
Primary Occlusion of the Fourth Ventricle: Case Report and Review of the Literature
 ,
,
Abstract
:1. Introduction
Case Report
2. Materials and Methods
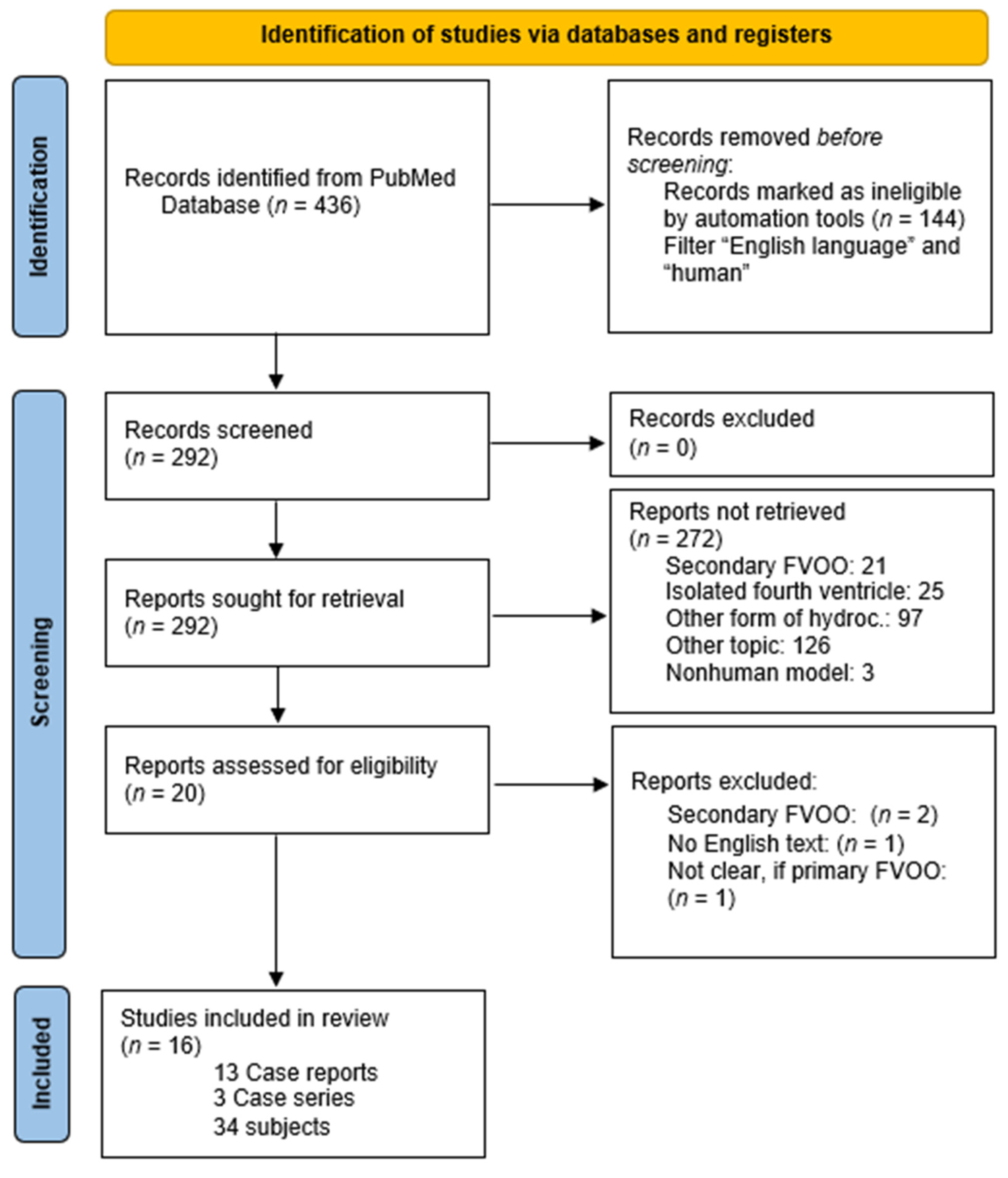
Search Strategy and Article Selection
3. Results
3.1. Clinical Features
3.2. Treatments
4. Discussion
4.1. Symptoms
4.2. Diagnostic
4.3. Therapy
4.3.1. ETV
4.3.2. Open, Suboccipital Approach
4.3.3. Endoscopic Transaqueductal Approach
4.3.4. Shunting Procedures
4.4. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohanty, A.; Biswas, A.; Satish, S.; Praharaj, S.S.; Sastry, K.V.R. Treatment options for Dandy-Walker malformation. J. Neurosurg. 2006, 105, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Calabro, F.; Arcuri, T.; Jinkins, J.R. Blake’s pouch cyst: An entity within the Dandy-Walker continuum. Neuroradiology 2000, 42, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, H.; Maeda, A.; Kumano, K.; Kimoto, T.; Fujisawa, Y.; Akai, T. Rapid deterioration of primary fourth ventricular outlet obstruction resulting in syndrome of inappropriate antidiuretic hormone secretion. Pediatr. Int. 2014, 56, e30–e32. [Google Scholar] [CrossRef]
- ELLIOTT, G.B.; WOLLIN, D.W. Defect of the corpus callosum and congenital occlusion of fourth ventricle with tuberous sclerosis. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1961, 85, 701–705. [Google Scholar] [PubMed]
- Torres-Corzo, J.; Sanchez-Rodriguez, J.; Cervantes, D.; Rodriguez-Della Vecchia, R.; Muruato-Araiza, F.; Hwang, S.W.; Rangel-Castilla, L. Endoscopic transventricular transaqueductal Magendie and Luschka foraminoplasty for hydrocephalus. Neurosurgery 2014, 74, 426–435; discussion 436. [Google Scholar] [CrossRef] [PubMed]
- Roth, J.; Ben-Sira, L.; Udayakumaran, S.; Constantini, S. Contrast ventriculo-cisternography: An auxiliary test for suspected fourth ventricular outlet obstruction. Childs. Nerv. Syst. 2012, 28, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Marin-Sanabria, E.A.; Yamamoto, H.; Nagashima, T.; Kohmura, E. Evaluation of the management of arachnoid cyst of the posterior fossa in pediatric population: Experience over 27 years. Childs. Nerv. Syst. 2007, 23, 535–542. [Google Scholar] [CrossRef]
- Cornips, E.M.J.; Overvliet, G.M.; Weber, J.W.; Postma, A.A.; Hoeberigs, C.M.; Baldewijns, M.M.L.L.; Vles, J.S.H. The clinical spectrum of Blake’s pouch cyst: Report of six illustrative cases. Childs. Nerv. Syst. 2010, 26, 1057–1064. [Google Scholar] [CrossRef]
- Spennato, P.; Sacco, M.; Cinalli, G. Diverticular Enlargement of Foramen of Luschka and Hydrocephalus in Child with Noonan Syndrome. World Neurosurg. 2019, 125, 371–373. [Google Scholar] [CrossRef]
