
Impact of Indoor Air Pollution in Pakistan—Causes and Management


Abstract
:
1. Introduction
2. Indoor Air Pollution
3. Sources and Key Indoor Air Pollutants in Pakistan
3.1. Indoor Particulate Matter and Dust Ingestion
3.2. Indoor Smoke, COx, VOC, and Pollutants from Household Energy Sources, Tobacco, and Building Materials
3.3. Bioaerosols and Airborne Microflora in Residential Environments
3.4. Low-Temperature Health Hazards
4. Indoor Air Effluence Threats
4.1. Major Health Hazards of Indoor Air Contamination
4.2. Impact of Interior Physical Environment on Productivity of Indoor Workers/Academicians
4.3. Indoor Pollution in Hospital Environment
5. Harmful Effects of the Indoor Pollution
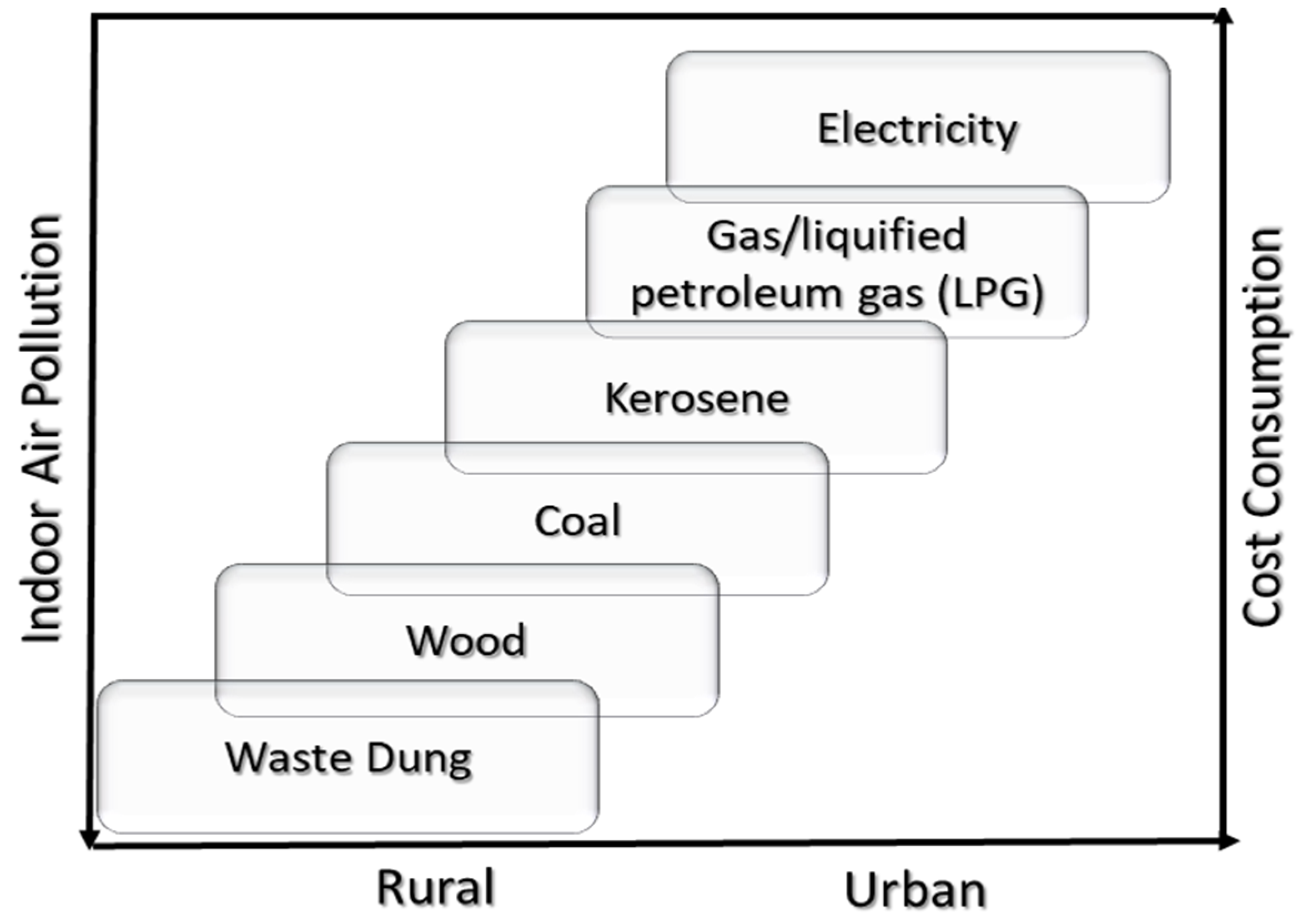
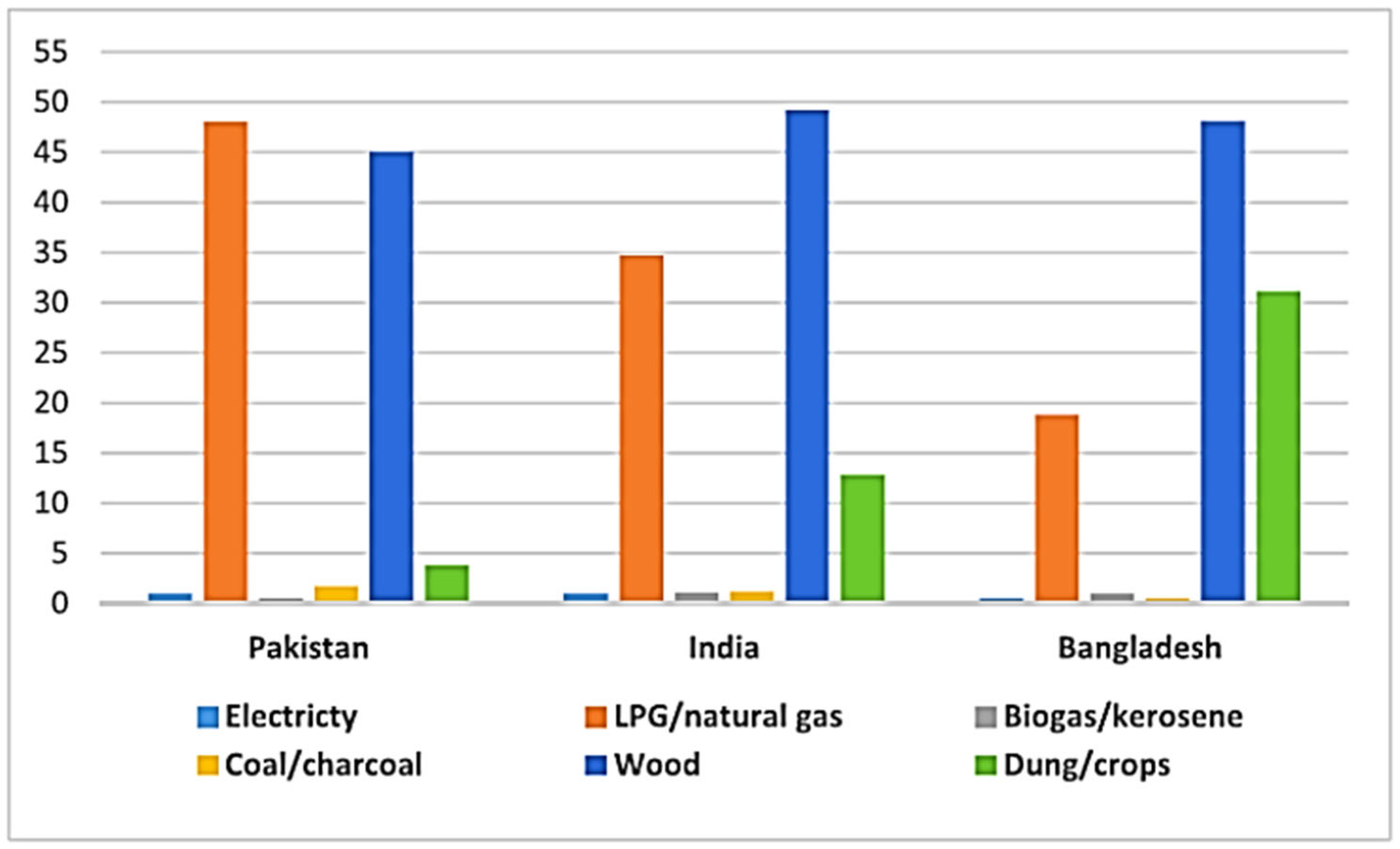
- Around 2.4 billion people worldwide (i.e., one-third of the global population) use open fires and stoves fueled by the biomass (wood, animal dung, crop, etc.), coal, and kerosene for cooking. These burning activities produce several harmful indoor air pollutants [181].
- The indoor air pollution has been responsible for >4 million deaths per year, including over 2 million deaths of children (under 5 years) [20].
- The effects of indoor pollution were observed in the form of >6 million premature deaths per annum [20].
- Women and children seem to be more influenced by indoor cooking activities, which have caused great health effects [184].
- The Environmental Protection Agency (EPA) refers to the IAQ within and around buildings. According to the EPA, the indoor pollution can cause major environmental risks to the public health. The common indoor pollutants include CO, radon, pests, dust, mites, lead, smoke, bacteria, bioaerosols, etc., in addition to the increased humidity and precipitation levels.
- The indoor pollutants have caused short term effects such as eye irritation, nasal itching, throat rashes, headaches, fatigue, dizziness, asthma symptoms, etc. However, the long-term effects due to chronic exposure to indoor pollutants include the respiratory/heart diseases, as well as cancer effects.
- According to a careful estimate, acute lung cancer risks of ~6% have been reported in the adult population due to unhealthy fuel usage [157].
- According to a study in Pakistan, using unhealthy indoor fuels and living rooms with attached kitchens produced a child mortality rate of about 145 deaths/1000 live births [103]. On the other hand, houses using clean fuel or separate kitchens have ~10 deaths/1000 live births. Moreover, up to 80 deaths/1000 women have been reported because of indoor kitchen fuels [185]. Comparatively, the male population was found to be less affected.
