
Ostomy Belt Use Improves Quality of Life in Patients with a Stoma

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
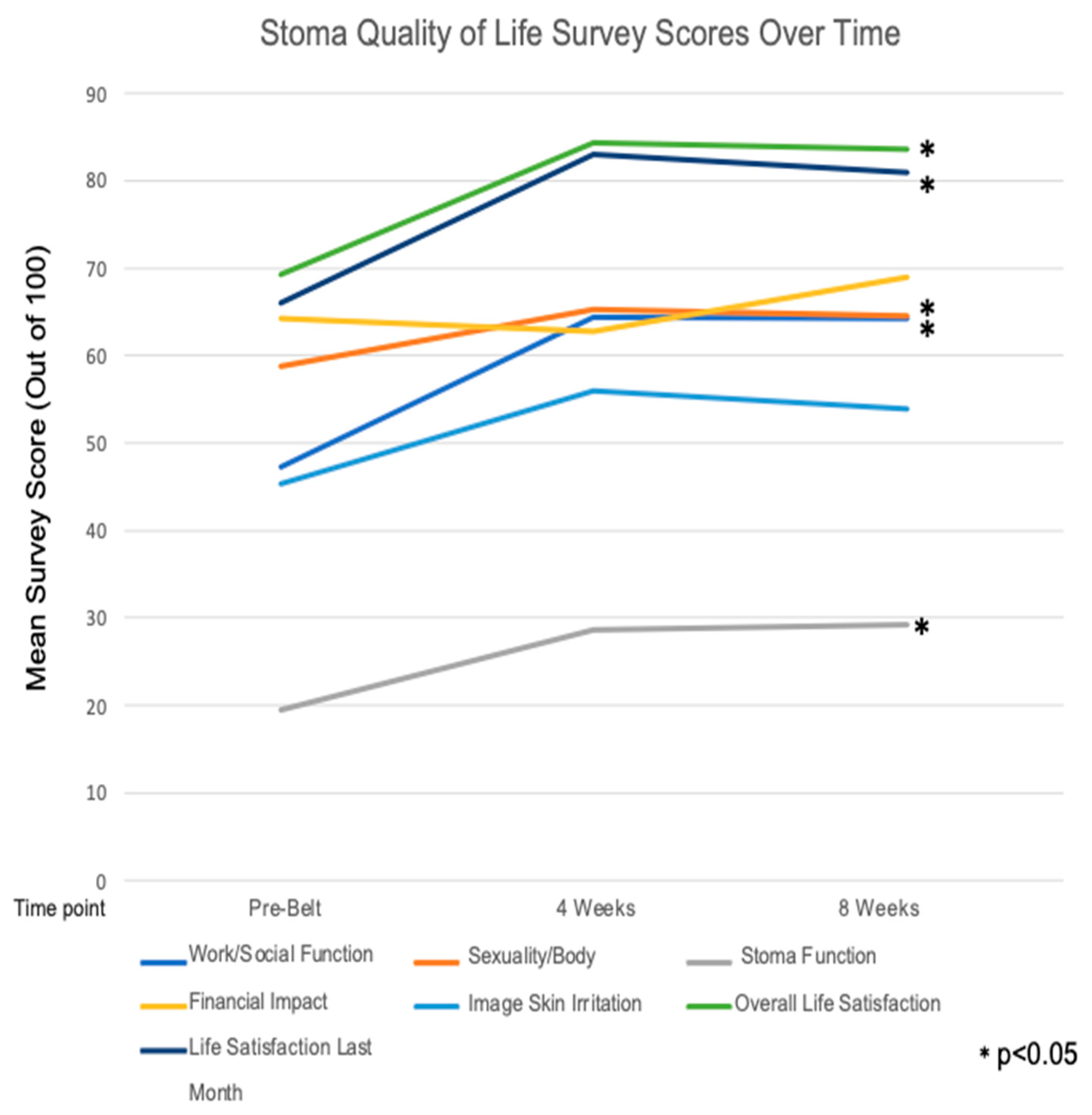
3.2. Ostomy Belt Survey Results over Time
3.3. Subgroup Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ambe, P.C.; Kurz, N.R.; Nitschke, C.; Odeh, S.F.; Möslein, G.; Zirngibl, H. Intestinal Ostomy. Dtsch. Arztebl. Int. 2018, 115, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Colwell, J.C.; Bain, K.A.; Hansen, A.S.; Droste, W.; Vendelbo, G.; James-Reid, S. International Consensus Results: Development of Practice Guidelines for Assessment of Peristomal Body and Stoma Profiles, Patient Engagement, and Patient Follow-up. J. Wound Ostomy Cont. Nurs. 2019, 46, 497–504. [Google Scholar] [CrossRef]
- Ang, S.G.; Chen, H.C.; Siah, R.J.; He, H.G.; Klainin-Yobas, P. Stressors relating to patient psychological health following stoma surgery: An integrated literature review. Oncol. Nurs. Forum 2013, 40, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Vonk-Klaassen, S.M.; de Vocht, H.M.; den Ouden, M.E.; Eddes, E.H.; Schuurmans, M.J. Ostomy-related problems and their impact on quality of life of colorectal cancer ostomates: A systematic review. Qual. Life Res. 2016, 25, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Schiergens, T.S.; Hoffmann, V.; Schobel, T.N.; Englert, G.H.; Kreis, M.E.; Thasler, W.E.; Werner, J.; Kasparek, M.S. Long-term Quality of Life of Patients With Permanent End Ileostomy: Results of a Nationwide Cross-Sectional Survey. Dis. Colon. Rectum 2017, 60, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Zewude, W.C.; Derese, T.; Suga, Y.; Teklewold, B. Quality of Life in Patients Living with Stoma. Ethiop. J. Health Sci. 2021, 31, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.L.; Augusto, F.S.; Gomboski, G. Health-Related Quality of Life in Persons with Ostomies Managed in an Outpatient Care Setting. J. Wound Ostomy Cont. Nurs. 2016, 43, 158–164. [Google Scholar] [CrossRef]
- Alenezi, A.; McGrath, I.; Kimpton, A.; Livesay, K. Quality of life among ostomy patients: A narrative literature review. J. Clin. Nurs. 2021, 30, 3111–3123. [Google Scholar] [CrossRef]
- Ayaz-Alkaya, S. Overview of psychosocial problems in individuals with stoma: A review of literature. Int. Wound J. 2019, 16, 243–249. [Google Scholar] [CrossRef]
- Cakir, S.K.; Ozbayir, T. The effect of preoperative stoma site marking on quality of life. Pak. J. Med. Sci. 2018, 34, 149–153. [Google Scholar] [CrossRef]
