
The Computed Sinusoid

Abstract
:1. Introduction
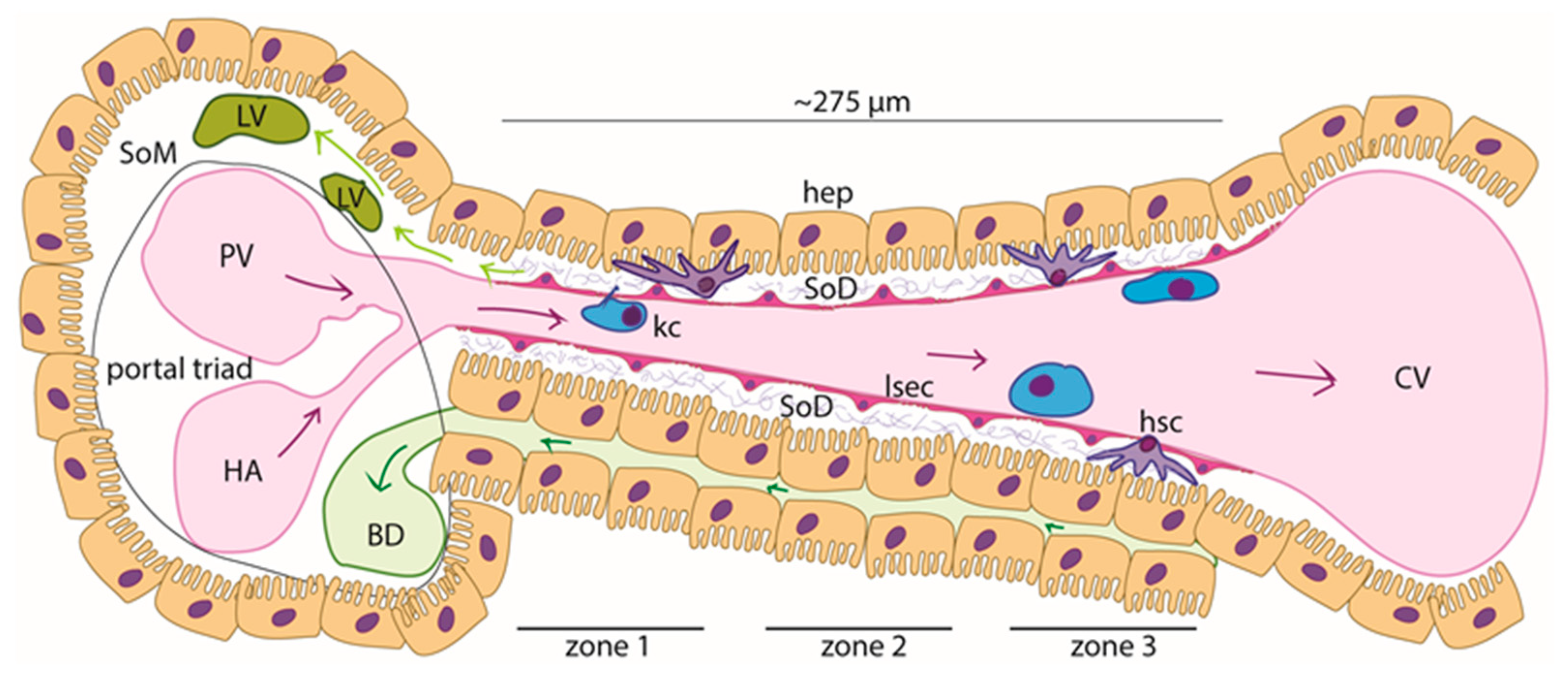
1.1. The Hepatic Sinusoid
1.2. Models of the Hepatic Sinusoids
2. Materials and Methods
2.1. Computational Fluid Dynamics (CFD) Simulations
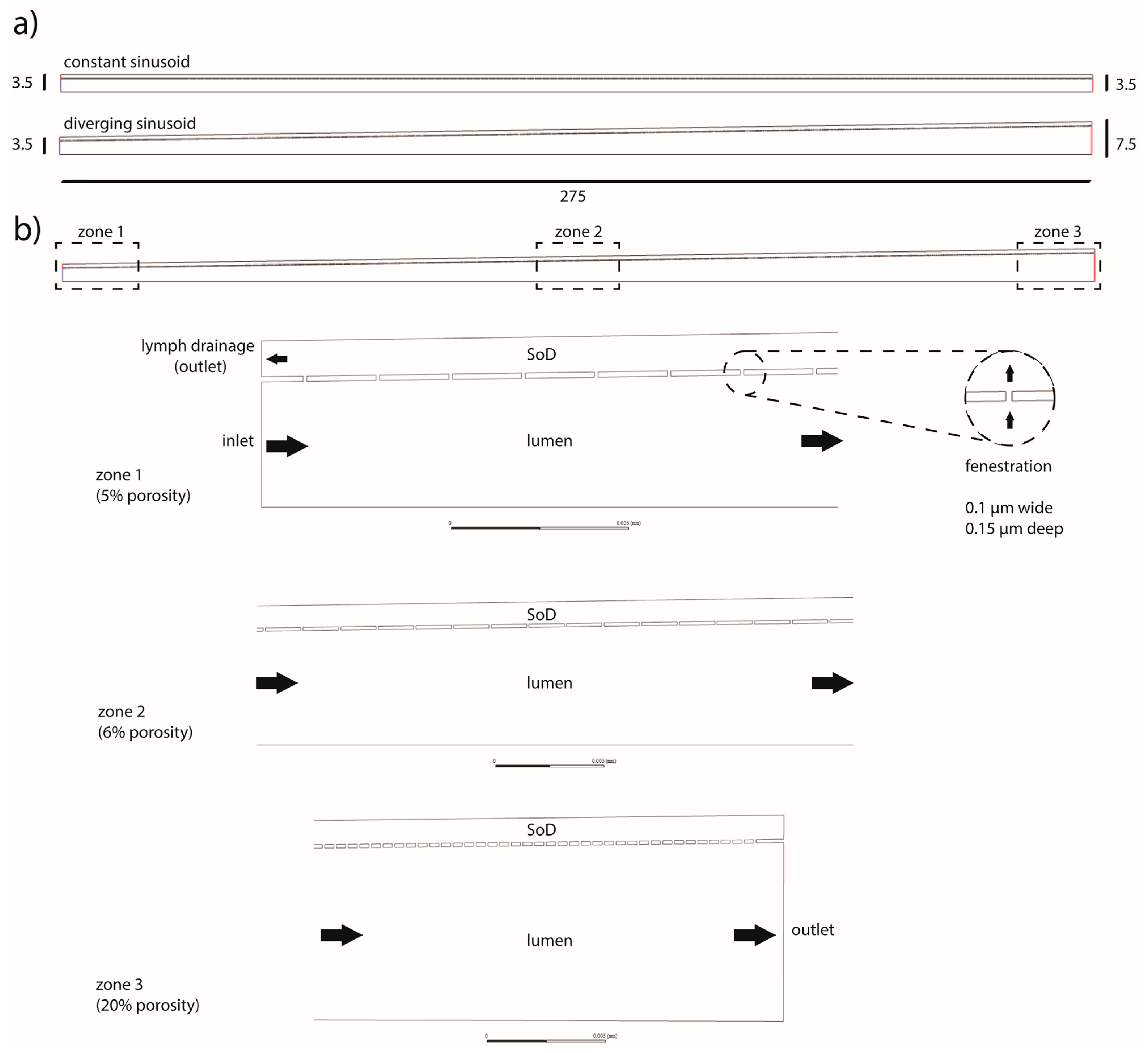
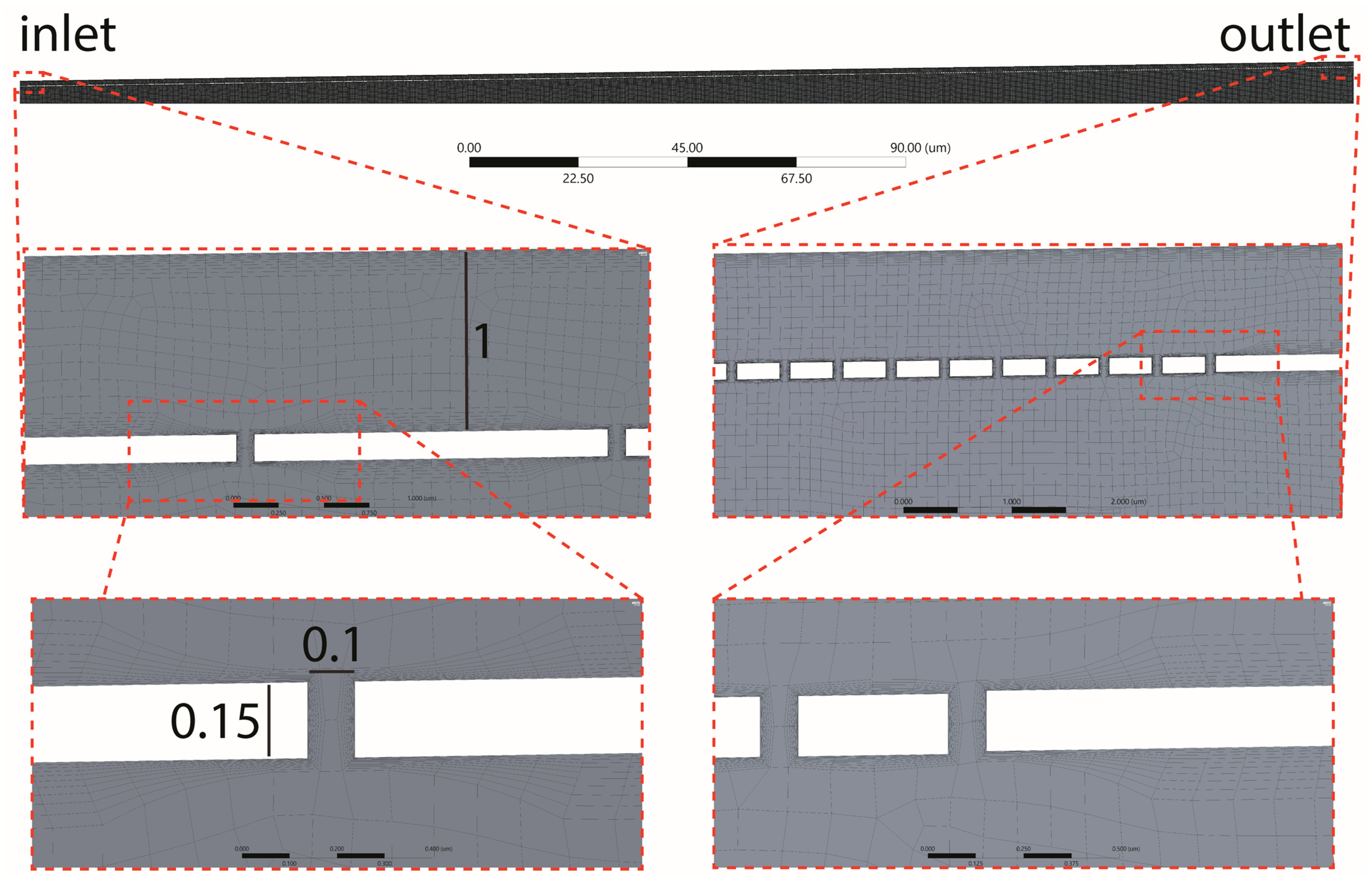
2.2. Geometry and Mesh
- The sinusoid was designed as a half-section measuring 275 µm long. Two half-sections were evaluated, one with a constant radius (3.5 µm) and one with a linearly increasing radius (the inlet/outlet radii were, respectively, set to 3.5 µm and 7.5 µm).
- The SoD was modeled as a 1 µm thick 2D chamber surrounding the sinusoid lumen and communicating with it via fenestrations.
- The fenestrations were modeled as 100 nm long and 150 nm high channels connecting the sinusoidal lumen with the SoD (Figure 3).
- The main walls (of the sinusoidal lumen and the Space of Disse lumen) were formed as two coaxial rectangles (or trapezoids when the sinusoid had a diverging section).
- Fenestrations were modeled as a linear pattern.
- The sketch was converted into a surface, and a symmetry axis was introduced (halving the model).
