
Predicting SARS-CoV-2 Variant Using Non-Invasive Hand Odor Analysis: A Pilot Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Hand Odor Collection
2.2. Confirmation of SARS-CoV-2 Infection
2.3. Sample Collection
2.4. Patient Demographics
2.5. HS-SPME- GC–MS Method
2.6. Data Pre-Processing
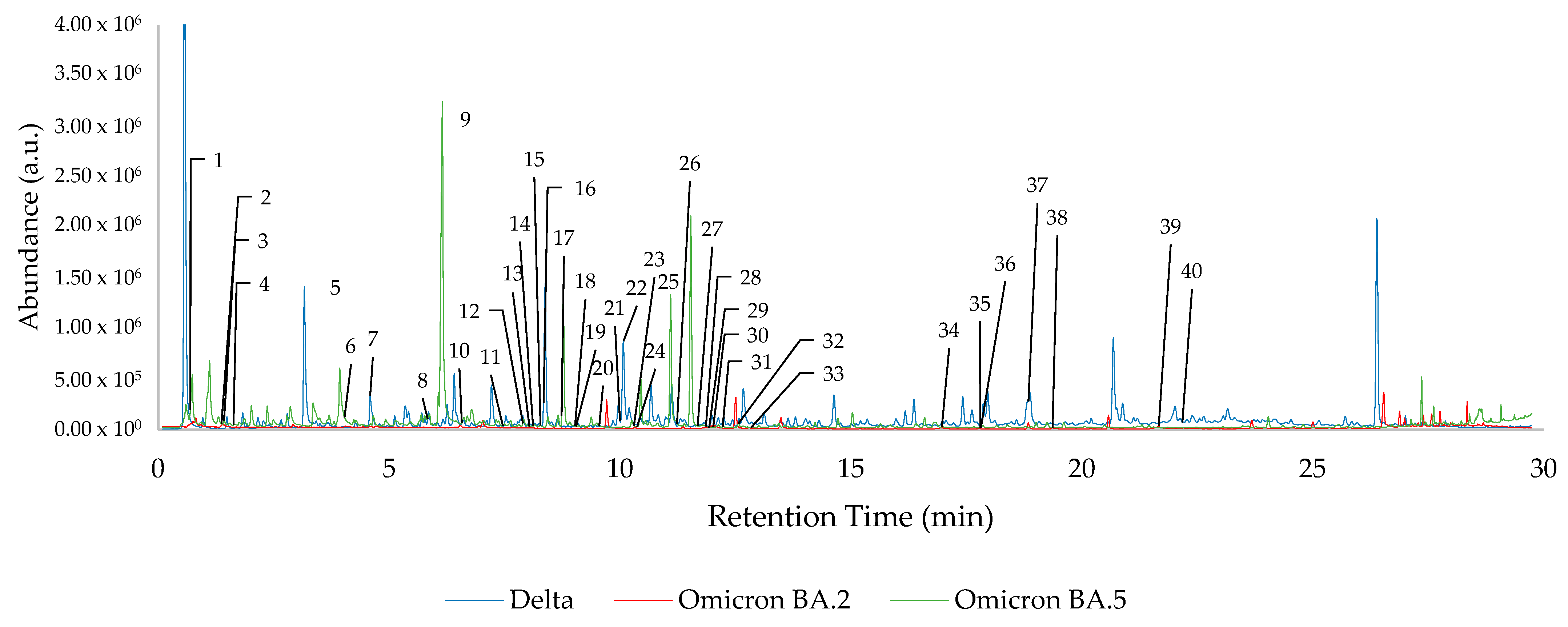
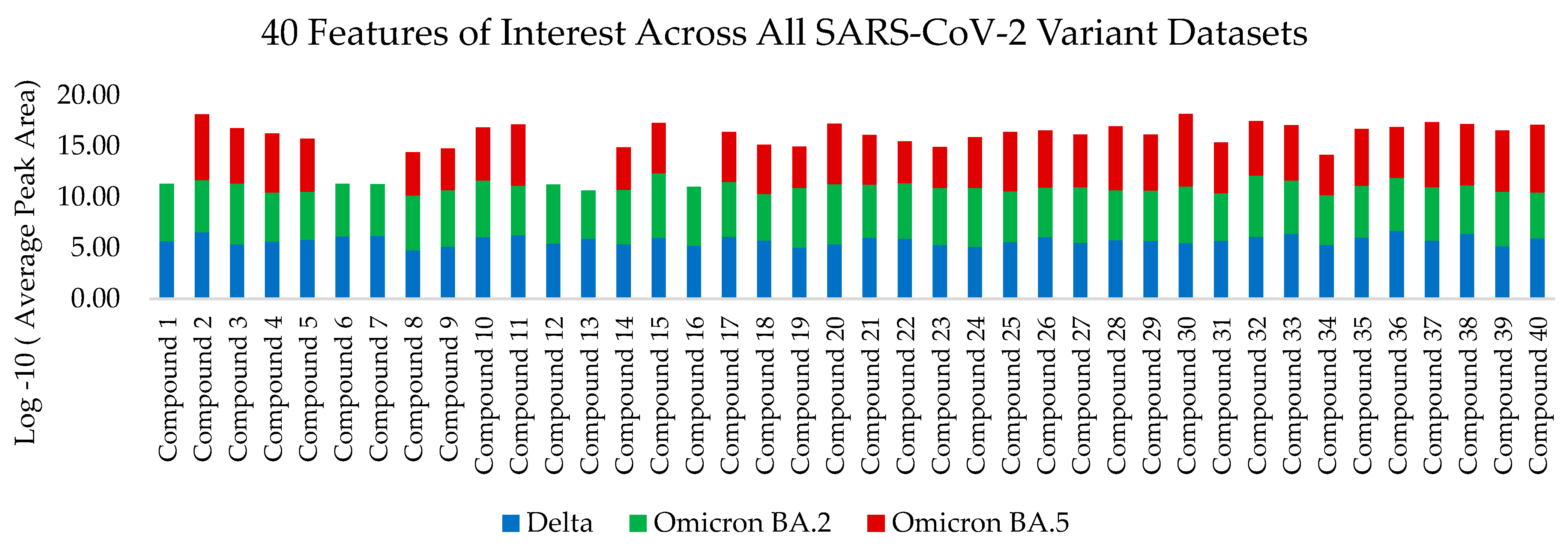
2.7. Features of Interest
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Delta | Omicron BA.2 | Omicron BA.5 | ||
|---|---|---|---|---|
| Race | Black | 18 | 4 | 17 |
| White | - | 8 | 6 | |
| Hispanic/Latinx | 1 | 1 | - | |
| Unknown | 1 | - | - | |
| Sex at Birth | Female | 13 | 10 | 13 |
| Male | 7 | 3 | 10 | |
| Age | 18–24 | - | 5 | 1 |
| 25–30 | 3 | 1 | 4 | |
| 31–45 | 8 | 2 | 4 | |
| 46–60 | 4 | 3 | 6 | |
| 60+ | 5 | 2 | 8 |

References
- Centers for Disease Control and Prevention, CDC. COVID Data Tracker: Variant Proportions. Available online: https://covid.cdc.gov/covid-data-tracker/#variant-proportions (accessed on 12 August 2022).
- Fernandes, Q.; Inchakalody, V.P.; Merhi, M.; Mestiri, S.; Taib, N.; Moustafa Abo El-Ella, D.; Bedhiafi, T.; Raza, A.; Al-Zaidan, L.; Mohsen, M.O.; et al. Emerging COVID-19 Variants and Their Impact on SARS-CoV-2 Diagnosis, Therapeutics and Vaccines. Ann. Med. 2022, 54, 524–540. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. SARS-CoV-2 Variant Classifications and Definitions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html#concern (accessed on 8 December 2022).