- Goldstine, J.; van Hees, R.; van de Vorst, D.; Skountrianos, G.; Nichols, T. Factors influencing health-related quality of life of those in the Netherlands living with an ostomy. Br. J. Nurs. 2019, 28, S10–S17. [Google Scholar] [CrossRef] [PubMed]
- Khalilzadeh Ganjalikhani, M.; Tirgari, B.; Roudi Rashtabadi, O.; Shahesmaeili, A. Studying the effect of structured ostomy care training on quality of life and anxiety of patients with permanent ostomy. Int. Wound J. 2019, 16, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Pittman, J.; Rawl, S.M.; Schmidt, C.M.; Grant, M.; Ko, C.Y.; Wendel, C.; Krouse, R.S. Demographic and clinical factors related to ostomy complications and quality of life in veterans with an ostomy. J. Wound Ostomy Cont. Nurs. 2008, 35, 493–503. [Google Scholar] [CrossRef]
- Chunli Liao, Y.Q. Factors associated with stoma quality of life among stoma patients. Int. J. Nurs. Sci. 2014, 1, 196–201. [Google Scholar] [CrossRef]
- Russell, S. Physical activity and exercise after stoma surgery: Overcoming the barriers. Br. J. Nurs. 2017, 26, S20–S26. [Google Scholar] [CrossRef] [PubMed]
- Eyl, R.E.; Koch-Gallenkamp, L.; Jansen, L.; Walter, V.; Carr, P.; Hoffmeister, M.; Chang-Claude, J.; Brenner, H.; Arndt, V. Potential determinants of physical inactivity among long-term colorectal cancer survivors. J. Cancer Surviv. 2018, 12, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Pittman, J.; Colwell, J.; Mulekar, M.S. Ostomy Complications and Quality of Life of Ostomy Support Belt/Garment Wearers: A Web-Based Survey. J. Wound Ostomy Cont. Nurs. 2022, 49, 60–68. [Google Scholar] [CrossRef]
- Baxter, N.N.; Novotny, P.J.; Jacobson, T.; Maidl, L.J.; Sloan, J.; Young-Fadok, T.M. A stoma quality of life scale. Dis. Colon. Rectum 2006, 49, 205–212. [Google Scholar] [CrossRef]
- Kuruvilla, K.; Osler, T.; Hyman, N.H. A comparison of the quality of life of ulcerative colitis patients after IPAA vs ileostomy. Dis. Colon. Rectum 2012, 55, 1131–1137. [Google Scholar] [CrossRef]
- Neuman, H.B.; Patil, S.; Fuzesi, S.; Wong, W.D.; Weiser, M.R.; Guillem, J.G.; Paty, P.B.; Nash, G.M.; Temple, L.K. Impact of a temporary stoma on the quality of life of rectal cancer patients undergoing treatment. Ann. Surg. Oncol. 2011, 18, 1397–1403. [Google Scholar] [CrossRef]
- Knowles, S.R.; Wilson, J.; Wilkinson, A.; Connell, W.; Salzberg, M.; Castle, D.; Desmond, P.; Kamm, M.A. Psychological well-being and quality of life in Crohn’s disease patients with an ostomy: A preliminary investigation. J. Wound Ostomy Cont. Nurs. 2013, 40, 623–629. [Google Scholar] [CrossRef]
- Kittscha, J.; Fairbrother, G.; Bliokas, V.; Wilson, V. Adjustment to an Ostomy: An Integrative Literature Review. J. Wound Ostomy Cont. Nurs. 2022, 49, 439–448. [Google Scholar] [CrossRef]