2.3. Solver Configuration
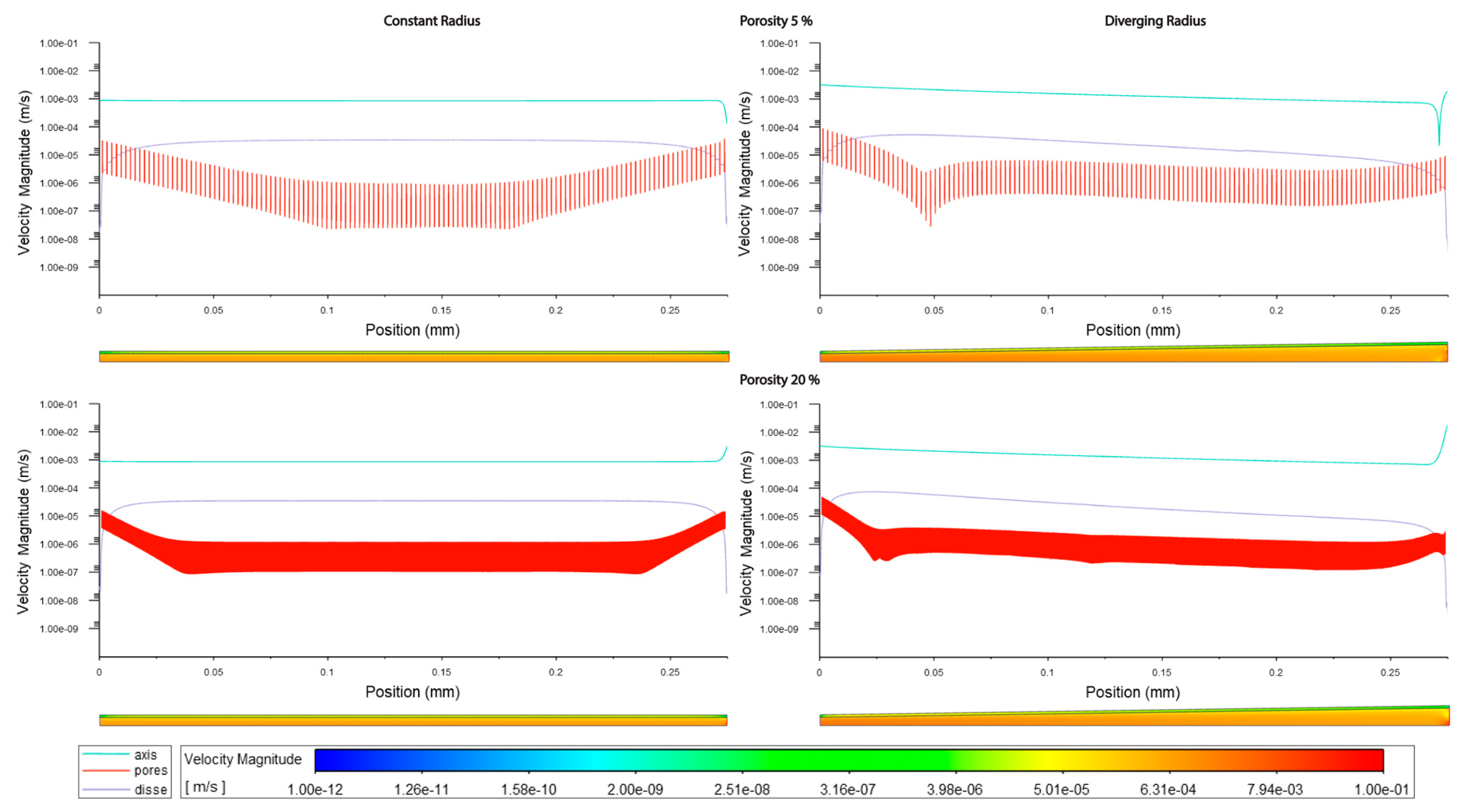
3. Results
4. Discussion
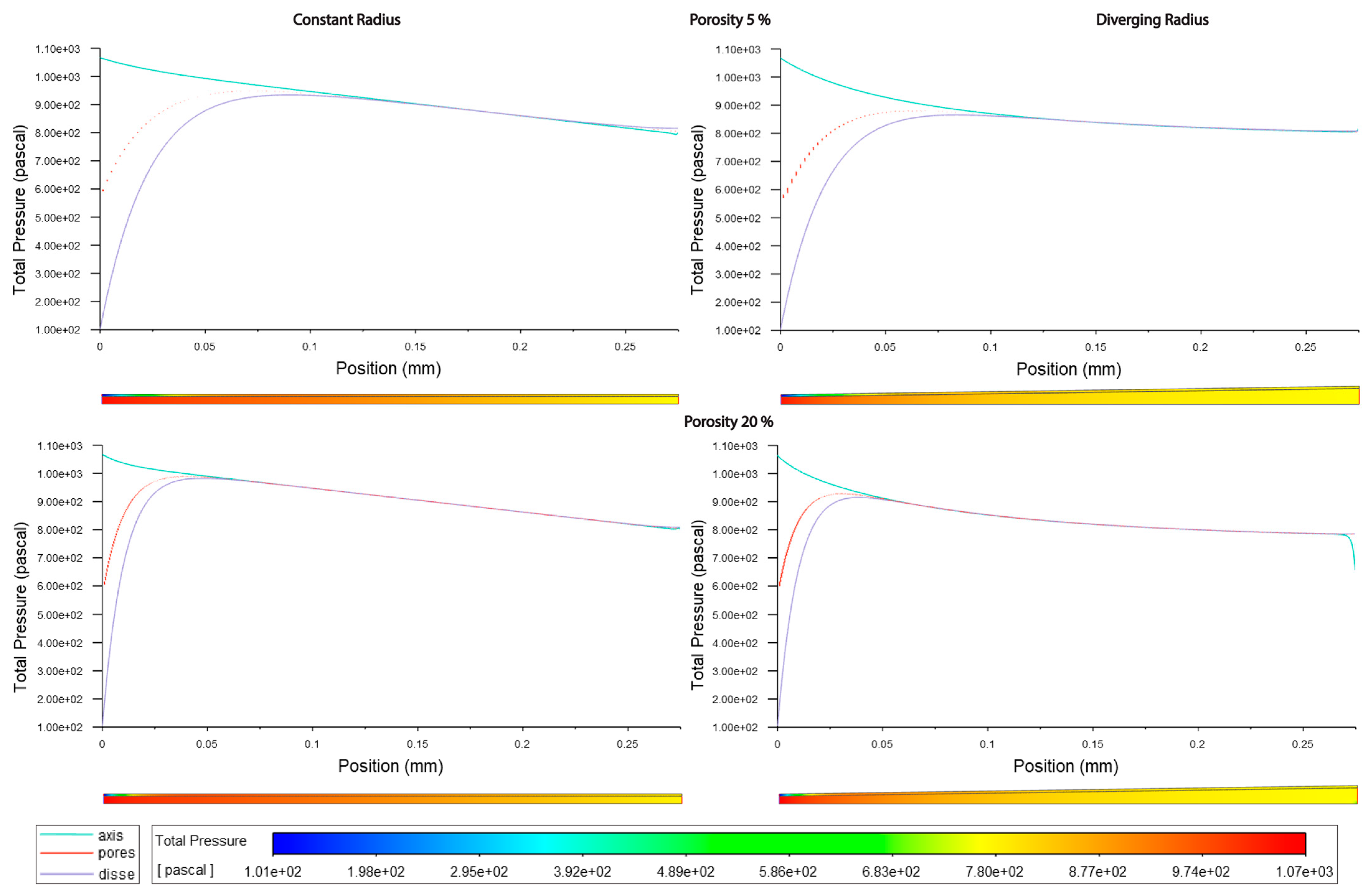
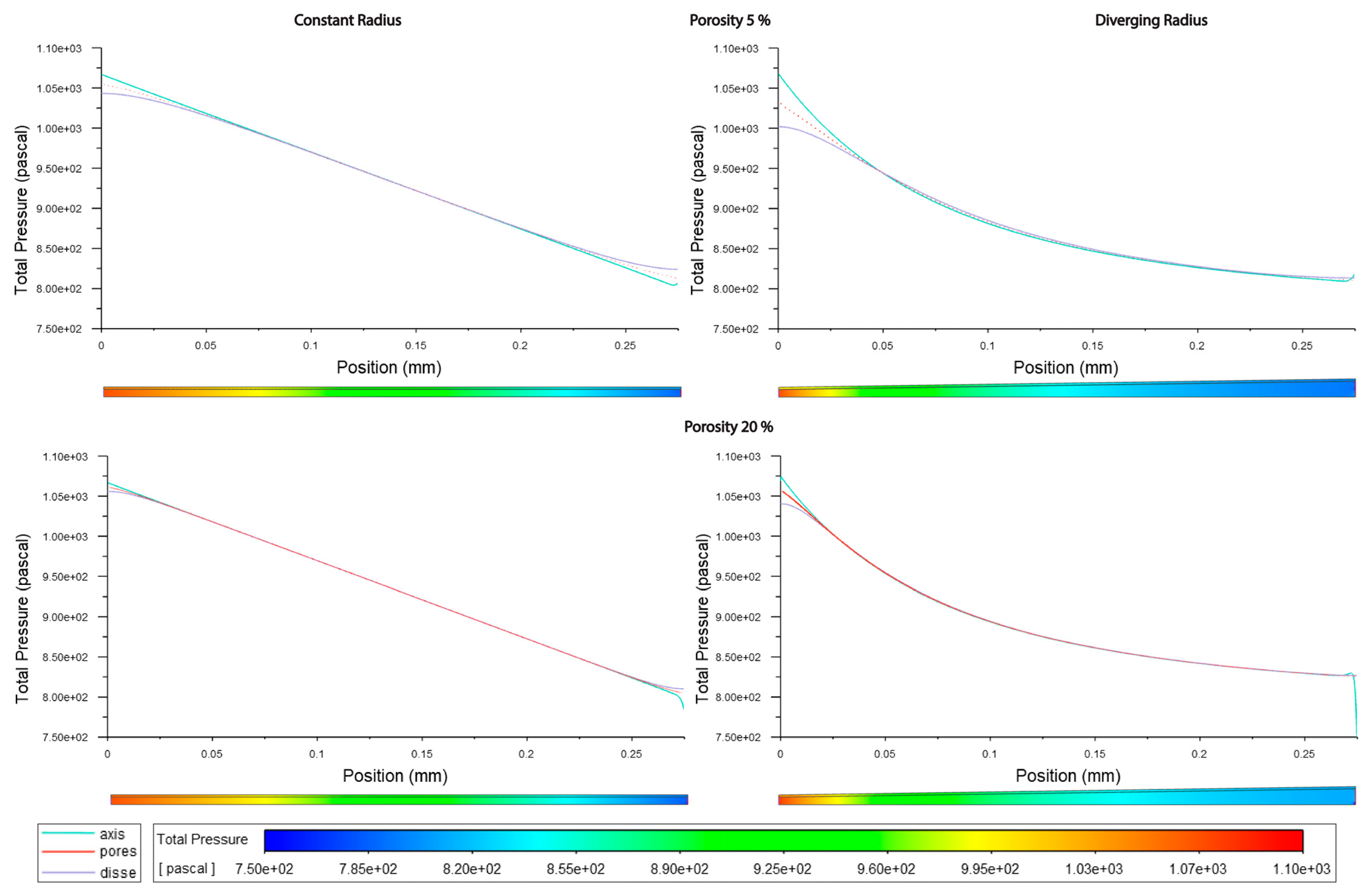
4.1. Major Insights about Sinusoidal Pressure (P)
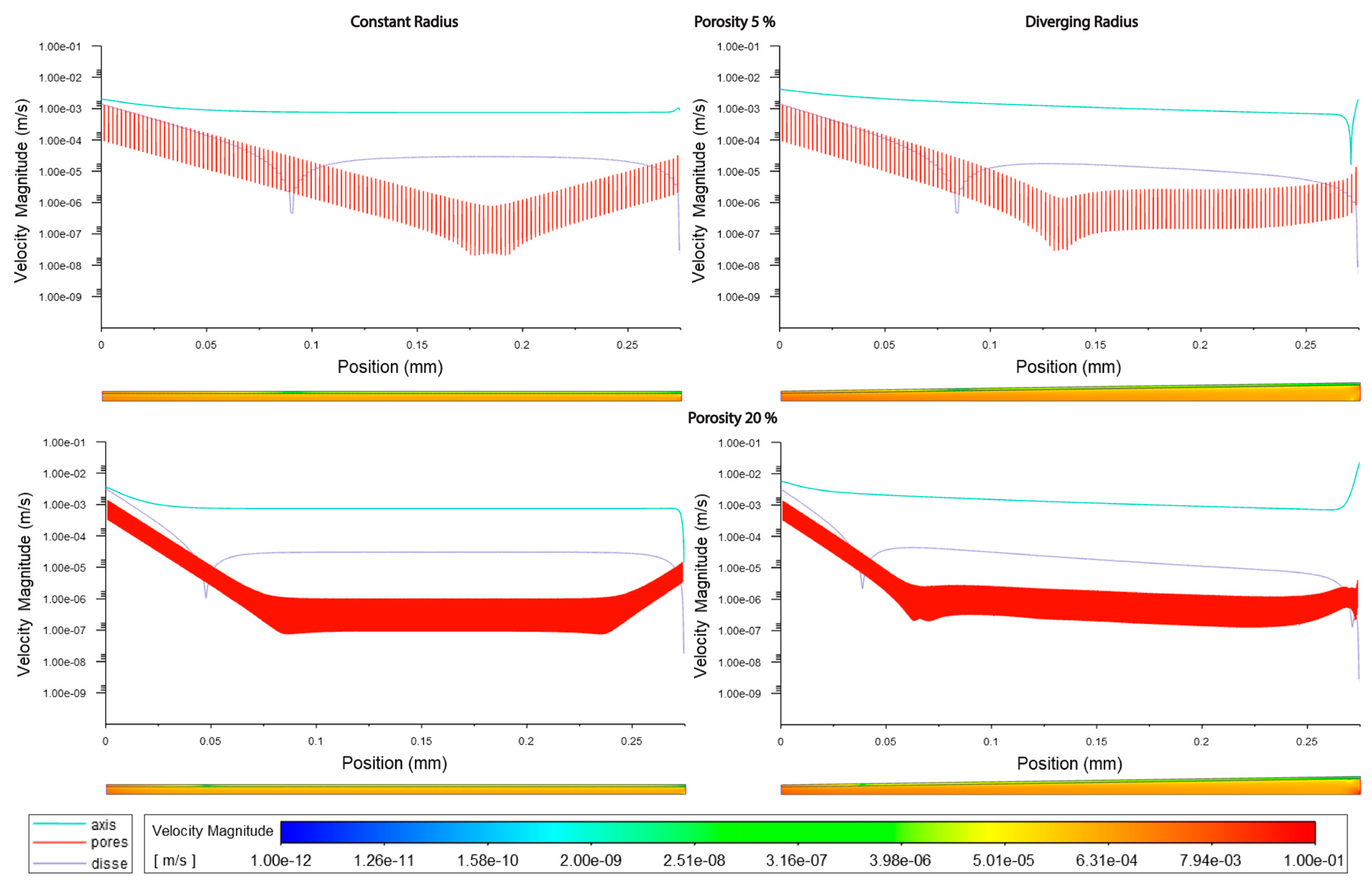
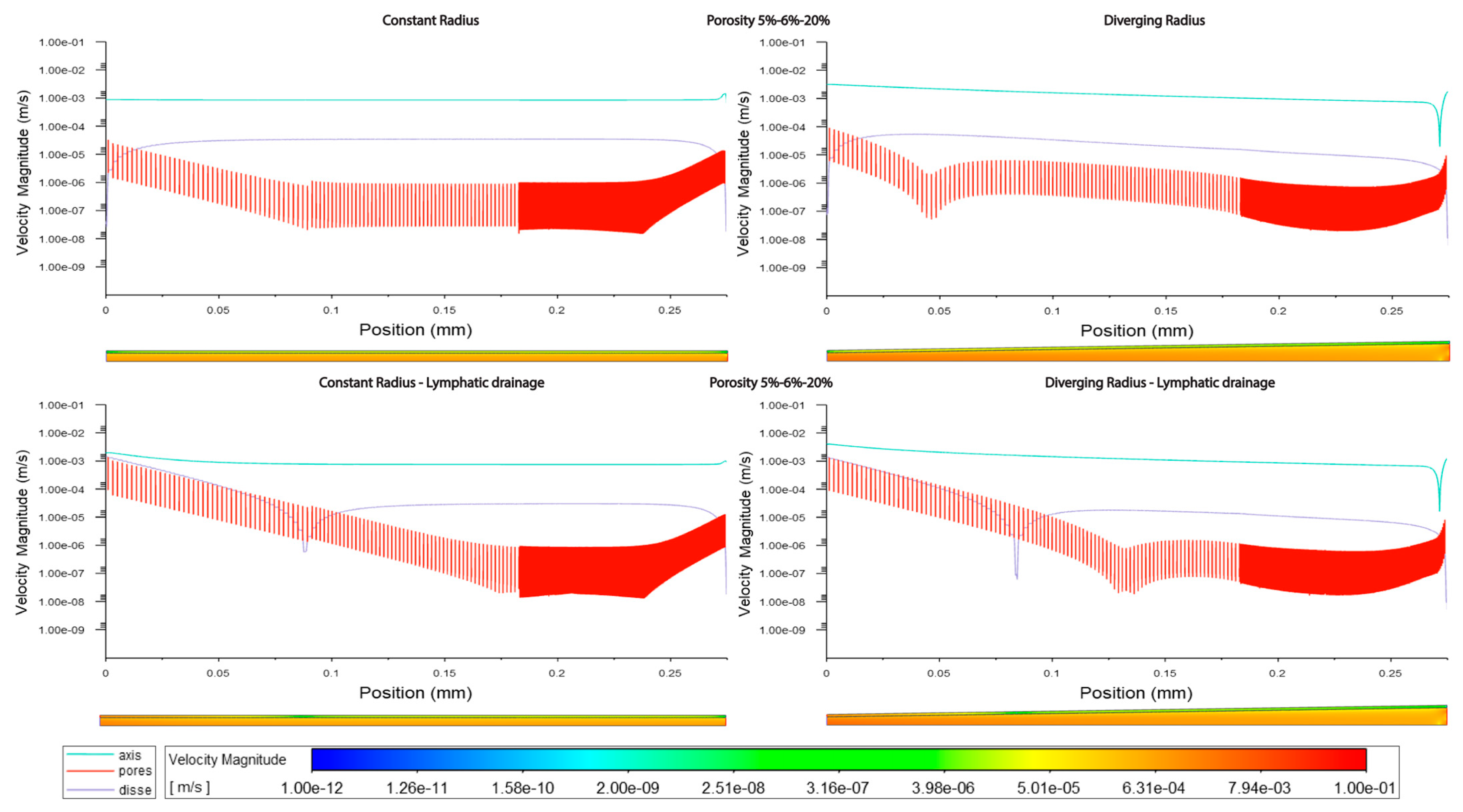
4.2. Major Insights Regarding Flow Velocity (V)
4.3. General Considerations and Limitations
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ehrlich, A.; Duche, D.; Ouedraogo, G.; Nahmias, Y. Challenges and Opportunities in the Design of Liver-on-Chip Microdevices. Annu. Rev. Biomed. Eng. 2019, 21, 219–239. [Google Scholar] [CrossRef]
- Cogger, V.C.; Hunt, N.J.; Le Couteur, D.G. Fenestrations in the Liver Sinusoidal Endothelial Cell. In The Liver; Wiley: Hoboken, NJ, USA, 2020; pp. 435–443. [Google Scholar] [CrossRef]
- Wake, K.; Motomatsu, K.; Dan, C.; Kaneda, K. Three-Dimensional Structure of Endothelial Cells in Hepatic Sinusoids of the Rat as Revealed by the Golgi Method. Cell Tissue Res. 1988, 253, 563–571. [Google Scholar] [CrossRef] [PubMed]
- MacPhee, P.J.; Schmidt, E.E.; Groom, A.C. Intermittence of Blood Flow in Liver Sinusoids, Studied by High-Resolution in Vivo Microscopy. Am. J. Physiol.—Gastrointest. Liver Physiol. 1995, 269, G692–G698. [Google Scholar] [CrossRef]
- Komatsu, H.; Koo, A.; Guth, P.H. Leukocyte Flow Dynamics in the Rat Liver Microcirculation. Microvasc. Res. 1990, 40, 1–13. [Google Scholar] [CrossRef]
- Eguchi, H.; Sato, N.; Matsumura, T.; Minamiyama, M.; Kawano, S.; Kamada, T. The Microcirculatory Properties around the Hepatic Periportal and Pericentral Regions of Rats. In Proceedings of the Fourth World Congress for Microcirculation, Beijing, China, 20–22 July 1987. [Google Scholar]
- Horn, T.; Henriksen, J.H.; Christoffersen, P. The Sinusoidal Lining Cells in “Normal” Human Liver. A Scanning Electron Microscopic Investigation. Liver 1986, 6, 98–110. [Google Scholar] [CrossRef]
- Vidal-Vanaclocha, F.; Barberá-Guillem, E. Fenestration Patterns in Endothelial Cells of Rat Liver Sinusoids. J. Ultrastruct. Res. Mol. Struct. Res. 1985, 90, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Wack, K.E.; Ross, M.A.; Zegarra, V.; Sysko, L.R.; Watkins, S.C.; Stolz, D.B. Sinusoidal Ultrastructure Evaluated during the Revascularization of Regenerating Rat Liver. Hepatology 2001, 33, 363–378. [Google Scholar] [CrossRef]