- Ninomiya, M.; Ueno, Y.; Funayama, R.; Nagashima, T.; Nishida, Y.; Kondo, Y.; Inoue, J.; Kakazu, E.; Kimura, O.; Nakayama, K.; et al. Use of Illumina Deep Sequencing Technology To Differentiate Hepatitis C Virus Variants. J. Clin. Microbiol. 2012, 50, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Hokynar, K.; Norja, P.; Laitinen, H.; Palomäki, P.; Garbarg-Chenon, A.; Ranki, A.; Hedman, K.; Söderlund-Venermo, M. Detection and Differentiation of Human Parvovirus Variants by Commercial Quantitative Real-Time PCR Tests. J. Clin. Microbiol. 2004, 42, 2013–2019. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.M.; Jackwood, M.W.; Gelb, J. Differentiation of Infectious Bronchitis Virus Serotypes Using Polymerase Chain Reaction and Restriction Fragment Length Polymorphism Analysis. Avian Dis. 1993, 37, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Vo, V.; Tillett, R.L.; Papp, K.; Shen, S.; Gu, R.; Gorzalski, A.; Siao, D.; Markland, R.; Chang, C.L.; Baker, H.; et al. Use of Wastewater Surveillance for Early Detection of Alpha and Epsilon SARS-CoV-2 Variants of Concern and Estimation of Overall COVID-19 Infection Burden. Sci. Total Environ. 2022, 835, 155410. [Google Scholar] [CrossRef] [PubMed]
- Erster, O.; Mendelson, E.; Levy, V.; Kabat, A.; Mannasse, B.; Asraf, H.; Azar, R.; Ali, Y.; Shirazi, R.; Bucris, E.; et al. Rapid and High-Throughput Reverse Transcriptase Quantitative PCR (RT-QPCR) Assay for Identification and Differentiation between SARS-CoV-2 Variants B.1.1.7 and B.1.351. Microbiol. Spectr. 2021, 9, e00506-21. [Google Scholar] [CrossRef] [PubMed]
- Roche. Roche Launches COVID-19 Test That Detects and Differentiates the Emerging Variant of Interest BA.2.75. Available online: https://www.prnewswire.com/news-releases/roche-launches-covid-19-test-that-detects-and-differentiates-the-emerging-variant-of-interest-ba2-75--301609342.html (accessed on 2 September 2022).
- Mendel, J.; Frank, K.; Edlin, L.; Hall, K.; Webb, D.; Mills, J.; Holness, H.K.; Furton, K.G.; Mills, D.E. Preliminary Accuracy of COVID-19 Odor Detection by Canines and HS-SPME-GC-MS Using Exhaled Breath Samples. Forensic Sci. Int. 2021, 3, 100155. [Google Scholar] [CrossRef] [PubMed]
- Ruszkiewicz, D.M.; Sanders, D.; O’Brien, R.; Hempel, F.; Reed, M.J.; Riepe, A.C.; Bailie, K.; Brodrick, E.; Darnley, K.; Ellerkmann, R.; et al. Diagnosis of COVID-19 by Analysis of Breath with Gas Chromatography-Ion Mobility Spectrometry—A Feasibility Study. EClinicalMedicine 2020, 29–30, 100609. [Google Scholar] [CrossRef] [PubMed]
- Gokool, V.A.; Crespo-Cajigas, J.; Mallikarjun, A.; Collins, A.; Kane, S.A.; Plymouth, V.; Nguyen, E.; Abella, B.S.; Holness, H.K.; Furton, K.G.; et al. The Use of Biological Sensors and Instrumental Analysis to Discriminate COVID-19 Odor Signatures. Biosensors 2022, 12, 1003. [Google Scholar] [CrossRef] [PubMed]
- Curran, A.M.; Rabin, S.I.; Furton, K.G. Analysis of the Uniqueness and Persistence of Human Scent. Forensic Sci. Commun. 2005, 7, 1–12. [Google Scholar]
- Shirasu, M.; Touhara, K. The Scent of Disease: Volatile Organic Compounds of the Human Body Related to Disease and Disorder. J. Biochem. 2011, 150, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Woollam, M.; Angarita-Rivera, P.; Siegel, A.P.; Kalra, V.; Kapoor, R.; Agarwal, M. Exhaled VOCs Can Discriminate Subjects with COVID-19 from Healthy Controls. J. Breath Res. 2022, 16, 036002. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Cajigas, J.; Gokool, V.A.; Ramírez Torres, A.; Forsythe, L.; Abella, B.S.; Holness, H.K.; Johnson, A.T.C.; Postrel, R.; Furton, K.G. Investigating the Use of SARS-CoV-2 (COVID-19) Odor Expression as a Non-Invasive Diagnostic Tool—Pilot Study. Diagnostics 2023, 13, 707. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. cobas SARS-CoV-2—Instructions For Use. Available online: https://www.fda.gov/media/136049/download (accessed on 14 January 2023).