- BARR, M.L. Observations on the foramen of Magendie in a series of human brains. Brain 1948, 71, 281–289. [Google Scholar] [CrossRef]
- Carpentier, A.; Brunelle, F.; Philippon, J.; Clemenceau, S. Obstruction of Magendie’s and Luschka’s foramina. Cine-MRI, aetiology and pathogenesis. Acta Neurochir. 2001, 143, 517–521; discussion 521–522. [Google Scholar] [CrossRef]
- Longatti, P.; Fiorindi, A.; Martinuzzi, A.; Feletti, A. Primary obstruction of the fourth ventricle outlets: Neuroendoscopic approach and anatomic description. Neurosurgery 2009, 65, 1078–1085; discussion 1085–1086. [Google Scholar] [CrossRef]
- Rifkinson-Mann, S.; Sachdev, V.P.; Huang, Y.P. Congenital fourth ventricular midline outlet obstruction. J. Neurosurg. 1987, 67, 595–599. [Google Scholar] [CrossRef]
- Barany, L.; Baksa, G.; Patonay, L.; Racz, G.; Ganslandt, O.; Buchfelder, M.; Kurucz, P. Primary Obstruction of the Foramen of Luschka: Anatomy, Histology, and Clinical Significance. World Neurosurg. 2018, 112, e288–e297. [Google Scholar] [CrossRef]
- Holland, H.C.; Graham, W.L.; Holland, C.H.C.; Graham, C.W.L.; Barany, L.; Baksa, G.; Patonay, L.; Racz, G.; Ganslandt, O.; Buchfelder, M.; et al. Congenital atresia of the foramina of Luschka and Magendie with hydrocephalus; report of a case in an adult. J. Neurosurg. 1958, 15, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Longatti, P.; Fiorindi, A.; Feletti, A.; Baratto, V. Endoscopic opening of the foramen of magendie using transaqueductal navigation for membrane obstruction of the fourth ventricle outlets. J. Neurosurg. 2006, 105, 924–927. [Google Scholar] [CrossRef] [PubMed]
- Suehiro, T.; Inamura, T.; Natori, Y.; Sasaki, M.; Fukui, M. Successful neuroendoscopic third ventriculostomy for hydrocephalus and syringomyelia associated with fourth ventricle outlet obstruction. J. Neurosurg. 2000, 93, 326–329. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Huang, Y.C.; Chang, C.N.; Chuang, H.L.; Scott, R.M. Membranous obstruction of the fourth ventricle outlet. Pediatr. Neurosurg. 2001, 35, 43–47. [Google Scholar] [CrossRef]
- Ishi, Y.; Asaoka, K.; Kobayashi, H.; Motegi, H.; Sugiyama, T.; Yokoyama, Y.; Echizenya, S.; Itamoto, K. Idiopathic fourth ventricle outlet obstruction successfully treated by endoscopic third ventriculostomy: A case report. Springerplus 2015, 4, 565. [Google Scholar] [CrossRef]
- Karachi, C.; Le Guerinel, C.; Brugieres, P.; Melon, E.; Decq, P. Hydrocephalus due to idiopathic stenosis of the foramina of Magendie and Luschka. J. Neurosurg. 2003, 98, 897–902. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Fujimura, M.; Tominaga, T. Syringomyelia with obstructive hydrocephalus at the foramens of Luschka and Magendie successfully treated by endoscopic third ventriculostomy. Surg. Neurol. 2009, 71, 349–352; discussion 352. [Google Scholar] [CrossRef] [PubMed]