- Wisse, E.; De Zanger, R.B.; Jacobs, R.; McCuskey, R.S. Scanning Electron Microscope Observations on the Structure of Portal Veins, Sinusoids and Central Veins in Rat Liver. Scan. Electron Microsc. 1983, Pt 3, 1441–1452. [Google Scholar]
- Henriksen, J.H.; Lassen, N.A. Pressure Profile in Liver Sinusoids A Model of Localization of Sinusoidal Resistance in the Normal and Cirrhotic Liver. Liver 1988, 8, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.J.; Chang, S.; Kim, O.Y.; Kang, B.K.; Park, J.; Lim, J.H.; Yun Huang, J.; Kim, Y.K.; Byun, J.H.; Gho, Y.S. Three-Dimensional Imaging of Hepatic Sinusoids in Mice Using Synchrotron Radiation Micro-Computed Tomography. PLoS ONE 2013, 8, e68600. [Google Scholar] [CrossRef]
- Ryou, M.; Stylopoulos, N.; Baffy, G. Nonalcoholic Fatty Liver Disease and Portal Hypertension. Explor. Med. 2020, 1, 149–169. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Iwakiri, Y. Lymphatics in the Liver. Curr. Opin. Immunol. 2018, 53, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Iwakiri, Y. The Hepatic Lymphatic Vascular System: Structure, Function, Markers, and Lymphangiogenesis. Cell. Mol. Gastroenterol. Hepatol. 2016, 2, 733–749. [Google Scholar] [CrossRef]
- Jeong, J.; Tanaka, M.; Iwakiri, Y. Hepatic Lymphatic Vascular System in Health and Disease. J. Hepatol. 2022, 77, 206–218. [Google Scholar] [CrossRef] [PubMed]
- Santambrogio, L. The Lymphatic Fluid. Int. Rev. Cell Mol. Biol. 2018, 337, 111–133. [Google Scholar] [CrossRef]
- Hsu, M.C.; Itkin, M. Lymphatic Anatomy. Tech. Vasc. Interv. Radiol. 2016, 19, 247–254. [Google Scholar] [CrossRef]
- Bonfiglio, A.; Leungchavaphongse, K.; Repetto, R.; Siggers, J.H. Mathematical Modeling of the Circulation in the Liver Lobule. J. Biomech. Eng. 2010, 132, 111011. [Google Scholar] [CrossRef]
- Siggers, J.H.; Leungchavaphongse, K.; Ho, C.H.; Repetto, R. Mathematical Model of Blood and Interstitial Flow and Lymph Production in the Liver. Biomech. Model. Mechanobiol. 2014, 13, 363–378. [Google Scholar] [CrossRef]