- Food and Drug Administration. BINAXNOW COVID-19 AG CARD (PN 195-000)—INSTRUCTIONS FOR USE. Available online: https://www.fda.gov/media/141570/download (accessed on 14 January 2023).
- Le Cao, K.-A.; Rohart, F.; Gonzalez, I.; Dejean, S.; Gautier, B.; Bartolo, F.; Monget, P.; Coquery, J.; Yao, F.; Liquet, B. mixOmics: Omics Data Integration Project. R Package Version 6.1.1. Available online: https://CRAN.R-project.org/package=mixOmics (accessed on 11 August 2022).




| Dominant COVID-19 Variant at Time of Collection | Collection Timespan | # Samples |
|---|---|---|
| Delta | June–October 2021 | 20 |
| Omicron BA.2 | February–May 2022 | 13 |
| Omicron BA.5 | July–September 2022 | 23 |
| sPLS-DA Model Accuracy Rates | |||
|---|---|---|---|
| Suspected Variant | Delta vs. Omicron BA.2 | Omicron BA.2 vs. Omicron BA.5 | Delta vs. Omicron BA.5 |
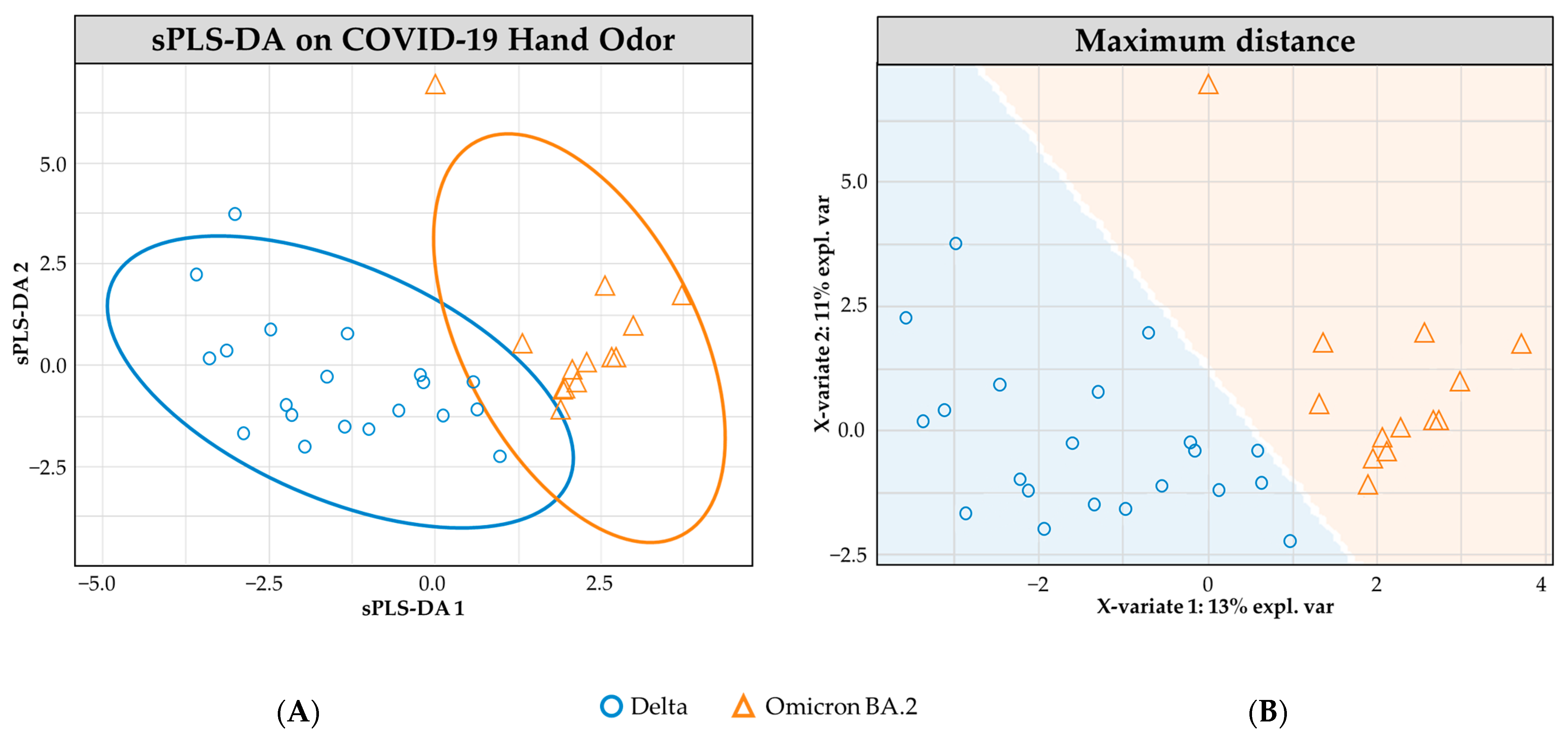
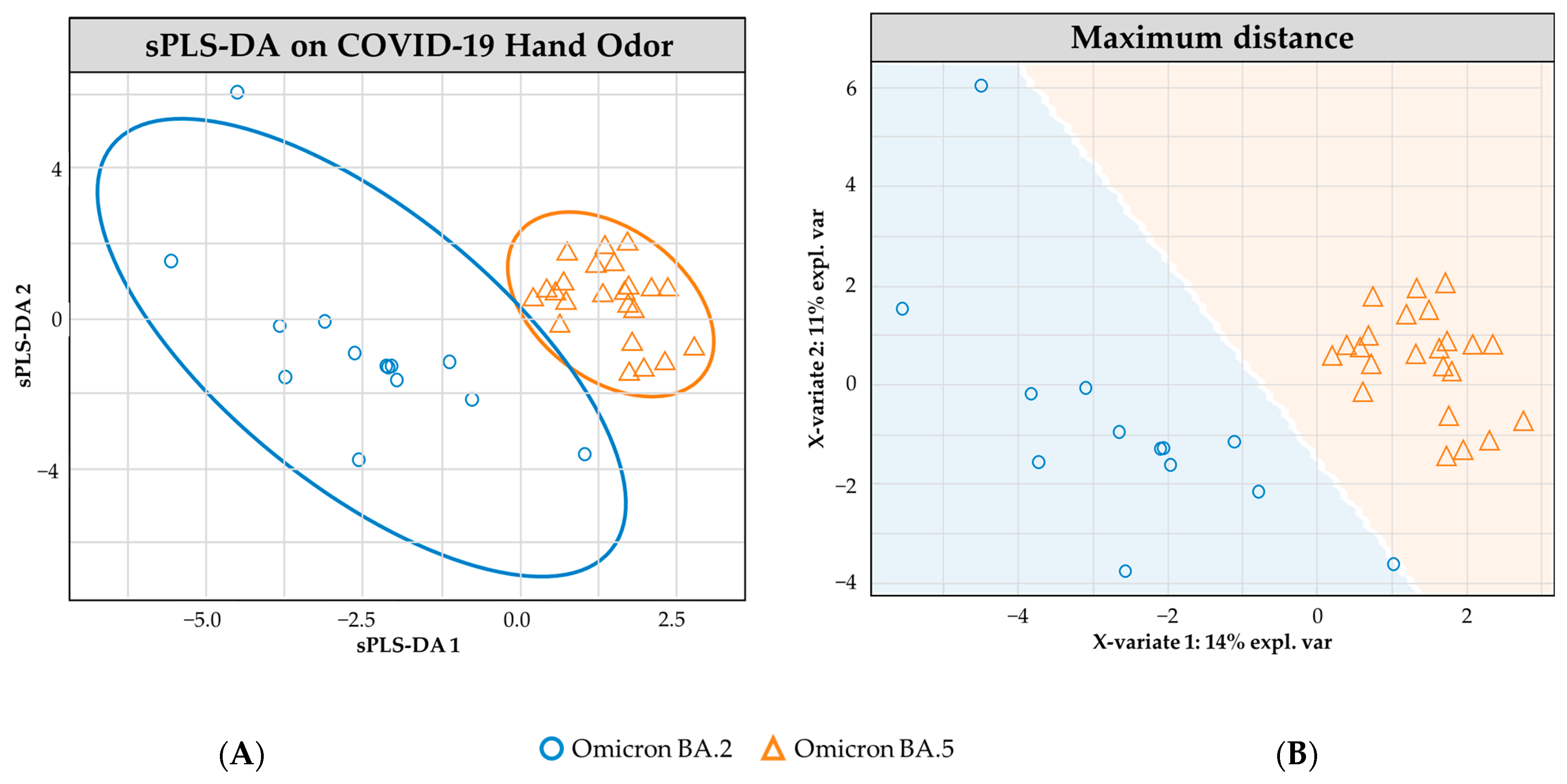
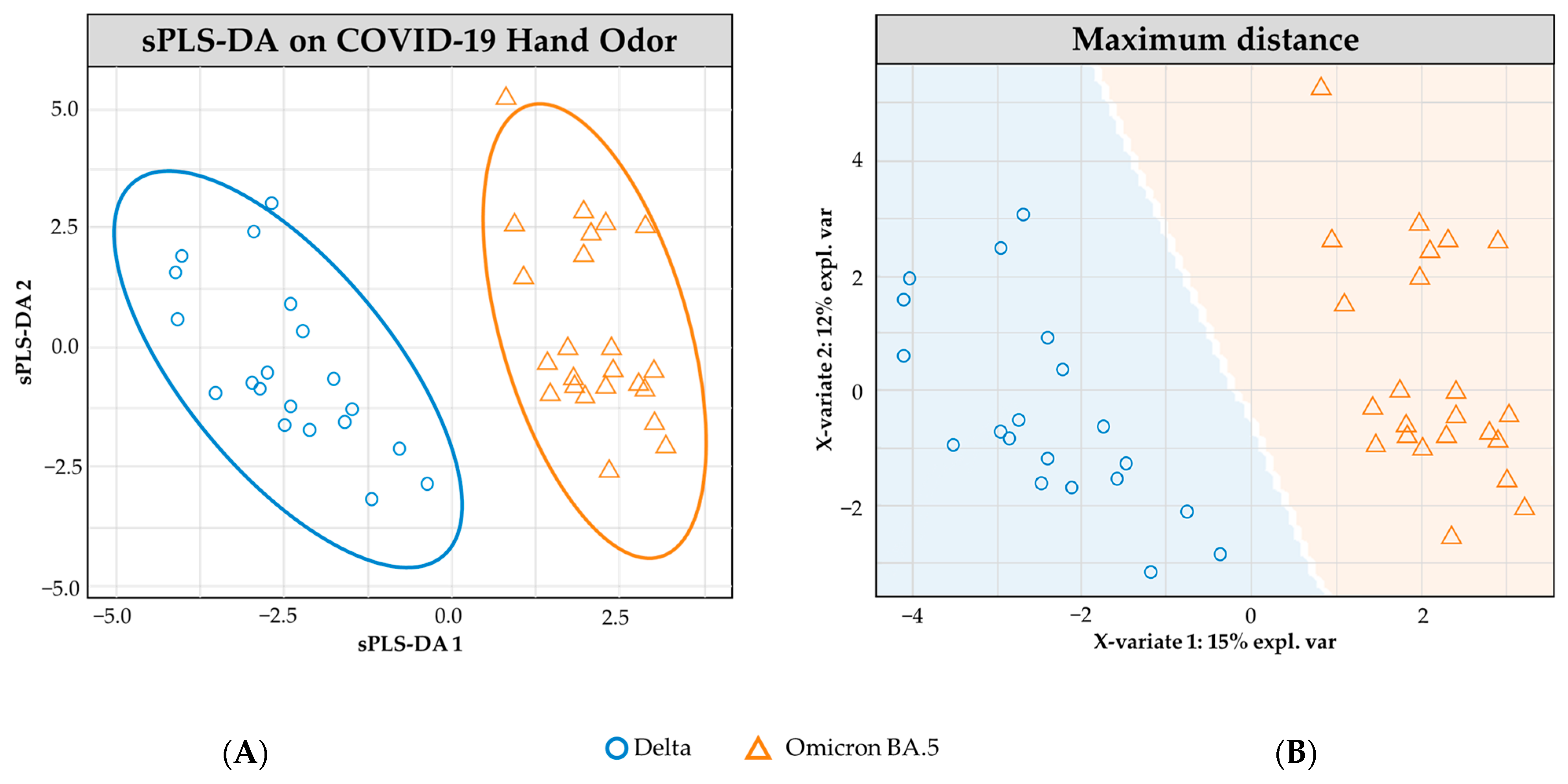
| Overall | 71.2% (±1.0) | 78.5% (±0.8) | 95.2% (±0.4) |
| Delta | 62.8% (±1.6) | - | 93.0% (±0.4) |
