
Posterosuperior Segments of the Liver: Comparison of Short-Term Outcomes between Open and Minimally Invasive Surgery Performed by a Single Surgeon


Abstract
:1. Introduction
2. Methods
2.1. Variables and Definitions
2.2. Surgical Techniques
2.2.1. OLR Technique
2.2.2. LLR Techniques
2.3. Study Endpoints
2.4. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Surgical Characteristics
3.3. Postoperative Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OLR | Open liver resection |
| LLL | Laparoscopic liver resection |
| PSS | Posterosuperior segment |
| LOS | Length of stay |
References
- Reich, H.; McGlynn, F.; DeCaprio, J.; Budin, R. Laparoscopic excision of benign liver lesions. Obstet. Gynecol. 1991, 78 Pt 2, 956–958. [Google Scholar] [PubMed]
- Buell, J.F.; Cherqui, D.; Geller, D.A.; O’rourke, N.; Iannitti, D.; Dagher, I.; Koffron, A.J.; Thomas, M.; Gayet, B.; Han, H.S.; et al. The International Position on Laparoscopic Liver Surgery: The Louisville Statement, 2008. Ann. Surg. 2009, 250, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.Y.; Han, H.S.; Yoon, Y.S.; Shin, S.H. Feasibility of laparoscopic liver resection for tumors located in the posterosuperior segments of the liver, with a special reference to overcoming current limitations on tumor location. Surgery 2008, 144, 32–38. [Google Scholar] [CrossRef]
- Wakabayashi, G.; Cherqui, D.; Geller, D.A.; Buell, J.F.; Kaneko, H.; Han, H.S.; Asbun, H.; O’rourke, N.; Tanabe, M.; Koffron, A.J.; et al. Recommendations for laparoscopic liver resection: A report from the second international consensus conference held in Morioka. Ann. Surg. 2015, 261, 619–629. [Google Scholar]
- Abu Hilal, M.; Aldrighetti, L.; Dagher, I.; Edwin, B.; Troisi, R.I.; Alikhanov, R.; Aroori, S.; Belli, G.; Besselink, M.; Briceno, J.; et al. The Southampton Consensus Guidelines for Laparoscopic Liver Surgery: From Indication to Implementation. Ann. Surg. 2018, 268, 11–18. [Google Scholar] [CrossRef]
- Lee, W.; Han, H.-S.; Yoon, Y.-S.; Cho, J.Y.; Choi, Y.; Shin, H.K.; Choi, H.; Jang, J.S.; Kwon, S.U. Comparison of laparoscopic liver resection for hepatocellular carcinoma located in the posterosuperior segments or anterolateral segments: A case-matched analysis. Surgery 2016, 160, 1219–1226. [Google Scholar] [CrossRef]
- Guro, H.; Cho, J.Y.; Han, H.S.; Yoon, Y.S.; Choi, Y.; Jang, J.S.; Kwon, S.U.; Kim, S.; Choi, J.K. Laparoscopic liver resection of hepatocellular carcinoma located in segments 7 or 8. Surg. Endosc. 2018, 32, 872–878. [Google Scholar] [CrossRef]
- Tanaka, S.; Kubo, S.; Kanazawa, A.; Takeda, Y.; Hirokawa, F.; Nitta, H.; Nakajima, T.; Kaizu, T.; Kaneko, H.; Wakabayashi, G. Validation of a Difficulty Scoring System for Laparoscopic Liver Resection: A Multicenter Analysis by the Endoscopic Liver Surgery Study Group in Japan. J. Am. Coll. Surg. 2017, 225, 249–258.e1. [Google Scholar] [CrossRef]