- In this concern, using clean fuels and safe indoor burning sources can reduce the indoor pollution to protect from health hazards. As per the WHO guidelines, safe fuels include solar energy, electricity, biogas, natural gas, and liquefied petroleum gas, which minimize the environmental pollution [186].
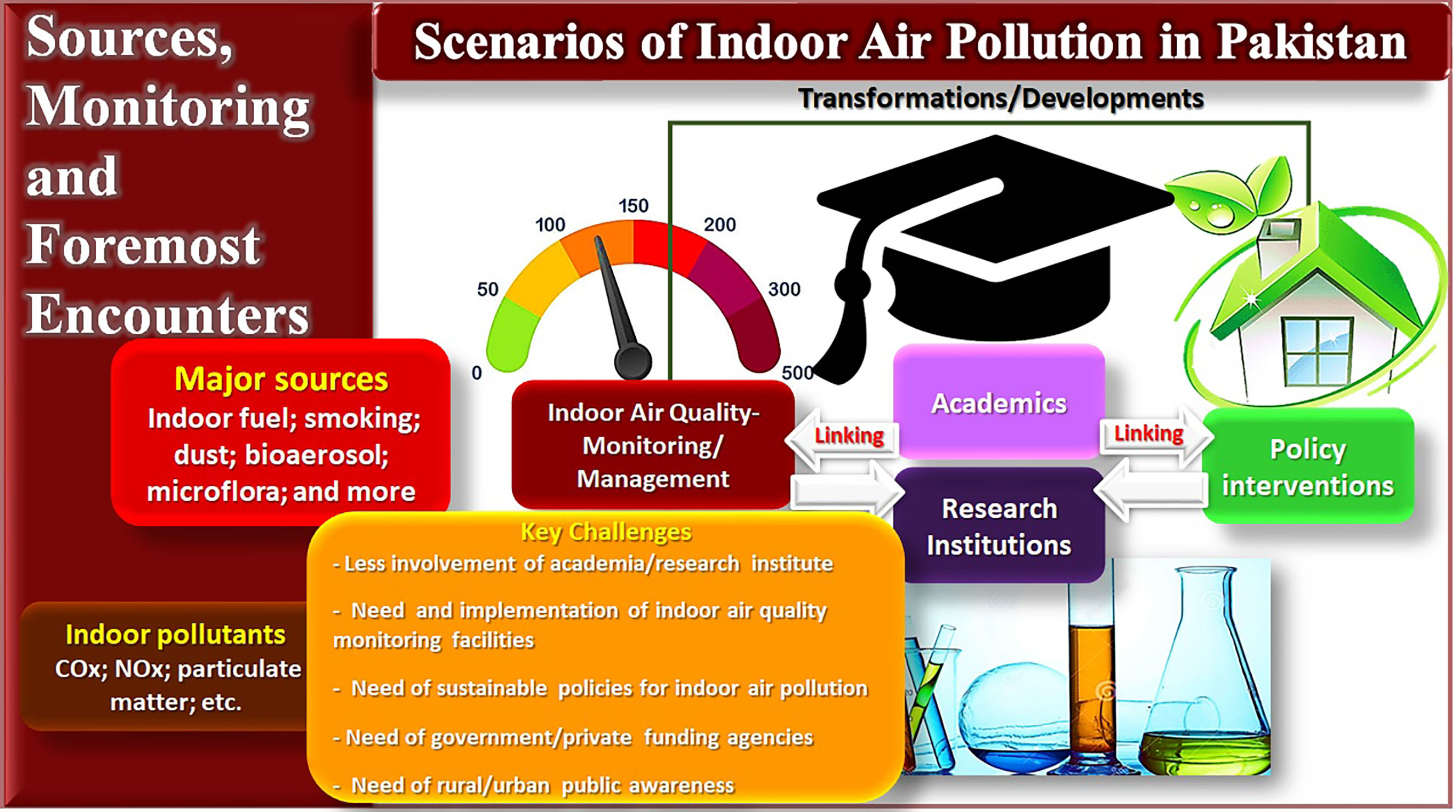
6. Indoor Air Quality Management and Challenges on Monitoring/Regulating IAQ in Pakistan
7. Need of Industry–Academia–Research Cooperation to Support Indoor Air Pollution Control
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kausar, A.; Ahmad, I.; Zhu, T.; Shahzad, H.; Eisa, M. Exigency for the Control and Upgradation of Indoor Air Quality—Forefront Advancements Using Nanomaterials. Pollutants 2023, 3, 123–149. [Google Scholar] [CrossRef]
- Zeng, Y.; Laguerre, A.; Gall, E.T.; Heidarinejad, M.; Stephens, B. Experimental Evaluations of the Impact of an Additive Oxidizing Electronic Air Cleaner on Particles and Gases. Pollutants 2022, 2, 98–134. [Google Scholar] [CrossRef]
- Dwivedi, S.; Taushiba, A.; Zehra, F.; Gupta, S.K.; Lawrence, A. Revelations to Indoor Air Pollutants and Health Risk Assessment on Women: A case study. Hyg. Environ. Health Adv. 2022, 5, 100038. [Google Scholar] [CrossRef]
- Amen, N.-E.; Eqani, S.A.M.A.S.; Bilal, K.; Ali, N.; Rajeh, N.; Adelman, D.; Shen, H.; Lohmann, R. Molecularly tracing of children exposure pathways to environmental organic pollutants and the Autism Spectrum Disorder Risk. Environ. Pollut. 2022, 315, 120381. [Google Scholar] [CrossRef]
- Imran, M.; Khan, S.; Nassani, A.A.; Haffar, M.; Zaman, K. Access to sustainable healthcare infrastructure: A review of industrial emissions, coal fires, and particulate matter. Environ. Sci. Pollut. Res. 2023, 30, 69080–69095. [Google Scholar] [CrossRef]
- Khan, W.A.; Shah, S.A.; Khan, A. In Pakistan, the Transport and Urban Air Pollution Impacts on Human Health and Practical Steps to Avoid Them: A Review. J. Int. Coop. Dev. 2022, 5, 20. [Google Scholar] [CrossRef]
- Udaipurwala, I.H. Air Pollution and Health Hazards: A Menacing Situation in Pakistan. J. Bahria Univ. Med. Dent. Coll. 2022, 12, 66–67. [Google Scholar] [CrossRef]
- Imran, M.; Khan, S.; Zaman, K.; Khan, H.U.R.; Rashid, A. Assessing Green Solutions for Indoor and Outdoor Environmental Quality: Sustainable Development Needs Renewable Energy Technology. Atmosphere 2022, 13, 1904. [Google Scholar] [CrossRef]
- Lolli, F.; Marinello, S.; Coruzzolo, A.M.; Butturi, M.A. Post-Occupancy Evaluation’s (POE) Applications for Improving Indoor Environment Quality (IEQ). Toxics 2022, 10, 626. [Google Scholar] [CrossRef]
- Lolli, F.; Coruzzolo, A.M.; Marinello, S.; Traini, A.; Gamberini, R. A Bibliographic Analysis of Indoor Air Quality (IAQ) in Industrial Environments. Sustainability 2022, 14, 10108. [Google Scholar] [CrossRef]
- Kausar, A. Progress in green nanocomposites for high-performance applications. Mater. Res. Innov. 2021, 25, 53–65. [Google Scholar] [CrossRef]
- Kausar, A.; Ahmad, I.; Maaza, M.; Eisa, M.; Bocchetta, P. Polymer/Fullerene Nanocomposite for Optoelectronics—Moving toward Green Technology. J. Compos. Sci. 2022, 6, 393. [Google Scholar] [CrossRef]
- Kausar, A.; Ahmad, I.; Maaza, M.; Eisa, M. State-of-the-Art Nanoclay Reinforcement in Green Polymeric Nanocomposite: From Design to New Opportunities. Minerals 2022, 12, 1495. [Google Scholar] [CrossRef]
- Hou, S.; Tang, Y.; Zhu, T.; Huang, Z.-H.; Liu, Y.; Sun, Y.; Li, X.; Shen, F. The molecular simulation and experimental investigation of toluene and naphthalene adsorption on ordered porous silica. Chem. Eng. J. 2022, 435, 134844. [Google Scholar] [CrossRef]
- Hou, S.; Tang, Y.; Zhu, T.; Huang, Z.-H.; Liu, Y.; Sun, Y.; Li, X.; Shen, F. Adsorptive removal of gas phase naphthalene on ordered mesoporous carbon. J. Hazard. Mater. 2022, 436, 129208. [Google Scholar] [CrossRef]
- Hou, S.; He, S.; Zhu, T.; Li, J.; Ma, L.; Du, H.; Shen, W.; Kang, F.; Huang, Z.-H. Environment-friendly preparation of exfoliated graphite and functional graphite sheets. J. Mater. 2021, 7, 136–145. [Google Scholar] [CrossRef]
- Mata, T.M.; Martins, A.A.; Calheiros, C.S.; Villanueva, F.; Alonso-Cuevilla, N.P.; Gabriel, M.F.; Silva, G.V. Indoor Air Quality: A Review of Cleaning Technologies. Environments 2022, 9, 118. [Google Scholar] [CrossRef]
- Colbeck, I.; Nasir, Z.A.; Ali, Z. The state of indoor air quality in Pakistan—A review. Environ. Sci. Pollut. Res. 2010, 17, 1187–1196. [Google Scholar] [CrossRef]
- Pluschke, P.; Schleibinger, H. Indoor Air Pollution; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Amegah, A.K.; Jaakkola, J.J. Household air pollution and the sustainable development goals. Bull. World Health Organ. 2016, 94, 215. [Google Scholar] [CrossRef]
- Mata, T.M.; Felgueiras, F.; Martins, A.A.; Monteiro, H.; Ferraz, M.P.; Oliveira, G.M.; Gabriel, M.F.; Silva, G.V. Indoor air quality in elderly centers: Pollutants emission and health effects. Environments 2022, 9, 86. [Google Scholar] [CrossRef]
- Peng, Z.; Deng, W.; Tenorio, R. Investigation of indoor air quality and the identification of influential factors at primary schools in the North of China. Sustainability 2017, 9, 1180. [Google Scholar] [CrossRef]
- Liang, J. Chemical Modeling for Air Resources: Fundamentals, Applications, and Corroborative Analysis; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Gopalakrishnan, P.; Kavinraj, M.; Vivekanadhan; Jeevitha, N. Effect of Indoor Air Quality on Human Health—A Review; AIP Publishing LLC: New York, NY, USA, 2021; p. 030005. [Google Scholar]
- Norris, C.L.; Edwards, R.; Ghoroi, C.; Schauer, J.J.; Black, M.; Bergin, M.H. A pilot study to quantify volatile organic compounds and their sources inside and outside homes in urban India in summer and winter during normal daily activities. Environments 2022, 9, 75. [Google Scholar] [CrossRef]
- Li, C.; Zhu, Q.; Jin, X.; Cohen, R.C. Elucidating Contributions of Anthropogenic Volatile Organic Compounds and Particulate Matter to Ozone Trends over China. Environ. Sci. Technol. 2022, 56, 12906–12916. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Xu, H.; Qi, B.; Du, R.; Gui, K.; Wang, H.; Jiang, W.; Liang, L.; Xu, W. Characterization of atmospheric trace gases and particulate matter in Hangzhou, China. Atmos. Chem. Phys. 2018, 18, 1705–1728. [Google Scholar] [CrossRef]
- Villanueva, F.; Ródenas, M.; Ruus, A.; Saffell, J.; Gabriel, M.F. Sampling and analysis techniques for inorganic air pollutants in indoor air. Appl. Spectrosc. Rev. 2022, 57, 531–579. [Google Scholar] [CrossRef]
- Zhu, Y.; Wei, Z.; Yang, X.; Tao, S.; Zhang, Y.; Shangguan, W. Comprehensive control of PM 2.5 capture and ozone emission in two-stage electrostatic precipitators. Sci. Total Environ. 2022, 858, 159900. [Google Scholar] [CrossRef]
- Andersen, C.; Omelekhina, Y.; Rasmussen, B.B.; Nygaard Bennekov, M.; Skov, S.N.; Køcks, M.; Wang, K.; Strandberg, B.; Mattsson, F.; Bilde, M. Emissions of soot, PAHs, ultrafine particles, NOx, and other health relevant compounds from stressed burning of candles in indoor air. Indoor Air 2021, 31, 2033–2048. [Google Scholar] [CrossRef]
- Kureshi, R.R.; Thakker, D.; Mishra, B.K.; Ahmed, B. Use Case of Building an Indoor Air Quality Monitoring System. In Use Case of Building an Indoor Air Quality Monitoring System; IEEE: Piscataway, NJ, USA, 2021; pp. 747–752. [Google Scholar]
- Mehmood, T.; Zhu, T.; Ahmad, I.; Li, X. Ambient PM2. 5 and PM10 bound PAHs in Islamabad, Pakistan: Concentration, source and health risk assessment. Chemosphere 2020, 257, 127187. [Google Scholar] [CrossRef]
- Chen, Y.; Lv, D.; Li, X.; Zhu, T. PM2. 5-bound phthalates in indoor and outdoor air in Beijing: Seasonal distributions and human exposure via inhalation. Environ. Pollut. 2018, 241, 369–377. [Google Scholar] [CrossRef]
