1. Introduction
Primary biliary cholangitis (PBC) is a chronic autoimmune illness that preferentially affects the interlobular bile channels (cholangitis), causing cholestasis, the retention of bile salts in the liver, and secondary hepatocyte damage. Although the disease can proceed to cirrhosis, liver failure, and death, the onset is frequently silent and sneaky [
1]. It is a chronic, autoimmune, slowly progressing liver condition that primarily affects middle-aged women at a ratio of about 10:1 [
2]. It has been discovered that genes associated with X-linked immunodeficiencies can cause granuloma formation and elevated immunoglobulin (Ig) M levels, which are frequent observations in PBC. X chromosome monosomy is observed in women with PBC, but the cause of this gender difference is not fully understood [
3].
The onset of cirrhosis and its complications, however, play a significant role in the disease’s outlook. All patients should begin and continue receiving ursodeoxycholic acid because it is linked to a better prognosis. The clinical outcome of ursodeoxycholic acid is correlated with the biochemical reaction, but patients with incomplete responses still have a better prognosis than those who do not receive treatment. Before the US Food and Drug Administration’s 2016 clearance of Obeticholic acid (OCA), UDCA was the only medication authorised for the treatment of PBC. Bezafibrate might work well as an off-label substitute for obeticholic acid, especially in patients with pruritus. Obeticholic acid was recently approved as a second-line treatment. Early results indicate a triple therapy using ursodeoxycholic acid, obeticholic acid, and bezafibrate, whereas other promising drugs are being evaluated in clinical trials [
4].
Obeticholic acid is an endogenous ligand for the farnesoid X receptor (FXR) that is produced from the bile acid chenodeoxycholic acid. When it comes to activating FXR, obeticholic acid is roughly 100 times more potent than chenodeoxycholic acid. Hepatocytes are protected from bile acid toxicity by FXR signalling, which reduces bile acid production and promotes choleresis by upregulating bile acid transporters. Additionally, FXR controls additional pathways with immediate anti-inflammatory and antifibrotic results [
5].
Nanotechnology has been progressively incorporated into and gradually adopted by numerous disciplines [
6,
7]. For example, nanometre drugs, or granules of the nano dimension, always have the special ability to be quickly absorbed while maintaining low concentrations and immunogenicity. Additionally, serum longevity and the pattern of deposition in the primed objects will be impacted by the variation in particle size. These disciplines all demonstrate how promising nanotechnology is as a method of drug discovery and clinical application. As an illustration, nanometre medicines, or nano-size granules, always have the special qualities of being readily taken while maintaining low concentrations and immunogenicity. Additionally, the diversification of particle size will have an impact on the pattern of deposition in the primed objects as well as serum longevity. These diverse fields of study demonstrate that nanotechnology is a potent approach for drug discovery and clinical implementation [
8,
9].
2. Pathophysiology of Primary Biliary Cholangitis
Intrahepatic bile duct damage, caused by inflammation and primarily T-cell-mediated, is a hallmark of PBC. The most widely accepted theory regarding the cause of PBC is that a genetically susceptible patient comes into contact with an autoimmune-triggering event, despite the fact that there is no absolute surety regarding this. A virus, allergen, chemical, or medicine could be the cause of this triggering incident. There is no single cause, and each patient’s immune system is triggered by different things. Genetic influences come from Major Histocompatibility Complex (MHC) class II genes (DR8, DQA1 × 0102, DQ/1 × 0402), MHC class III genes (C4 blank, C4B2), and non-MHC genes (Exon 1 of CTLA-4). Identified familial risk factors include PBC/positive anti-mitochondrial antibodies (AMA), impaired T-cell regulation, extrahepatic autoimmune diseases, and a greater prevalence in individuals who have a family member with PBC, particularly an identical twin. Recurrent urinary tract infections (possibly linked to exposure to bacterial components or antibiotic use), exposure to toxic chemicals, and cigarette smoking are examples of potential environmental factors, particularly in genetically vulnerable people. No matter what triggers the immunological reaction in PBC, biliary epithelial cells are the target. The E2 subunit of the Pyruvate Dehydrogenase Complex (PDC) is the primary target of anti-mitochondrial antibodies (AMA), which are extremely disease-specific and directed against the 2-oxo acid dehydrogenase family of multi-enzyme complexes found on the inner mitochondrial membrane. In PBC cases, the expression of PDC-E2 or a molecule that interacts with specific anti-PDC-E2 antibodies is elevated on biliary epithelial cells. Additionally, a number of molecular mimicry peptides to PDC-ER (found in viral or bacterial proteins) have epitopes that are chemically related to self-peptides. A loss of humoral tolerance and a rise in autoreactive CD4+CD8+PDC-E2-specific T cells in the liver are both possible effects of elevated PDC-E2. The biliary epithelial cells in the intrahepatic bile ducts’ lining are harmed during the subsequent autoimmune T cell reaction, which also causes inflammation, scarring, and the destruction of the interlobular and septal bile ducts. Bile then leaks through bile channels and into the liver parenchyma as a result. Bile ions damage hepatocytes, causing necrosis and apoptosis and leading to fibrosis and cirrhosis [
10].
