
Perfecting the Puzzle of Pathophysiology: Exploring Combination Therapy in the Treatment of Type 2 Diabetes


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
Case
2. Current Guidelines for Treating T2DM: Are They Effective?
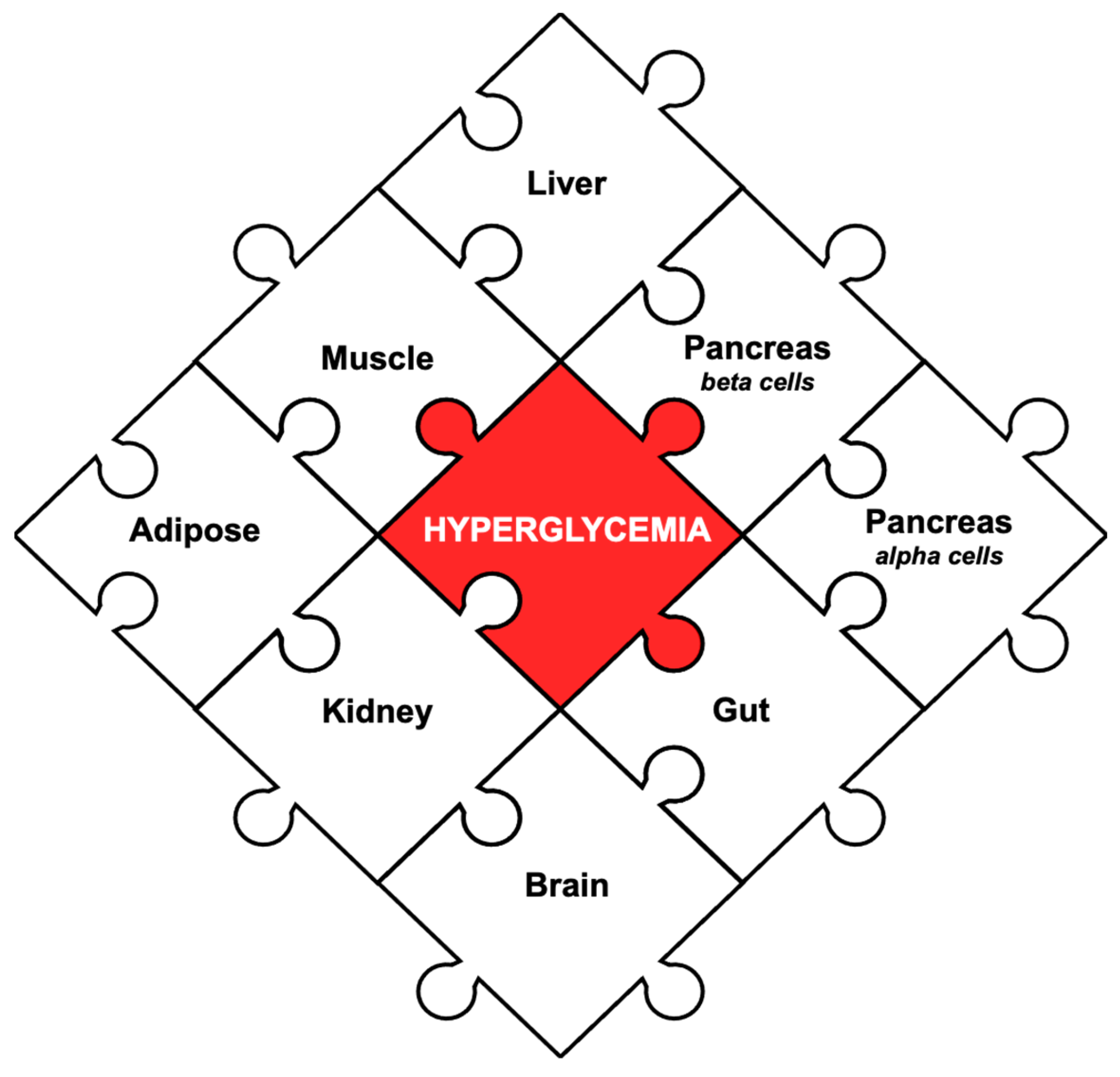
3. Pathophysiology of T2DM: The Ominous Octet Theory
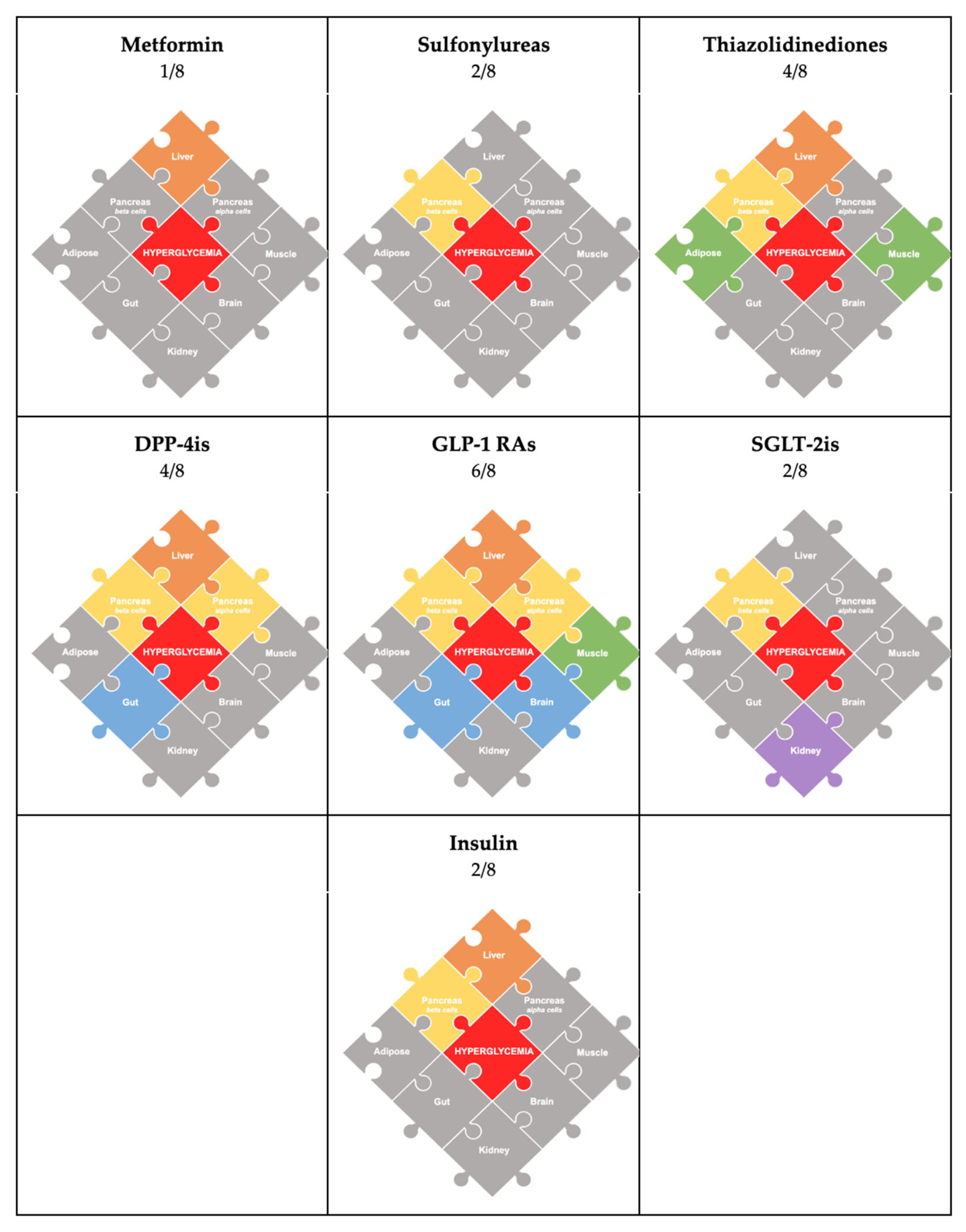
4. Antihyperglycemic Agents (Figure 2: Color-Coded by Medication)
5. Monotherapy vs. Dual Therapy
6. Existing Combination Studies