- Han, Y.; Li, X.; Zhu, T.; Lv, D.; Chen, Y.; Hou La Zhang, Y.; Ren, M. Characteristics and relationships between indoor and outdoor PM2. 5 in Beijing: A residential apartment case study. Aerosol Air Qual. Res. 2016, 16, 2386–2395. [Google Scholar] [CrossRef]
- Sá, J.P.; Branco, P.T.; Alvim-Ferraz, M.C.; Martins, F.G.; Sousa, S.I. Radon in Indoor Air: Towards Continuous Monitoring. Sustainability 2022, 14, 1529. [Google Scholar] [CrossRef]
- López, L.; Dessì, P.; Cabrera-Codony, A.; Rocha-Melogno, L.; Kraakman, B.; Naddeo, V.; Balaguer, M.; Puig, S. CO2 in indoor environments: From environmental and health risk to potential renewable carbon source. Sci. Total Environ. 2022, 856, 159088. [Google Scholar] [CrossRef]
- Ubando, A.T.; Africa, A.D.M.; Maniquiz-Redillas, M.C.; Culaba, A.B.; Chen, W.-H. Reduction of particulate matter and volatile organic compounds in biorefineries: A state-of-the-art review. J. Hazard. Mater. 2021, 403, 123955. [Google Scholar] [CrossRef]
- Zhang, Y.; Shen, F.; Yang, Y.; Niu, M.; Chen, D.; Chen, L.; Wang, S.; Zheng, Y.; Sun, Y.; Zhou, F. Insights into the Profile of the Human Expiratory Microbiota and Its Associations with Indoor Microbiotas. Environ. Sci. Technol. 2022, 56, 6282–6293. [Google Scholar] [CrossRef]
- Zhou, F.; Niu, M.; Zheng, Y.; Sun, Y.; Wu, Y.; Zhu, T.; Shen, F. Impact of outdoor air on indoor airborne microbiome under hazy air pollution: A case study in winter Beijing. J. Aerosol Sci. 2021, 156, 105798. [Google Scholar] [CrossRef]
- Niu, M.; Shen, F.; Zhou, F.; Zhu, T.; Zheng, Y.; Yang, Y.; Sun, Y.; Li, X.; Wu, Y.; Fu, P. Indoor air filtration could lead to increased airborne endotoxin levels. Environ. Int. 2020, 142, 105878. [Google Scholar] [CrossRef]
- Figueiredo, D.M.; Duyzer, J.; Huss, A.; Krop, E.J.; Gerritsen-Ebben, M.; Gooijer, Y.; Vermeulen, R.C. Spatio-temporal variation of outdoor and indoor pesticide air concentrations in homes near agricultural fields. Atmos. Environ. 2021, 262, 118612. [Google Scholar] [CrossRef]
- Li, T.; Yu, Y.; Sun, Z.; Duan, J. A comprehensive understanding of ambient particulate matter and its components on the adverse health effects based from epidemiological and laboratory evidence. Part. Fibre Toxicol. 2022, 19, 67. [Google Scholar] [CrossRef]
- Duarte, R.M.; Gomes, J.F.; Querol, X.; Cattaneo, A.; Bergmans, B.; Saraga, D.; Maggos, T.; Di Gilio, A.; Rovelli, S.; Villanueva, F. Advanced instrumental approaches for chemical characterization of indoor particulate matter. Appl. Spectrosc. Rev. 2022, 57, 705–745. [Google Scholar] [CrossRef]
- Ilacqua, V.; Scharko, N.; Zambrana, J.; Malashock, D. Survey of residential indoor particulate matter measurements 1990–2019′. Indoor Air 2022, 32, e13057. [Google Scholar] [CrossRef]
- Busenkell, E.; Collins, C.M.; Moy, M.L.; Hart, J.E.; Grady, S.T.; Coull, B.A.; Schwartz, J.D.; Koutrakis, P.; Garshick, E. Modification of associations between indoor particulate matter and systemic inflammation in individuals with COPD. Environ. Res. 2022, 209, 112802. [Google Scholar] [CrossRef] [PubMed]
- Ścibor, M.; Balcerzak, B.; Galbarczyk, A.; Targosz, N.; Jasienska, G. Are we safe inside? Indoor air quality in relation to outdoor concentration of PM10 and PM2. 5 and to characteristics of homes. Sustain. Cities Soc. 2019, 48, 101537. [Google Scholar] [CrossRef]
- Elbayoumi, M.; Ramli, N.A.; Yusof, N.F.F.M.; Yahaya, A.S.B.; Al Madhoun, W.; Ul-Saufie, A.Z. Multivariate methods for indoor PM10 and PM2. 5 modelling in naturally ventilated schools buildings. Atmos. Environ. 2014, 94, 11–21. [Google Scholar] [CrossRef]
- Tasić, V.; Jovašević-Stojanović, M.; Vardoulakis, S.; Milošević, N.; Kovačević, R.; Petrović, J. Comparative assessment of a real-time particle monitor against the reference gravimetric method for PM10 and PM2. 5 in indoor air. Atmos. Environ. 2012, 54, 358–364. [Google Scholar] [CrossRef]
- Anjum, M.S.; Ali, S.M.; Subhani, M.A.; Anwar, M.N.; Nizami, A.-S.; Ashraf, U.; Khokhar, M.F. An emerged challenge of air pollution and ever-increasing particulate matter in Pakistan; a critical review. J. Hazard. Mater. 2021, 402, 123943. [Google Scholar] [CrossRef]
- Leffel, B.; Tavasoli, N.; Liddle, B.; Henderson, K.; Kiernan, S. Metropolitan air pollution abatement and industrial growth: Global urban panel analysis of PM10, PM2. 5, NO2 and SO2. Environ. Sociol. 2022, 8, 94–107. [Google Scholar] [CrossRef]
- Dang, N.; Zhang, H.; Salam, M.M.A.; Li, H.; Chen, G. Foliar dust particle retention and metal accumulation of five garden tree species in Hangzhou: Seasonal changes. Environ. Pollut. 2022, 306, 119472. [Google Scholar] [CrossRef]
- Aslam, R.; Sharif, F.; Baqar, M.; Shahzad, L. Source identification and risk assessment of polycyclic aromatic hydrocarbons (PAHs) in air and dust samples of Lahore City. Sci. Rep. 2022, 12, 2459. [Google Scholar] [CrossRef]
- Kansiime, W.K.; Mugambe, R.K.; Atusingwize, E.; Wafula, S.T.; Nsereko, V.; Ssekamatte, T.; Nalugya, A.; Coker, E.S.; Ssempebwa, J.C.; Isunju, J.B. Use of biomass fuels predicts indoor particulate matter and carbon monoxide concentrations; evidence from an informal urban settlement in Fort Portal city, Uganda. BMC Public Health 2022, 22, 1723. [Google Scholar] [CrossRef]
- Nafees, A.A.; Taj, T.; Kadir, M.M.; Fatmi, Z.; Lee, K.; Sathiakumar, N. Indoor air pollution (PM2.5) due to secondhand smoke in selected hospitality and entertainment venues of Karachi, Pakistan. Tob. Control 2012, 21, 460–464. [Google Scholar] [CrossRef]
- Tao, S.; Shen, G.; Cheng, H.; Ma, J. Toward clean residential energy: Challenges and priorities in research. Environ. Sci. Technol. 2021, 55, 13602–13613. [Google Scholar] [CrossRef]
- Yaqoob, H.; Teoh, Y.H.; Din, Z.U.; Sabah, N.U.; Jamil, M.A.; Mujtaba, M.; Abid, A. The potential of sustainable biogas production from biomass waste for power generation in Pakistan. J. Clean. Prod. 2021, 307, 127250. [Google Scholar] [CrossRef]
- Arif, M.; Parveen, S. Carcinogenic effects of indoor black carbon and particulate matters (PM2.5 and PM10) in rural households of India. Environ. Sci. Pollut. Res. 2021, 28, 2082–2096. [Google Scholar] [CrossRef]
- Cush, K.; Koh, K.; Saikawa, E. Impacts of biomass and garbage burning on air quality in South/Southeast Asia. In Biomass Burning in South and Southeast Asia; CRC Press: Boca Raton, FL, USA, 2021; pp. 3–20. [Google Scholar]
- Colbeck, I.; Nasir, Z.A.; Ali, Z. Characteristics of indoor/outdoor particulate pollution in urban and rural residential environment of Pakistan. Indoor Air 2010, 20, 40–51. [Google Scholar] [CrossRef]
- Mendell, A.Y.; Mahdavi, A.; Siegel, J.A. Particulate matter concentrations in social housing. Sustain. Cities Soc. 2022, 76, 103503. [Google Scholar] [CrossRef]
- Junaid, M.; Syed, J.H.; Abbasi, N.A.; Hashmi, M.Z.; Malik, R.N.; Pei, D.-S. Status of indoor air pollution (IAP) through particulate matter (PM) emissions and associated health concerns in South Asia. Chemosphere 2018, 191, 651–663. [Google Scholar] [CrossRef]
- Qayyum, F.; Mehmood, U.; Tariq, S.; Nawaz, H. Particulate matter (PM2.5) and diseases: An autoregressive distributed lag (ARDL) technique. Environ. Sci. Pollut. Res. 2021, 28, 67511–67518. [Google Scholar] [CrossRef]
- Anwar, M.N.; Shabbir, M.; Tahir, E.; Iftikhar, M.; Saif, H.; Tahir, A.; Murtaza, M.A.; Khokhar, M.F.; Rehan, M.; Aghbashlo, M. Emerging challenges of air pollution and particulate matter in China, India, and Pakistan and mitigating solutions. J. Hazard. Mater. 2021, 416, 125851. [Google Scholar] [CrossRef]
- Kamran, M.; Cheema, A.M.; Saima, M.I.T.K.; Fatima, Z.; Nosheen, B.; Shahid, M.K. Global Concern Of Air Pollution And The Case Of Pakistani Society: An Islamic Perspective On Green Environment. Webology 2022, 19, 8321–8325. [Google Scholar]