- Russolillo, N.; Maina, C.; Fleres, F.; Langella, S.; Lo Tesoriere, R.; Ferrero, A. Comparison and validation of three difficulty scoring systems in laparoscopic liver surgery: A retrospective analysis on 300 cases. Surg. Endosc. 2020, 34, 5484–5494. [Google Scholar] [CrossRef]
- Halls, M.C.; Berardi, G.; Cipriani, F.; Barkhatov, L.; Lainas, P.; Harris, S.; D’Hondt, M.; Rotellar, F.; Dagher, I.; Aldrighetti, L.; et al. Development and validation of a difficulty score to predict intraoperative complications during laparoscopic liver resection. Br. J. Surg. 2018, 105, 1182–1191. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Fuks, D.; Kokudo, N.; Gayet, B. Difficulty of Laparoscopic Liver Resection: Proposal for a New Classification. Ann. Surg. 2018, 267, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Ban, D.; Tanabe, M.; Ito, H.; Otsuka, Y.; Nitta, H.; Abe, Y.; Hasegawa, Y.; Katagiri, T.; Takagi, C.; Itano, O.; et al. A novel difficulty scoring system for laparoscopic liver resection. J. Hepatobiliary Pancreat. Sci. 2014, 21, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, G. What has changed after the Morioka consensus conference 2014 on laparoscopic liver resection? HepatoBiliary Surg. Nutr. 2016, 5, 281–289. [Google Scholar] [CrossRef]
- Tanaka, S.; Kawaguchi, Y.; Kubo, S.; Kanazawa, A.; Takeda, Y.; Hirokawa, F.; Nitta, H.; Nakajima, T.; Kaizu, T.; Kaibori, M.; et al. Validation of index-based IWATE criteria as an improved difficulty scoring system for laparoscopic liver resection. Surgery 2019, 165, 731–740. [Google Scholar] [CrossRef]
- Tripke, V.; Huber, T.; Mittler, J.; Lang, H.; Heinrich, S. Prediction of complexity and complications of laparoscopic liver surgery: The comparison of the Halls-score to the IWATE-score in 100 consecutive laparoscopic liver resections. J. Hepatobiliary Pancreat. Sci. 2020, 27, 380–387. [Google Scholar] [CrossRef]
- Hibi, T.; Cherqui, D.; Geller, D.A.; Itano, O.; Kitagawa, Y.; Wakabayashi, G. Expanding indications and regional diversity in laparoscopic liver resection unveiled by the International Survey on Technical Aspects of Laparoscopic Liver Resection (INSTALL) study. Surg. Endosc. 2016, 30, 2975–2983. [Google Scholar] [CrossRef]
- Strasberg, S.M.; Belghiti, J.; Clavien, P.A.; Gadzijev, E.; Garden, J.O.; Lau, W.Y.; Makuuchi, M.; Strong, R.W. The Brisbane 2000 Terminology of Liver Anatomy and Resections. HPB 2000, 2, 333–339. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. PLoS Med. 2007, 4, 1623–1627. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Doyle, D.J.; Hendrix, J.M.; Garmon, E.H. American Society of Anesthesiologists Classification. Available online: https://europepmc.org/article/NBK/nbk441940 (accessed on 4 June 2023).
