
The Influence of Root Prominence on the Onset of Gingival Recession: A Systematic Review
 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Databases and Search Strategy
2.2. Eligibility Criteria
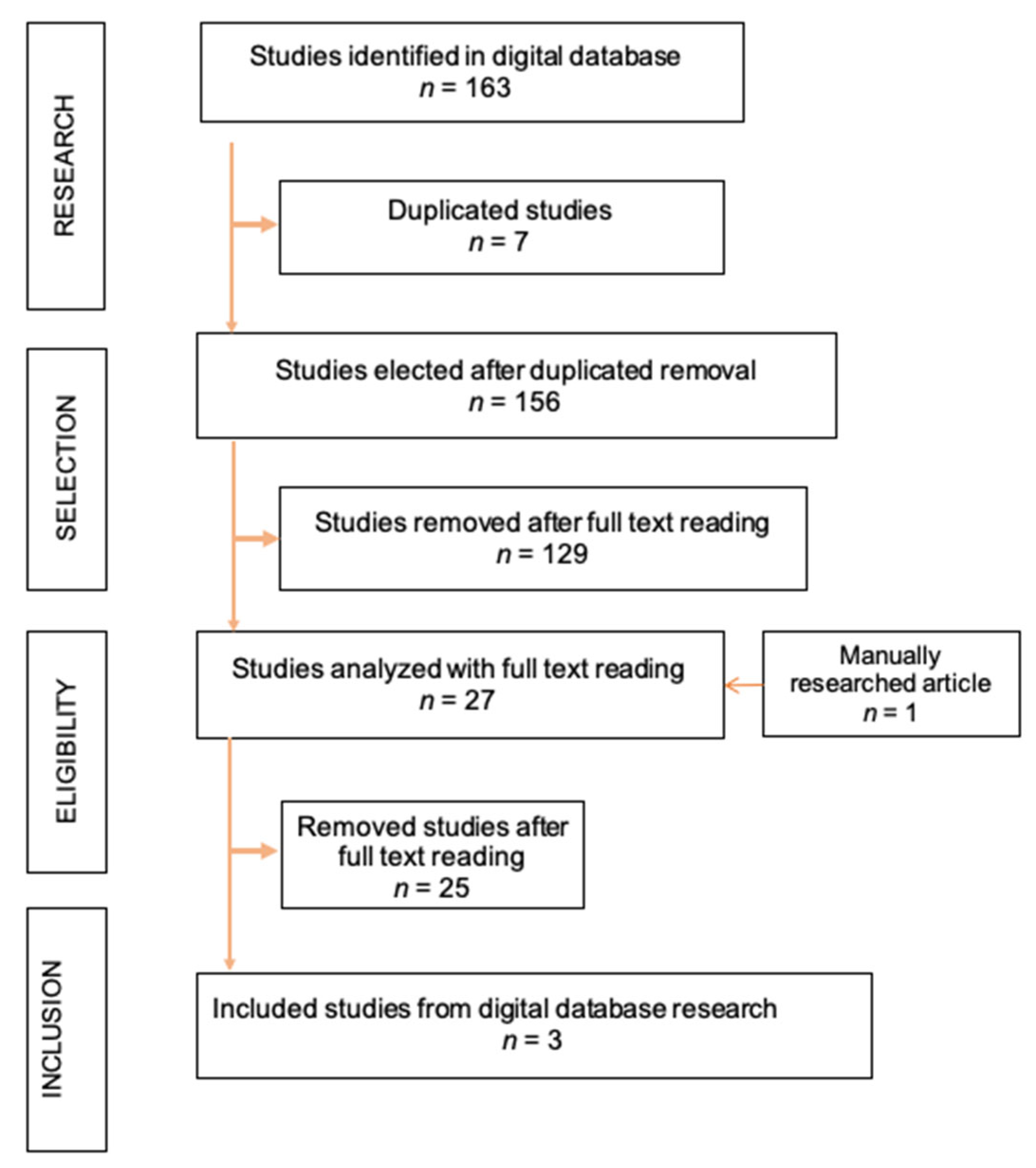
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Studies Description
3.3. Quality Assessment
4. Discussion
4.1. Existent Classifications for Gingival Recession Defects and Future Suggestions
4.2. Limitations and Strengths of the Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fernandes, G.V.D.O.; Santos, N.B.; Siqueira, R.A.; Wang, H.L.; Blanco-Carrion, J.; Fernandes, J.C. Autologous platelet concentrate of 2nd and 3rd generations efficacy in the surgical treatment of gingival recession: An overview of systematic reviews. J. Indian Soc. Periodontol. 2021, 25, 463–479. [Google Scholar] [CrossRef]
- Pilloni, A.; Marini, L.; Zeza, B.; Ferlosio, A.; Aghazada, R. Histologic Analysis of Clinically Healthy Human Gingiva in Patients with Altered Passive Eruption. Dent. J. 2021, 9, 29. [Google Scholar] [CrossRef] [PubMed]
- Serino, G.; Wennström, J.L.; Lindhe, J.; Eneroth, L. The prevalence and distribution of gingival recession in subjects with a high standard of oral hygiene. J. Clin. Periodontol. 1994, 21, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Jati, A.S.; Furquim, L.Z.; Consolaro, A. Gingival recession: Its causes and types, and the importance of orthodontic treatment. Dent. Press J. Orthod. 2016, 21, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Rubin, E.; Reisner, H. Essentials of Rubin’s Pathology, 6th ed.; Wolters Kluwer: Hong Kong, China, 2013. [Google Scholar]
- Zucchelli, G. Chirurgia Estetica Mucogengivale; Quintessenza Edizioni: Milan, Italy, 2012. [Google Scholar]
- Mythri, S.; Arunkumar, S.; Hegde, S.; Rajesh, S.; Munaz, M.; Ashwin, D. Etiology and occurrence of gingival recession—An epidemiological study. J. Indian Soc. Periodontol. 2015, 19, 671. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Testori, T.; de Sanctis, M. Clinical and Anatomical Factors Limiting Treatment Outcomes of Gingival Recession: A New Method to Predetermine the Line of Root Coverage. J. Periodontol. 2006, 77, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Tavelli, L.; Barootchi, S.; Stefanini, M.; Wang, H.L.; Cortellini, P. Clinical Remarks on the Significance of Tooth Malposition and Papillae Dimension on the Prediction of Root Coverage. Int. J. Periodontics Restor. Dent. 2020, 40, 795–803. [Google Scholar] [CrossRef]
- Stefanini, M.; Marzadori, M.; Aroca, S.; Felice, P.; Sangiorgi, M.; Zucchelli, G. Decision making in root-coverage procedures for the esthetic outcome. Periodontol. 2000 2018, 77, 54–64. [Google Scholar] [CrossRef]
- Saletta, D.; Baldi, C.; Nieri, M.; Ceppatelli, P.; Franceschi, D.; Rotundo, R.; Cairo, F.; Pini Prato, G.P. Root Curvature: Differences Among Dental Morphotypes and Modifications After Mechanical Instrumentation. J. Periodontol. 2005, 76, 723–730. [Google Scholar] [CrossRef]
- El Chaar, E.S.; Oshman, S.; Danesh-Sani, S.; Pooria, D.; Fallah Abed, P.; Castaño, A. Increasing Contact Between Soft Tissue Graft and Blood Supply A Technique for Managing Connective Tissue Grafting Over Prominent Root—Clinical case studies. Curr. Opin. Cosmet. Dent. 2016, 32, 52–66. [Google Scholar]