- de Gouveia Santos, V.L.; Chaves, E.C.; Kimura, M. Quality of life and coping of persons with temporary and permanent stomas. J. Wound Ostomy Cont. Nurs. 2006, 33, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Whiteley, I.; Randall, S.; Stanaway, F.F. Comparison of Adjustment or Adaptation to the Formation of a Temporary versus a Permanent Ostomy: A Systematic Review. J. Wound Ostomy Cont. Nurs. 2024, 51, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Annells, M. The experience of flatus incontinence from a bowel ostomy: A hermeneutic phenomenology. J. Wound Ostomy Cont. Nurs. 2006, 33, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Sun, V.; Grant, M.; McMullen, C.K.; Altschuler, A.; Mohler, M.J.; Hornbrook, M.C.; Herrinton, L.J.; Baldwin, C.M.; Krouse, R.S. Surviving colorectal cancer: Long-term, persistent ostomy-specific concerns and adaptations. J. Wound Ostomy Cont. Nurs. 2013, 40, 61–72. [Google Scholar] [CrossRef]
- Torquato Lopes, A.P.; Decesaro, M. The adjustments experienced by persons with an ostomy: An integrative review of the literature. Ostomy Wound Manag. 2014, 60, 34–42. [Google Scholar]
- Manderson, L. Boundary breaches: The body, sex and sexuality after stoma surgery. Soc. Sci. Med. 2005, 61, 405–415. [Google Scholar] [CrossRef]
- Mishra, S.I.; Scherer, R.W.; Snyder, C.; Geigle, P.M.; Berlanstein, D.R.; Topaloglu, O. Exercise interventions on health-related quality of life for people with cancer during active treatment. Cochrane Database Syst. Rev. 2012, 2012, Cd008465. [Google Scholar] [CrossRef]
- Packer, N.; Hoffman-Goetz, L.; Ward, G. Does physical activity affect quality of life, disease symptoms and immune measures in patients with inflammatory bowel disease? A systematic review. J. Sports Med. Phys. Fit. 2010, 50, 1–18. [Google Scholar]
- Park, J.; Rivard, S.J.; Maguire, L.; Varlamos, C.; Duby, A.; Hendren, S. Parastomal Hernia Rates and Exercise after Ostomy Surgery. Dis. Colon. Rectum 2023, 66, 823–830. [Google Scholar] [CrossRef]
- Richbourg, L.; Thorpe, J.M.; Rapp, C.G. Difficulties experienced by the ostomate after hospital discharge. J. Wound Ostomy Cont. Nurs. 2007, 34, 70–79. [Google Scholar] [CrossRef]
- Salvadalena, G.D. The incidence of stoma and peristomal complications during the first 3 months after ostomy creation. J. Wound Ostomy Cont. Nurs. 2013, 40, 400–406. [Google Scholar] [CrossRef]
- Hoeflok, J. Ostomy Belts. Available online: https://badgut.org/information-centre/ostomies/ostomy-belts/ (accessed on 6 September 2023).