- Barron, J.O.; Orabi, D.; Moro, A.; Quintini, C.; Berber, E.; Aucejo, F.N.; Sasaki, K.; Kwon, C.-H.D. Validation of the IWATE criteria as a laparoscopic liver resection difficulty score in a single North American cohort. Surg. Endosc. 2021, 36, 3601–3609. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Garden, O.J.; Padbury, R.; Rahbari, N.N.; Adam, R.; Capussotti, L.; Fan, S.T.; Yokoyama, Y.; Crawford, M.; Makuuchi, M.; et al. Bile leakage after hepatobiliary and pancreatic surgery: A definition and grading of severity by the International Study Group of Liver Surgery. Surgery 2011, 149, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Brooke-Smith, M.; Crawford, M.; Adam, R.; Koch, M.; Makuuchi, M.; Dematteo, R.P.; Christophi, C.; et al. Posthepatectomy liver failure: A definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery 2011, 149, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Maddern, G.; Koch, M.; Hugh, T.J.; Fan, S.T.; Nimura, Y.; Figueras, J.; Vauthey, J.-N.; et al. Post-hepatectomy haemorrhage: A definition and grading by the International Study Group of Liver Surgery (ISGLS). HPB 2011, 13, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Pringle, J.H.V. Notes on the arrest of hepatic hemorrhage due to trauma. Ann. Surg. 1908, 48, 541–549. [Google Scholar] [CrossRef]
- Abu Hilal, M.; Tschuor, C.; Kuemmerli, C.; López-Ben, S.; Lesurtel, M.; Rotellar, F. Laparoscopic posterior segmental resections: How I do it: Tips and pitfalls. Int. J. Surg. 2020, 82, 178–186. [Google Scholar] [CrossRef]
- Machado, M.A.C.; Makdissi, F.F.; Galvão, F.H.; Machado, M.C. Intrahepatic Glissonian approach for laparoscopic right segmental liver resections. Am. J. Surg. 2008, 196, e38–e42. [Google Scholar] [CrossRef]
- Cheng, K.-C.; Yeung, Y.-P.; Ho, K.-M.; Chan, F.K.-M. Laparoscopic Right Posterior Sectionectomy for Malignant Lesions: An Anatomic Approach. J. Laparoendosc. Adv. Surg. Tech. 2015, 25, 646–650. [Google Scholar] [CrossRef]
- Ishizawa, T.; Gumbs, A.A.; Kokudo, N.; Gayet, B. Laparoscopic segmentectomy of the liver: From segment I to VIII. Ann. Surg. 2012, 256, 959–964. [Google Scholar] [CrossRef]
- Teramoto, K.; Kawamura, T.; Takamatsu, S.; Noguchi, N.; Nakamura, N.; Arii, S. Laparoscopic and Thoracoscopic Partial Hepatectomy for Hepatocellular Carcinoma. World J. Surg. 2003, 27, 1131–1136. [Google Scholar] [CrossRef]
- Fiorentini, G.; Ratti, F.; Cipriani, F.; Catena, M.; Paganelli, M.; Aldrighetti, L. Tips and Tricks for a Laparoscopic Approach to Paracaval Liver Segments. Ann. Surg. Oncol. 2018, 25, 1695–1698. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.-W.; Su, W.-L.; Wang, S.-N. Alternative Laparoscopic Intracorporeal Pringle Maneuver by Huang’s Loop. World J. Surg. 2018, 42, 3312–3315. [Google Scholar] [CrossRef] [PubMed]