- Debbaut, C.; Vierendeels, J.; Casteleyn, C.; Cornillie, P.; Van Loo, D.; Simoens, P.; Van Hoorebeke, L.; Monbaliu, D.; Segers, P. Perfusion Characteristics of the Human Hepatic Microcirculation Based on Three-Dimensional Reconstructions and Computational Fluid Dynamic Analysis. J. Biomech. Eng. 2012, 134, 011003. [Google Scholar] [CrossRef]
- Piergiovanni, M.; Bianchi, E.; Capitani, G.; Li Piani, I.; Ganzer, L.; Guidotti, L.G.; Iannacone, M.; Dubini, G. Microcirculation in the Murine Liver: A Computational Fluid Dynamic Model Based on 3D Reconstruction from In Vivo Microscopy. J. Biomech. 2017, 63, 125–134. [Google Scholar] [CrossRef]
- Hu, J.; Lü, S.; Feng, S.; Long, M. Flow Dynamics Analyses of Pathophysiological Liver Lobules Using Porous Media Theory. Acta Mech. Sin. Xuebao 2017, 33, 823–832. [Google Scholar] [CrossRef]
- Rani, H.P.; Sheu, T.W.H.; Chang, T.M.; Liang, P.C. Numerical Investigation of Non-Newtonian Microcirculatory Blood Flow in Hepatic Lobule. J. Biomech. 2006, 39, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Rohan, E.; Turjanicová, J.; Lukeš, V. Multiscale Modelling of Liver Perfusion. In Proceedings of the 15 International Conference on Computational Plasticity: Fundamentals and Applications, COMPLAS 2019, Barcelona, Spain, 3–5 September 2019; pp. 343–353. [Google Scholar]
- Debbaut, C.; Monbaliu, D.; Casteleyn, C.; Cornillie, P.; Van Loo, D.; Van Hoorebeke, L.; Simoens, P.; Pirenne, J.; Segers, P. Multiscale Modeling of the Blood Circulation in the Human Liver Using Vascular Corrosion Casting and Micro-CT Imaging Techniques. In Proceedings of the ASME 2011 Summer Bioengineering Conference, Parts A and B, Farmington, PA, USA, 22–25 June 2011; American Society of Mechanical Engineers: New York, NY, USA, 2011; pp. 451–452. [Google Scholar] [CrossRef]
- Ricken, T.; Dahmen, U.; Dirsch, O. A Biphasic Model for Sinusoidal Liver Perfusion Remodeling after Outflow Obstruction. Biomech. Model. Mechanobiol. 2010, 9, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi-Badejani, R.; Mosharaf-Dehkordi, M.; Ahmadikia, H. An Image-Based Geometric Model for Numerical Simulation of Blood Perfusion within the Liver Lobules. Comput. Methods Biomech. Biomed. Eng. 2020, 23, 987–1004. [Google Scholar] [CrossRef]