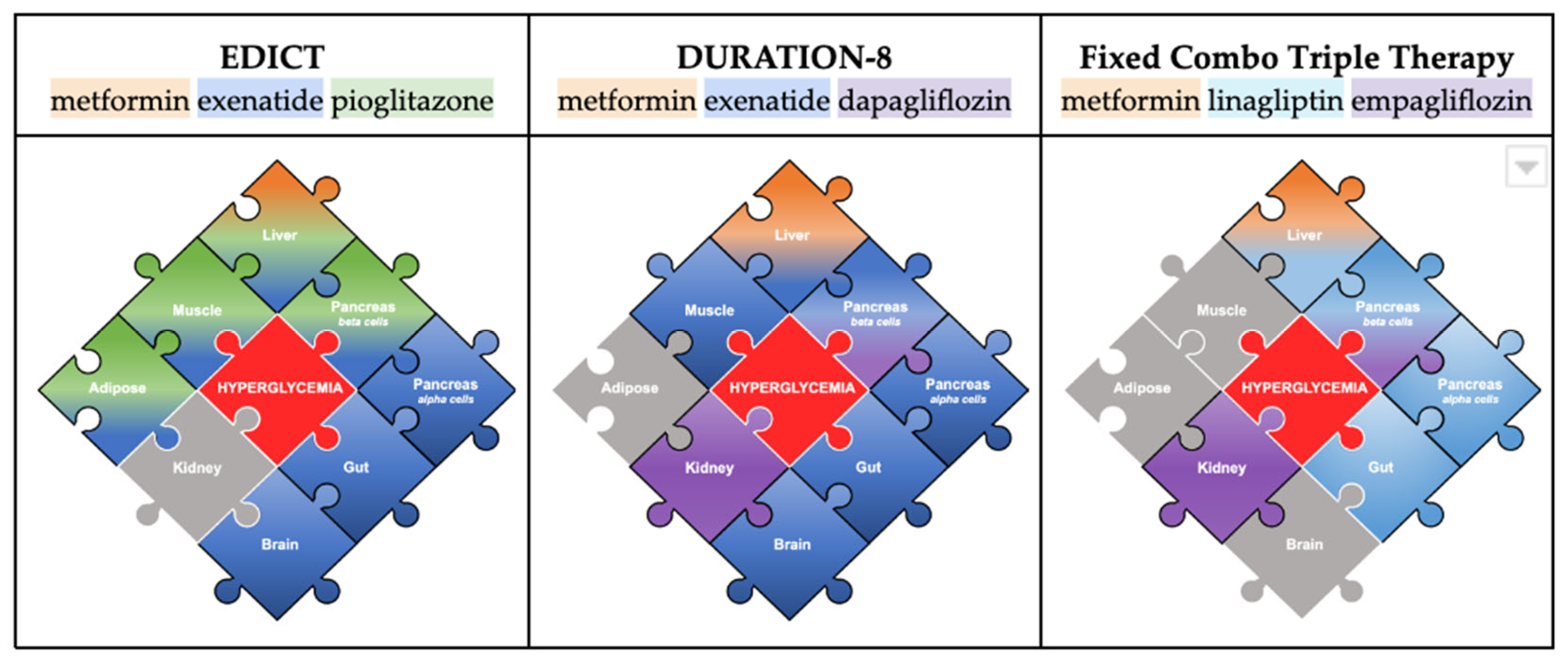
6.1. Combination of Metformin, TZD, and GLP-1RA (7/8 of the Puzzle Addressed)
6.2. Combination of Metformin, GLP-1RA, and SGLT-2i (7/8 of the Puzzle Addressed)
6.3. Fixed-Combination Therapy: Metformin, DPP-4i, SGLT-2i (5/8 of the Puzzle Addressed)
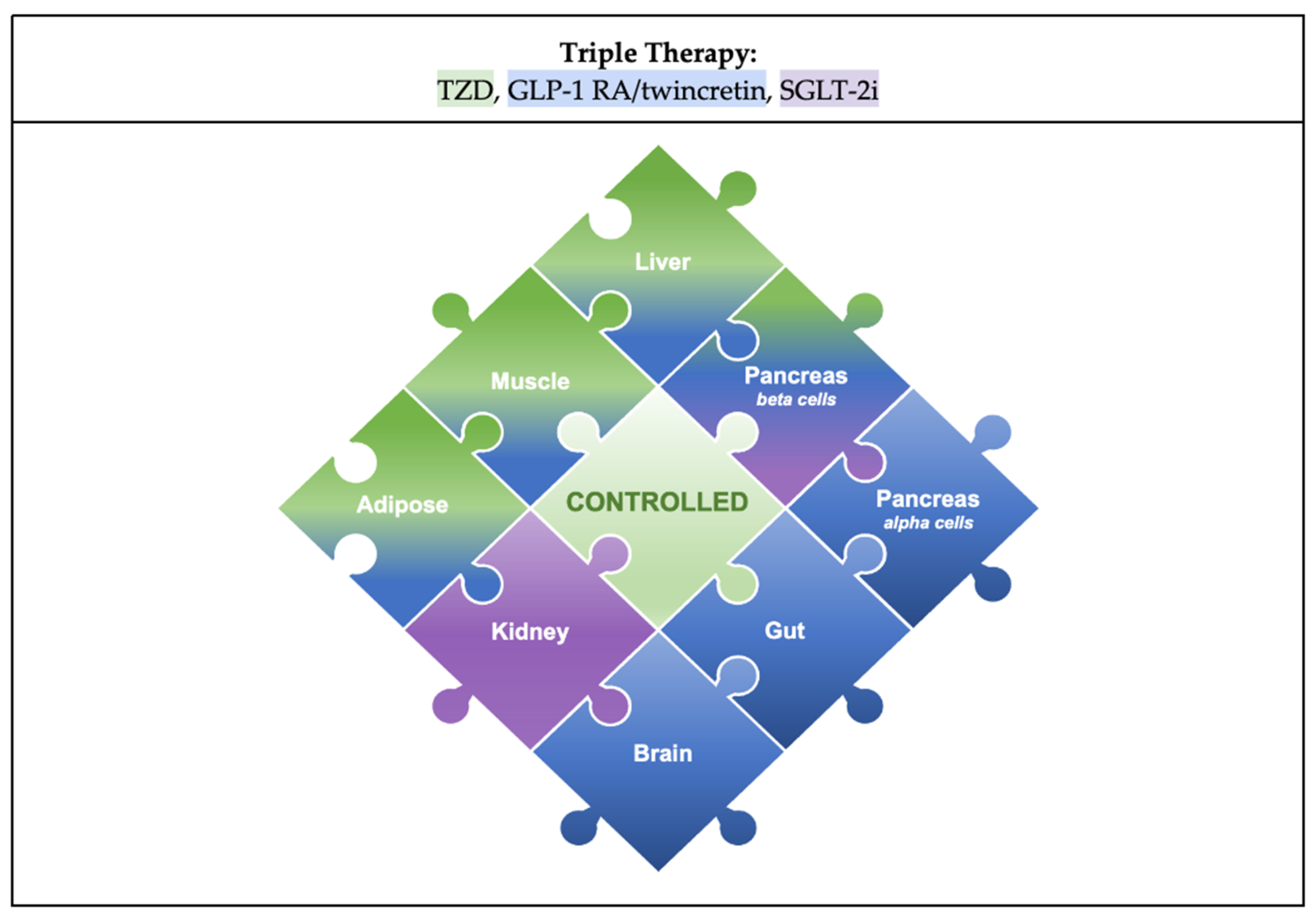
7. Ideal Combination
8. Therapy Approach: Glucocentric or Cardio–Renal-Centric?
9. Limitations
10. Back to the Case
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report Website. Available online: https://www.cdc.gov/diabetes/data/statistics-report/index.html (accessed on 25 January 2023).
- Statistics about Diabetes [Internet]. Statistics about Diabetes|ADA. Available online: https://diabetes.org/about-us/statistics/about-diabetes (accessed on 25 January 2023).
- Fang, M.; Wang, D.; Coresh, J.; Selvin, E. Trends in Diabetes Treatment and Control in U.S. Adults, 1999–2018. N. Engl. J. Med. 2021, 384, 2219–2228. [Google Scholar] [CrossRef]
- Blonde, L.; Umpierrez, G.E.; Reddy, S.S.; McGill, J.B.; Berga, S.L.; Bush, M.; Chandrasekaran, S.; DeFronzo, R.A.; Einhorn, D.; Galindo, R.J.; et al. American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan-2022 Update. Endocr. Pract. 2022, 28, 923–1049. [Google Scholar] [CrossRef] [PubMed]
- American Association of Clinical Endocrinology [Internet]. Available online: https://pro.aace.com/pdfs/diabetes/AACE_2019_Diabetes_Algorithm_03.2021.pdf (accessed on 25 January 2023).