- Tomassini, F.; Scuderi, V.; Colman, R.; Vivarelli, M.; Montalti, R.; Troisi, R.I. The single surgeon learning curve of laparoscopic liver resection: A continuous evolving process through stepwise difficulties. Medicine 2016, 95, e5138. [Google Scholar] [CrossRef] [PubMed]
- Vigano, L.; Laurent, A.; Tayar, C.; Tomatis, M.; Ponti, A.; Cherqui, D. The Learning Curve in Laparoscopic Liver Resection: Improved feasibility and reproducibility. Ann. Surg. 2009, 250, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Cucchetti, A.; Cescon, M.; Ercolani, G.; Bigonzi, E.; Torzilli, G.; Pinna, A.D. A Comprehensive Meta-regression Analysis on Outcome of Anatomic Resection Versus Nonanatomic Resection for Hepatocellular Carcinoma. Ann. Surg. Oncol. 2012, 19, 3697–3705. [Google Scholar] [CrossRef]
- Li, S.; Huang, T.; Shen, S.; Hua, Y.; Hu, W.; Kuang, M.; Peng, B.; Liang, L. Anatomical versus non-anatomical liver resection for hepatocellular carcinoma exceeding Milan criteria. Br. J. Surg. 2017, 104, 118–127. [Google Scholar] [CrossRef]
- Moris, D.; Tsilimigras, D.I.; Kostakis, I.D.; Ntanasis-Stathopoulos, I.; Shah, K.N.; Felekouras, E.; Pawlik, T.M. Anatomic versus non-anatomic resection for hepatocellular carcinoma: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2018, 44, 927–938. [Google Scholar] [CrossRef]
- Li, L.; Xu, L.; Wang, P.; Zhang, M.; Li, B. The risk factors of intraoperative conversion during laparoscopic hepatectomy: A systematic review and meta-analysis. Langenbeck’s Arch. Surg. 2022, 407, 469–478. [Google Scholar] [CrossRef]
- Yoon, Y.-S.; Han, H.-S.; Cho, J.Y.; Ahn, K.S. Total laparoscopic liver resection for hepatocellular carcinoma located in all segments of the liver. Surg. Endosc. 2010, 24, 1630–1637. [Google Scholar] [CrossRef]
- Berardi, G.; Aghayan, D.; Fretland, Å.A.; Elberm, H.; Cipriani, F.; Spagnoli, A.; Montalti, R.; Ceelen, W.P.; Aldrighetti, L.; Abu Hilal, M.; et al. Multicentre analysis of the learning curve for laparoscopic liver resection of the posterosuperior segments. Br. J. Surg. 2019, 106, 1512–1522. [Google Scholar] [CrossRef]
- Buell, J.F.; Thomas, M.J.; Doty, T.C.; Gersin, K.S.; Merchen, T.D.; Gupta, M.; Rudich, S.M.; Woodle, E.S. An initial experience and evolution of laparoscopic hepatic resectional surgery. Surgery 2004, 136, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Bueno, A.; Rotellar, F.; Benito, A.; Martí-Cruchaga, P.; Zozaya, G.; Hermida, J.; Pardo, F. Laparoscopic limited liver resection decreases morbidity irrespective of the hepatic segment resected. HPB 2014, 16, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Aldrighetti, L.; Guzzetti, E.; Pulitanò, C.; Cipriani, F.; Catena, M.; Paganelli, M.; Ferla, G. Case-matched analysis of totally laparoscopic versus open liver resection for HCC: Short and middle term results. J. Surg. Oncol. 