1. Introduction
According to the United Nations, the world population is aging [
1]. In 2020, approximately 728 million people were aged 65 years or older (9.3%), with the expectation that this number will grow, reaching roughly 1.5 billion (16%) by 2050. In the United States, where the elderly comprise 15% of the population, they alarmingly accounted for 35% of the laparotomies conducted [
2].
Prior studies had shown that the morbidity and mortality among this population are significantly higher [
2,
3,
4,
5], with a longer length of stay (LOS) at the hospital and in the intensive care unit (ICU) [
4]. Emergency laparotomy (EL) is a lifesaving procedure undertaken primarily in acute cases. EL is performed to address many different acute abdominal situations, and it is often performed in patients with sepsis or shock. According to the current literature, the 30-day mortality after EL is between 10 and 18% [
6]; however, in patients presenting with septic shock, it reaches 34.7% [
7].
Because each case presents with individualized difficulties, a wide array of outcomes can be present, including an increased risk of peri- or postoperative death, the development of postoperative complications, prolonged length of hospital stays, or an alternative discharge destination (rehabilitation/assisted leaving/skilled nursing home).
A report published by the Association of Surgeons of Great Britain and Ireland (ASGBI) in 2007 concluded that the customary care for emergency surgical admissions was substandard. Inadequate senior input, the poor use of resources, and being admitted under the wrong specialty were identified as key contributing factors to poor patient outcomes following laparotomy [
8].
The diversity between indications for surgery and patient characteristics likely significantly contributes to postoperative death and complications following EL [
8]. Accepted care bundles consisting of early identification of high-risk patients, early antibiotic administration, and early surgical intervention have been shown to improve outcomes, reducing mortality and morbidity by 53% after EL [
9].
A significant number of elderly patients with underestimated or under-recognized surgical pathologies are hospitalized in non-general surgery departments (internal medicine, geriatric, or medical intensive care units). A lack of immediate demanding intervention for patients who inherently possess an increased risk for surgical complications and mortality and are admitted to lower-acuity inpatient wards rather than a surgical service may be associated with a slower assessment, clinical deterioration, and worse patient outcomes. However, the evidence to support such a hypothesis for these associations is scarce [
8,
10]. This research aimed to evaluate the outcomes of elderly patients following EL in a tertiary referral center hospital and identify factors that may predict adverse outcomes in this vulnerable group. We hypothesized that under-prioritizing elderly patients with acute surgical pathologies for medical or non-general surgery services is associated with increased mortality and morbidity compared with patients admitted to a surgical facility.
2. Methods
2.1. Study Design and Population
A retrospective review of the charts of all patients aged 65 years and older who underwent EL in our institute between 1 January 2017 and 31 December 2019 was conducted. Our study was conducted under the supervision of the Hadassah Medical Center institutional review board. We excluded patients aged <65 years on the day of surgery and patients who underwent EL due to organ transplantation or its complications or had urological or gynecological emergencies. Additionally, we excluded those individuals who underwent an elective laparotomy or required any emergency general surgery that did not include a formal midline laparotomy (e.g., laparoscopic surgeries, groin herniorrhaphy).
The collected data included demographics, comorbidities, indications for emergency surgery, primary admitting departments, and surgical interventions (one-stage surgery or abbreviated laparotomy). Additional information regarding the length of hospital stay (LOS), the need for an intensive care unit (ICU), and the discharge destination was obtained and collated.
Patients were divided into two groups. Those admitted to the general surgery treating team, including both inpatient wards and surgical intensive care units, constituted the “Directly admitted to general surgery service” group. Patients taken to surgery from other hospital departments were included in the “Admitted to non-general surgery departments” group. Postoperatively, all patients were treated under the guidance and supervision of the general surgical team.
2.2. Data and Outcome Measures
The comorbidities evaluated were retrieved from patients’ charts and included previous abdominal surgery, smoking, diabetes mellitus (DM), ischemic heart disease (IHD), hypertension, congestive heart failure (CHF), chronic lung disease, active malignancy, obesity (BMI > 30), chronic renal failure (with or without dialysis), chronic immunosuppression, and peripheral vascular disease (PVD).
The primary outcome was survival and discharge home. Other discharge destinations, such as nursing homes, rehabilitation centers, and assisted living facilities (ALFs), did not qualify as returning home. All patients were followed up for at least 30 days following discharge.