- Cahn, A.; Cefalu, W.T. Clinical Considerations for Use of Initial Combination Therapy in Type 2 Diabetes. Diabetes Care 2016, 39 (Suppl. S2), S137–S145. [Google Scholar] [CrossRef]
- Abdul-Ghani, M.A.; Puckett, C.; Triplitt, C.; Maggs, D.; Adams, J.; Cersosimo, E.; DeFronzo, R.A. Initial combination therapy with metformin, pioglitazone and exenatide is more effective than sequential add-on therapy in subjects with new-onset diabetes. Results from the Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes (EDICT): A randomized trial. Diabetes Obes. Metab. 2015, 17, 268–275. [Google Scholar] [CrossRef]
- Phung, O.J.; Sobieraj, D.M.; Engel, S.S.; Rajpathak, S.N. Early combination therapy for the treatment of type 2 diabetes mellitus: Systematic review and meta-analysis. Diabetes Obes. Metab. 2014, 16, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.; Kamaruddin, N.A.; Visvanathan, J.; Santani, R. Defining Disease Progression and Drug Durability in Type 2 Diabetes Mellitus. Eur. Endocrinol. 2019, 15, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41, 2669–2701. [Google Scholar] [CrossRef]
- Jabbour, S. Durability of response to dapagliflozin: A review of long-term efficacy and safety. Curr. Med. Res. Opin. 2017, 33, 1685–1696. [Google Scholar] [CrossRef] [PubMed]
- Karamanou, M.; Protogerou, A.; Tsoucalas, G.; Androutsos, G.; Poulakou-Rebelakou, E. Milestones in the history of diabetes mellitus: The main contributors. World J. Diabetes 2016, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A. Lilly lecture 1987. The triumvirate: Beta-cell, muscle, liver. A collusion responsible for NIDDM. Diabetes 1988, 37, 667–687. [Google Scholar] [CrossRef] [PubMed]
- Defronzo, R.A. Banting Lecture. From the triumvirate to the ominous octet: A new paradigm for the treatment of type 2 diabetes mellitus. Diabetes 2009, 58, 773–795. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E.; Barrett, E.J.; Bevilacqua, S.; DeFronzo, R.A. Effect of fatty acids on glucose production and utilization in man. J. Clin. Investig. 1983, 72, 1737–1747. [Google Scholar] [CrossRef] [PubMed]
- Roden, M.; Price, T.B.; Perseghin, G.; Petersen, K.F.; Rothman, D.L.; Cline, G.W.; Shulman, G.I. Mechanism of free fatty acid-induced insulin resistance in humans. J. Clin. Investig. 1996, 97, 2859–2865. [Google Scholar] [CrossRef] [PubMed]
- Kashyap, S.; Belfort, R.; Gastaldelli, A.; Pratipanawatr, T.; Berria, R.; Pratipanawatr, W.; Bajaj, M.; Mandarino, L.; DeFronzo, R.; Cusi, K. A sustained increase in plasma free fatty acids impairs insulin secretion in nondiabetic subjects genetically predisposed to develop type 2 diabetes. Diabetes 2003, 52, 2461–2474. [Google Scholar] [CrossRef] [PubMed]
- Meier, J.J.; Nauck, M.A. Incretins and the development of type 2 diabetes. Curr. Diab Rep. 2006, 6, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Cervera, A.; Wajcberg, E.; Sriwijitkamol, A.; Fernandez, M.; Zuo, P.; Triplitt, C.; Musi, N.; DeFronzo, R.A.; Cersosimo, E. Mechanism of action of exenatide to reduce postprandial hyperglycemia in type 2 diabetes. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E846–E852. [Google Scholar] [CrossRef] [PubMed]
- Baron, A.D.; Schaeffer, L.; Shragg, P.; Kolterman, O.G. Role of hyperglucagonemia in maintenance of increased rates of hepatic glucose output in type II diabetics. Diabetes 1987, 36, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Defronzo, R.A.; Glass, L.; Consoli, A.; Giordano, M.; Bressler, P.; Delprato, S. Glucagon dose-response curve for hepatic glucose production and glucose disposal in type 2 diabetic patients and normal individuals. Metabolism 2002, 51, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Rahmoune, H.; Thompson, P.W.; Ward, J.M.; Smith, C.D.; Hong, G.; Brown, J. Glucose transporters in human renal proximal tubular cells isolated from the urine of patients with non-insulin-dependent diabetes. Diabetes 2005, 54, 3427–3434. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Liu, Y.; Mahankali, S.; Pu, Y.; Mahankali, A.; Wang, J.; DeFronzo, R.A.; Fox, P.T.; Gao, J.H. Altered hypothalamic function in response to glucose ingestion in obese humans. Diabetes 1999, 48, 1801–1806. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.S.; Epstein, S.; Corkey, B.E.; Grant, S.F.; Gavin, J.R., 3rd; Aguilar, R.B. The Time Is Right for a New Classification System for Diabetes: Rationale and Implications of the beta-Cell-Centric Classification Schema. Diabetes Care 2016, 39, 179–186. [Google Scholar] [CrossRef]
