1. Introduction
Female epispadias is a very rare entity with a reported incidence of 1:450,000 female live births [
1]. It has a varied spectrum of clinical presentations ranging from being incidentally detected to complete urinary incontinence. The milder variants are often missed and diagnosed during pelvic assessment for unrelated causes or during obstetric procedures [
2]. Of the clinically symptomatic cases presenting to healthcare facilities, urinary incontinence is the most common presentation [
2]. The classical examination findings of female epispadias include patulous urethral opening positioned ventrally within the vestibule, bifid clitoris, anteriorly-placed vaginal opening, poorly developed mons, and pubic diastasis [
2]. Perineal excoriation and ammoniacal dermatitis can also be seen in completely incontinent cases. A classification provided by Davis divides the cases of female epispadias into vestibular, subsymphyseal, and retrosymphyseal on the basis of increasing severity of incontinence [
3]. Around 30–75% of female epispadias are associated with vesicoureteric reflux [
4]. It can be due to low-capacity bladders, lateral ureteric ectopia, incompetent ureterovesical junction, etc.
As in any other disease phenotype belonging to the bladder exstrophy-epispadias complex (BEEC), the goals of surgical reconstruction of female epispadias include the creation of cosmetically acceptable genitalia, urinary continence, and the preservation of the upper tracts [
5]. The traditional staged repair of female epispadias includes urethroplasty followed by bladder neck reconstruction [
2]. Over the last two decades, single-stage repairs of female epispadias have gained significant popularity as these procedures not only yield satisfactory functional outcomes but also avoid the extensive surgical morbidity associated with the classical staged repair [
6,
7,
8]. However, the previous descriptions of single-stage bladder neck reconstructions have either not addressed or commented upon important issues such as urethral length [
7,
8], which is crucial while providing bladder outlet resistance, or have utilized futile exercises such as bladder neck suspension sutures, etc. [
7]. The aim of the present study is to share the early outcomes of our surgical technique in females with incontinent epispadias, i.e., the Single-stage Trans-vestibular And Foley’s assisted Epispadias Repair (STAFER) technique.
2. Materials and Methods
This retrospective single-center study included all girls, aged <14 years, with incontinent epispadias who had undergone epispadias repair with bladder neck plication utilizing our technique over a four-year study period (January 2016 to December 2019). All surgeries were performed by a single surgeon (M.B.). In view of the retrospective nature of the study, an ethical waiver was obtained by the Institutional review board.
The perineal anatomy was assessed on preoperative clinical examination and was documented in all cases. Similar to previous studies, the incontinence was categorized into four grades on the basis of severity [
8]: grade 0 (completely dry during day and night), grade 1 (occasional episodes of urine leakage leading to damp undergarments or requiring pads occasionally but not daily), grade 2 (frequent episodes of urine leakage with a dry period of <3 h), and grade 3 (completely incontinent). The postoperative incontinence status was also assessed subjectively and was compared with the preoperative status.
As a departmental policy, a battery of investigations was done in all cases preoperatively and at a 6-months follow-up visit. Renal bladder ultrasound (RBUS) and micturating cystourethrogram (MCUG) were performed to rule out any associated urogenital anomalies. The preoperative MCUG scan also confirmed the status of the bladder neck and the absence of vesicoureteric reflux (VUR). Postoperatively, both these investigations were performed to yield information on the status of upper tracts (dilatation and/or reflux), bladder capacity, and post-void residue. In addition, isotope renal scintigraphy studies (at baseline and 6-months follow-up) were also performed at our center. Technetium-99m diethylenetriamine pentaacetate (DTPA) and technetium-99m dimercaptosuccinic acid (DMSA) scans assessed the glomerular filtration rate (GFR) and the presence of renal scars respectively.