2010, 102, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Scuderi, V.; Barkhatov, L.; Montalti, R.; Ratti, F.; Cipriani, F.; Pardo, F.; Tranchart, H.; Dagher, I.; Rotellar, F.; Abu Hilal, M.; et al. Outcome after laparoscopic and open resections of posterosuperior segments of the liver. Br. J. Surg. 2017, 104, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Fuks, D.; Gayet, B. Laparoscopic surgery of postero-lateral segments: A comparison between transthoracic and abdominal ap-proach. Updates Surg. 2015, 67, 141–145. [Google Scholar] [CrossRef]
- Morise, Z.; Kawabe, N.; Tomishige, H.; Nagata, H.; Kawase, J.; Arakawa, S.; Isetani, M. How Far Can We Go with Laparoscopic Liver Resection for Hepatocellular Carcinoma? Laparoscopic Sectionectomy of the Liver Combined with the Resection of the Major Hepatic Vein Main Trunk. BioMed Res. Int. 2015, 2015, 960752. [Google Scholar] [CrossRef]
- Cipriani, F.; Ratti, F.; Paganelli, M.; Reineke, R.; Catena, M.; Aldrighetti, L. Laparoscopic or open approaches for posterosuperior and anterolateral liver resections? A propensity score based analysis of the degree of advantage. HPB 2019, 21, 1676–1686. [Google Scholar] [CrossRef]
- Taesombat, W.; Nonthasoot, B.; Sutherasan, M.; Nivatvongs, S.; Sirichindakul, B. Long-term outcomes of laparoscopic versus open liver resection for hepatocellular carcinoma: Retrospective case-matched study. Int. J. Surg. Open 2020, 24, 12–17. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristics | Total | OLR | LLR | p-Value |
|---|---|---|---|---|
| Period of resection | <0.001 | |||
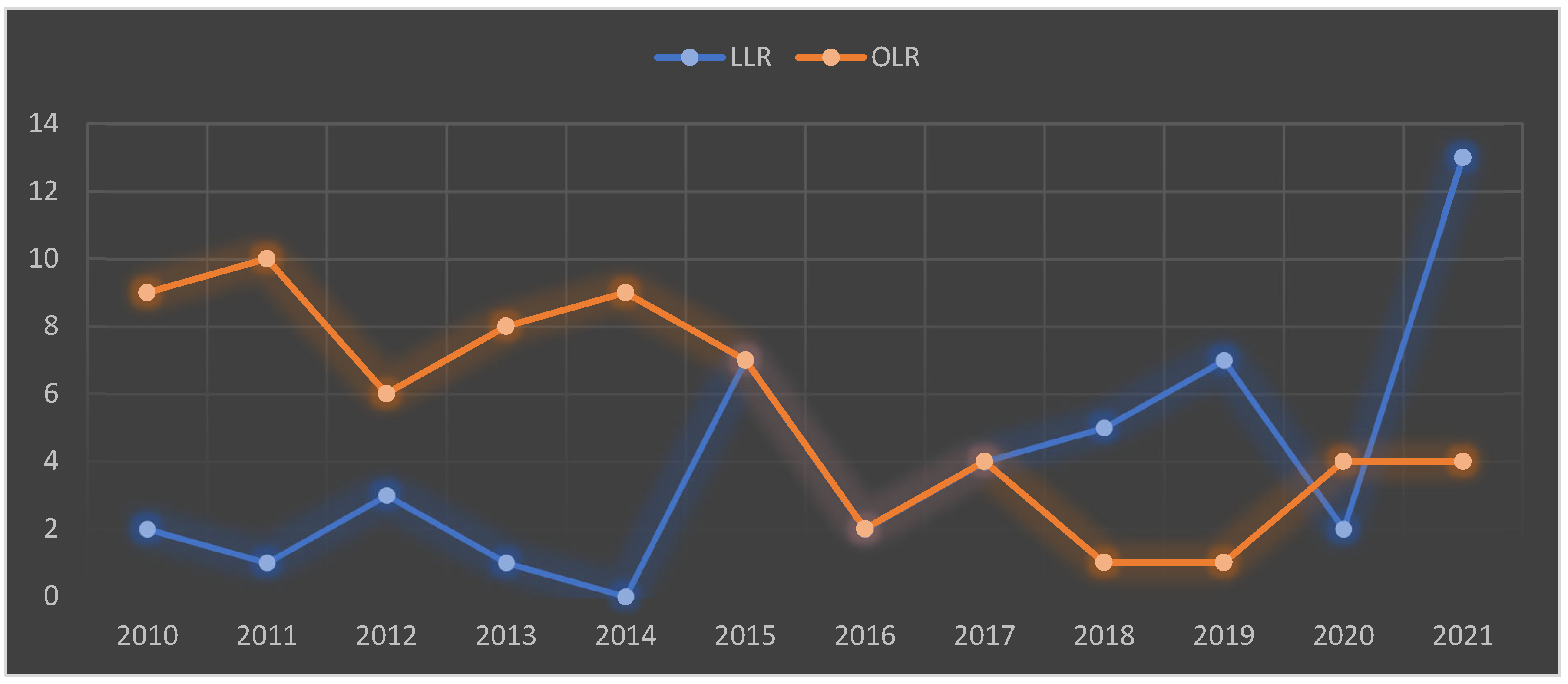
| 2010–2015 | 65 (56.2%) | 49 (75.3%) | 16 (24.6%) | |
| 2016–2021 | 47 (43.7%) | 14 (29.7%) | 33 (70.2%) | |
| Median age (IQR), years | 70 (58.7–75.2) | 70 (61–74) | 70 (57.5–76) | 0.701 |
| Male sex, n (%) | 88 (78.5%) | 52 (80.0%) | 36 (76.5%) | 0.669 |
| Median BMI (IQR) | 25.4 (23.7–28.3) | 25.5 (23.8–28.4) | 25.4 (23.2–27.7) | 0.618 |
| Previous liver surgery, n (%) | 14 (12.5%) | 12 (18.4%) | 2 (4.2%) | 0.025 |
| Preoperative ascites | 8 (7.0%) | 5 (7.6%) | 3 (4.5%) | 0.797 |
| Charlson Comorbidity Index, median (IQR) | 5 (4–8) | 5 (3–8) | 6 (4–7.5) | 0.612 |
| ASA score, n (%) | 0.0140 | |||
| 1 | 1/112 (2.6%) | 2/65 (3.1%) | 1/47 (2.1%) | |
| 2 | 61/112 (54.4%) | 39/65 (60.0%) | 22/47 (46.8%) | |
| 3 | 48/112 (42.8%) | 24/65 (36.9%) | 24/47 (51.0%) | |
| 4 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Etiology, n (%) | 0.470 | |||
| Cholangiocarcinoma | 7 (6.2%) | 6 (9.5%) | 1 (2.1%) | |
| HCC | 51 (45.5%) | 24 (38.0%) | 27 (55.1%) | |