The secondary outcomes measured were the rate of readmission (30 days after discharge from initial hospitalization), ICU admission and readmission, need for stoma formation, need for tracheostomy, and home parenteral nutritional support. Post-surgery complications such as surgical site infection (SSI), urinary tract infection (UTI), acute kidney injury (AKI), pneumonia, central line-associated bloodstream infection (CLABSI), intra-abdominal abscess, gastrointestinal bleeding (GIB), deep vein thrombosis (DVT), and pulmonary embolism (PE) were additionally included.
4. Results
4.1. Patients’ Characteristics and Surgery Indications
During the study period, EL was performed on 200 patients aged ≥65 and older. There were 106 (53%) male patients, and the mean age was 77 ± 8.3 years; 79 patients (40%) were octogenarians (≥80 years). Fifty-three patients (26.5%) underwent more than one abdominal surgery during their admission. Planned relaparotomy (open abdomen technique) was a standard for all patients with acute mesenteric ischemia (AMI); others required repeat laparotomies due to severe abdominal sepsis.
Sixty-nine patients (34.5%) were initially admitted to a non-general surgery department.
Table 1 presents the details of the patients’ demographics and comorbidities. The patients directly admitted to the general surgical department were slightly older than those admitted to non-general surgery departments and reported a higher rate of previous abdominal surgeries.
The most common indication for EL was bowel obstruction encompassing both large- and small-bowel obstructions, observed in 91 patients (45%); among them, 25 (27.5%) had bowel obstruction secondary to incarcerated hernias. Other frequent indications included acute mesenteric ischemia (AMI) in 33 cases (17%) and hollow viscus perforation in 44 patients (22%). The remaining 32 cases (“other”, 16%) involved indications like gastrointestinal bleeding, toxic colitis, volvulus, eventration, trauma, etc. Importantly, a greater number of patients who developed AMI and “other” abdominal emergencies were initially admitted to non-general surgery services (
Table 2).
4.2. Outcomes
Fifty-nine (29.5%) patients died during their hospitalization. Within the patients who were discharged, 110 (78%) were discharged home, and 31 (22%) were discharged to an assisted living facility (ALF). Of all discharged patients, 33 (23%) were readmitted to the hospital within 30 days of discharge. Eighty-two patients (41%) underwent ostomy creation. Notably, a substantial proportion of patients among those who underwent an EL required admission to the ICU (169, 85%). However, if the patient was initially admitted to a non-general surgery department, there was a significantly higher risk of ICU admission or readmission post initial transfer to the inpatient ward (p = 0.016 and p = 0.005, respectively).
A significantly greater number and proportion of patients who were admitted to a non-general surgery department (37, 53.6%) died during their admission when compared to the “directly admitted to general surgical service” group (22 patients, 16.8%, p= 0.0001).
Table 3 shows the patient outcomes in the two groups.
Patients initially admitted to a non-general surgery department had significantly worse overall outcomes, including higher mortality, requirement for multiple surgical interventions, and a higher rate of stoma formation (all p < 0.001).
Additionally, patients initially placed in a non-general surgery department were discharged with unfavorable discharge characteristics, including a higher rate of readmission, discharge to ALF, more frequent tracheostomies, and total parenteral nutrition (TPN) dependence (all <0.001).
Table 4 shows the pattern of complications in the two groups of the cohort. Patients admitted to any non-general surgery service presented with more infectious complications (pneumonia and CLABSI). Also, the postoperative AKI rate was higher in the “non-general surgery departments” group (all
p < 0.002).
4.3. Factors Associated with Survival and Favorable Discharge
In the univariable analysis, initial admission to a surgical department carried a higher probability of favorable discharge (OR 6.684, CI-3.472–12.867, p-value < 0.001) compared with patients who had EL directly from a non-general surgery department.