3. Operative Procedure
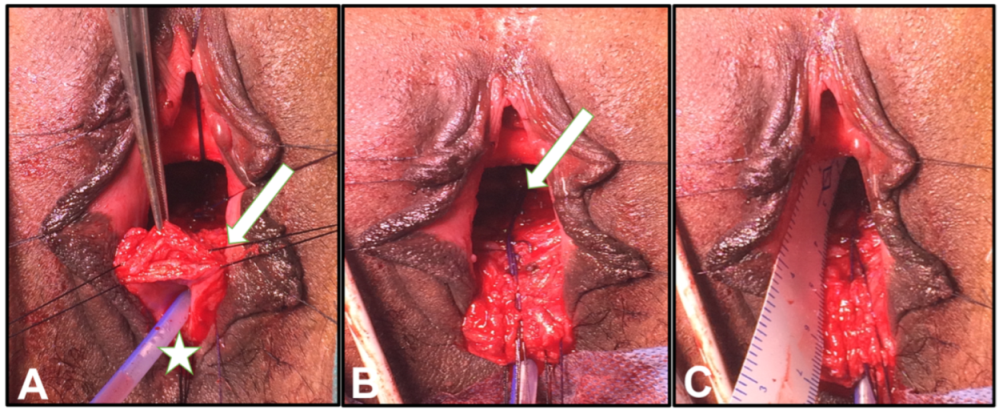
Under general anesthesia, the child was positioned in the lithotomy position. Perineal anatomy was assessed. After cleaning the operative field, two labial retraction stitches were placed. Foley’s catheter (10 or 12 French) was inserted per-urethrally and its bulb was inflated with 15 mL of sterile water. A periurethral incision was given. Two retraction sutures were placed in the periurethral soft tissue to minimize handling of the urethral meatus (
Figure 1A). Subsequently, the dissection was continued circumferentially around the urethral meatus and the incision was deepened using electrocautery. Using a constant pull over the urethral catheter (provided by heavy artery forceps), the dissection of the urethra was continued proximally preserving the periurethral plexus (
Figure 1A). A cautious dissection was also done on the inferior aspect of the urethra to avoid any injury to the vagina. Soft tissue mobilization in the subpubic space was continued beyond the bladder neck till the pelvic floor was visualized, and the suspensory ligaments were divided. When a wider area of dissection with exposed bladder neck was visualized, the bladder neck plication was started over the urethral catheter using interrupted 6-0 Polydioxanone (PDS) sutures. The first stitch was taken proximal to the bulb of the urethral catheter (
Figure 1B). Subsequently, the bulb of the catheter was deflated and it was advanced in the urinary bladder. The catheter was then secured at the urethral meatus with the meatal retraction sutures before the subsequent plication and urethral tubularization was performed. After bladder neck plication was completed, simple interrupted PDS sutures were placed proximal to the distal for urethral tubularization. The length of the tubularized urethra was measured carefully. The neourethral meatus was created dorsal to the previously positioned urethral meatus using 5-0 monofilament sutures. Finally, the genitoplasty (vestibuloplasty and clitoroplasty) was performed using 5-0 monofilament sutures. In the postoperative period, an intermittent clamping-declamping of the catheter was started from postoperative day 4. The urethral catheter was kept in situ for 7–10 days and the child was discharged from the hospital. After the removal of the catheter, the child and the parents were counseled and trained for timed-voiding with the maintenance of a bladder diary.
Following discharge, the oral antibiotic cover was given for one week. At the first follow-up visit (at 2 weeks), the perineal wound was examined and the bladder diary was assessed. Timed voiding and Kegel’s exercises (if the child was more than 5 years of age) were reinforced. Further follow-up visits were scheduled monthly for 6 months and then yearly. Continence status was evaluated at each visit while the radiological and nuclear scans were performed 6-months post-surgery.
The data were expressed as numbers and averages (mean with standard deviation). The continuous variables were compared using Student’s t-test. A p-value of <0.05 was considered statistically significant.
4. Results
Nine girls with incontinent epispadias and having continuous dribbling of urine were included in the present study. A patulous bladder neck, bifid clitoris, and pubic diastasis were noted on preoperative clinical examination in these cases. The average (SD) age at surgery of the cohort was 7.9 (3.8) years (
Table 1). Baseline RBUS was unremarkable and MCUG ruled out preoperative VUR in all patients. The preoperative average (SD) GFR of the cohort was 103 (10) mL/min/1.73 m
2 and DMSA scans ruled out any renal scarring in them.