| CRLM | 48 (42.8%) | 32 (50.7%) | 16 (32.6%) | |
| LM | 2 (1.7%) | 1 (1.5%) | 1 (2.1%) | |
| Benign disease | 4 (3.5%) | 2 (3.0%) | 2 (4.2%) | |
| Child–Pugh score, median (IQR) | 6 (5–7) | 6 (5–7) | 6 (5–7) | 0.147 |
| Child–Pugh n (%) | 0.103 | |||
| A | 74 (66.0%) | 47 (72.3%) | 27 (57.4%) | |
| B | 38 (33.9%) | 18 (27.6%) | 20 (42.5%) | |
| Meld score, median (IQR) | 8 (6–10) | 7 (6–10) | 8 (7–12) | 0.034 |
| Median tumor size, mm (IQR) | 31 (22–43) | 32 (24–47) | 26 (21–41) | 0.103 |
| N lesions, median (IQR) | 1 (1–2) | 1 (1–2) | 1 (1–1.5) | 0.026 |
| Tumor location, n (%) | 0.441 | |||
| I | 1 (0.8%) | 1 (1.5%) | 0 (0.0%) | |
| IVa | 4 (3.5%) | 2 (3.0%) | 2 (4.2%) | |
| VIs | 10 (8.9%) | 6 (9.2%) | 4 (8.5%) | |
| VII | 57 (50.8%) | 35 (53.8%) | 22 (46.8%) | |
| VIII | 40 (35.7%) | 21 (32.3%) | 19 (40.4%) | |
| Iwate score, Difficulty Index, median (IQR) | 7 (6–10) | 8 (7–10) | 7 (5–9) | <0.001 |
| Iwate, Difficulty Level | <0.001 | |||
| Low | 3 (2.6%) | 1 (1.5%) | 2 (4.2%) | |
| Intermediate | 32 (28.5%) | 11 (16.9%) | 21 (44.6%) | |
| Advanced | 45 (40.1%) | 26 (40.0%) | 19 (40.4%) | |
| Expert | 32 (28.5%) | 27 (41.5%) | 5 (10.6%) | |
| IMM, Difficulty Level | 0.352 | |||
| I | 49 (43.7%) | 23 (48.9%) | 26 (40.0%) | |
| II | 10 (8.9%) | 4 (8.5%) | 6 (9.2%) | |
| III | 53 (47.3%) | 20 (42.5%) | 33 (50.7%) | |
| Intraoperative Detailes | Total | OLR | LLR | p-Value |
|---|---|---|---|---|
| Operative time, median (IQR) | 300 (223.7–248.7) | 315 (240–360) | 250 (210–315) | 0.012 |
| Tipe of resection, n (%) | 0.121 | |||
| Anatomical resection | 55/112 (50.8%) | 36/65 (55.4%) | 19/47 (40.4%) | |
| Atypical resection | 57/112 (49.2%) | 29/65 (44.6%) | 28/47 (59.6%) | |
| Pringle Manuever time, median (IQR) | 30.0 (14.2–47.2) | 30.0 (12.0–45.0) | 30.0 (15.5–52.0) | 0.678 |
| Blood loss (mL), median (IQR) | 150 (100–200) | 150 (100–300) | 100 (100–200) | 0.194 |
| Conversion rate, n (%) | 15/47 (31.9%) | / | 15/47 (31.9%) | / |
| Postoperative Outcomes | Total | OLR | LLR | p-Value |
|---|---|---|---|---|
| LOS, days (IQR) | 10 (7.75–14.5) | 11 (9–21) | 8 (7–11) | <0.001 |
| ICU LOS, days (IQR) | 1 (1–2.25) | 2 (1–3) | 1(0–2) | 0.011 |
| Severe complications, Clavien–Dindo > 3b | 5 (4.4%) | 4 (6.1%) | 1 (2.1%) | 0.315 |
| Clavien–Dindo, n (%) | <0.001 | |||
| 1 | 46/112 (41.0%) | 35/65 (53.8%) | 11/47 (23.4%) | |
| 2 | 39/112 (34.8%) | 27/65 (41.5%) | 12/47 (25.5%) | |
| 3a | 18/112 (16.0%) | 16/65 (24.6%) | 2/47 (4.2%) | |
| 3b | 4/112 (3.5%) | 3/65 (4.6%) | 1/47 (2.1%) | |
| 4a | 0/112 (0.0%) | 0/65 (0.0%) | 0/47 (0.0%) | |
| 4b | 1/112 (0.8%) | 1/65 (1.5%) | 0/47 (0.0%) | |
| 5 | 1/112 (0.8%) | 1/65 (1.5%) | 0/47 (0.0%) | |
| Bile leakage, n (%) | 0.129 | |||
| A | 6 (5.3%) | 5 (7.6%) | 1 (2.1%) | |
| B | 1 (0.8%) | 1 (1.5%) | 0 (0.0%) | |