3. Therapies
3.1. First-Line Transport
The medication UDCA (Ursodeoxycholic acid), also known as ursodiol (Actigall, Urso), is commonly used first. It helps move bile through your liver. UDCA does not cure primary biliary cholangitis, but it seems to improve liver function and reduce liver scarring. It is less likely to help with itching and fatigue. Its side effects may include weight gain, hair loss, and diarrhoea.
3.2. Second-Line Transport
The drugs used in second-line transport are Obeticholic acid (OCA), Benzafibrate, triple therapy (UDCA, OCA, Benzafibrate), and liver transplant [
10].
4. Obeticholic Acid
4.1. Invention and Development
The farnesoid X receptor (FXR), which plays a role in numerous physiological and pathological processes, was discovered to have the most physiologically active ligand in 1999. This receptor is found in the natural bile acid chenodeoxycholic acid. Roberto Pel-licciari and associates at the University of Perugia created, investigated, and patented a number of alkylated bile acid analogues, with 6 ethyl chenodeoxycholic acid emerging as the most powerful FXR agonist. FXR-dependent intestinal and liver functions have been suggested as potential therapeutic targets for human diseases. The first FXR agonist used in human drug trials was obeticholic acid [
11].
4.2. Description
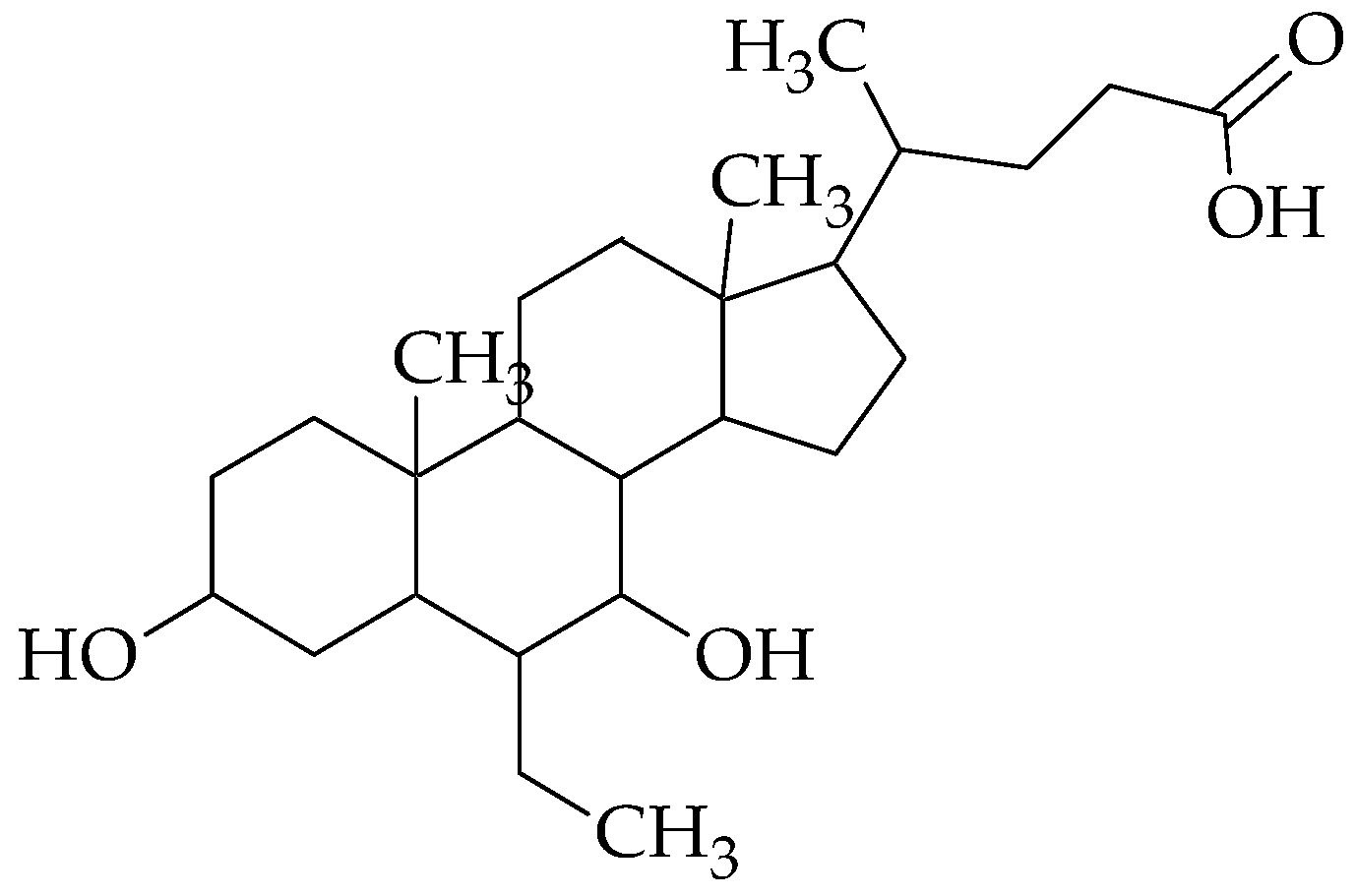
Obeticholic acid, an orally bioavailable semi-synthetic bile acid derivative and agonist of the nuclear bile acid receptor farnesoid X receptor (FXR), may be used to reduce liver exposure to bile acids. Following oral administration, obeticholic acid targets and