- Asghar, K.; Ali, A.; Tabassum, A.; Nadeem, S.; Hakim, S.; Amin, M.; Raza, G.; Bashir, S.; Afshan, N.; Usman, N. Assessment of particulate matter (PM) in ambient air of different settings and its associated health risk in Haripur city, Pakistan. Braz. J. Biol. 2022, 84, 256190. [Google Scholar] [CrossRef]
- Aslam, R.; Sharif, F.; Baqar, M.; Nizami, A.-S.; Ashraf, U. Role of ambient air pollution in asthma spread among various population groups of Lahore City: A case study. Environ. Sci. Pollut. Res. 2022, 30, 8682–8697. [Google Scholar] [CrossRef] [PubMed]
- Jiao, X.; Xiong, R.; Luo, Z.; Li, Y.; Cheng, H.; Rashid, A.; Shen, G.; Tao, S. Household energy stacking and structures in Pakistan–results from a multiple-energy study in Azad Kashmir and Punjab. J. Environ. Sci. 2022, 133, 152–160. [Google Scholar] [CrossRef]
- Rashid, F.; Sarwar, S.; Habib, S.; Tahir, H.; Ali, I.N.; Abbas, T.A. Particulate Matter Concentration and Microbial Load in Heavy Traffic Areas of District Lahore, Pakistan: PM and Microbial Concentration in Heavy Traffic Areas. Pak. BioMedical J. 2022, 5, 34–39. [Google Scholar] [CrossRef]
- Barr, K.J.; Johnson, C.L.; Cohen, J.; D’Souza, P.; Gallegos, E.I.; Tsai, C.-C.; Dunlop, A.L.; Corwin, E.J.; Barr, D.B.; Ryan, P.B. Legacy Chemical Pollutants in House Dust of Homes of Pregnant African Americans in Atlanta. Toxics 2022, 10, 755. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Lyu, H.; Ma, X.; Ren, G.; Song, J.; Jing, X.; Liu, Y. Comparative effects of environmental factors on bacterial communities in two types of indoor dust: Potential risks to university students. Environ. Res. 2022, 203, 111869. [Google Scholar] [CrossRef]
- Zhu, J.; Zhang, X.; Liao, K.; Wu, P.; Jin, H. Microplastics in dust from different indoor environments. Sci. Total Environ. 2022, 833, 155256. [Google Scholar] [CrossRef]
- Cao, Z.; Xu, F.; Covaci, A.; Wu, M.; Yu, G.; Wang, B.; Deng, S.; Huang, J. Differences in the seasonal variation of brominated and phosphorus flame retardants in office dust. Environ. Int. 2014, 65, 100–106. [Google Scholar] [CrossRef]
- Ali, N.; Van den Eede, N.; Dirtu, A.C.; Neels, H.; Covaci, A. Assessment of human exposure to indoor organic contaminants via dust ingestion in Pakistan. Indoor Air 2012, 22, 200–211. [Google Scholar] [CrossRef]
- Ali, N.; Ali, L.; Mehdi, T.; Dirtu, A.C.; Al-Shammari, F.; Neels, H.; Covaci, A. Levels and profiles of organochlorines and flame retardants in car and house dust from Kuwait and Pakistan: Implication for human exposure via dust ingestion. Environ. Int. 2013, 55, 62–70. [Google Scholar] [CrossRef]
- Khalid, F.; Qadir, A.; Hashmi, M.Z.; Mehmood, A.; Aslam, I.; Zhang, G.; Ahmed, Z. Evaluation of ceiling fan dust as an indicator of indoor PCBs pollution in selected cities of Punjab, Pakistan: Implication on human health. Arab. J. Geosci. 2022, 15, 874. [Google Scholar] [CrossRef]
- Waheed, S.; Khan, M.U.; Sweetman, A.J.; Jones, K.C.; Moon, H.-B.; Malik, R.N. Exposure of polychlorinated naphthalenes (PCNs) to Pakistani populations via non-dietary sources from neglected e-waste hubs: A problem of high health concern. Environ. Pollut. 2020, 259, 113838. [Google Scholar] [CrossRef]
- Dai, Q.; Min, X.; Weng, M. A review of polychlorinated biphenyls (PCBs) pollution in indoor air environment. J. Air Waste Manag. Assoc. 2016, 66, 941–950. [Google Scholar] [CrossRef]
- Yana, S.; Nizar, M.; Mulyati, D. Biomass waste as a renewable energy in developing bio-based economies in Indonesia: A review. Renew. Sustain. Energy Rev. 2022, 160, 112268. [Google Scholar] [CrossRef]
- Kaygusuz, K. Energy for sustainable development: A case of developing countries. Renew. Sustain. Energy Rev. 2012, 16, 1116–1126. [Google Scholar] [CrossRef]
- Kaygusuz, K. Energy services and energy poverty for sustainable rural development. Renew. Sustain. Energy Rev. 2011, 15, 936–947. [Google Scholar] [CrossRef]
- Hattori, S.; Iwamatsu, T.; Miura, T.; Tsutsumi, F.; Tanaka, N. Investigation of Indoor Air Quality in Residential Buildings by Measuring CO2 Concentration and a Questionnaire Survey. Sensors 2022, 22, 7331. [Google Scholar] [CrossRef]
- Morris, J.; Reilly, J.; Paltsev, S.; Sokolov, A.; Cox, K. Representing Socio-Economic Uncertainty in Human System Models. Earth’s Future 2022, 10, e2021EF002239. [Google Scholar] [CrossRef]
- Patel, N.; Okocha, B.; Narayan, S.; Sheth, M. Indoor air pollution from burning biomass & child health. IJSR 2013, 2, 492–506. [Google Scholar]
- Yousafzai, A.W.; Khan, S.A.; Bano, S.; Khan, M.M. Exploring the phenomenon of suicidal behaviour (SB): An explanatory, mixed-method study in rural Pakistan. Int. J. Soc. Psychiatry 2022, 68, 1629–1635. [Google Scholar] [CrossRef]
- Imran, M.; Zahid, A.; Mouneer, S.; Özçatalbaş, O.; Ul Haq, S.; Shahbaz, P.; Muzammil, M.; Murtaza, M.R. Relationship between Household Dynamics, Biomass Consumption, and Carbon Emissions in Pakistan. Sustainability 2022, 14, 6762. [Google Scholar] [CrossRef]
- Mboumboue, E.; Njomo, D. Potential contribution of renewables to the improvement of living conditions of poor rural households in developing countries: Cameroon׳ s case study. Renew. Sustain. Energy Rev. 2016, 61, 266–279. [Google Scholar] [CrossRef]
- Qi, J.; Liu, L.; Wu, J. Improving Combustion Technology for Cooking Activities for Pollutant Emission Reduction and Carbon Neutrality. Atmosphere 2022, 13, 561. [Google Scholar] [CrossRef]
- Woolley, K.E.; Dickinson-Craig, E.; Lawson, H.L.; Sheikh, J.; Day, R.; Pope, F.D.; Greenfield, S.M.; Bartington, S.E.; Warburton, D.; Manaseki-Holland, S. Effectiveness of interventions to reduce household air pollution from solid biomass fuels and improve maternal and child health outcomes in low-and middle-income countries: A systematic review and meta-analysis. Indoor Air 2022, 32, e12958. [Google Scholar] [CrossRef] [PubMed]
- Rehman, A.; Ma, H.; Ozturk, I.; Ulucak, R. Sustainable development and pollution: The effects of CO2 emission on population growth, food production, economic development, and energy consumption in Pakistan. Environ. Sci. Pollut. Res. 2022, 29, 17319–17330. [Google Scholar] [CrossRef] [PubMed]
- Soomro, H.; Shah, S.F.; Sahito, W.S.; Uqaili, M.A.; Kumar, L.; Nixon, J.D.; Harijan, K. Assessment of Sustainable Biomass Energy Technologies in Pakistan Using the Analytical Hierarchy Process. Sustainability 2022, 14, 11388. [Google Scholar] [CrossRef]
- Yousaf, H.; Amin, A.; Baloch, A.; Akbar, M. Investigating household sector’s non-renewables, biomass energy consumption and carbon emissions for Pakistan. Environ. Sci. Pollut. Res. 2021, 28, 40824–40834. [Google Scholar] [CrossRef]
- Imran, M.; Özçatalbaş, O.; Bakhsh, K. Rural household preferences for cleaner energy sources in Pakistan. Environ. Sci. Pollut. Res. 2019, 26, 22783–22793. [Google Scholar] [CrossRef]
- Irfan, M.; Zhao, Z.-Y.; Panjwani, M.K.; Mangi, F.H.; Li, H.; Jan, A.; Ahmad, M.; Rehman, A. Assessing the energy dynamics of Pakistan: Prospects of biomass energy. Energy Rep. 2020, 6, 80–93. [Google Scholar] [CrossRef]
- Ahmed, M.; Shuai, C.; Abbas, K.; Rehman, F.U.; Khoso, W.M. Investigating health impacts of household air pollution on woman’s pregnancy and sterilization: Empirical evidence from Pakistan, India, and Bangladesh. Energy 2022, 247, 123562. [Google Scholar] [CrossRef]
- Pope, D.P.; Mishra, V.; Thompson, L.; Siddiqui, A.R.; Rehfuess, E.A.; Weber, M.; Bruce, N.G. Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries. Epidemiol. Rev. 2010, 32, 70–81. [Google Scholar] [CrossRef]
- Haider, M.R.; Rahman, M.M.; Islam, F.; Khan, M.M. Association of low birthweight and indoor air pollution: Biomass fuel use in Bangladesh. J. Health Pollut. 2016, 6, 18–25. [Google Scholar] [CrossRef]
- Nasir, Z.A.; Murtaza, F.; Colbeck, I. Role of poverty in fuel choice and exposure to indoor air pollution in Pakistan. J. Integr. Environ. Sci. 2015, 12, 107–117. [Google Scholar] [CrossRef]