| Liver failure, n (%) | 1 (0.8%) | 1 (1.5%) | 0 (0.0%) | NA |
| Postoperative ascites, n (%) | 11 (9.8%) | 9 (13.8%) | 2 (4.2%) | 0.095 |
| Bleeding, n (%) | 5 (4.4%) | 4 (6.1%) | 1 (2.1%) | 0.315 |
| Pulmonary complications, n (%) | 23 (20.5%) | 15 (23.0%) | 8 (17.0%) | 0.438 |
| Postoperative infection, n (%) | 19 (16.9%) | 9 (13.8%) | 10 (21.2%) | 0.305 |
| Cardiovascular complications, n (%) | 12 (10.7%) | 7 (10.7%) | 5 (10.6%) | 0.987 |
| Cerebrovascular complication, n (%) | 1 (0.8%) | 1 (1.5%) | 0 (0.0%) | NA |
| Readmission within 90 days, n (%) | 12 (10.7%) | 8 (12.3%) | 4 (8.5%) | 0.527 |
| Mortality within 90 days, n (%) | 1 (0.8%) | 1 (1.5%) | 0 (0.0%) | NA |
| Variable | No Severe Complication (n = 107) | Severe Complication (n = 5) | p-Value |
|---|---|---|---|
| Age ≥ 65 y | 67 (62.6%) | 3 (60.0%) | 0.907 |
| Gender, male | 83 (77.5%) | 5 (100.0%) | NA |
| BMI > 25 kg/m2 | 61 (57.0%) | 3 (60.0%) | 0.902 |
| ASA score ≥ 3 | 45 (42.0%) | 3 (60.0%) | 0.435 |
| Charlson Comorbidity Index, n (%) | 0.524 | ||
| 0–1 | 6 (5.60%) | 0 (0.0%) | |
| 2–3 | 21 (19.6%) | 0 (0.0%) | |
| 4–5 | 30 (28.0%) | 2 (40.0%) | |
| 6–7 | 20 (18.6%) | 2 (40.0%) | |
| >8 | 30 (28.0%) | 1 (20.0%) | |
| Liver chirrosis, n (%) | 6 (5.6%) | 2 (40.0%) | 0.004 |
| Child–Pugh grade B, n (%) | 37 (34.5%) | 1 (20.0%) | 0.508 |
| MELD score, median (IQR) | 8 (6–10) | 8 (5–9) | 0.910 |
| Tumor size ≥ 3 cm, n (%) | 54 (50.4%) | 3 (60.0%) | 0.684 |
| Tumor location | 0.446 | ||
| Segment 1 | 1 (0.9%) | 0 (0.0%) | |
| Segment 4s | 4 (3.7%) | 0 (0.0%) | |
| Segment 6s | 9 (8.4%) | 1 (20.0%) | |
| Segment 7 | 56 (52.3%) | 1 (20.0%) | |
| Segment 8 | 37 (34.5%) | 3 (60.0%) | |
| Multiple lesions, n (%) | 38 (35.0%) | 4 (80.0%) | 0.046 |
| Proximity to the major hepatic vessels, n (%) | 58 (54.2%) | 4 (80.0%) | 0.262 |
| Segmentectomy, n (%) | 52 (48.5%) | 3 (60.0%) | 0.625 |
| LLR, n (%) | 46 (42.9%) | 1 (20.0%) | 0.315 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giuffrida, M.; Iaria, M.; Dalla Valle, R. Posterosuperior Segments of the Liver: Comparison of Short-Term Outcomes between Open and Minimally Invasive Surgery Performed by a Single Surgeon. Livers 2023, 3, 674-686. https://doi.org/10.3390/livers3040044
Giuffrida M, Iaria M, Dalla Valle R. Posterosuperior Segments of the Liver: Comparison of Short-Term Outcomes between Open and Minimally Invasive Surgery Performed by a Single Surgeon. Livers. 2023; 3(4):674-686. https://doi.org/10.3390/livers3040044
Chicago/Turabian StyleGiuffrida, Mario, Maurizio Iaria, and Raffaele Dalla Valle. 2023. "Posterosuperior Segments of the Liver: Comparison of Short-Term Outcomes between Open and Minimally Invasive Surgery Performed by a Single Surgeon" Livers 3, no. 4: 674-686. https://doi.org/10.3390/livers3040044