binds to FXR expressed in the liver and gut, triggering FXR-mediated bile acid and inflammatory, fibrotic, and metabolic pathways. This decreases hepatic exposure to bile acids by inhibiting bile acid synthesis in the hepatocytes and increasing bile acid transport out of the hepatocytes. FXR is implicated in liver fibrosis, hepatic and intestinal inflammation, and bile acid homeostasis [
12]. The structure of obeticholic acid is shown in
Figure 1.
Category: Farnesoid X receptor agonists;
Structural name: Obeticholic acid;
Molecular formula: C26H44O4;
Chemical name: 6α-ethyl-chenodeoxycholic acid;
Molecular weight: 420.63 g/mol;
Description: white to off-white powder;
Melting point: 108–110 °C (226–230 °F)
Solubility: soluble in methanol, acetone, and ethyl acetate.
4.3. Mechanism of Action
Obeticholic acid is a brand-new variant of the main biliary acid in humans, chenodeoxycholic acid (BA). OCA is an FXR agonist, which plays a significant part in the enterohepatic circulation of Bas. FXR is a nuclear receptor that is primarily expressed in the gastrointestinal tract (liver and intestine). The main intracellular BA receptor, or FXR, controls a number of metabolic procedures involved in BA synthesis, transport, and detoxification.
By inducing a change in transcription, FXR carries out its intended tasks. With different regions involved in DNA binding, ligand binding, and transactivation, the protein has a multidomain structure.
As a consequence of ligand binding, co-bound co-repressor proteins become dissociated, and co-activator proteins are recruited, which increases the expression of the target gene [
13].