- Rougier, A.; Menegon, P. MRI evidence of membranous occlusion of the foramen of Magendie. Acta Neurochir. 2009, 151, 693–694. [Google Scholar] [CrossRef]
- Shimoda, Y.; Murakami, K.; Narita, N.; Tominaga, T. Fourth Ventricle Outlet Obstruction with Expanding Space on the Surface of Cerebellum. World Neurosurg. 2017, 100, 711.e1–711.e5. [Google Scholar] [CrossRef]
- Giannetti, A.V.; Malheiros, J.A.; Da Silva, M.C. Fourth ventriculostomy: An alternative treatment for hydrocephalus due to atresia of the Magendie and Luschka foramina. J. Neurosurg. Pediatr. 2011, 7, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Duran, D.; Hadzipasic, M.; Kahle, K.T. Mystery Case: Acute hydrocephalus caused by radiographically occult fourth ventricular outlet obstruction. Neurology 2017, 88, e36–e37. [Google Scholar] [CrossRef]
- Tyagi, G.; Bhat, D.I.; Devi, B.I.; Shukla, D. Multiple Remote Sequential Supratentorial Epidural Hematomas-An Unusual and Rare Complication After Posterior Fossa Surgery. World Neurosurg. 2019, 128, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Yu, Q.; Sun, X.; Xiao, H.; Wang, K.; Sun, F.; Sui, Q. Hydrocephalus Due to Idiopathic Fourth Ventricle Outflow Obstruction. J. Craniofac. Surg. 2019, 30, e397–e400. [Google Scholar] [CrossRef]
- Krejčí, O.; Krejčí, T.; Mrůzek, M.; Večeřa, Z.; Šalounová, D.; Lipina, R. Hydrocephalus Caused by Primary Fourth Ventricle Outlet Obstruction: Our Experience and Literature Review. World Neurosurg. 2021, 148, e425–e435. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Case No. | Author | Sex/Age | Presentation | Treatment | Follow-Up | Outcome |
|---|---|---|---|---|---|---|
| 1 | Suehiro et al., 2000 [17] | f/27 years | Dizziness, headache, nausea, syringomyelia | ETV | Not reported | All symptoms resolved completely |
| 2 | Huang et al., 2001 [19] | f/15 years | Amenhorrhea, headache, nausea, vomiting | Suboccipital craniotomy, C1 laminectomy, splitting of vermis, removal of membrane | 14 months | All symptoms resolved completely |
| 3 | Carpentier et al., 2001 [11] | f/58 years | Headache, nausea, vomiting, instability (frequent falls), cerebellar ataxia, pseudo-vertebrobasilar insufficiency, blindness with head rotation (maybe due to compression of VA in foramen magnum) | ETV | 36 months | All symptoms resolved completely |
| 4 | Longatti et al., 2006 [16] | f/64 years | Cervical spine pain, nighttime headache, disturbed gait, dizziness, cerebellar ataxia | Transaqueductal Magendieplasty (ETV scheduled, not performed, since basilar tip left no space for stoma) | At least 4 months | All symptoms resolved completely |