- Siddiqui, A.R.; Peerson, J.; Brown, K.H.; Gold, E.B.; Lee, K.; Bhuta, Z.A. Indoor air pollution from solid fuel use and low birth weight (LBW) in Pakistan. Epidemiology 2005, 16, S86. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Indoor Air Pollution from Solid Fuels and Risk of Low Birth Weight and Stillbirth. In Report from a Symposium Held at the Annual Conference of the International Society for Environmental Epidemiology (ISEE), 13–16 September 2005, Johannesburg, South Africa; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Khan, M.S.B.; Lohano, H.D. Household air pollution from cooking fuel and respiratory health risks for children in Pakistan. Environ. Sci. Pollut. Res. 2018, 25, 24778–24786. [Google Scholar] [CrossRef]
- Taksande, A.M.; Yeole, M. Risk factors of Acute Respiratory Infection (ARI) in under-fives in a rural hospital of Central India. J. Pediatr. Neonatal Individ. Med. 2016, 5, e050105. [Google Scholar]
- Quinn, A.K.; Bruce, N.; Puzzolo, E.; Dickinson, K.; Sturke, R.; Jack, D.W.; Mehta, S.; Shankar, A.; Sherr, K.; Rosenthal, J.P. An analysis of efforts to scale up clean household energy for cooking around the world. Energy Sustain. Dev. 2018, 46, 1–10. [Google Scholar] [CrossRef]
- Naz, S.; Page, A.; Agho, K.E. Household air pollution from use of cooking fuel and under-five mortality: The role of breastfeeding status and kitchen location in Pakistan. PLoS ONE 2017, 12, e0173256. [Google Scholar] [CrossRef]
- Fatmi, Z.; Rahman, A.; Kazi, A.; Kadir, M.M.; Sathiakumar, N. Situational analysis of household energy and biomass use and associated health burden of indoor air pollution and mitigation efforts in Pakistan. Int. J. Environ. Res. Public Health 2010, 7, 2940–2952. [Google Scholar] [CrossRef]
- Yasmin, N.; Grundmann, P. Home-cooked energy transitions: Women empowerment and biogas-based cooking technology in Pakistan. Energy Policy 2020, 137, 111074. [Google Scholar] [CrossRef]
- Shams, Z.I.; Javed, T.; Zubair, A.; Waqas, M.; Ali, S.; Ahmed, A. Carbon Monoxide Concentrations in Kitchens of Gas-fired Burners, Karachi, Pakistan: Carbon Monoxide in Karachi Bungalow and Apartment Kitchens. Pak. J. Sci. Ind. Res. Ser. A Phys. Sci. 2022, 65, 25–32. [Google Scholar] [CrossRef]
- Iqbal, S.; Anwar, S.; Akram, W.; Irfan, M. Factors leading to adoption of biogas technology: A case study of District Faisalabad, Punjab, Pakistan. Int. J. Acad. Res. Bus. Soc. Sci. 2013, 3, 2222–6990. [Google Scholar] [CrossRef] [PubMed]
- Yasmin, I.; Akram, W.; Adeel, S.; Chandio, A.A. Non-adoption decision of biogas in rural Pakistan: Use of multinomial logit model. Environ. Sci. Pollut. Res. 2022, 29, 53884–53905. [Google Scholar] [CrossRef] [PubMed]
- Karanasiou, A.; Alastuey, A.; Amato, F.; Renzi, M.; Stafoggia, M.; Tobias, A.; Reche, C.; Forastiere, F.; Gumy, S.; Mudu, P. Short-term health effects from outdoor exposure to biomass burning emissions: A review. Sci. Total Environ. 2021, 781, 146739. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.W.; Lu, H.F.; Liu, Z.S. Development and application of the Ames test using a direct-exposure module: The assessment of mutagenicity of incense and sidestream cigarette smoke. Indoor Air 2022, 32, e13140. [Google Scholar] [CrossRef]
- Öberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- Naeem, A.; Rafiq, L.; Nazar, R.; Kashif, M.; Naqvi, S.H.Z. An assessment of Risk Factors and Health Impacts Associated with Indoor Air Pollution and Tobacco Smoke in Lahore, Pakistan. J. Qual. Assur. Agric. Sci. 2022, 2, 37–45. [Google Scholar]
- Zaidi, S.; Moin, O.; Khan, J. Second-hand smoke in indoor hospitality venues in Pakistan. Int. J. Tuberc. Lung Dis. 2011, 15, 972–977. [Google Scholar] [CrossRef]
- Khan, J.A.; Amir Humza Sohail, A.M.; Arif Maan, M.A. Tobacco control laws in Pakistan and their implementation: A pilot study in Karachi. J. Pak. Med. Assoc. 2016, 66, 875. [Google Scholar]
- Amir, M.; Khan, U.; Baig, M. Evaluation of Consequences of Cigarette smoking on General Population of Pakistan. Asian J. Multidisc. Stud. 2020, 8, 5. [Google Scholar]
- Khwaja, M.A.; Shams, T. Pakistan National Ambient Air Quality Standards: A comparative Assessment with Selected Asian Countries and World Health Organization (WHO); Sustainable Development Policy Institute: Islamabad, Pakistan, 2020. [Google Scholar]
- Abdul Jabbar, S.; Tul Qadar, L.; Ghafoor, S.; Rasheed, L.; Sarfraz, Z.; Sarfraz, A.; Sarfraz, M.; Felix, M.; Cherrez-Ojeda, I. Air quality, pollution and sustainability trends in South Asia: A population-based study. Int. J. Environ. Res. Public Health 2022, 19, 7534. [Google Scholar] [CrossRef]
- Ahmed, T.; Usman, M.; Scholz, M. Biodeterioration of buildings and public health implications caused by indoor air pollution. Indoor Built Environ. 2018, 27, 752–765. [Google Scholar] [CrossRef]
- Farooq, S.; Yaqoob, I. Awareness towards efficiency of green and conventional building materials used in Pakistan. Proc. Pak. Acad. Sci. A Phys. Comput. Sci. 2019, 56, 75–84. [Google Scholar]
- Rafique, M.; Rahman, S.U.; Mahmood, T.; Rahman, S.; Rehman, S.U. Radon exhalation rate from soil, sand, bricks, and sedimentary samples collected from Azad Kashmir, Pakistan. Russ. Geol. Geophys. 2011, 52, 450–457. [Google Scholar] [CrossRef]
- Majid, M.I.; Khan, M.I. Techno-economic analysis of green construction regulations plus survey for prototype implementation in karachi. Pak. J. Sci. Ind. Res. Ser. A Phys. Sci. 2021, 64, 161–172. [Google Scholar] [CrossRef]
- Nazaroff, W.W. Indoor bioaerosol dynamics. Indoor Air 2016, 26, 61–78. [Google Scholar] [CrossRef]
- Nimra, A.; Ali, Z.; Sultan, S.; Nasir, Z.A.; Sidra, S.; Hussain, A. Molecular sequencing and phylogenetic analysis of bioaerosols in hospital wards with different ventilation conditions. J. Infect. Dev. Ctries. 2022, 16, 157–165. [Google Scholar] [CrossRef]
- Lee, G.; Yoo, K. A review of the emergence of antibiotic resistance in bioaerosols and its monitoring methods. Rev. Environ. Sci. Bio/Technol. 2022, 21, 799–827. [Google Scholar] [CrossRef]
- Mandal, J.; Brandl, H. Bioaerosols in indoor environment—A review with special reference to residential and occupational locations. Open Environ. Biol. Monit. J. 2011, 4, 83–96. [Google Scholar]
- Hassan, A.; Zeeshan, M. Microbiological indoor air quality of hospital buildings with different ventilation systems, cleaning frequencies and occupancy levels. Atmos. Pollut. Res. 2022, 13, 101382. [Google Scholar] [CrossRef]
- Grogan, S.N.; Mainelis, G. Effect of sampling duration on culturable and viable bioaerosol determination when using Rutgers Electrostatic Passive Sampler (REPS). J. Aerosol Sci. 2022, 166, 106066. [Google Scholar] [CrossRef]
- Wathes, C. Bioaerosols in Animal Houses. In Bioaerosols Handbook; CRC Press: Boca Raton, FL, USA, 2020; pp. 547–577. [Google Scholar]
- Mukhtar, S.; Mukhtar, S.; Hani, U.; Iram, S. Scenario Of Aspergillus Indoor Contamination In Pakistan (2000–2020)—A Review. Environ. Contam. Rev. 2021, 4, 24–28. [Google Scholar]
- Bukhari, S.S.I. Characterization of Bioaerosols and Particulate Matter (PM) in Residential Settings of Asthmatic Patients of Lahore, Pakistan Air Microflora and Particulate Matter in Asthmatic Houses. Iran. J. Allergy Asthma Immunol. 2021, 20, 147. [Google Scholar] [PubMed]
- Nasir, Z.A.; Colbeck, I.; Sultan, S.; Ahmed, S. Bioaerosols in residential micro-environments in low income countries: A case study from Pakistan. Environ. Pollut. 2012, 168, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Roy, R.; Jan, R.; Joshi, U.; Bhor, R.; Pai, K.; Satsangi, P.G. Characterization, pro-inflammatory response and cytotoxic profile of bioaerosols from urban and rural residential settings in Pune, India. Environ. Pollut. 2020, 264, 114698. [Google Scholar] [CrossRef] [PubMed]