| Omicron BA.2 | 79.6% (±0.7) | 70.9% (±1.0) | - |
| Omicron BA.5 | - | 86.2% (±1.2) | 97.4% (±0.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gokool, V.A.; Crespo-Cajigas, J.; Ramírez Torres, A.; Forsythe, L.; Abella, B.S.; Holness, H.K.; Johnson, A.T.C.; Postrel, R.; Furton, K.G. Predicting SARS-CoV-2 Variant Using Non-Invasive Hand Odor Analysis: A Pilot Study. Analytica 2023, 4, 206-216. https://doi.org/10.3390/analytica4020016
Gokool VA, Crespo-Cajigas J, Ramírez Torres A, Forsythe L, Abella BS, Holness HK, Johnson ATC, Postrel R, Furton KG. Predicting SARS-CoV-2 Variant Using Non-Invasive Hand Odor Analysis: A Pilot Study. Analytica. 2023; 4(2):206-216. https://doi.org/10.3390/analytica4020016
Chicago/Turabian StyleGokool, Vidia A., Janet Crespo-Cajigas, Andrea Ramírez Torres, Liam Forsythe, Benjamin S. Abella, Howard K. Holness, Alan T. Charlie Johnson, Richard Postrel, and Kenneth G. Furton. 2023. "Predicting SARS-CoV-2 Variant Using Non-Invasive Hand Odor Analysis: A Pilot Study" Analytica 4, no. 2: 206-216. https://doi.org/10.3390/analytica4020016