| 5 | Rougier et al., 2009 [23] | m/60 years | Headache, unsteady gait | Suboccipital approach, fenestration of membrane | At least 6 months | All symptoms resolved completely |
| 6 | Kawaguchi et al., 2009 [22] | m/55 years | Syrinx, sensory disturbance, discrete movement disturbance of bilateral upper limb, dysuria, spine deformity, hyperreflection of upper limbs, hyorreflection of lower limbs, rectovesical dysfunction | ETV | Not reported | Some symptoms resolved completely |
| 7 | Giannetti et al., 2011 [25] | f/8 years | Headache, vomiting, decreased alertness, gait ataxia | Suboccipital endoscopic opening of the membranes | 36 months | Some symptoms resolved completely |
| 8 | Hashimoto et al., 2014 [3] | m/20 months | SIADH, vomiting | EVD, later ETV | Not reported | All symptoms resolved completely |
| 9 | Ishi et al., 2015 [20] | m/3 years | Headache, vomiting | EVD, 2 days later ETV Transaqueductal endoscpic exploration of fourth ventricle | 20 months after second ETV | All symptoms resolved completely |
| 10 | Shimoda et al., 2017 [24] | f/66 years | First admission: gait disturbance, wide based gate, cerebellar ataxia, dizziness, nausea, incontinence Second admission: disturbed balance, drowsiness | First admission: VPS (fourth ventricle enlargement 9 months after shunting), Second admission: ETV | Not reported | Improvement of symptoms |
| 11 | Duran et al., 2017 [26] | f/19 | Diplopia, headache, papilledema, abducens nerve palsy | Suboccipital craniotomy, later ventriculo-peritoneal shunting | Not reported | Some symptoms (diplopia) resoled after suboccipital craniotomy, all symptoms resolves after shunting, |
| 12 | Tyagi et al., 2019 [27] | m/22 | Headache, vomiting, truncal ataxia, papilledema, gaze-evoked nystagmus, dysarthria | Posterior fossa decompression, magendieplasty | Epidural hematoma, serial surgical evacuation | |
| 13 | Bai et al., 2019 [28] | 15 | Headache, vomiting | Suboccipital craniotomy, resection of membrane | 12 months | Improvement of symptoms |
| Case No. | Author | Sex/Age | Presentation | Treatment | Follow-Up | Outcome (Clinic) |
|---|---|---|---|---|---|---|
| 14–16 | Karachi et al., 2003 [21] | 14: 21/f 15: 53/f 16: 68/m | 14: headache, projectile vomiting, bilateral papilledema, 15: vertigo, positional nausea, slight postural instability 16: gait disorders, sphincter disorders, disorders of higher functions, stepping gait, postural instability, urinary incontinence, frontal syndrome | 14: ETV 15: ETV 16: ETV | 14: 26 months 15: 24 months 16: 58 months | 14–16: all symptoms resolved completely |