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD) | N (%) | |
|---|---|---|---|
| Age (years) | 48 (10) | ||
| Sex | |||
| Female | 20 (40.0) | ||
| Male | 25 (50.0) | ||
| Missing | 5 (10.0) | ||
| Language | |||
| English | 45 (90.0) | ||
| Spanish | 5 (10.0) | ||
| Highest Attained Educational Level | |||
| Completed High School | 14 (28.0) | ||
| Doctorate | 3 (6.0) | ||
| Master’s | 4 (8.0) | ||
| Some High School | 2 (4.0) | ||
| Undergraduate | 22 (44.0) | ||
| Missing | 5 (10.0) | ||
| Waist Circumference (Inches) | 38 (5) | ||
| Body Mass Index | 25 (5) | ||
| Ostomy Type | |||
| Colostomy | 21 (42.0) | ||
| Ileostomy | 24 (48.0) | ||
| Missing | 5 (10.0) | ||
| Temporary vs. Permanent Ostomy | |||
| Temporary | 28 (56.0) | ||
| Permanent | 12 (24.0) | ||
| Missing | 10 (20.0) | ||
| Underlying Illness | |||
| Inflammatory Bowel Disease | 11 (25.0) | ||
| Colorectal or other GI Malignancy | 22 (50.0) | ||
| Non-GI Malignancy | 9 (20.5) | ||
| Other | 2 (4.5) | ||
| Time from Surgery | |||
| <1 month | 15 (33.3) | ||
| 1–3 months | 21 (46.7) | ||
| >3 months | 9 (20.0) | ||
| Time Point | |||||
|---|---|---|---|---|---|
| Measure | Pre-Belt | 4 Weeks | 8 Weeks | Test Statistic | p-Value |
| Mean (SD) | Mean (SD) | Mean (SD) | |||
| Work/Social Function | 47.19 (3.10) | 64.41 (3.41) | 64.19 (3.79) | F(2, 72) = 30.321 | <0.001 |
| Sexuality and Body Image | 58.71 (3.13) | 65.29 (3.20) | 64.57 (3.36) | F(2, 68) = 3.336 | 0.041 |
| Stoma Function | 19.48 (3.25) | 28.60 (2.88) | 29.28 (2.80) | F(2, 72) = 8.717 | <0.001 |
| Financial Impact | 64.19 (6.32) | 62.84 (6.25) | 68.92 (5.43) | F(2, 72) = 0.517 | 0.599 |
| Skin Irritation | 45.40 (4.89) | 55.92 (4.37) | 53.95 (4.38) | F(2, 74) = 2.366 | 0.101 |
| Life Satisfaction (Overall) | 69.21 (3.34) | 84.28 (2.84) | 83.67 (2.68) | F(2, 76) = 14.772 | <0.001 |
| Life Satisfaction (Last Month) | 66.05 (3.88) | 83.00 (3.33) | 80.90 (3.43) | F(2, 76) = 10.295 | <0.001 |
| Ostomy Permanence | |||||
|---|---|---|---|---|---|
| Time Point | Temporary | Permanent | Test Statistic | p-Value | |
| Mean (SD) | Mean (SD) | ||||
| Pre-Belt | Life Satisfaction (Overall) | 67 (23) | 72 (16) | t(38) = −0.618 | 0.541 |
| Life Satisfaction (Last Month) | 63 (26) | 72 (17) | t(38) = −1.125 | 0.268 | |
| Work | 46 (19) | 51 (18) | t(38) = −0.901 | 0.373 | |
| Sexuality and Body Image | 55 (18) | 64 (18) | t(37) = −1.440 | 0.158 | |
| Stoma Function | 16 (21) | 25 (15) | t(38) = −1.445 | 0.157 | |
| Financial | 65 (37) | 54 (37) | t(38) = 0.857 | 0.397 | |
| Skin Irritation | 50 (35) | 46 (26) | t(38) = 0.373 | 0.711 | |
| 4 Weeks | Life Satisfaction (Overall) | 81 (20) | 92 (09) | t(37) = −2.394 | 0.022 * |
| Life Satisfaction (Last Month) | 78 (24) | 93 (09) | t(37) = −2.893 | 0.006 * | |
| Work | 60 (20) | 75 (19) | t(35) = −2.046 | 0.048 * | |
| Sexuality and Body Image | 61 (18) | 74 (17) | t(34) = −1.905 | 0.065 | |
| Stoma Function | 26 (17) | 35 (17) | t(35) = −1.461 | 0.153 | |