- Colbeck, I.; Nasir, Z.A.; Hasnain, S.; Sultan, S. Indoor air quality at rural and urban sites in Pakistan. Water Air Soil Pollut. Focus 2008, 8, 61–69. [Google Scholar] [CrossRef]
- Hafeez, S.; Ali, Z.; Nasir, Z.A.; Sultan, S. Assessment of Microbial Air Quality within Facilities of Waste Transfer Stations and Disposal Sites of Lahore, Pakistan. Pol. J. Environ. Stud. 2021, 30, 5567–5576. [Google Scholar] [CrossRef]
- Colbeck, I.; Sidra, S.; Ali, Z.; Ahmed, S.; Nasir, Z.A. Spatial and temporal variations in indoor air quality in Lahore, Pakistan. Int. J. Environ. Sci. Technol. 2019, 16, 2565–2572. [Google Scholar] [CrossRef]
- Safdar, S.; Ali, Z.; Colbeck, I.; Nasir, Z.A. Airborne Microflora and Particulate Matter in Residential Houses in Lahore, Pakistan’. Available online: https://scholar.googleusercontent.com/scholar?q=cache:eKkf7eG3b6MJ:scholar.google.com/+Airborne+microflora+and+particulate+matter+in+residential+houses+in+Lahore,+Pakistan&hl=zh-CN&as_sdt=0,5 (accessed on 20 February 2023).
- Kumar, P.; Singh, A.; Singh, R. Seasonal variation and size distribution in the airborne indoor microbial concentration of residential houses in Delhi and its impact on health. Aerobiologia 2021, 37, 719–732. [Google Scholar] [CrossRef]
- Sidra, S.; Ali, Z.; Sultan, S.; Ahmed, S.; Colbeck, I.; Nasir, Z.A. Assessment of airborne microflora in the indoor micro-environments of residential houses of Lahore, Pakistan. Aerosol Air Qual. Res. 2015, 15, 2385–2396. [Google Scholar] [CrossRef]
- Sajjad, H.; Ghaffar, A. Observed, simulated and projected extreme climate indices over Pakistan in changing climate. Theor. Appl. Climatol. 2019, 137, 255–281. [Google Scholar] [CrossRef]
- Dilawar, A.; Chen, B.; Arshad, A.; Guo, L.; Ehsan, M.I.; Hussain, Y.; Kayiranga, A.; Measho, S.; Zhang, H.; Wang, F. Towards Understanding Variability in Droughts in Response to Extreme Climate Conditions over the Different Agro-Ecological Zones of Pakistan. Sustainability 2021, 13, 6910. [Google Scholar] [CrossRef]
- Abbas, S.; Ali, G.; Qamer, F.M.; Irteza, S.M. Associations of air pollution concentrations and energy production dynamics in Pakistan during lockdown. Environ. Sci. Pollut. Res. 2022, 29, 35036–35047. [Google Scholar] [CrossRef]
- Maan, Y.A.M.A.; Jameel, M.; Akhtar, M. A Simulation Based Study of Energy Conservation of Residences In Lahore, Pakistan. J. Arts Soc. Sci. 2021, 8, 104–113. [Google Scholar]
- Colbeck, I.; Nasir, Z.A.; Ali, Z. The state of ambient air quality in Pakistan—A review. Environ. Sci. Pollut. Res. 2010, 17, 49–63. [Google Scholar] [CrossRef]
- Munir, R.; Khayyam, U. Tropospheric Ozone Concentration Over PAKISTAN. In Asian Atmospheric Pollution; Elsevier: Amsterdam, The Netherlands, 2022; pp. 349–365. [Google Scholar]
- Rabbani, U.; Razzaq, S.; Irfan, M.; Semple, S.; Nafees, A.A. Indoor air pollution and respiratory health in a metropolitan city of Pakistan. J. Occup. Environ. Med. 2022, 64, 761–765. [Google Scholar] [CrossRef]
- Ghani, N.; Tariq, F.; Javed, H.; Nisar, N.; Tahir, A. Low-temperature health hazards among workers of cold storage facilities in Lahore, Pakistan. Med. Pr. 2019, 71, 1–7. [Google Scholar] [CrossRef]
- Cocchiara, R.A.; Mannocci, A.; Backhaus, I.; Thiene, D.D.; Sestili, C.; Barbato, D.; Torre, G.L. The Relationship Between Environment and Mental Health. In Environmental Alteration Leads to Human Disease; Springer: Berlin/Heidelberg, Germany, 2022; pp. 229–240. [Google Scholar]
- Smith, K.R.; Mehta, S.; Maeusezahl-Feuz, M. Indoor air pollution from household use of solid fuels. Comp. Quantif. Health Risks: Glob. Reg. Burd. Dis. Attrib. Sel. Major Risk Factors 2004, 2, 1435–1493. [Google Scholar]
- Hu, F.; Guo, Y. Health impacts of air pollution in China. Front. Environ. Sci. Eng. 2021, 15, 74. [Google Scholar] [CrossRef]
- Pandey, A.; Brauer, M.; Cropper, M.L.; Balakrishnan, K.; Mathur, P.; Dey, S.; Turkgulu, B.; Kumar, G.A.; Khare, M.; Beig, G. Health and economic impact of air pollution in the states of India: The Global Burden of Disease Study 2019. Lancet Planet. Health 2021, 5, e25–e38. [Google Scholar] [CrossRef]
- Balakrishnan, K.; Dey, S.; Gupta, T.; Dhaliwal, R.; Brauer, M.; Cohen, A.J.; Stanaway, J.D.; Beig, G.; Joshi, T.K.; Aggarwal, A.N. The impact of air pollution on deaths, disease burden, and life expectancy across the states of India: The Global Burden of Disease Study 2017. Lancet Planet. Health 2019, 3, e26–e39. [Google Scholar] [CrossRef]
- Yamamoto, S.; Phalkey, R.; Malik, A. A systematic review of air pollution as a risk factor for cardiovascular disease in South Asia: Limited evidence from India and Pakistan. Int. J. Hyg. Environ. Health 2014, 217, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Paleologos, K.E.; Selim, M.Y.; Mohamed, A.-M.O. Indoor Air Quality: Pollutants, Health Effects, and Regulations. In Pollution Assessment for Sustainable Practices in Applied Sciences and Engineering; Elsevier: Amsterdam, The Netherlands, 2021; pp. 405–489. [Google Scholar]
- Sarwar, F.; Alam, K.; Chow, C.W.; Saeed, M.; Malik, R.N. Pulmonary Dysfunction Augmenting Bacterial Aerosols in Leather Tanneries of Punjab, Pakistan. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 2925. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, U.; Razzak, S.; Burney, P.; Nafees, A.A. Indoor Air Pollutants and Respiratory Outcomes Among Adult Pakistani Papulation: A Cross Sectional Survey. Eur. Respir. Soc. 2020, 56, 1299. [Google Scholar]
- Jordanova, D.; Jordanova, N.; Lanos, P.; Petrov, P.; Tsacheva, T. Magnetism of outdoor and indoor settled dust and its utilization as a tool for revealing the effect of elevated particulate air pollution on cardiovascular mortality. Geochem. Geophys. Geosystems 2012, 13, Q08Z49. [Google Scholar] [CrossRef]
- Farah, N.; Khan, I.A. Awareness about the health impacts of indoor air pollution on rural women in District Faisalabad. J. Glob. Innov. Agric. Soc. Sci 2015, 3, 90–95. [Google Scholar] [CrossRef]
- Kouser, S.; Munir, S. Does communal women empowerment mitigate the risk of acute respiratory infection among under-five children in Pakistan? Public Health 2022, 205, 133–138. [Google Scholar] [CrossRef]
- Nair, A.N.; Anand, P.; George, A.; Mondal, N. A review of strategies and their effectiveness in reducing indoor airborne transmission and improving indoor air quality. Environ. Res. 2022, 213, 113579. [Google Scholar] [CrossRef]
- Tariq, N.; Jaffry, T.; Fiaz, R.; Rajput, A.M.; Khalid, S. Awareness About Indoor Air Pollution In General Population Of Rawalpindi And Islamabad. Pak. J. Public Health 2018, 8, 80–83. [Google Scholar] [CrossRef]
- Aslam, I.; Baqar, M.; Qadir, A.; Mumtaz, M.; Li, J.; Zhang, G. Polychlorinated biphenyls in indoor dust from urban dwellings of Lahore, Pakistan: Congener profile, toxicity equivalency, and human health implications. Indoor Air 2021, 31, 1417–1426. [Google Scholar] [CrossRef]
- Khan, M.U.; Besis, A.; Li, J.; Zhang, G.; Malik, R.N. New insight into the distribution pattern, levels, and risk diagnosis of FRs in indoor and outdoor air at low-and high-altitude zones of Pakistan: Implications for sources and exposure. Chemosphere 2017, 184, 1372–1387. [Google Scholar] [CrossRef]
- Khan, M.U.; Li, J.; Zhang, G.; Malik, R.N. New insight into the levels, distribution and health risk diagnosis of indoor and outdoor dust-bound FRs in colder, rural and industrial zones of Pakistan. Environ. Pollut. 2016, 216, 662–674. [Google Scholar] [CrossRef]
- Rehman, K.; Fatima, F.; Waheed, I.; Akash, M.S.H. Prevalence of exposure of heavy metals and their impact on health consequences. J. Cell. Biochem. 2018, 119, 157–184. [Google Scholar] [CrossRef]
- Hamid, N.; Syed, J.H.; Junaid, M.; Mahmood, A.; Li, J.; Zhang, G.; Malik, R.N. Elucidating the urban levels, sources and health risks of polycyclic aromatic hydrocarbons (PAHs) in Pakistan: Implications for changing energy demand. Sci. Total Environ. 2018, 619, 165–175. [Google Scholar] [CrossRef]
