
“I Wouldn’t Even Know What to Ask for”: Patients’ and Caregivers’ Experiences of Psychological Support for Huntington’s Disease in Italy

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodological Approach
2.2. Sampling and Recruitment
2.3. Participants
2.4. Procedure
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
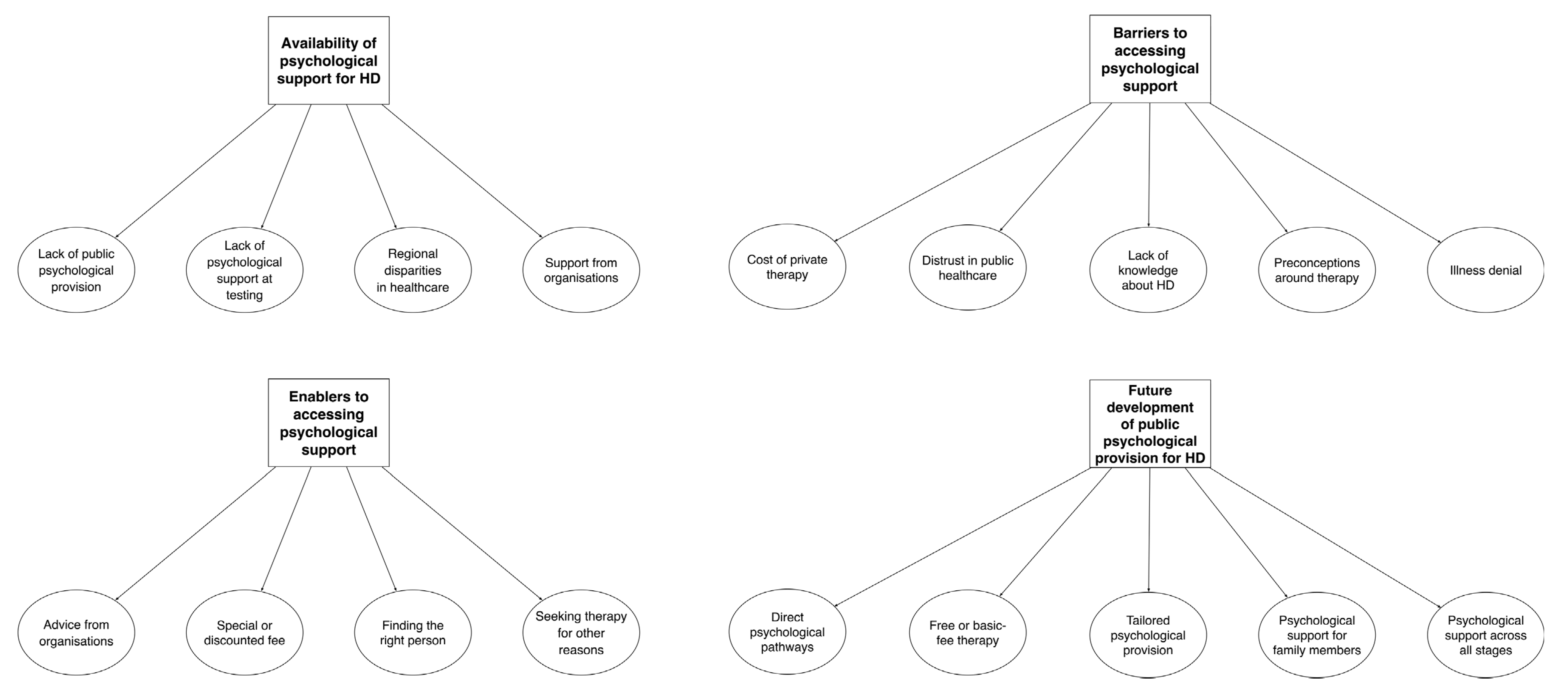
3.1. Overview of Identified Themes and Codes
3.2. Theme 1—‘Unfortunately, That’s Our Country for You’: Availability of Psychological Support in HD
In my opinion, the big problem is public psychological support in general, not just for HD. Because I did not receive any psychological support even after I suffered a heart attack, after spending a week in the ICU. […] Public psychological provision is extremely scarce.—Caregiver 7
It’s almost laughable, non-existent. At least in my case, sadly.—Patient 7
There are no services around here. Nothing.—Caregiver 3
I had my genetic test in 2010. It was me, my sister, and my newlywed wife. They gave us the results and only said ‘as you know, the disease can be inherited with a 50% chance’. My sister was fine, I had the gene. […] And that was it. I did not receive any psychological support; they just gave me the unvarnished truth. It made me feel distraught.—Patient 1
I wasn’t expecting them to play it down, but they also gave me the results making me feel as if I was just about to die, as if it was the most horrible news in the world. It felt devastating and overwhelming.—Patient 5
The way they delivered the news really was really traumatic. There was no psychological support, they simply told my husband: ‘your sister is fine, you are sick’.—Caregiver 1
They told me: ‘Just put this envelope [the results] in a drawer and get on with your life’. But that’s not how it goes, obviously. […] It’s terrifying. Absolutely terrifying.—Patient 2
Unfortunately, Italy is split into two, you know. In the north certain things work better, despite all the country’s problems, and the centre still manages to make do. But if you go south, things get pretty difficult, I believe.—Caregiver 7
I don’t think public psychological services can help you, because we don’t have enough psychologists. […] Our local orthopaedics department is shutting down because they are out of surgeons. We have no orthopaedic doctors, let alone psychologists.—Patient 3
I believe psychological services for people who have difficulties are more present in regions where public healthcare functions better. […] As long as we have this patchworked Health Service, with different rules and wait times across regions, it’ll always be hard to reach some equality. Unfortunately, that’s our country for you.—Caregiver 5
If I need anything, I know I have my HD organisation. They call me often, roughly once a month, to check in on me. They always tell me to let them know straight away if there’s something going on, to call them. So, I feel looked after.—Patient 3
They told me that they were there for me, if I needed anything. That I could call them anytime.—Patient 6
As far as I know, the psychological support for HD is left to non-profit organisations which take care of patients in the community.—Caregiver 5