5. Obeticholic Acid Action on Primary Biliary Cholangitis
The major human bile acid chenodeoxycholic acid is the source of OCA (6-ethyl-chenodeoxycholic acid), a selective Farnesoid-X-receptor (FXR) agonist that has been chemically altered to make it 100 times more effective than chenodeoxycholic acid. The liver, colon, adrenal glands, and kidneys all express the FXR nuclear receptor, which is important for the production and enterohepatic circulation of bile acids. By downregulating the main enzymes involved in the synthesis of bile acids, cytochrome P450 7A1 (CYP7A1) and CYP8B1, and upregulating the expression of bilirubin exporter pumps, FXR activation in the liver decreases the conversion of cholesterol to bile acids. The sodium-dependent bile acid transporter is downregulated in the ileum by activation of the FXR receptor, which also reduces bile acid synthesis by raising the expression of fibroblast growth factor in the liver by inhibiting CYP7A1. OCA thus improves bile flow in cholestatic circumstances, protecting the hepatocytes from the build-up of cytotoxic bile acids. OCA is also anti-inflammatory and possesses antifibrotic characteristics, according to a number of preclinical investigations [
14].
6. Approaches of Nanotechnology
Applications of nanotechnology to medicine and physiology entail the development of materials and tools with a high degree of specificity for subcellular (i.e., molecular) interactions with the body. This may translate into cellular- and tissue-specific clinical interventions aimed at maximizing therapeutic effectiveness with minimum adverse effects. Additionally, nanomedicine offers a novel strategy that concentrates on tolerance induction rather than immunosuppression, offering great promise for the therapy of autoimmune diseases. Immune-modifying agents can be engineered into tolerogenic nanoparticles to safely and efficiently target the antigen-specific immune response in autoimmune diseases. Given the anatomical characteristics and immunological sensitivity of PBC, these may be particularly effective.
There was a method put forth that specifically manipulates LSECs (liver sinusoidal endothelial cells) to activate NKT (natural killer T cells)-cell-mediated liver cancer immunotherapy using obeticholic acid (OCA), a selective farnesoid X receptor (FXR) agonist that is clinically authorised. Studies on the in vivo biodistribution of the injected OCA-NE (Obeticholic acid nanoemulsion) showed that it mostly collected in the liver, particularly in LSECs and Kupffer cells. As a result, OCA-NE treatment greatly inhibited the growth of the hepatic tumour in a murine orthotopic H22 tumour model, outperforming the oral administration of free OCA. According to an immunologic study, the OCA-NE increased NKT cell populations inside the tumour as well as the secretion of CXCL16 (secretion of chemokine (C–X–C motif) ligand 16) and IFN (interferon). Overall, our study offers fresh proof of the antitumor activity of primary bile acid receptors, which should encourage the application of nanotechnology [
15,
16,
17,
18].
7. Conclusions
The recent approval of OCA, an FXR agonist, in the treatment of PBC is an important advance for patients who are at an increased risk of liver-related complications despite UDCA therapy or are unable to tolerate UDCA. OCA is registered for the treatment of primary biliary cholangitis. PBC is an autoimmune disease of the liver characterised by cirrhosis, cholestasis, fibrosis, and the destruction and inflammation of the intrahepatic bile ducts. In this review, we concentrated on numerous nanotechnology therapeutic modalities for liver illness or PBC. Immune-modifying drugs can be incorporated into tolerogenic nanoparticles to safely and effectively target the antigen-specific immune response in autoimmune disorders. Additionally, it has been shown that an OCA nanoemulsion can control the liver’s antitumor immunity and the CXCR6/CXCL16-dependent increase in NKT cells.