Intraoperatively, the average length of the tubularized urethra (
Figure 1C) was 4.9 cm (range 4–5.9). The average operative duration was 50 min. The postoperative course was uneventful and was devoid of any major complications. None of the patients developed urinary tract infections. Three patients had superficial surgical site infections and were managed conservatively with perineal hygiene and local antibiotic washes (
Table 1). In addition, the urethral catheter was kept for one additional week in these cases. The average (SD) hospital stay and follow-up duration of the cohort were 10.5 (2.2) days and 45.1 (8.8) months, respectively.
Preoperatively, all cases had grade 3 incontinence status. Upon follow-up (
Table 2), eight patients were voiding in a good stream without any lower urinary tract symptoms, while one was persistently incontinent (grade 3). Of those achieving continence, six remained completely dry (grade 0) since their first follow-up visits. The remaining two girls initially had grade 2 incontinences which improved to grade 1 after six months of follow-up. None of the patients required redo bladder neck plication or bladder neck repair. Postoperative RBUS showed significant post-void residue in one girl having grade II VUR on an MCUG scan. She was managed conservatively and showed no functional deterioration on subsequent follow-up. RBUS and MCUG scans were unremarkable in the remaining patients. The postoperative average (SD) GFR of the cohort was 101 (8) mL/min/1.73 m
2 and did not differ from the average preoperative GFR (
p > 0.05 using
t-test). In addition, the DMSA scans were also normal in all of them.
5. Discussion
The successful treatment of incontinence in cases of female epispadias has been available in the literature since the time of Young [
9]. Over the years, many surgical techniques have been described. A classic staged repair involves urethral and genital reconstruction at 18 months of age followed by bladder neck repair at 4–5 years of age [
4]. Gearhart et al. have reported overall continence rates of 87.5% utilizing this approach [
4]. However, repeated procedures add significant morbidity to the overall growth and development of children. In contrast, a complete reconstruction approach was described by Hendren et al. in 1981 [
10]. The approach involved perineal narrowing of the urethra, bladder neck reconstruction, and ureteral reimplantation (if necessary) in the same setting. Being a single-stage reconstruction, this approach was useful for children presenting later in childhood because of the presence of adequate bladder capacity in them. However, this procedure permeated the concept of single-stage repair of female epispadias. Since then, many surgeons have highlighted the importance of one-stage repair [
6,
7,
8].
The operative technique described in the present study yielded favorable functional outcomes in our cohort. At the end of six months of follow-up, eight out of nine girls had a dry period of more than 3 h. Six of them were completely dry and had no wetting episodes at all. The incontinence of the remaining patient was due to coexisting neurogenic bladder due to spina bifida, which was missed during the initial workup.