| Financial | 63 (39) | 57 (36) | t(35) = 0.487 | 0.629 | |
| Skin Irritation | 57 (26) | 57 (30) | t(36) = 0.061 | 0.952 | |
| 8 Weeks | Life Satisfaction (Overall) | 79 (18) | 93 (10) | t(37) = −2.547 | 0.015 * |
| Life Satisfaction (Last Month) | 74 (24) | 94 (09) | t(36) = −3.677 | <0.001 * | |
| Work | 58 (22) | 80 (20) | t(37) = −2.896 | 0.006 * | |
| Sexuality and Body Image | 59 (18) | 75 (19) | t(37) = −2.594 | 0.014 * | |
| Stoma Function | 24 (15) | 42 (16) | t(37) = −3.383 | 0.002 * | |
| Financial | 69 (34) | 77 (29) | t(37) = −0.750 | 0.458 | |
| Skin Irritation | 53 (30) | 63 (20) | t(37) = −1.009 | 0.320 | |
| Ostomy Type | |||||
|---|---|---|---|---|---|
| Time Point | Ileostomy | Colostomy | Test Statistic | p-Value | |
| Mean (SD) | Mean (SD) | ||||
| Pre-Belt | Life Satisfaction (Overall) | 66 (21) | 65 (23) | t(43) = −0.123 | 0.902 |
| Life Satisfaction (Last Month) | 63 (24) | 64 (25) | t(43) = 0.145 | 0.885 | |
| Work/Social Function | 48 (22) | 47 (17) | t(43) = −0.091 | 0.928 | |
| Sexuality and Body Image | 58 (21) | 56 (14) | t(39) = −0.503 | 0.618 | |
| Stoma Function | 21 (17) | 19 (23) | t(36) = −0.266 | 0.791 | |
| Financial Impact | 78 (30) | 52 (40) | t(36) = −2.411 | 0.021 * | |
| Skin Irritation | 41 (26) | 57 (33) | t(43) = 1.873 | 0.068 | |
| 4 Weeks | Life Satisfaction (Overall) | 81 (18) | 87 (17) | t(38) = 1.184 | 0.244 |
| Life Satisfaction (Last Month) | 79 (22) | 85 (21) | t(38) = 0.917 | 0.365 | |
| Work/Social Function | 64 (22) | 65 (19) | t(36) = 0.129 | 0.898 | |
| Sexuality and Body Image | 63 (22) | 66 (15) | t(33) = 0.428 | 0.671 | |
| Stoma Function | 30 (18) | 29 (15) | t(36) = −0.240 | 0.812 | |
| Financial Impact | 68 (36) | 60 (40) | t(36) = −0.625 | 0.536 | |
| Skin Irritation | 50 (30) | 66 (21) | t(37) = 1.886 | 0.067 | |
| 8 Weeks | Life Satisfaction (Overall) | 82 (19) | 85 (17) | t(35) = 0.447 | 0.657 |
| Life Satisfaction (Last Month) | 77 (26) | 85 (18) | t(35) = 1.047 | 0.302 | |
| Work/Social Function | 64 (25) | 67 (21) | t(35) = 0.433 | 0.668 | |
| Sexuality and Body Image | 63 (21) | 64 (19) | t(35) = 0.236 | 0.815 | |
| Stoma Function | 29 (18) | 29 (17) | t(35) = 0.080 | 0.937 | |
| Financial Impact | 70 (32) | 68 (35) | t(35) = −0.153 | 0.880 | |
| Skin Irritation | 45 (32) | 65 (19) | t(30) = 2.383 | 0.024 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karhu, E.K.; Hernandez, A.E.; Restrepo, A.M.; Hui, V.W. Ostomy Belt Use Improves Quality of Life in Patients with a Stoma. Surgeries 2024, 5, 92-102. https://doi.org/10.3390/surgeries5010011
Karhu EK, Hernandez AE, Restrepo AM, Hui VW. Ostomy Belt Use Improves Quality of Life in Patients with a Stoma. Surgeries. 2024; 5(1):92-102. https://doi.org/10.3390/surgeries5010011
Chicago/Turabian StyleKarhu, Elisa K., Alexandra E. Hernandez, Ana M. Restrepo, and Vanessa W. Hui. 2024. "Ostomy Belt Use Improves Quality of Life in Patients with a Stoma" Surgeries 5, no. 1: 92-102. https://doi.org/10.3390/surgeries5010011