- Sonwani, S.; Madaan, S.; Arora, J.; Suryanarayan, S.; Rangra, D.; Mongia, N.; Vats, T.; Saxena, P. Inhalation exposure to atmospheric nanoparticles and its associated impacts on human health: A review. Front. Sustain. Cities 2021, 3, 690444. [Google Scholar] [CrossRef]
- Bai, L.; Li, C. Investigation of Indoor Polycyclic Aromatic Hydrocarbons (PAHs) in Rural Northeast China: Pollution Characteristics, Source Analysis, and Health Assessment. Buildings 2022, 12, 153. [Google Scholar] [CrossRef]
- Rafique, M.; Manzoor, N.; Rahman, S.; Rahman, S.; Rajput, M. Assessment of lung cancer risk due to indoor radon exposure in inhabitants of the state of Azad Kashmir Pakistan. Int. J. Radiat. Res. 2012, 10, 19–29. [Google Scholar]
- Xue, S.; Zhang, B.; Zhao, X. Brain drain: The impact of air pollution on firm performance. J. Environ. Econ. Manag. 2021, 110, 102546. [Google Scholar] [CrossRef]
- Wang, L.; Dai, Y.; Kong, D. Air pollution and employee treatment. J. Corp. Financ. 2021, 70, 102067. [Google Scholar] [CrossRef]
- La Nauze, A.; Severnini, E.R. Air Pollution and Adult Cognition: Evidence from Brain Training; National Bureau of Economic Research: Cambridge, MA, USA, 2021. [Google Scholar]
- Saleem, A.; Ali, S.A.; Zaman, K.; Muhammad, A.; Shehzad, K.; Ullah, I. Impact of Interior Physical Environment on Academicians’productivity In Pakistan Higher Education Institutes Perspectives. Iran. J. Manag. Stud. 2012, 5, 25–46. [Google Scholar]
- Kamal, A.; Cincinelli, A.; Martellini, T.; Palchetti, I.; Bettazzi, F.; Malik, R.N. Health and carcinogenic risk evaluation for cohorts exposed to PAHs in petrochemical workplaces in Rawalpindi city (Pakistan). Int. J. Environ. Health Res. 2016, 26, 37–57. [Google Scholar] [CrossRef]
- Zhao, L.; Liu, M.; Liu, L.; Guo, W.; Yang, H.; Chen, S.; Yu, J.; Li, M.; Fang, Q.; Lai, X. The association of co-exposure to polycyclic aromatic hydrocarbon and phthalates with blood cell-based inflammatory biomarkers in children: A panel study. Environ. Pollut. 2022, 307, 119479. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Taniyasu, S.; Yamashita, N.; Khan, M.K.; Masood, S.S.; Saied, S.; Khwaja, H.A. Per-and polyfluoroalkyl substances in the atmospheric total suspended particles in Karachi, Pakistan: Profiles, potential sources, and daily intake estimates. Chemosphere 2022, 288, 132432. [Google Scholar] [CrossRef] [PubMed]
- Baqer, N.S.; Mohammed, H.A.; Albahri, A.; Zaidan, A.; Al-qaysi, Z.; Albahri, O. Development of the Internet of Things sensory technology for ensuring proper indoor air quality in hospital facilities: Taxonomy analysis, challenges, motivations, open issues and recommended solution. Measurement 2022, 192, 110920. [Google Scholar] [CrossRef]
- Baqer, N.S.; Mohammed, H.A.; Albahri, A. Development of a real-time monitoring and detection indoor air quality system for intensive care unit and emergency department. Signa Vitae 2022, 1, 16. [Google Scholar]
- Zhou, Y.; Yang, G. Real-time monitoring of pollutants in occupied indoor environments: A pilot study of a hospital in China. J. Build. Eng. 2022, 59, 105105. [Google Scholar] [CrossRef]
- Nimra, A.; Ali, Z.; Khan, M.; Gulshan, T.; Sidra, S.; Gardezi, J.; Tarar, M.; Saleem, M.; Nasir, Z.A.; Colbeck, I. Comparative ambient and indoor particulate matter analysis of operation theatres of government and private (trust) hospitals of Lahore, Pakistan. J. Anim. Plant Sci. 2015, 25, 628–635. [Google Scholar]
- Gholami Motlagh, V.; Ahmadzadehtalatapeh, M.; Mohammadi, O. Effect of Turbulent and Laminar Flow Mechanisms on Airflow Patterns and CO2 Distribution in an Operating Room: A Numerical Analysis. In Scientia Iranica; Sharif University of Technology: Tehran, Iran, 2022. [Google Scholar]
- World Health Organization (WHO). WHO Guidelines for Indoor Air Quality. In Selected Pollutants; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2010. [Google Scholar]
- Apte, K.; Salvi, S. Household air pollution and its effects on health. F1000Research 2016, 5, 2593. [Google Scholar] [CrossRef]
- Raju, S.; Siddharthan, T.; McCormack, M.C. Indoor air pollution and respiratory health. Clin. Chest Med. 2020, 41, 825–843. [Google Scholar] [CrossRef]
- Zhang, J.; Smith, K.R. Indoor air pollution: A global health concern. Br. Med. Bull. 2003, 68, 209–225. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Situation Analysis of Household Energy Use and Indoor Air Pollution in Pakistan. In Situation Analysis of Household Energy Use and Indoor Air Pollution in Pakistan; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Organizatio, W.H. WHO Guidelines for Indoor Air Quality. In Household Fuel Combustion; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Irfan, M.; Cameron, M.P.; Hassan, G. Interventions to mitigate indoor air pollution: A cost-benefit analysis. PLoS ONE 2021, 16, e0257543. [Google Scholar] [CrossRef]
- Ahmed, M.; Xiao, Z.; Shen, Y. Estimation of Ground PM2. 5 Concentrations in Pakistan Using Convolutional Neural Network and Multi-Pollutant Satellite Images. Remote Sens. 2022, 14, 1735. [Google Scholar] [CrossRef]
- Butt, M.S.; Kuklane, K.; Saleem, J.; Zakar, R.; Bukhari, G.M.J.; Ishaq, M. Evaluation of occupational exposure to heat stress and working practices in the small and mid-sized manufacturing industries of Lahore, Pakistan. Avicenna 2022, 2022, 5. [Google Scholar] [CrossRef]
- Sheraz, M.; Mir, K.A.; Anus, A.; Kim, S.; Lee, W.R. SARS-CoV-2 airborne transmission: A review of risk factors and possible preventative measures using air purifiers. Environ. Sci. Process. Impacts 2022, 24, 2191–2216. [Google Scholar] [CrossRef]
- Ramzan, M.; Qasim, M.; Habib, A.; Mukhtar, R. A Study on Uses and Management of Indoor Plants in Pakistan. Int. J. Agric. Biol. 2007, 9, 517–518. [Google Scholar]
- Nasir, Z.A.; Colbeck, I.; Ali, Z.; Ahmad, S. Indoor particulate matter in developing countries: A case study in Pakistan and potential intervention strategies. Environ. Res. Lett. 2013, 8, 024002. [Google Scholar] [CrossRef]
- Raza, M.Y.; Wasim, M.; Sarwar, M.S. Development of Renewable Energy Technologies in rural areas of Pakistan. Energy Sources Part A Recovery Util. Environ. Eff. 2020, 42, 740–760. [Google Scholar] [CrossRef]
- Ponce, P.; Khan, S.A.R. A causal link between renewable energy, energy efficiency, property rights, and CO2 emissions in developed countries: A road map for environmental sustainability. Environ. Sci. Pollut. Res. 2021, 28, 37804–37817. [Google Scholar] [CrossRef]
- Assadi, M.R.; Ataebi, M.; sadat Ataebi, E.; Hasani, A. Prioritization of renewable energy resources based on sustainable management approach using simultaneous evaluation of criteria and alternatives: A case study on Iran’s electricity industry. Renew. Energy 2022, 181, 820–832. [Google Scholar] [CrossRef]
- Khalil, F.A.; Asif, M.; Anwar, S.; ul Haq, S.; Illahi, F. Solar Tracking Techniques and Implementation in Photovoltaic Power Plants: A Review: Solar Tracking Techniques and Implementation in Photovoltaic Power Plants. Proc. Pak. Acad. Sci. A Phys. Comput. Sci. 2017, 54, 231–241. [Google Scholar]
- Chien, F.; Kamran, H.W.; Albashar, G.; Iqbal, W. Dynamic planning, conversion, and management strategy of different renewable energy sources: A sustainable solution for severe energy crises in emerging economies. Int. J. Hydrog. Energy 2021, 46, 7745–7758. [Google Scholar] [CrossRef]
- Zender–Świercz, E. Improvement of indoor air quality by way of using decentralised ventilation. J. Build. Eng. 2020, 32, 101663. [Google Scholar] [CrossRef]
- Singh, R.; Dewan, A. Implementation of the Right to Healthy Environment: Regulations for running air conditioners in public buildings and recognition of biological pollutants. Res. Sq. 2022, preprint. [Google Scholar] [CrossRef]