Author Contributions
Conceptualization, D.P. and J.P.; resources, M.P.; data curation, J.P. and T.G.; writing—original draft preparation, K.P.; writing—review and editing, D.P. and M.P.; visualization, D.P.; supervision, J.P.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
All authors would like to convey our thanks to Management and Principal, P.S.G.V.P. Mandal’s College of Pharmacy, Shahada, Dist. Nandurbar, for furnishing all the essential facilities to accomplish this review work.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Invernizzi, P.; Floreani, A.; Carbone, M.; Marzioni, M.; Craxi, A.; Muratori, L.; Gentilucci, U.V.; Gardini, I.; Gasbarrini, A.; Kruger, P.; et al. Primary Biliary Cholangitis: Advances in management and treatment of the disease. Dig. Liver Dis. 2017, 49, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Selmi, C.; Bowlus, C.L.; Gershwin, M.E.; Coppel, R.L. Primary biliary cirrhosis. Lancet 2011, 377, 1600–1609. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, P.; Miozzo, M.; Battezzati, P.M.; Bianchi, I.; Grati, F.R.; Simoni, G.; Selmi, C.; Watnik, M.; Gershwin, M.E.; Podda, M. Frequency of monosomy X in women with primary biliary cirrhosis. Lancet 2004, 363, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Laschtowitz, A.; de Veer, R.C.; Van der Meer, A.J.; Schramm, C. Diagnosis and treatment of primary Biliary cholangitis. United European Gastroenterol. J. 2020, 8, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Nevens, F.; Andreone, P.; Mazzella, G.; Strasser, S.I. A Placebo-Controlled Trial of Obeticholic Acid in Primary Biliary Cholangitis. N. Engl. J. Med. 2016, 375, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Chan, V.S. Nanomedicine: An unresolved regulatory issue. Regul. Toxicol. Pharmacol. 2006, 46, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.K. The role of nanobiotechnology in drug discovery. Drug Discov. Today 2005, 10, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Groneberg, D.A.; Giersig, M.; Welte, T.; Pison, U. Nanoparticle-based Diagnosis and therapy. Curr. Drug Targets 2006, 7, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Datar, R.H. Medical applications of nanotechnology. Natl. Med. J. India 2006, 19, 27–32. [Google Scholar] [PubMed]
- Younossi, Z.M.; Bernstein, D.; Shiffman, M.L.; Kwo, P.; Kim, W.R.; Kowdley, K.V.; Jacobson, I.M. Diagnosis and Management of Primary Biliary Cholangitis. Am. J. Gastroenterol. 2019, 114, 48–63. [Google Scholar]
- Obeticholic Acid. Available online: https://en.wikipedia.org/wiki/Obeticholic_acid (accessed on 28 February 2023).
- Obeticholic Acid. Available online: https://pubchem.ncbi.nlm.nih.gov (accessed on 28 February 2023).
- Obeticholic Acid. Available online: https://flipper.diff.org (accessed on 28 February 2023).
- Jhaveri, M.A.; Kowdley, K.V. New developments in the Treatment of primary biliary cholangitis—Role of obeticholic acid. Ther. Clin. Risk Manag. 2017, 13, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, S.K.; Parveen, S.; Panda, J.J. The present and future of nanotechnology in human health care. Nanomed 2007, 3, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Wang, L.; Woo, E.; He, X.; Yang, G.; Bowlus, C.; Leung, P.S.C.; Gershwin, M.E. Clinical Management of Primary Biliary Cholangitis-Strategies and Evolving Trends. Clin. Rev. Allergy Immunol. 2020, 59, 175–194. [Google Scholar] [CrossRef] [PubMed]
- Ji, G.; Ma, L.; Yao, H.; Ma, S.; Si, X.; Wang, Y.; Bao, X.; Ma, L.; Chen, F.; Ma, C.; et al. Precise delivery of obeticholic acid via nanoapproach for triggering natural killer T cell-mediated liver cancer immunotherapy. Acta Pharm. Sin. B 2020, 10, 2171–2182. [Google Scholar] [CrossRef] [PubMed]
- Patil, J.; Sayyed, H.; Suryawanshi, H.; Patil, B. Formulation and Evaluation of Verdant Tablets Containing Saponin-Coalesced Silver Nanoparticles Got from Fenugreek Seed Extract. Chem. Proc. 2022, 8, 56. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



{kind=link}