- Mosharaf-Dehkordi, M. A Fully Coupled Porous Media and Channels Flow Approach for Simulation of Blood and Bile Flow through the Liver Lobules. Comput. Methods Biomech. Biomed. Eng. 2019, 22, 901–915. [Google Scholar] [CrossRef]
- Schwen, L.O.; Krauss, M.; Niederalt, C.; Gremse, F.; Kiessling, F.; Schenk, A.; Preusser, T.; Kuepfer, L. Spatio-Temporal Simulation of First Pass Drug Perfusion in the Liver. PLoS Comput. Biol. 2014, 10, e1003499. [Google Scholar] [CrossRef] [PubMed]
- Schwen, L.O.; Schenk, A.; Kreutz, C.; Timmer, J.; Rodríguez, M.M.B.; Kuepfer, L.; Preusser, T. Representative Sinusoids for Hepatic Four-Scale Pharmacokinetics Simulations. PLoS ONE 2015, 10, e133653. [Google Scholar] [CrossRef]
- Barléon, N.; Clarke, R.J.; Ho, H. Novel Methods for Segment-Specific Blood Flow Simulation for the Liver. Comput. Methods Biomech. Biomed. Eng. 2018, 21, 780–783. [Google Scholar] [CrossRef]
- Rezania, V.; Coombe, D.; Tuszynski, J.A. A Physiologically-Based Flow Network Model for Hepatic Drug Elimination III: 2D/3D DLA Lobule Models. Theor. Biol. Med. Model. 2016, 13, 9. [Google Scholar] [CrossRef]
- Ni, Y.; Li, J.-M.; Liu, M.-K.; Zhang, T.-T.; Wang, D.-P.; Zhou, W.-H.; Hu, L.-Z.; Lv, W.-L. Pathological Process of Liver Sinusoidal Endothelial Cells in Liver Diseases. World J. Gastroenterol. 2017, 23, 7666–7677. [Google Scholar] [CrossRef]
- Horn, T.; Christoffersen, P.; Henriksen, J.H. Alcoholic Liver Injury: Defenestration in Noncirrhotic Livers-a Scanning Electron Microscopic Study. Hepatology 1987, 7, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Hilmer, S.N.; Cogger, V.C.; Fraser, R.; McLean, A.J.; Sullivan, D.; Le Couteur, D.G. Age-Related Changes in the Hepatic Sinusoidal Endothelium Impede Lipoprotein Transfer in the Rat. Hepatology 2005, 42, 1349–1354. [Google Scholar] [CrossRef]
- Brainerd, C.; Gorti, V.; Janes, M.; Jones, K.; Khayat, S.; Liu, A.; Noonan-shueh, M.; Rao, S. Variable Fenestration of A 3D Nanoprinted Liver Sinusoid on a Chip. Dr. Ryan D. Sochol Department of Mechanical Engineering. Available online: http://hdl.handle.net/1903/24764 (accessed on 29 September 2021).