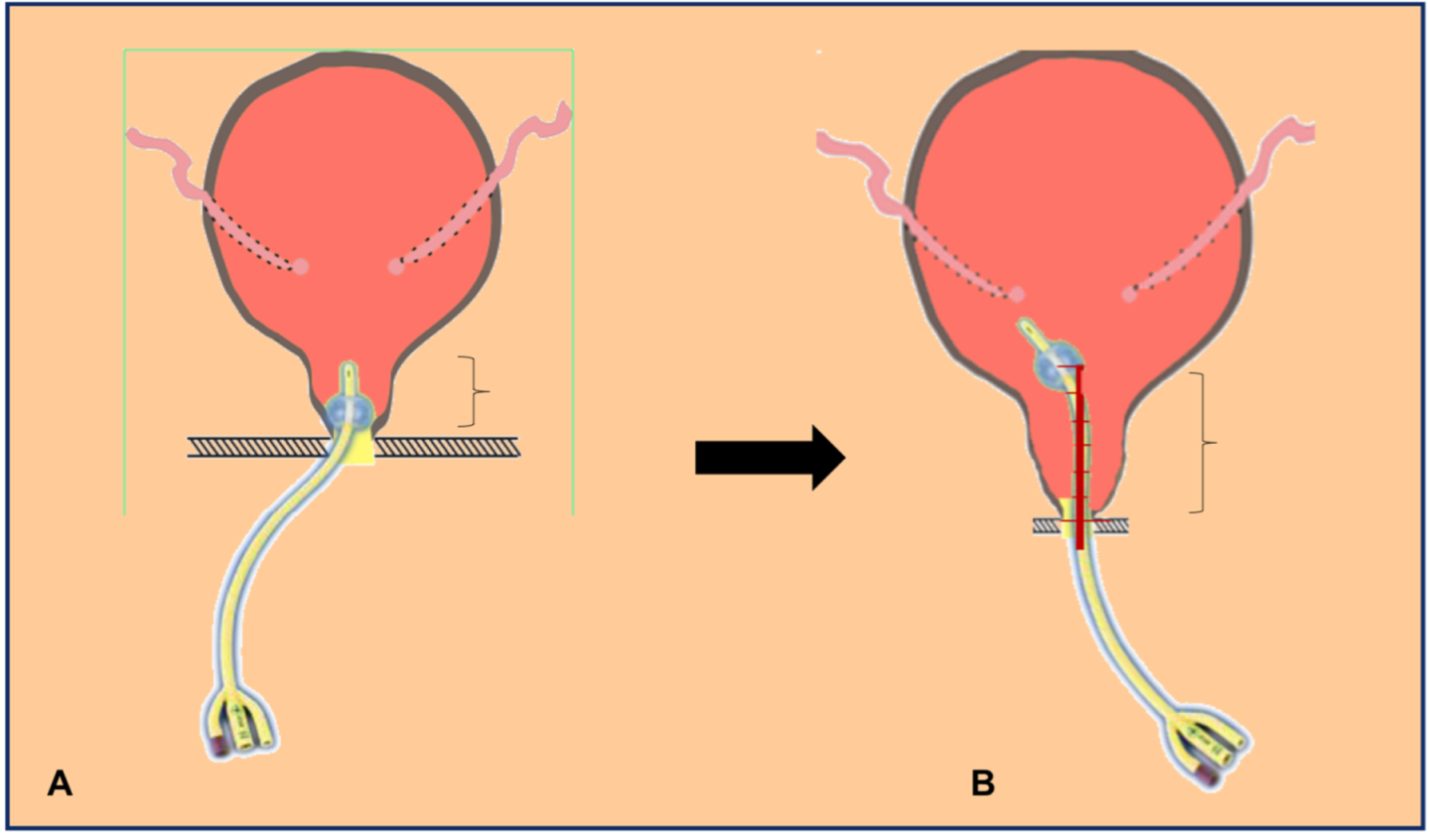
Nevertheless, the encouraging results with the STAFER technique can be attributed to several factors. First, the trans-vestibular route provides direct access to the bladder neck in girls with pubic diastasis (widely placed pubic bones) and short urethra. As a result, the bladder neck plication can be performed efficaciously under direct vision. Second, the constant pull by the inflated bulb of the Foley’s catheter provides continuous traction, thus, aiding in the dissection and the mobilization of the urethra. In addition, Foley’s catheter also provides a firm scaffold for uniform tubularization of the urethra. Third, it is believed that a few millimeters of extra length can be purchased by interrupted suturing with constant traction provided by the urethral catheter. This observation of urethral lengthening was evident in our cohort with an average intraoperative urethral length of almost 5 cm (
Figure 2). As per Poiseuille’s equation of fluid dynamics, the resistance to the flow is directly proportional to the length. Upon applying this equation in the present setting, the STAFER technique helps in increasing the resistance to the flow of urine and aids in urinary continence. Fourth, the urethra was never opened during the plication procedure. This minimizes the risk of stricture formation. Finally, the abovementioned technique avoids any laparotomy scar and the virginity of the peritoneum is also maintained.
