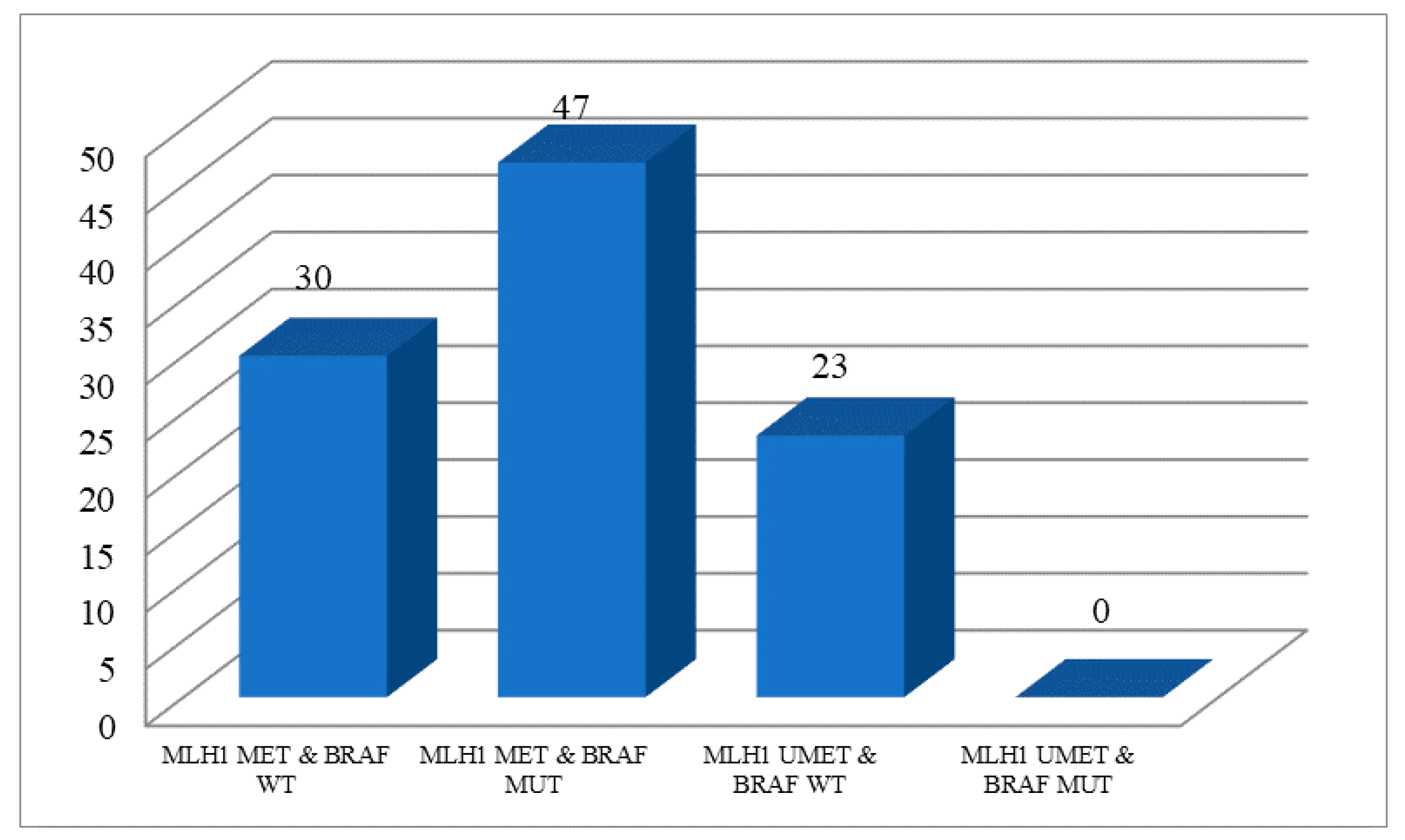
3.2. MLH1 Methylation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Prz. Gastroenterol. 2019, 14, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today (accessed on 15 January 2022).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Institute, N.C. Cancer Stat Facts: Colorectal Cancer. Available online: https://seer.cancer.gov/statfacts/html/colorect.html (accessed on 20 January 2022).