| 17–26 | Longatti et al., 2009 [12] | 17: m/53 18: f/49 19: m/70 20: m/73 21: m/64 22: m/36 23: m/65 24: m/69 25: m/69 26: m/58 | 17: ideomotor slowdown, gait difficulties, depression 18: dizziness, gait difficulties, memory impairment 19: gait difficulties, ideomotor slowdown, incontinence 20: gait difficulties, ideomotor slowdown, memory impairment 21: gait difficulties, incontinence 22: dizziness, visusal impairment, headache, vomiting 23: cervical pain, headache, gait difficulties, dizziness, nausea, vomiting 24: gait difficulties, memory impairment 25: gait difficulties, incontinence, memory impairment 26: gait difficulties | 17–22, 24–26: ETV, all transaqueductal exploration 20: additional aqueductoplasty 23: magendieplasty | 17: 12 years 18: 7 years 19: 6 years 20: 6 years 21: lost to follow up 22: 2 months, lost to follow up 23: 34 months 24: 15 months 25: 5 months 26: 3 months | 23: all symptoms resolved completely 17–22, 24–26: improvement of symptoms |
| 27–34 | Krejci et al., 2021 [29] | 27: 22/f 28: 74/f 29: 54/f 30: 22/f 31: 33/m 32: 44/m 33: 30/m 34: 28/f | 27: headache, vertigo, gait disturbance, diplopia, 28: headache, Hakim triad, vomiting, 29: Hakim triad, 30: headache, vomiting, gait disturbance, 31: headache, intracranial hypertension, diplopia, vomiting, vertigo, papilledema, cognitive impairment 32: headache, vertigo 33: headache, vomiting 34: headache, vomiting, vertigo, papilledema | 27: ETV 28: ETV 29: ETV 30: ETV 31: craniotomy 32: craniotomy 33: ventricular drainage 34: ETV | 27: 132 months 28: 84 months 29: 24 months 30: 48 months 31: 125 months 32: 108 months 33: - 34: 7 months | 27: all symptoms resolved completely 28: all symptoms resolved completely 29: improvement of symptoms (later VP shunt) 30: all symptoms resolved completely 31: all symptoms resolved completely 32: all symptoms resolved completely 33: death before treatment 34: improvement of symptoms (after re-ETV) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilbers, E.; Zawy Alsofy, S.; Schipmann, S.; Ewelt, C.; Fortmann, T.; Lewitz, M.; Schwake, M. Primary Occlusion of the Fourth Ventricle: Case Report and Review of the Literature. Surgeries 2023, 4, 665-677. https://doi.org/10.3390/surgeries4040063
Wilbers E, Zawy Alsofy S, Schipmann S, Ewelt C, Fortmann T, Lewitz M, Schwake M. Primary Occlusion of the Fourth Ventricle: Case Report and Review of the Literature. Surgeries. 2023; 4(4):665-677. https://doi.org/10.3390/surgeries4040063
Chicago/Turabian StyleWilbers, Eike, Samer Zawy Alsofy, Stephanie Schipmann, Christian Ewelt, Thomas Fortmann, Marc Lewitz, and Michael Schwake. 2023. "Primary Occlusion of the Fourth Ventricle: Case Report and Review of the Literature" Surgeries 4, no. 4: 665-677. https://doi.org/10.3390/surgeries4040063