- Nicolucci, M.; Arlin, M. Gingival Recession—Etiology and Treatment. Prev. Dent. Can. 2011, 2, 6–11. [Google Scholar]
- Zachrisson, B.U. Orthodontics and periodontics. In Clinical Periodontology and Implant Dentistry, 3rd ed.; Munksgaard: Copenhagen, Denmark, 1998; pp. 741–793. [Google Scholar]
- Goldstein, M.; Brayer, L.; Schwartz, Z. A Critical Evaluation of Methods for Root Coverage. Crit. Rev. Oral Biol. Med. 1996, 7, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Thorstensson, H.; Falk, H.; Hugoson, A.; Olsson, J. Some salivary factors in insulin-dependent diabetics. Acta Odontol. Scand. 1989, 47, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Chambrone, D.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. The influence of tobacco smoking on the outcomes achieved by root-coverage procedures: A systematic review. J. Am. Dent. Assoc. 2009, 140, 294–306. [Google Scholar] [CrossRef]
- Kasaj, A. Gingival Recession Management; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Mlinek, A.; Smukler, H.; Buchner, A. The Use of Free Gingival Grafts for the Coverage of Denuded Roots. J. Periodontol. 1973, 44, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Lindhe, J. Parodontologia Clinica e Implantologia Orale, 6th ed.; Edi-Ermes: Milan, Italy, 2016; Volumes 1–2. [Google Scholar]
- Farsoun, C.F.; Castro, F.; Farsoun, J.; Fernandes, J.C.H.; Fernandes, G.V.O. Gingival recession in canines orthodontically aligned: A narrative Review. Int. J. Sci. Dent. 2023, 3, 100–121. [Google Scholar] [CrossRef]
- Wennstrom, J.L.; Lindhe, J.; Sinclair, F.; Thilander, B. Some periodontal tissue reactions to orthodontic tooth movement in monkeys. J. Clin. Periodontol. 1987, 14, 121–129. [Google Scholar] [CrossRef]
- Tezel, A.; Çanakçi, V.; Şiçek, Y.; Demir, T. Evaluation of Gingival Recession in Left-and Right-Handed Adults. Int. J. Neurosci. 2001, 110, 135–146. [Google Scholar] [CrossRef]
- Banihashemrad, S.A.; Fatemi, K.; Najafi, M.H. Effect of Smoking on Gingival Recession. Dent. Res. J. 2008, 5, 1–4. [Google Scholar]
- Tróia, P.M.B.P.S.; Spuldaro, T.R.; Fonseca, P.A.B.; Fernandes, G.V.O. Presence of Gingival Recession or Noncarious Cervical Lesions on Teeth under Occlusal Trauma: A Systematic Review. Eur. J. Gen. Dent. 2021, 10, 50–59. [Google Scholar] [CrossRef]
- Kassab, M.M.; Cohen, R.E. The etiology and prevalence of gingival recession. J. Am. Dent. Assoc. 2003, 134, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.D. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Chambrone, L.; Sukekava, F.; Araújo, M.G.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Root-Coverage Procedures for the Treatment of Localized Recession-Type Defects: A Cochrane Systematic Review. J. Periodontol. 2010, 81, 452–478. [Google Scholar] [CrossRef] [PubMed]
- Poormoradi, B.; Torkzaban, P.; Gholami, L.; Hooshyarfard, A.; Farhadian, M. Effect of Er, Cr (YSGG Laser Root Conditioning on the Success of Root Coverage with Subepithelial Connective Tissue Graft): A Randomized Clinical Trial with a 6-Month Follow-Up. J. Dent. 2018, 15, 230–239. [Google Scholar]