- Adam, M.P.; Ardinger, H.H.; Pagon, R.A.; Wallace, S.E.; Bean, L.J.H.; Gripp, K.W.; Mirzaa, G.M.; Amemiya, A. GeneReviews; University of Wahington: Seattle, WA, USA, 1993. [Google Scholar]
- Hsieh, P.; Yamane, K. DNA mismatch repair: Molecular mechanism, cancer, and ageing. Mech. Ageing Dev. 2008, 129, 391–407. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, J.M.; Christensen, E.R.; Tester, D.J.; Kim, C.Y.; Roche, P.C.; Burgart, L.J.; Thibodeau, S.N. Hypermethylation of the hMLH1 promoter in colon cancer with microsatellite instability. Cancer Res. 1998, 58, 3455–3460. [Google Scholar]
- Menahem, B.; Alves, A.; Regimbeau, J.M.; Sabbagh, C. Lynch Syndrome: Current management In 2019. J. Visc. Surg. 2019, 156, 507–514. [Google Scholar] [CrossRef]
- Sun, B.L. Current Microsatellite Instability Testing in Management of Colorectal Cancer. Clin. Colorectal. Cancer 2021, 20, e12–e20. [Google Scholar] [CrossRef]
- Fishel, R. Mismatch repair. J. Biol. Chem. 2015, 290, 26395–26403. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Provenzale, D.; Llor, X.; Halverson, A.L.; Grady, W.; Chung, D.C.; Haraldsdottir, S.; Markowitz, A.J.; Slavin, T.P.; Hampel, H.; et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Colorectal, Version 2.2019. J. Natl. Compr. Canc. Netw. 2019, 17, 1032–1041. [Google Scholar] [CrossRef] [Green Version]
- Battaglin, F.; Naseem, M.; Lenz, H.J.; Salem, M.E. Microsatellite instability in colorectal cancer: Overview of its clinical significance and novel perspectives. Clin. Adv. Hematol. Oncol. 2018, 16, 735–745. [Google Scholar]
- Kishore, C.; Bhadra, P. Current advancements and future perspectives of immunotherapy in colorectal cancer research. Eur. J. Pharmacol. 2021, 893, 173819. [Google Scholar] [CrossRef]
- Popat, S.; Hubner, R.; Houlston, R.S. Systematic review of microsatellite instability and colorectal cancer prognosis. J. Clin. Oncol. 2005, 23, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Hampel, H.; Frankel, W.L.; Martin, E.; Arnold, M.; Khanduja, K.; Kuebler, P.; Clendenning, M.; Sotamaa, K.; Prior, T.; Westman, J.A.; et al. Feasibility of screening for Lynch syndrome among patients with colorectal cancer. J. Clin. Oncol. 2008, 26, 5783–5788. [Google Scholar] [CrossRef] [PubMed]
- Cerretelli, G.; Ager, A.; Arends, M.J.; Frayling, I.M. Molecular pathology of Lynch syndrome. J. Pathol. 2020, 250, 518–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lièvre, A.; de la Fouchardière, C.; Samalin, E.; Benoist, S.; Phelip, J.M.; André, T.; Lledo, G. BRAF V600E-mutant colorectal cancers: Where are we? Bull. Cancer 2020, 107, 881–895. [Google Scholar] [CrossRef]
- Bläker, H.; Haupt, S.; Morak, M.; Holinski-Feder, E.; Arnold, A.; Horst, D.; Sieber-Frank, J.; Seidler, F.; von Winterfeld, M.; Alwers, E.; et al. Age-dependent performance of BRAF mutation testing in Lynch syndrome diagnostics. Int. J. Cancer 2020, 147, 2801–2810. [Google Scholar] [CrossRef]
- Snowsill, T.; Coelho, H.; Huxley, N.; Jones-Hughes, T.; Briscoe, S.; Frayling, I.M.; Hyde, C. Molecular testing for Lynch syndrome in people with colorectal cancer: Systematic reviews and economic evaluation. Health Technol. Assess. 2017, 21, 1–238. [Google Scholar] [CrossRef] [Green Version]
- Syngal, S.; Brand, R.E.; Church, J.M.; Giardiello, F.M.; Hampel, H.L.; Burt, R.W.; Gastroenterology, A.C.O. ACG clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am. J. Gastroenterol. 2015, 110, 223–262, quiz 263. [Google Scholar] [CrossRef] [Green Version]
- Hampel, H. NCCN increases the emphasis on genetic/familial high-risk assessment in colorectal cancer. J. Natl. Compr. Cancer Netw. 2014, 12, 829–831. [Google Scholar] [CrossRef]
- Giardiello, F.M.; Allen, J.I.; Axilbund, J.E.; Boland, C.R.; Burke, C.A.; Burt, R.W.; Church, J.M.; Dominitz, J.A.; Johnson, D.A.; Kaltenbach, T.; et al. Guidelines on genetic evaluation and management of Lynch syndrome: A consensus statement by the US Multi-Society Task Force on colorectal cancer. Gastroenterology 2014, 147, 502–526. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Frankel, W.L. A practical guide to biomarkers for the evaluation of colorectal cancer. Mod. Pathol. 2019, 32, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Network, N.C.C. NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High Risk Assesment: Colorectal. Available online: https://www.nccn.org/professionals/physician_gls/pdf/genetics_colon.pdf (accessed on 21 January 2022).