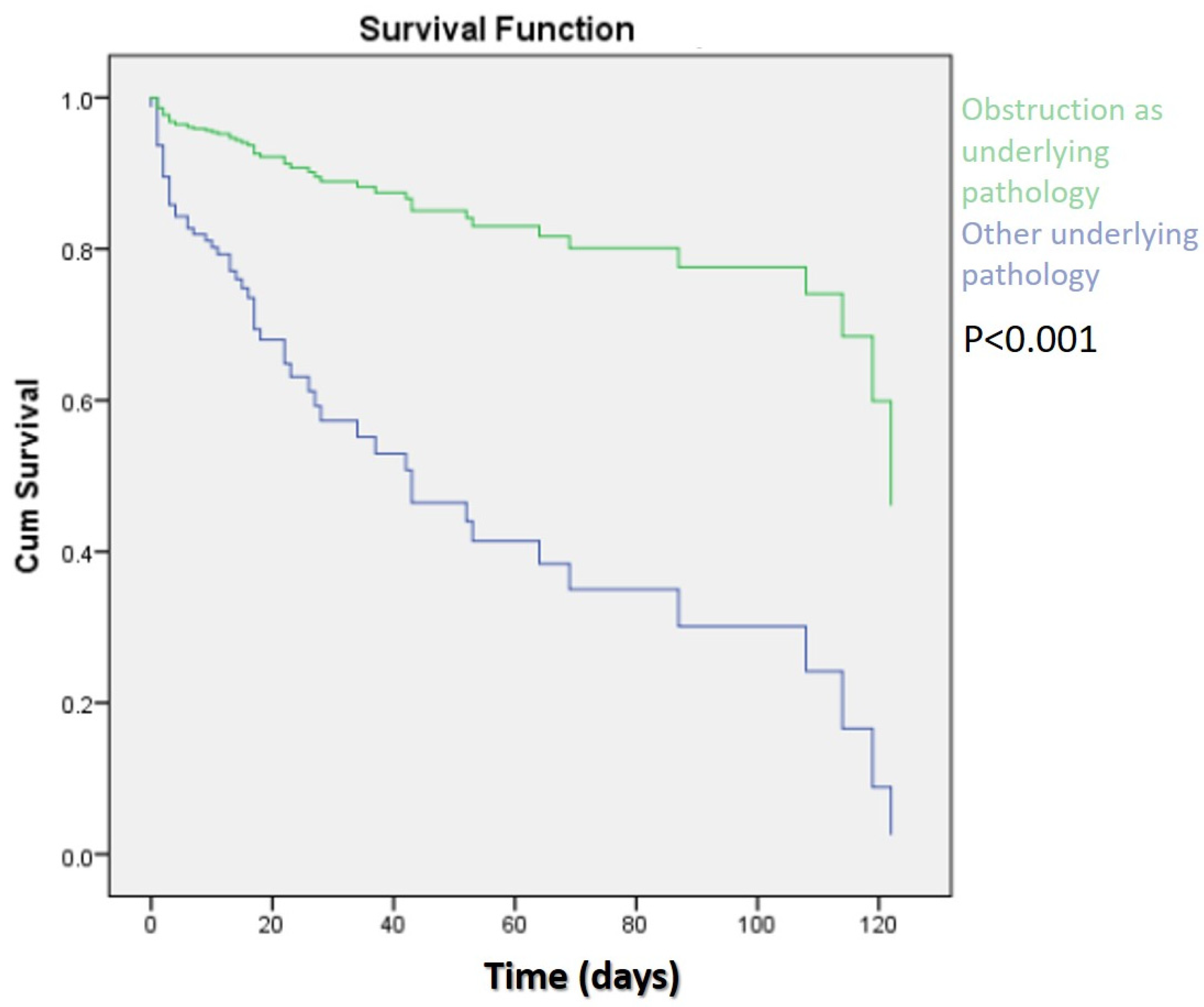
In the multivariant survival analysis, using the Cox regression model, we found the following negative predictors for survival: age ≥80 years old (HR-0.352, 95%CI: 0.204–0.608,
p < 0.001), heart failure (HR-0.530, 95%CI: 0.303–0.928,
p < 0.026), and dialysis (HR-0.263, 95%CI: 0.076–0.915,
p < 0.0.36). Bowel obstruction as an indication for surgery was a positive predictor of survival (HR-4.732, 95%CI: 2.009–10.664,
p < 0.001) (
Figure 1).
In a multivariate analysis using binary logistic regression models, positive predictors for discharge home were male gender (p = 0.03), bowel obstruction as an indication for surgery (p < 0.001), and patients initially treated by a surgeon (as opposed to patients admitted to a non-general surgery service) (p = 0.003).
Patients who underwent multiple surgical interventions during the same admission had a decreased probability of successful discharge home (OR 5.49, p-value < 0.001). This includes patients who underwent emergency repeat surgery to resolve complications after an initial elective or emergency abdominal surgery (general, urological, or gynecologic surgery) or those requiring an open abdomen after emergent surgical intervention with the intention of closure at a later date within the admission.