- Rasperini, G.; Acunzo, R.; Limiroli, E. Decision Making in Gingival Recession Treatment: Scientific Evidence and Clinical Experience. Clin. Adv. Periodontics 2011, 1, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Marques, T.; Santos NBMd Sousa, M.; Fernandes, J.C.H.; Fernandes, G.V.O. Mixed-Thickness Tunnel Access (MiTT) through a Linear Vertical Mucosal Incision for a Minimally Invasive Approach for Root Coverage Procedures in Anterior and Posterior Sites: Technical Description and Case Series with 1-Year Follow-Up. Dent. J. 2023, 11, 235. [Google Scholar] [CrossRef]
- Marques, T.M.; Santos, N.B.M.; Montero, J.; Correia, A.; Fernandes, G.V.O. The Effect of the Interproximal Creeping Attachment in Aesthetic Site After Root Coverage Surgery with VISTA Technique—A Case Report. Indian J. Dent. Res. 2023, 34, 90–93. [Google Scholar] [CrossRef]
- Evginer, M.S.; Olgun, E.; Parlak, H.M.; Dolgun, A.B.; Keceli, H.G. Comparison of two techniques in gingival recession treatment: A randomized one-year clinical follow-up study. Dent. Med. Probl. 2022, 59, 121–130. [Google Scholar] [CrossRef]
- Núñez, J.; Sanz-Esporrin, J.; Caffesse, R.; Sanz, M. A Two-Step Surgical Approach with Flattening of the Root Surface to Treat Localized Gingival Recessions Affecting Mandibular Incisors: A Case Series Report. J. Esthet. Restor. Dent. 2018, 38, 683–690. [Google Scholar] [CrossRef]
- Gil, A.; Bakhshalian, N.; Min, S.; Zadeh, H.H. Treatment of multiple recession defects with vestibular incision subperiosteal tunnel access (VISTA): A retrospective pilot study utilizing digital analysis. J. Esthet. Restor. Dent. 2018, 30, 572–579. [Google Scholar] [CrossRef]
- Gil, A.; Bakhshalian, N.; Min, S.; Nart, J.; Zadeh, H. Three-Dimensional Volumetric Analysis of Multiple Gingival Recession Defects Treated by the Vestibular Incision Subperiosteal Tunnel Access (VISTA) Procedure. J. Esthet. Restor. Dent. 2019, 39, 687–695. [Google Scholar] [CrossRef]
- Buti, J.; Baccini, M.; Nieri, M.; La Marca, M.; Pini-Prato, G.P. Bayesian network meta-analysis of root coverage procedures: Ranking efficacy and identification of best treatment. J. Clin. Periodontol. 2013, 40, 372–386. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.T.; Menezes, C.C.; Kahn, S.; Fischer, R.G.; Figueredo, C.M.S.; Fernandes, G.V.O. Gingival recession treatment with enamel matrix derivative associated with coronally advanced flap and subepithelial connective tissue graft: A split-mouth randomized controlled clinical trial with molecular evaluation. Clin. Oral Investig. 2022, 26, 1453–1463. [Google Scholar] [CrossRef] [PubMed]
- Wennström, J.L. Mucogingival Therapy. Ann. Periodontol. 1996, 1, 671–701. [Google Scholar] [CrossRef]
- Kahn, S.; Araújo, I.T.E.; Dias, A.T.; Souza, A.B.; Chambrone, L.; Fernandes, G.V.O. Histologic and histomorphometric analysis of connective tissue grafts harvested by the parallel incision method: A pilot randomized controlled trial comparing macro- and microsurgical approaches. Quintessence Int. 2021, 52, 772–778. [Google Scholar] [CrossRef]