- de Biase, D.; Acquaviva, G.; Visani, M.; Sanza, V.; Argento, C.M.; De Leo, A.; Maloberti, T.; Pession, A.; Tallini, G. Molecular Diagnostic of Solid Tumor Using a Next Generation Sequencing Custom-Designed Multi-Gene Panel. Diagnostics 2020, 10, 250. [Google Scholar] [CrossRef] [PubMed]
- Yurgelun, M.B.; Hampel, H. Recent Advances in Lynch Syndrome: Diagnosis, Treatment, and Cancer Prevention. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 101–109. [Google Scholar] [CrossRef]
- Kuismanen, S.A.; Holmberg, M.T.; Salovaara, R.; de la Chapelle, A.; Peltomäki, P. Genetic and epigenetic modification of MLH1 accounts for a major share of microsatellite-unstable colorectal cancers. Am. J. Pathol. 2000, 156, 1773–1779. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Cunningham, J.M.; Winters, J.L.; Guenther, J.C.; French, A.J.; Boardman, L.A.; Burgart, L.J.; McDonnell, S.K.; Schaid, D.J.; Thibodeau, S.N. BRAF mutations in colon cancer are not likely attributable to defective DNA mismatch repair. Cancer Res. 2003, 63, 5209–5212. [Google Scholar] [PubMed]
- Xiao, B.; Luo, J.; Xie, E.; Kong, L.; Tang, J.; Liu, D.; Mao, L.; Sui, Q.; Li, W.; Hong, Z.; et al. Comparisons of screening strategies for identifying Lynch syndrome among patients with MLH1-deficient colorectal cancer. Eur. J. Hum. Genet. 2020, 28, 1555–1562. [Google Scholar] [CrossRef]
- Newton, K.; Jorgensen, N.M.; Wallace, A.J.; Buchanan, D.D.; Lalloo, F.; McMahon, R.F.; Hill, J.; Evans, D.G. Tumour MLH1 promoter region methylation testing is an effective prescreen for Lynch Syndrome (HNPCC). J. Med. Genet. 2014, 51, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Adar, T.; Rodgers, L.H.; Shannon, K.M.; Yoshida, M.; Ma, T.; Mattia, A.; Lauwers, G.Y.; Iafrate, A.J.; Chung, D.C. A tailored approach to BRAF and MLH1 methylation testing in a universal screening program for Lynch syndrome. Mod. Pathol. 2017, 30, 440–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, A.; McCracken, J.; Li, Y.; Xu, L. The practice of universal screening for Lynch syndrome in newly diagnosed endometrial carcinoma. Health Sci. Rep. 2018, 1, e43. [Google Scholar] [CrossRef]
- Evans, D.G.; Lalloo, F.; Ryan, N.A.; Bowers, N.; Green, K.; Woodward, E.R.; Clancy, T.; Bolton, J.; McVey, R.J.; Wallace, A.J.; et al. Advances in genetic technologies result in improved diagnosis of mismatch repair deficiency in colorectal and endometrial cancers. J. Med. Genet. 2022, 59, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.O. Precision treatment in colorectal cancer: Now and the future. JGH Open 2019, 3, 361–369. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| dMMR/MSI-H Samples | N° (Frequency) |
|---|---|
| BRAF MUT | 47 (47.0%) |
| BRAF MUT & MLH1 MET | 47 (100.0%) |
| BRAF MUT & MLH1 UMET | 0 (/) |
| BRAF WT | 53 (53.0%) |
| BRAF WT & MLH1 MET | 30 (56.6%) |
| BRAF WT & MLH1 UMET | 23 (43.4) |
| TOTAL | 100 |
| dMMR/MSI-H Samples | N° (Frequency) |
|---|---|
| MLH1 MET | 77 (77.0%) |
| MLH1 MET & BRAF WT | 30 (39.0%) |
| MLH1 MET & BRAF MUT | 47 (61%) |
| MLH1 UMET | 23 (23.0%) |
| MLH1 UMET & BRAF WT | 23 (100%) |
| MLH1 UMET & BRAF MUT | 0 (/) |
| TOTAL | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maloberti, T.; De Leo, A.; Sanza, V.; Merlo, L.; Visani, M.; Acquaviva, G.; Coluccelli, S.; Altimari, A.; Gruppioni, E.; Zagnoni, S.; et al. BRAF and MLH1 Analysis Algorithm for the Evaluation of Lynch Syndrome Risk in Colorectal Carcinoma Patients: Evidence-Based Data from the Analysis of 100 Consecutive Cases. J. Mol. Pathol. 2022, 3, 115-124. https://doi.org/10.3390/jmp3030011
Maloberti T, De Leo A, Sanza V, Merlo L, Visani M, Acquaviva G, Coluccelli S, Altimari A, Gruppioni E, Zagnoni S, et al. BRAF and MLH1 Analysis Algorithm for the Evaluation of Lynch Syndrome Risk in Colorectal Carcinoma Patients: Evidence-Based Data from the Analysis of 100 Consecutive Cases. Journal of Molecular Pathology. 2022; 3(3):115-124. https://doi.org/10.3390/jmp3030011
Chicago/Turabian StyleMaloberti, Thais, Antonio De Leo, Viviana Sanza, Lidia Merlo, Michela Visani, Giorgia Acquaviva, Sara Coluccelli, Annalisa Altimari, Elisa Gruppioni, Stefano Zagnoni, and et al. 2022. "BRAF and MLH1 Analysis Algorithm for the Evaluation of Lynch Syndrome Risk in Colorectal Carcinoma Patients: Evidence-Based Data from the Analysis of 100 Consecutive Cases" Journal of Molecular Pathology 3, no. 3: 115-124. https://doi.org/10.3390/jmp3030011