- Kahn, S.E.; Haffner, S.M.; Heise, M.A.; Herman, W.H.; Holman, R.R.; Jones, N.P.; Kravitz, B.G.; Lachin, J.M.; O’Neill, M.C.; Zinman, B.; et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N. Engl. J. Med. 2006, 355, 2427–2443. [Google Scholar] [CrossRef]
- Sherifali, D.; Nerenberg, K.; Pullenayegum, E.; Cheng, J.E.; Gerstein, H.C. The effect of oral antidiabetic agents on A1C levels: A systematic review and meta-analysis. Diabetes Care 2010, 33, 1859–1864. [Google Scholar] [CrossRef]
- Veelen, A.; Erazo-Tapia, E.; Oscarsson, J.; Schrauwen, P. Type 2 diabetes subgroups and potential medication strategies in relation to effects on insulin resistance and beta-cell function: A step toward personalised diabetes treatment? Mol. Metab. 2021, 46, 101158. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A.; Inzucchi, S.; Abdul-Ghani, M.; Nissen, S.E. Pioglitazone: The forgotten, cost-effective cardioprotective drug for type 2 diabetes. Diabetes Vasc. Dis. Res. 2019, 16, 133–143. [Google Scholar] [CrossRef] [PubMed]
- van Baar, M.J.B.; van Ruiten, C.C.; Muskiet, M.H.A.; van Bloemendaal, L.; RG, I.J.; van Raalte, D.H. SGLT2 Inhibitors in Combination Therapy: From Mechanisms to Clinical Considerations in Type 2 Diabetes Management. Diabetes Care 2018, 41, 1543–1556. [Google Scholar] [CrossRef]
- Rizvi, A.A.; Linhart, A.; Vrablik, M.; Liberopoulos, E.; Rizzo, M. Safety and benefit of incretin-based therapies in patients with type 2 diabetes: Learnings and reflections. Expert Opin. Drug Saf. 2022, 21, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Makrilakis, K. The Role of DPP-4 Inhibitors in the Treatment Algorithm of Type 2 Diabetes Mellitus: When to Select, What to Expect. Int. J. Environ. Res. Public Health 2019, 16, 2720. [Google Scholar] [CrossRef] [PubMed]
- Ostergaard, L.; Frandsen, C.S.; Madsbad, S. Treatment potential of the GLP-1 receptor agonists in type 2 diabetes mellitus: A review. Expert Rev. Clin. Pharmacol. 2016, 9, 241–265. [Google Scholar] [CrossRef]
- Sandoval, D.; Sisley, S.R. Brain GLP-1 and insulin sensitivity. Mol. Cell. Endocrinol. 2015, 418 Pt 1, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Huang, T.; Chen, A.; Chen, X.; Wang, L.; Shen, F.; Gu, X. Glucagon-like peptide 1 improves insulin resistance in vitro through anti-inflammation of macrophages. Braz. J. Med. Biol. Res. 2016, 49, e5826. [Google Scholar] [CrossRef] [PubMed]
- Buteau, J.; El-Assaad, W.; Rhodes, C.J.; Rosenberg, L.; Joly, E.; Prentki, M. Glucagon-like peptide-1 prevents beta cell glucolipotoxicity. Diabetologia 2004, 47, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Holst, J.J.; Madsbad, S. Semaglutide seems to be more effective the other GLP-1Ras. Ann. Transl. Med. 2017, 5, 505. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Sathyapalan, T.; Sahebkar, A. Molecular mechanisms by which GLP-1 RA and DPP-4i induce insulin sensitivity. Life Sci. 2019, 234, 116776. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, S. Tirzepatide: A Novel, Once-weekly Dual GIP and GLP-1 Receptor Agonist for the Treatment of Type 2 Diabetes. touchREV Endocrinol. 2022, 18, 10–19. [Google Scholar] [CrossRef]
- Zaccardi, F.; Webb, D.R.; Htike, Z.Z.; Youssef, D.; Khunti, K.; Davies, M.J. Efficacy and safety of sodium-glucose co-transporter-2 inhibitors in type 2 diabetes mellitus: Systematic review and network meta-analysis. Diabetes Obes. Metab. 2016, 18, 783–794. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Mayfield, J.A.; White, R.D. Insulin therapy for type 2 diabetes: Rescue, augmentation, and replacement of beta-cell function. Am. Fam. Physician 2004, 70, 489–500. [Google Scholar]