- Kahn, S.; Oliveira, L.Z.; Dias, A.T.; Fernandes, G.V.O. Clinical evaluation and biological understanding of the early step-by-step healing after periodontal microsurgery: A case report with PES analysis comparing initial and 31-day result. J. Adv. Periodontol. Implant Dent. 2022, 14, 141–145. [Google Scholar] [CrossRef]
- Maia, V.T.G.; Kahn, S.; Souza, A.B.; Fernandes, G.V.O. Deepithelialized Connective Tissue Graft and The Reminiscent Epithelial Content After Harvested by the Harris’ Technique: A Histological and Morphometrical Case Series. Clin. Adv. Periodontics 2021, 11, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.; Dias, A.T.; Nobre, V.; Oliveira, L.Z.; Fernandes, G.V.O. Endodontic and periodontal treatment of complete buccal root and apex exposition: A challenging case report with 17 months follow-up. Clin. Adv. Periodontics 2022, 12, 152–158. [Google Scholar] [CrossRef]
- Santamaria, M.P.; Ambrosano, G.M.B.; Casati, M.Z.; Nociti, F.H., Jr.; Sallum, A.W.; Sallum, E.A. The influence of local anatomy on the outcome of treatment of gingival recession associated with non-carious cervical lesions. J. Periodontol. 2010, 81, 1027–1034. [Google Scholar] [CrossRef]
- De Rouck, T.; Eghbali, R.; Collys, K.; De Bruyn, H.; Cosyn, J. The gingival biotype revisited: Transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J. Clin. Periodontol. 2009, 36, 428–433. [Google Scholar] [CrossRef]
- Miller, P.D. Root coverage using the free soft tissue autograft following citric acid application. III. A successful and predictable procedure in areas of deep-wide recession. Int. J. Periodontics Restor. Dent. 1985, 5, 14–37. [Google Scholar]
- Holbrook, T.; Ochsenbein, C. Complete coverage of the denuded root surface with a one-stage gingival graft. Int. J. Periodontics Restor. Dent. 1983, 3, 8–27. [Google Scholar]
- Tinti, C.; Vincenzi, G.; Cortellini, P.; Prato, G.P.; Clauser, C. Guided Tissue Regeneration in the Treatment of Human Facial Recession. A 12-Case Report. J. Periodontol. 1992, 63, 554–560. [Google Scholar] [CrossRef]
- Thurow, R.C. Atlas of Orthodontics Principles, 2nd ed.; Mosby: St. Louis, MI, USA, 1977. [Google Scholar]
- Maynard, J.G.; Ochsenbein, C. Mucogingival Problems, Prevalence and Therapy in Children. J. Periodontol. 1975, 46, 543–552. [Google Scholar] [CrossRef]
- Lang, N.P.; Löe, H. The Relationship Between the Width of Keratinized Gingiva and Gingival Health. J. Periodontol. 1972, 43, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Odenrick, L.; Modéer, T. Periodontal status following surgical-orthodontic alignment of impacted teeth. Acta Odontol. Scand. 1978, 36, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Heaney, T.G.; Atherton, J.D. Periodontal Problems Associated with the Surgical Exposure of Unerupted Teeth. Br. J. Orthod. 1976, 3, 79–85. [Google Scholar] [CrossRef]
- Modéer, T.; Odenrick, L. Post-treatment periodontal status of labially erupted maxillary canines. Acta Odontol. Scand. 1980, 38, 253–256. [Google Scholar] [CrossRef]
- Sullivan, H.C.; Atkins, J.H. Free autogenous gingival grafts. 3. Utilization of grafts in the treatment of gingival recession. Periodontics 1968, 6, 152–160. [Google Scholar]