- Chen, Y.; Li, X.; Zhang, X.; Zhang, Y.; Gao, W.; Wang, R.; He, D. Air conditioner filters become sinks and sources of indoor microplastics fibers. Environ. Pollut. 2022, 292, 118465. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Xiao, H.; Sun, H.; Wang, B.; Lin, B.; Shi, W.; Huang, W. Performance analysis of room air conditioners via questionnaire and integrated field test. Appl. Therm. Eng. 2021, 196, 117243. [Google Scholar] [CrossRef]
- AlMulla, A.A.; Berekaa, M.; Dahlawi, S. Human Exposure Assessment to Air Pollutants in AC Filters from Agricultural, Industrial, and Residential Areas. Atmosphere 2022, 13, 1899. [Google Scholar] [CrossRef]
- Aslam, I.; Mumtaz, M.; Qadir, A.; Jamil, N.; Baqar, M.; Mahmood, A.; Ahmad, S.R.; Zhang, G. Organochlorine pesticides (OCPs) in air-conditioner filter dust of indoor urban setting: Implication for health risk in a developing country. Indoor Air 2021, 31, 807–817. [Google Scholar] [CrossRef]
- Arif, S.; Tabusum, S.; Gul, N. Pesticides Residues In The Human Breast Milk Of Primiparous And Multiparous Women Of Karachi, Pakistan. Feb-Fresenius Environ. Bull. 2022, 31, 9494–9498. [Google Scholar]
- Waleed, K.; Mirza, F.M. Examining fuel choice patterns through household energy transition index: An alternative to traditional energy ladder and stacking models. Environ. Dev. Sustain. 2023, 25, 6449–6501. [Google Scholar] [CrossRef]
- Shahid, M.A.K.; Ahmad, N.; Hussain, K.; Ahmad, N. Indoor, Out Door Air Pollution (Ioap), Cost Effective Methodologies And Potential Intervention Strategies. iJCEM 2015, 1, 11–25. [Google Scholar]
- Wang, Y.; Sun, M.; Yang, X.; Yuan, X. Public awareness and willingness to pay for tackling smog pollution in China: A case study. J. Clean. Prod. 2016, 112, 1627–1634. [Google Scholar] [CrossRef]
- Loewy, S.A.; Kelly, G.W.; Nathanson, M.D. Indoor Pollution in Commercial Buildings: Legal Requirements and Emerging Trends. Temp. Envtl. L. Tech. J. 1992, 11, 239. [Google Scholar]
- Kankaria, A.; Nongkynrih, B.; Gupta, S.K. Indoor air pollution in India: Implications on health and its control. Indian J. Community Med. 2014, 39, 203. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Unit | Districts | |||
|---|---|---|---|---|---|
| Faisalabad | Sargodha | Jhang | |||
| Population | Total | Millions | 5.4 | 2.6 | 2.8 |
| Male | Percentage | 50.7 | 51.5 | 52.0 | |
| Female | Percentage | 49.9 | 48.5 | 48.0 | |
| Urban | Percentage | 47.7 | 28.1 | 23.4 | |
| Rural | Percentage | 52.3 | 71.9 | 76.6 | |
| Average household size | Persons living in one house | Number of persons | 7.2 | 6.5 | 6.5 |
| House type | Pacca (cemented) | Percentage | 69.8 | 77.75 | 37.5 |
| Kacha (mud) | Percentage | 30.17 | 22.24 | 62.5 | |
| Mode of cooking | Gas | Percentage of housing units | 26.7 | 9.0 | 5.1 |
| Other | Percentage of housing units | 73.3 | 91.0 | 94.9 | |
| Number of animals | Buffaloes and cows | Thousands | 2421 | 1495 | 1890 |
| Financial institutions | Commercial banks | Number of branches | 36 | 53 | 31 |
| Microfinance institutions | Number of banks | 2 | 2 | 3 | |
| Economic growth | Average annual growth | Percentage | 2.5 | 1.97 | 2.16 |
| Parameters (Time Average) | Pakistan | Air Quality Level for South Asia Countries (µg/m3) | WHO Standard | ||||
|---|---|---|---|---|---|---|---|
| India | Nepal | Sri Lanka | Bangladesh | Bhutan | |||
| Carbon Monoxide (CO) (8 h) | 5 | 2 | 10,000 | 10,000 | 10 | 2000 | Not Applicable |
| Nitrogen Dioxide (NO2) (24 h) | 80 | 80 | 80 | 100 | Not given | Not given | Not Applicable |
| Sulphur Dioxide (SO2) (24 h) | 120 | 80 | 70 | 80 | 365 | 80 | 125 |
| Ozone (O3) (1 h) | 130 | 180 | Not given | 200 | 235 | Not given | 150–200 |
| Lead (Pb) (Annual) | 1 | 0.50 | 0.5 | Not given | 0.5 | Not given | 0.5–1 |
| Particulate Matter (PM10) (24 h) | 150 | 100 | 120 | 100 | 150 | 100 | 50 |
| Particulate Matter (PM2.5) (24 h) | 35 | 60 | Not given | 50 | 65 | Not given | 25 |
| Region in Pakistan | Indoor Setting | Source | Pollutant | Concentration | Health Hazards | Ref. |
|---|---|---|---|---|---|---|
| Lahore | Living area | Traffic/seasonal changes | PM2.5 | >25 μg/m3 | Not reported | [49] |
| Karachi | Restaurants/cafés/clubs | Indoor smoking; heating; cooking; hospitality | PM2.5 | 25–390 μg/m3 | Not reported | [54] |
| Rural areas of Pakistan | Living area/Kitchen | Use of biomass fuel; indoor cooking | PM10, PM2.5, PM1 | 4000–8555 μg/m3 | Not reported | [59] |
| Rural and urban areas of Pakistan | Living area/Kitchen | Indoor biomass burning | PM2.5, PM10 | PM10 (>50 μg/m3); PM2.5 (>25 μg/m3) | Not reported | [61] |
| Haripur city | Living area/Kitchen | Outside traffic | PM2.5, PM10 | PM2.5 23.7–126.0 μg/m3; PM10 39.0–166.3μg/m3; | Not reported | [65] |
| Lahore | Living area/Kitchen | Outside air due to industrial and traffic pollution | PM2.5, PM10, CO, NO2, SO2, O3 | Not reported | 64% of asthma patients | [66] |
| Northern Pakistan | Living area/Kitchen | Brick kilns | PM1, PM2.5, and PM10 | PM1, PM2.5, and PM10 concentrations 3377, 2305, and 3567.67 µg/m3, respectively. | Not reported | [67] |
| Rural areas | Living area/Kitchen | Indoor dust exposure/ingestion | Polybrominated diphenyl ether, polychlorinated biphenyl, tri- (2-butoxyethyl) phosphate, triphenyl phosphate | ~15.2 ng/kg bw/day | Not reported | [73] |
| Lahore, Faisalabad, Bahawalnagar | Living area/Kitchen | Indoor dust; polychlorinated biphenyl concentrations | Polychlorinated biphenyls | ~34.39 ng/g, 9.94 ng/g, and 8.79 ng/g in Lahore, Faisalabad, Bahawalnagar, respectively | Not reported | [75] |
| Rural regions | Living area/Kitchen | Unhealthy fuel (wood, crop residues, charcoal, coal, kerosene, and animal dung) | Exposure to CO2, CO | Not reported | Respiratory infections in children | [100] |
| Rural regions | Living area/Kitchen | Indoor biomass; fuel burning | PM, CO2, CO | PM level 200–5000 μg/m3 carbon monoxide (CO) level ~29.4 ppm | Not reported | [104] |
| Bungalows and apartments | Living area/Kitchen | Gas-fired kitchens | CO | CO concentrations in the range 2.13–5.29 ppm | Not reported | [106] |
| Lahore | Living area/Kitchen | Tobacco smoke | PM; CO2 emissions | Not reported | Coughing/ sneezing; eye irritation | [112] |
| Pakistan cities | Indoor restaurants, bars, and cafes | Indoor smoking | PM, CO2 emissions | High PM2.5 level ~1745 μg/m3 | Not reported | [113] |
| Urban/Rural areas | Living area/Kitchen | Indoor bacteria | Bioaerosols | Concentration high i.e., 14,650 cfu/m3 | Not reported | [131] |
| Lahore | Kitchens and living rooms | Microflora concentrations | Microflora | ~9829–14,469 cfu m−3 | Not reported | [138] |
| Rawalpindi and Islamabad | Living area/Kitchen | Indoor air | Polyaromatic hydrocarbon | ~2132 pgm−3; in dust ~90.0 ng·g−1 | Respiratory system/cancer risks | [165] |
| Urban areas | Offices | Indoor air | Brominated or phosphorated flame retardants | Flame retardants concentration 128,000 ng·g−1 | Loss of indoor working productivity | [72] |
| Lahore | Hospitals; operating theatres | Indoor air | PM | PM concentrations 757–970 μg/m3 | Repeated infections in patients | [179] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kausar, A.; Ahmad, I.; Zhu, T.; Shahzad, H. Impact of Indoor Air Pollution in Pakistan—Causes and Management. Pollutants 2023, 3, 293-319. https://doi.org/10.3390/pollutants3020021
Kausar A, Ahmad I, Zhu T, Shahzad H. Impact of Indoor Air Pollution in Pakistan—Causes and Management. Pollutants. 2023; 3(2):293-319. https://doi.org/10.3390/pollutants3020021
Chicago/Turabian StyleKausar, Ayesha, Ishaq Ahmad, Tianle Zhu, and Hassan Shahzad. 2023. "Impact of Indoor Air Pollution in Pakistan—Causes and Management" Pollutants 3, no. 2: 293-319. https://doi.org/10.3390/pollutants3020021