- Kramer, C.K.; Zinman, B.; Retnakaran, R. Short-term intensive insulin therapy in type 2 diabetes mellitus: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2013, 1, 28–34. [Google Scholar] [CrossRef]
- Brown, J.B.; Conner, C.; Nichols, G.A. Secondary failure of metformin monotherapy in clinical practice. Diabetes Care 2010, 33, 501–506. [Google Scholar] [CrossRef]
- Christensen, D.H.; Rungby, J.; Thomsen, R.W. Nationwide trends in glucose-lowering drug use, Denmark, 1999–2014. Clin. Epidemiol. 2016, 8, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.C.; Cull, C.A.; Frighi, V.; Holman, R.R. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: Progressive requirement for multiple therapies (UKPDS 49). UK Prospective Diabetes Study (UKPDS) Group. JAMA 1999, 281, 2005–2012. [Google Scholar] [CrossRef] [PubMed]
- Bennett, W.L.; Maruthur, N.M.; Singh, S.; Segal, J.B.; Wilson, L.M.; Chatterjee, R.; Marinopoulos, S.S.; Puhan, M.A.; Ranasinghe, P.; Block, L.; et al. Comparative effectiveness and safety of medications for type 2 diabetes: An update including new drugs and 2-drug combinations. Ann. Intern. Med. 2011, 154, 602–613. [Google Scholar] [CrossRef] [PubMed]
- Richard, J.W., 3rd; Raskin, P. Updated review: Improved glycemic control with repaglinide-metformin in fixed combination for patients with type 2 diabetes. Clin. Med. Insights Endocrinol. Diabetes 2011, 4, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Ghani, M.; Puckett, C.; Adams, J.; Khattab, A.; Baskoy, G.; Cersosimo, E.; Triplitt, C.; DeFronzo, R.A. Durability of Triple Combination Therapy Versus Stepwise Addition Therapy in Patients with New-Onset T2DM: 3-Year Follow-Up of EDICT. Diabetes Care 2021, 44, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, S.A.; Frias, J.P.; Ahmed, A.; Hardy, E.; Choi, J.; Sjostrom, C.D.; Guja, C. Efficacy and Safety Over 2 Years of Exenatide Plus Dapagliflozin in the DURATION-8 Study: A Multicenter, Double-Blind, Phase 3, Randomized Controlled Trial. Diabetes Care 2020, 43, 2528–2536. [Google Scholar] [CrossRef]
- John, M.; Gopinath, D.; Kalra, S. Triple fixed drug combinations in type 2 diabetes. Indian J. Endocrinol. Metab. 2015, 19, 311–313. [Google Scholar] [CrossRef]
- Tiv, M.; Viel, J.F.; Mauny, F.; Eschwege, E.; Weill, A.; Fournier, C.; Fagot-Campagna, A.; Penfornis, A. Medication adherence in type 2 diabetes: The ENTRED study 2007, a French Population-Based Study. PLoS ONE 2012, 7, e32412. [Google Scholar] [CrossRef]
- Donnan, P.T.; MacDonald, T.M.; Morris, A.D. Adherence to prescribed oral hypoglycaemic medication in a population of patients with Type 2 diabetes: A retrospective cohort study. Diabet. Med. 2002, 19, 279–284. [Google Scholar] [CrossRef]
- Abramowicz, M.; Zuccotti, G.; Pflomm, J.-M. Trijardy XR-A New 3-Drug Combination for Type 2 Diabetes. JAMA 2020, 324, 2437–2438. [Google Scholar] [CrossRef]
- Raedler, L.A. Glyxambi (Empagliflozin/Linagliptin): A Dual-Acting Oral Medication Approved for the Treatment of Patients with Type 2 Diabetes. Am. Health Drug Benefits 2015, 8, 171–175. [Google Scholar] [PubMed]
- Huri, H.Z.; Lim, L.P.; Lim, S.K. Glycemic control and antidiabetic drugs in type 2 diabetes mellitus patients with renal complications. Drug Des. Devel Ther. 2015, 9, 4355–4371. [Google Scholar] [CrossRef] [PubMed]
- Razavi, M.; Wei, Y.Y.; Rao, X.Q.; Zhong, J.X. DPP-4 inhibitors and GLP-1RAs: Cardiovascular safety and benefits. Mil. Med. Res. 2022, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V. Glucagon-like peptide-1 analogues: An overview. Indian J. Endocrinol. Metab. 2013, 17, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Caramelli, B.; Gualandro, D.M. Both glucocentric and cardiocentric approaches are necessary for a resilient disease such as diabetes. Rev. Assoc. Med. Bras. 2018, 64, 212–213. [Google Scholar] [CrossRef]