5. Discussion
The mortality rate for elderly individuals with emergency abdominal pathologies who require a laparotomy is elevated [
11]. This study emphasizes the importance of the appropriate placement of patients within emergency department triage and admission. It is also crucial for the referring specialist to identify and alert the surgical staff about patients with suspected surgical pathology immediately for continued management by the surgical team.
In this study, we found that elderly patients who were initially admitted to a non-general surgery department and eventually underwent emergency laparotomy had a higher mortality rate, a decreased likelihood of being discharged home, a higher rate of ICU readmission, a greater risk for repeated surgeries, a higher rate of new stoma, needs for permanent tracheostomy, and TPN dependence compared to patients who were admitted directly to a general surgery service. In our large tertiary referral center, the overall in-hospital mortality in elderly patients undergoing emergency laparotomies was roughly 30%. This reported statistic is higher than previously identified in similar studies and requires further evaluation. First, we included only patients with serious abdominal pathologies who required an emergency laparotomy (bowel obstruction, mesenteric events, and hollow viscus perforations) in an almost octogenarian group. Second, the patients in this study’s cohort suffered critical illnesses that required ICU admission in 85% of the cases. International studies report a 7–21% short-term mortality rate, a long overall stay in hospital, and a large number of ICU admissions for patients undergoing EL [
1,
6]. The short-term mortality for the cohort requiring ICU admission was 37.9% [
12], which is a closer representative sample to the current results [
8].
Age-related physiological changes, frailty, multiple coexisting morbidities, and polypharmacy may result in nonspecific and atypical symptom presentation [
13,
14], resulting in misdiagnosis and delayed treatment of emergent conditions. The correct diagnosis for abdominal pain in elderly emergency room patients was reported to be between 40 and 82% [
15]. Avelino-Silva and Steinman [
16] showed that diagnostic discrepancies between admission and discharge occurred in 12.5% of elderly patients (>65 years old) and were independently associated with longer lengths of stays and increased in-hospital mortality. Naouri et al. [
17] identified that 36.5% of elderly patients (≥75) were admitted from the emergency room to an inappropriate ward, and about 20% of patients of all ages with gastroenterological complaints were admitted from the emergency room to an inappropriate ward for treatment by staff without subspecialist training. The retrospective nature of the current research limited its ability to assess the misdiagnosis of patients as a cause for incorrect placement on admission to the hospital or if they developed a new abdominal pathology while undergoing treatment for a different medical condition. Of the current cohort, 34.5% of patients were initially admitted to an inappropriate floor.
The percentage of patients with chronic lung disease or chronic renal failure was higher in the group of patients admitted to a non-general surgery department, which may contribute to inappropriate admission (e.g., chronic confounding symptoms or concomitantly diagnosed conditions); however, there were no differences in other comorbidities that can mask abdominal pathology.
A feared consequence for patients admitted to a non-general surgery department is a longer interval from initial clinical presentation to surgical intervention. Previous research has examined the importance of delayed progression toward EL. Svenningsen et al. [
18] demonstrated that a delay in surgical treatment is not associated with a higher mortality rate. However, this study included young patients (median age 68 years, range 19–96). Similarly, Vester-Andersen et al. [
19] did not show a significant relationship between delayed surgical intervention and mortality in a large sample; notably, their study encompassed patients with a median age of 66, including younger individuals. Furthermore, in contrast to the current research, laparoscopic procedures were included in the analysis, which could have contributed to more favorable results. A high postoperative mortality rate of 55.2% was observed in patients who arrived at an operation after admission to a department other than general surgery. This statistic is consistent with Saunders et al. [
8], who showed significantly higher rates of mortality in patients admitted to a medical department rather than general surgery (in all age groups analysis). Additionally, Khalil et al. [
10] found a significantly higher mortality rate among patients admitted to a medical ward as opposed to a surgical ward in all age groups, as well as a reduction in the time from admission to progression to surgery when patients were admitted directly to surgery. Our findings strengthen the conclusions drawn in previous research and build on previous research by narrowing the population by age and exemplifying that the elderly population is particularly vulnerable to delayed progression to surgery. Some explanations for the positive findings in an exclusively elderly population include changes to physiology, multiple comorbidities, and a varied, non-“classic” presentation of symptoms resulting in misdiagnosis, incorrect placement at admission, and a delay in the appropriate treatment.