Kajbafzadeh et al. have described their technique of single-stage cystoscopic guided bladder neck plication and urethrogenitoplasty in ten patients [
8]. Satisfactory results were demonstrated by the authors. Complete dryness was achieved in six patients while four had a dry period of >3 h with occasional urine leak. In addition, a similar technique to ours has been published by Yadav et al. in six cases of female epispadias [
7]. The authors also utilized Foley’s catheter and performed a single-stage epispadias repair with bladder neck plication via the perineal route. Although the authors also demonstrated satisfactory outcomes in all six cases, two key points from our experience required special mention. Firstly, bladder neck suspension to the pubic bone is not required. It is believed that this step, which plays a crucial role in the management of stress urinary incontinence, adds little in achieving dryness in girls with incontinent epispadias. Secondly, the concept of urethral lengthening and increase in bladder outlet resistance is more relevant in this aspect and is not highlighted in the study by Yadav et al. [
7].
The results of the present study must be interpreted within the context of a few limitations. First, this is a retrospective study with a very limited sample size. Second, the follow-up of the cohort ranges from 32–60 months. A longer follow-up is needed to study the long-term outcomes of the STAFER technique. Third, the average age of our study population was 7.8 years with the youngest girl being operated on at 3 years of age. Therefore, the outcomes of this technique are not well-known in children < 3 years of age. Finally, the rarity of the disease prevents us from drawing definite conclusions in regards to the efficacy of the STAFER technique and prospective studies need to be conducted in the future.
6. Conclusions
In a limited cohort of girls with incontinent epispadias, the STAFER technique provides favorable functional outcomes in terms of continence and upper tract function. Further studies comprising of a larger cohort of patients with a younger average age at surgery need to be conducted before definite conclusions regarding the efficacy of this technique are drawn.
Author Contributions
Conceptualization, M.B.; Formal analysis, S.A. and P.G.; Writing—original draft preparation, S.A. and M.B.; Writing—review and editing, M.B. and P.G. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available upon request of the respective author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- DEES, J.E. Congenital epispadias with incontinence. J. Urol. 1949, 62, 513–522. [Google Scholar] [CrossRef]
- Anand, S.; Lotfollahzadeh, S. Epispadias. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK563180/ (accessed on 20 March 2022).
- Davis, D. Epispadias in females and its surgical treatment. Surg. Gynecol. Obstet. 1928, 47, 680–696. [Google Scholar] [CrossRef]
- Gearhart, J.P.; Peppas, D.S.; Jeffs, R.D. Complete genitourinary reconstruction in female epispadias. J. Urol. 1993, 149, 1110–1113. [Google Scholar] [CrossRef]
- Anand, S.; Lotfollahzadeh, S. Bladder Exstrophy. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK563156/ (accessed on 20 March 2022).
- De Jong, T.P.; Dik, P.; Klijn, A.J. Female epispadias repair: A new 1-stage technique. J. Urol. 2000, 164, 492–494. [Google Scholar] [CrossRef]
- Yadav, S.S.; Agarwal, N.; Kumar, S.; Tomar, V.; Vyas, N.; Teli, R.; Badgurjar, M.K.; Bamaniya, M.K. Single-stage Female Epispadias Repair by Combined Infrasymphyseal Bladder Neck Plication and Urethrogenitoplasty: A Novel Technique. Urology 2017, 100, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Kajbafzadeh, A.M.; Talab, S.S.; Elmi, A.; Tourchi, A. Single-stage subsymphyseal cystoscopic-guided bladder neck plication and urethrogenitoplasty in female epispadias: Presentation of long-term follow-up. BJU Int. 2011, 108, 1200–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, H.H. An operation for the cure of incontinence associated with epispadias. J. Urol. 1922, 7, 1–32. [Google Scholar] [CrossRef]
- Hendren, W.H. Congenital female epispadias with incontinence. J. Urol. 1981, 125, 558–564. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).







{kind=link}
{kind=link}