- Jacob, S.; Krentz, A.J.; Deanfield, J.; Ryden, L. Evolution of Type 2 Diabetes Management from a Glucocentric Approach to Cardio-Renal Risk Reduction: The New Paradigm of Care. Drugs 2021, 81, 1373–1379. [Google Scholar] [CrossRef]
- Sun, F.; Chai, S.; Li, L.; Yu, K.; Yang, Z.; Wu, S.; Zhang, Y.; Ji, L.; Zhan, S. Effects of glucagon-like peptide-1 receptor agonists on weight loss in patients with type 2 diabetes: A systematic review and network meta-analysis. J. Diabetes Res. 2015, 2015, 157201. [Google Scholar] [CrossRef]
- Sun, F.; Wu, S.; Guo, S.; Yu, K.; Yang, Z.; Li, L.; Zhang, Y.; Quan, X.; Ji, L.; Zhan, S. Impact of GLP-1 receptor agonists on blood pressure, heart rate and hypertension among patients with type 2 diabetes: A systematic review and network meta-analysis. Diabetes Res. Clin. Pract. 2015, 110, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.; Wu, S.; Wang, J.; Guo, S.; Chai, S.; Yang, Z.; Li, L.; Zhang, Y.; Ji, L.; Zhan, S. Effect of glucagon-like peptide-1 receptor agonists on lipid profiles among type 2 diabetes: A systematic review and network meta-analysis. Clin. Ther. 2015, 37, 225–241.e228. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.A.; Meier, J.J.; Cavender, M.A.; Abd El Aziz, M.; Drucker, D.J. Cardiovascular Actions and Clinical Outcomes with Glucagon-Like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors. Circulation 2017, 136, 849–870. [Google Scholar] [CrossRef]
- Dutour, A.; Abdesselam, I.; Ancel, P.; Kober, F.; Mrad, G.; Darmon, P.; Ronsin, O.; Pradel, V.; Lesavre, N.; Martin, J.C.; et al. Exenatide decreases liver fat content and epicardial adipose tissue in patients with obesity and type 2 diabetes: A prospective randomized clinical trial using magnetic resonance imaging and spectroscopy. Diabetes Obes. Metab. 2016, 18, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Caruso, I.; Cignarelli, A.; Sorice, G.P.; Natalicchio, A.; Perrini, S.; Laviola, L.; Giorgino, F. Cardiovascular and Renal Effectiveness of GLP-1 Receptor Agonists vs. Other Glucose-Lowering Drugs in Type 2 Diabetes: A Systematic Review and Meta-Analysis of Real-World Studies. Metabolites 2022, 12, 183. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.Y.Y. Why Choose Between SGLT2 Inhibitors and GLP1-RA When You Can Use Both?: The Time to Act Is Now. Circulation 2021, 143, 780–782. [Google Scholar] [CrossRef] [PubMed]
- Yki-Jarvinen, H. Thiazolidinediones. N. Engl. J. Med. 2004, 351, 1106–1118. [Google Scholar] [CrossRef]
- Promrat, K.; Lutchman, G.; Uwaifo, G.I.; Freedman, R.J.; Soza, A.; Heller, T.; Doo, E.; Ghany, M.; Premkumar, A.; Park, Y.; et al. A pilot study of pioglitazone treatment for nonalcoholic steatohepatitis. Hepatology 2004, 39, 188–196. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A.; Chilton, R.; Norton, L.; Clarke, G.; Ryder, R.E.; Abdul-Ghani, M. Revitalization of pioglitazone: The optimum agent to be combined with a sodium-glucose co-transporter-2 inhibitor. Diabetes Obes. Metab. 2016, 18, 454–462. [Google Scholar] [CrossRef]
- Choi, J.G.; Winn, A.N.; Skandari, M.R.; Franco, M.I.; Staab, E.M.; Alexander, J.; Wan, W.; Zhu, M.; Huang, E.S.; Philipson, L.; et al. First-Line Therapy for Type 2 Diabetes with Sodium-Glucose Cotransporter-2 Inhibitors and Glucagon-Like Peptide-1 Receptor Agonists: A Cost-Effectiveness Study. Ann. Intern. Med. 2022, 175, 1392–1400. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gudoor, R.; Suits, A.; Shubrook, J.H. Perfecting the Puzzle of Pathophysiology: Exploring Combination Therapy in the Treatment of Type 2 Diabetes. Diabetology 2023, 4, 379-392. https://doi.org/10.3390/diabetology4030032
Gudoor R, Suits A, Shubrook JH. Perfecting the Puzzle of Pathophysiology: Exploring Combination Therapy in the Treatment of Type 2 Diabetes. Diabetology. 2023; 4(3):379-392. https://doi.org/10.3390/diabetology4030032
Chicago/Turabian StyleGudoor, Ridhi, Austen Suits, and Jay H. Shubrook. 2023. "Perfecting the Puzzle of Pathophysiology: Exploring Combination Therapy in the Treatment of Type 2 Diabetes" Diabetology 4, no. 3: 379-392. https://doi.org/10.3390/diabetology4030032