A delay in surgery had previously been shown to be related to complications and morbidity. In a study that included surgical specialties aside from general surgery, North et al. [
20] showed that delayed surgical treatment was associated with an increased risk of unplanned repeated surgery, ICU admission, and postoperative complications. Ong and his colleagues [
14] identified a higher complication rate in elderly patients (≥60) who required emergency abdominal surgery when surgery was delayed. Our study, in concordance with those results, showed that patients who were admitted under the direct supervision of the General Surgery department had a higher probability of favorable discharge, lower rates of complications such as pneumonia, gastrointestinal bleeding, and CLABSI, and fewer tracheostomies.
One potential cause of the delayed progression to surgery and incorrect placement of patients may be related to a lack of surgical consultations in the emergency room. Surgeons must change their mindset regarding emergent patients. These patients should be reviewed by a consultant surgeon and anesthetist at the earliest opportunity, and a decision regarding progression to surgery could be made based on the patient’s functional status, incorporating a preoperative plan such as increased hydration and early antibiotic treatment as well as a carefully detailed postoperative management plan including placement (ward, surgical high-dependency unit [HDU] or ICU), which can all be seen as important steps taken to reduce the aforementioned high mortality rate following EL. General surgeons undergo an extensive training program, which exposes them to a wide range of emergencies, making them skilled when identifying urgent surgical issues, which can reduce the time to operation and lead to better outcomes. In contrast, experienced internal medical practitioners may encounter fewer surgical emergencies and may not be as familiar with the critical aspect of rapidity of treatment in this patient group, which, as a result, may delay obtaining surgical treatment.
Bowel obstruction as the etiology for EL was found to be a positive predictor for both survival and favorable discharge. Roughly 90% of patients with bowel obstruction were managed immediately by the general surgical team, likely improving the time to progress to surgery even for those patients who had undergone a trial of conservative treatment, which has previously been shown to yield better outcomes [
10]. This observation may be related to the higher proportion of patients with previous abdominal surgeries managed by general surgeons, possibly indicating a higher index of suspicion and early surgical consultation for these patients. Male patients were more likely to be discharged home, which is in concordance with McCann [
21], who showed that in Ireland, female patients were more likely to be discharged to a nursing home rather than to their own homes.
Elderly patients at presentation to the emergency department present with “classic” symptomology or complaints less frequently and often present without objective findings either by physical exams or laboratory results (like fever, tachycardia, leukocytosis, etc.), clouding the physician’s judgment. This can be caused by physiology or masked by chronic medical conditions or medications [
13]. Therefore, a higher level of suspicion should be prioritized for elderly patients to exclude emergent pathology needing an early surgical consultation and high-quality radiological evaluation.
There is evidence that standardizing patient flow for emergency surgical pathology leads to better outcomes. In Denmark, a multidisciplinary perioperative care bundle has shown a significant reduction in 30-day mortality from 21.8% to 15.5% [
22]. This bundle consists of evidence-based elements, among which are key components of early evaluation of patients by experienced surgeons and anesthetists, a prompt abdominal CT, a short interval between the decision to operate and surgery, and planned postoperative intermediate care. A similar “bundle” approach has resulted in advantageous results in the UK [
9]. However, a care bundle addressing the specific problems in the elderly population has not yet been studied.
As we have already addressed, the influence on outcomes of a standardized pathway designed for elderly patients, consisting of early incorporation of a multi-disciplinary team including geriatric assessment, rapid surgical response, perioperative extensive resuscitation, and postoperative rehabilitation planning, should be investigated. Importantly, within this “care bundle”, there should also be a pathway to address limitations of care with an offer of palliation when surgical treatment is deemed ineffective. A bundle designed for elderly patients undergoing EL is currently being launched at our hospital, with data collection in progress.
Our study, however, has several limitations. Despite being conducted at a tertiary teaching hospital and including a large number of patients, its retrospective and single-center nature is associated with selection bias. Additionally, its retrospective nature limits our ability to estimate the interval between disease presentation and admission to the operating theater. Moreover, our data regarding non-general surgery admissions are limited, making it difficult to discern whether they resulted from misdiagnosis of abdominal pathology or incorrect placement on admission, or if the abdominal condition emerged while treating other medical issues.

 ,
, 

{kind=link}