- Heppell, C.; Roose, T.; Richardson, G. A Model for Interstitial Drainage Through a Sliding Lymphatic Valve. Bull. Math. Biol. 2015, 77, 1101–1131. [Google Scholar] [CrossRef] [PubMed]
- Swartz, M.A. The Physiology of the Lymphatic System. Adv. Drug Deliv. Rev. 2001, 50, 3–20. [Google Scholar] [CrossRef]
- Wisse, E.; De Zanger, R.; Charles, K.; Van Der Smissen, P.; McCuskey, R. The Liver Sieve: Considerations Concerning the Structure and Function of Endothelial Fenestrae, the Sinusoidal Wall and the Space of Disse. Hepatology 1985, 5, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Iwata, H.; Ueda, Y. Pharmacokinetic Considerations in Development of a Bioartificial Liver. Clin. Pharmacokinet. 2004, 43, 211–225. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | (i) Model; (ii) Method; (iii) Sinusoid Dimensions; (iv) Flow; (v) Pressure; (vi) Fenestrations |
|---|---|
| Wisse, 1983 [10] | (i) Rat; (ii) SEM; (vi) porosity is higher and fenestrations have wider diameters in zone 3 than in zone 1 (97.92 vs. 76.57 nm and 11.63 vs. 6.81%) |
| Vidal-Vanaclocha and Barbera-Guillem, 1985 [8] | (i) Rat; (ii) SEM; (vi) zone 3 has wider fenestrations (94–121 nm vs. 73–101 nm) and a higher frequency (10.21–10.68 fenestrations/µm2 vs. 5.74–6.26 fenestrations/µm2) than zone 1 and a greater number of sieve plates (1.73-fold greater) |
| Horn, 1986 [7] | (i) Human; (ii) SEM; (vi) in zone 3, fenestrations are more numerous (23.5 vs. 19.2%) than in zone 1, and porosity is higher in zone 3 than in zone 1 (9.1 vs. 7.6%) |
| Wake, 1988 [3] | (i) Rat; (ii) light and electron microscopy; (iii) centrilobular LSECs are larger (longer and wider) than periportal LSECs |
| Henriksen and Lassen, 1988 [11] | (i) Theoretical model; (iv) the shape of the sinusoid does not affect the flow profile, which is characterized by an increasing speed moving from zone 1 to zone 3; (v) in humans, the pressure drop between the portal and central veins is between 3 and 5 mmHg (450 Pa) |
| Komatsu, 1990 [5] | (i) Rat; (ii) in vivo fluorescence microscopy; (iii) the diameter of the sinusoid increases from zone 1 to zone 2 to zone 3; 6.4 µm–7 µm–8.3 µm; (iv) the flow rate increases along the sinusoid, 143–221–331 µm/s; (v) the interpolated values of pressure within sinusoids are as follows: zone 1, 68–50; zone 2, 50–40; and zone 3, 40–28 mmHg |
| MacPhee, 1995 [4] | (i) Mouse and rat; (ii) high resolution in vivo microscopy; (iv) the flow speed is highly variable due to interactions between blood cells and the cells of the sinusoid; generally, the velocity in zone 3 is greater than in zone 1 |
| Yoon, 2013 [12] | (i) Mouse; (ii) computed tomography; (iii) zone 1 features a smaller diameter (8.8 vs. 13.7 µm) than zone 3; (vi) zone 1 has a lower porosity than zone 3 |
| Ryou, 2020 [13] | (v) Clinical portal hypertension has pressure above 5 mmHg (666 Pa), while normal pressure is around 3.4 mmHg (450 Pa) |
| Ref. | Mod. Obj. | Dim. | Origin | Bound. Cond. | Eval. Param. | Highlights |
|---|---|---|---|---|---|---|
| Bonfiglio (2010) [19]; Siggers (2014) [20] | Lobule | 2D | Numerical | Phys., post-resection, and lymph production | P, blood flow distribution (v), and lymph flow | An infinite lattice of hexagonal lobules, the sinusoid space as a porous medium, the resection effect, anisotropy and shear-dependent tissue deformation, and lymph production |
| Debbaut (2012) [21] | Three lobules | 3D | Three human lobule casts digitized using a micro-CT scanner | Phys. | P, permeability, preferential flow pathways, and WSS | A liver circulation anisotropy estimation |
| Piergiovanni (2017) [22] | Sinusoidal network | 3D | In vivo images; mouse model | Phys. | vmean, FRmass, and WSS | Local hemodynamics; an investigation into different degrees of occlusion |
| Hu (2017) [23] | Lobule | 3D | Numerical | Phys.; path. (fibrosis; cirrhosis) | P, vmean, and FRvol | Porous media approach; fibrotic–cirrhotic lobule |
| Processor | Intel i5-10300H |
|---|---|
| Clock Freq. [GHz] | 2.50 |
| Core # | 8 |
| Ram [GB] | 8 |
| Constant Radius | Divergent Radius | |||
|---|---|---|---|---|
| P [Pa] | V [m/s] | P [Pa] | V [m/s] | |