- Liu, W.J.L.; Solt, C.W. A Surgical Procedure for the Treatment of Localized Gingival Recession in Conjunction with Root Surface Citric Acid Conditioning. J. Periodontol. 1980, 51, 505–509. [Google Scholar] [CrossRef]
- Benque, E.P.; Brunel, G.; Gineste, M.; Colin, L.; Duffort, J.; Fonvielle, E. Gingival Recession. Parodontol. J. 1984, 3, 207–241. [Google Scholar]
- Smith, R.G. Gingival recession Reappraisal of an enigmatic condition and a new index for monitoring. J. Clin. Periodontol. 1997, 24, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Pini-Prato, G.; Franceschi, D.; Cairo, F.; Nieri, M.; Rotundo, R. Classification of Dental Surface Defects in Areas of Gingival Recession. J. Periodontol. 2010, 81, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: An explorative and reliability study. J. Clin. Periodontol. 2011, 38, 661–666. [Google Scholar] [CrossRef]
- Mahajan, A. Mahajan’s Modification of the Miller’s Classification for Gingival Recession. Dent. Hypotheses 2010, 1, 45–50. [Google Scholar] [CrossRef]
- Armit, M.; Rosiline, J. Classification for Gingival Recession: A Mini review. Galore Int. J. Health Sci. Res. 2018, 3, 33–38. [Google Scholar]


{kind=link}
| Article | Author/Year/Country | Title | Objective | Study Design | Clinical Parameters Assessed |
|---|---|---|---|---|---|
| A1 [34] | Núñez et al., 2018/Spain | A two-step surgical approach with flattening of the root surface to treat localized gingival recessions affecting mandibular incisors: a case series report | To analyze the clinical outcome of the two-step procedure in patients with localized GR and prominent roots secondary to orthodontic therapy | Case series |
|
| A2 [35] | Gil et al., 2018/U.S.A. | Treatment of multiple recession defects with VISTA: a retrospective pilot study utilizing digital analysis | To examine the correlation between initial site-specific characteristics of patients with multiple GR defects and the outcome of RC therapy | Retrospective study |
|
| A3 [36] | Gil et al., 2019/U.S.A. | Three-dimensional volumetric analysis of multiple gingival recession defects treated by the VISTA procedure | To evaluate gingival volume changes following RC with the VISTA procedure | Retrospective study |
|
| Sample/Mean Age | Inclusion Criteria | Exclusion Criteria | Results | |
|---|---|---|---|---|
| A1 [34] |
|
|
|
|
| A2 [35] |
|
|
|
|
| A3 [36] |
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raso, G.; Santos, N.B.M.d.; Nassani, L.M.; Mello-Moura, A.C.V.; Fernandes, J.C.H.; Fernandes, G.V.O. The Influence of Root Prominence on the Onset of Gingival Recession: A Systematic Review. Surgeries 2024, 5, 103-114. https://doi.org/10.3390/surgeries5010012
Raso G, Santos NBMd, Nassani LM, Mello-Moura ACV, Fernandes JCH, Fernandes GVO. The Influence of Root Prominence on the Onset of Gingival Recession: A Systematic Review. Surgeries. 2024; 5(1):103-114. https://doi.org/10.3390/surgeries5010012
Chicago/Turabian StyleRaso, Girolamo, Nuno Bernardo Malta dos Santos, Leonardo M. Nassani, Anna Carolina Volpi Mello-Moura, Juliana Campos Hasse Fernandes, and Gustavo Vicentis Oliveira Fernandes. 2024. "The Influence of Root Prominence on the Onset of Gingival Recession: A Systematic Review" Surgeries 5, no. 1: 103-114. https://doi.org/10.3390/surgeries5010012