| max | 1067.69 | 0.001 | 1066.95 | 0.0032 |
| min | 800.146 | 0.0008 | 799.876 | 0.0007 |
| avg | 933.5973 | 0.00085 | 871.9508 | 0.0015 |
| Std.dev | 77.1903 | 1.00 × 10−5 | 69.201 | 0.0007 |
| Const. rad. 5% | Const. rad. Var | Const. rad 20% | |||||||
|---|---|---|---|---|---|---|---|---|---|
| l | f | D | l | f | D | l | f | D | |
| max | 0.00087 | 0.000038 | 0.000034 | 0.0015 | 0.000033 | 0.000035 | 0.0033 | 0.000016 | 0.000035 |
| min | 0.00013 | 0 | 0 | 0.00054 | 0 | 0 | 0.00085 | 0 | 0 |
| avg | 0.00084 | 2.8 × 10−6 | 0.000029 | 0.00086 | 1.2 × 10−6 | 0.00003 | 0.00086 | 0.000001 | 0.000032 |
| Std.dev | 0.000047 | 0.000005 | 0.000008 | 0.000044 | 2.5 × 10−6 | 7.7 × 10−6 | 0.00013 | 1.9 × 10−6 | 6.7 × 10−6 |
| Div. rad. 5% | Div. rad. Var | Div. rad. 20% | |||||||
| l | f | D | l | f | D | l | f | D | |
| max | 0.0031 | 0.00009 | 0.000053 | 0.0032 | 0.00009 | 0.000054 | 0.019 | 0.000049 | 0.000075 |
| min | 0.000022 | 0 | 0 | 0.000019 | 0 | 0 | 0.0007 | 0 | 0 |
| avg | 0.0015 | 0.000004 | 0.000025 | 0.0015 | 0.000002 | 0.000026 | 0.0015 | 1.8 × 10−6 | 0.000028 |
| Std.dev | 0.00066 | 8.5 × 10−6 | 0.000016 | 0.00067 | 6.63 × 10−6 | 0.000016 | 0.0011 | 4.3 × 10−6 | 0.000022 |
| Const. rad. 5% | Const. rad. Var | Const rad. 20% | |||||||
|---|---|---|---|---|---|---|---|---|---|
| l | f | D | l | f | D | l | f | D | |
| max | 0.002 | 0.0013 | 0.0014 | 0.002 | 0.0014 | 0.0014 | 0.0035 | 0.0014 | 0.003 |
| min | 0.00075 | 0 | 0 | 0.00065 | 0 | 0 | 0.000014 | 0 | 0 |
| avg | 0.00086 | 0.000057 | 0.00012 | 0.00086 | 0.000019 | 0.00012 | 0.00085 | 0.000029 | 0.00014 |
| Std.dev | 0.00024 | 0.00016 | 5.25 × 10−5 | 0.00025 | 0.00085 | 0.00026 | 0.0004 | 0.00012 | 0.00042 |
| Div. rad. 5% | Div. rad. Var | Div. rad. 20% | |||||||
| l | f | D | l | f | D | l | f | D | |
| max | 0.0041 | 0.0013 | 0.0014 | 0.004 | 0.0013 | 0.0014 | 0.025 | 0.0014 | 0.003 |
| min | 0.000016 | 0 | 0 | 0.000016 | 0 | 0 | 0.0007 | 0 | 0 |
| avg | 0.0014 | 0.000051 | 0.00011 | 0.0014 | 0.000025 | 0.00011 | 0.0017 | 0.000031 | 0.00012 |
| Std.dev | 0.0008 | 0.00015 | 0.00026 | 0.0008 | 0.00011 | 0.00025 | 0.0016 | 0.00013 | 0.00041 |
| Const. rad. 5% | Const. rad. Var | Const rad. 20% | |||||||
|---|---|---|---|---|---|---|---|---|---|
| l | f | D | l | f | D | l | f | D | |
| max | 1067 | 1054 | 1043 | 1067 | 1055 | 1044 | 1067 | 1061 | 1056 |
| min | 802 | 813 | 824 | 796 | 806 | 811 | 785 | 806 | 810 |
| avg | 934 | 934 | 934 | 933 | 883 | 931 | 933 | 933 | 933 |
| Std.dev | 76 | 73 | 73 | 77 | 67 | 74 | 77 | 76 | 76 |
| Div. rad. 5% | Div. rad. Var | Div. rad. 20% | |||||||
| l | f | D | l | f | D | l | f | D | |
| max | 1068 | 1031 | 1002 | 1067 | 1031 | 1001 | 1074 | 1056 | 1040 |
| min | 809 | 8110 | 813 | 805 | 802 | 806 | 748 | 826 | 827 |
| avg | 878 | 877 | 878 | 874 | 844 | 873 | 891 | 891 | 891 |
| Std.dev | 67 | 62 | 59 | 68 | 53 | 61 | 65 | 63 | 62 |
| Const. rad. 5% | Const. rad. Var | Const rad. 20% | |||||||
|---|---|---|---|---|---|---|---|---|---|
| l | f | D | l | f | D | l | f | D | |
| max | 1067 | 949 | 934 | 1067 | 952 | 939 | 1067 | 989 | 983 |
| min | 794 | 592 | 102 | 798 | 588 | 102 | 800 | 604 | 103 |
| avg | 917 | 876 | 836 | 919 | 857 | 840 | 917 | 900 | 881 |
| Std.dev | 73 | 65 | 140 | 71 | 50 | 140 | 69 | 65 | 110 |
| Div. rad. 5% | Div. rad. Var | Div. rad. 20% | |||||||
| l | f | D | l | f | D | l | f | D | |
| max | 1067 | 880 | 865 | 1067 | 883 | 868 | 1066 | 929 | 915 |
| min | 805 | 570 | 102 | 806 | 586 | 102 | 656 | 600 | 105 |
| avg | 869 | 828 | 791 | 870 | 823 | 792 | 850 | 834 | 816 |
| Std.dev | 65 | 50 | 129 | 65 | 34 | 128 | 68 | 50 | 93 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boninsegna, M.; McCourt, P.A.G.; Holte, C.F. The Computed Sinusoid. Livers 2023, 3, 657-673. https://doi.org/10.3390/livers3040043
Boninsegna M, McCourt PAG, Holte CF. The Computed Sinusoid. Livers. 2023; 3(4):657-673. https://doi.org/10.3390/livers3040043
Chicago/Turabian StyleBoninsegna, Matteo, Peter A. G. McCourt, and Christopher Florian Holte. 2023. "The Computed Sinusoid" Livers 3, no. 4: 657-673. https://doi.org/10.3390/livers3040043