I did not ask for [public] support. First of all, because I don’t believe we have any services around here. I wouldn’t even know what to ask for. I don’t think there are any services that could help.—Patient 3
3.3. Theme 2—‘I’m Afraid of Seeing Someone Who Doesn’t Know HD’: Barriers to Accessing Psychological Support
I went to see a psychologist a couple of times. But then I stopped because my partner was changing his job and we could not afford it.—Patient 6
To be honest, when it comes to [therapy] costs… well, 70 euros per week […] it’s hard. Even though it’s helpful. Very helpful.—Caregiver 7
I used to see a private psychologist for a few years. [Then] I lost my job, so I did not have the money to continue.—Patient 7
Personally, I could use some form of psychological help, but I can’t afford it. One of my daughters is already seeing a private psychologist, so I cannot afford two private therapies.—Patient 5
We get along just fine, but we can’t afford to spend 1000 euros a month to pay for therapy for the whole family.—Caregiver 1
Public healthcare is a disaster. It doesn’t work well. When we go to the hospital, for example, it’s a mess.—Caregiver 6
Unfortunately, waitlists for public psychological support are much longer.—Patient 7
The whole healthcare system needs to be reformed because it’s getting worse across the board.—Caregiver 5
We were advised to avoid psychologists in the public healthcare system, because they just fill you up with medications.—Patient 6
I saw a psychologist; she barely knew what HD was. She said to me: ‘Oh, I’ve heard about it once”. What do you mean you’ve heard about it once? That’s when I left.—Patient 7
If you go see a psychologist here, they won’t know what HD is. […] I’ve recently met my new GP, I told her my diagnosis, and she didn’t know what it was. After this she did catch up with the literature. But my GP didn’t know what disease it was!—Patient 3
I’m afraid of seeing someone who doesn’t know HD or knows little about it. ALS and Alzheimer’s are known, so you have centres, psychological services dedicated to them.—Patient 6
Well, I believe that psychological support only really exists for people who have severe issues.—Patient 5
The national healthcare system only offers sporadic help, and you need to have some severe problem. I am not severe enough, I’m too stable! [laughs]—Caregiver 1
My dad would have never accepted any psychological help. Because he felt he ‘was a man’, you know.—Patient 7
Up until a couple of years ago, if you told my husband about seeing a psychologist, he would tell you it was money down the drain. [...] It’s just this small-town mindset, you know—if you see a psychologist, it means you’re a fool.—Caregiver 1
I am not a person to work on his own subconscious, I don’t dig deep inside. So I don’t feel like having any psychological support for now.—Patient 1
My character is quite reserved, I am a bit withdrawn. So, I don’t like discussing my business, my feelings, or my problems with other people. I find my support within my family, with my sisters or my mother.—Caregiver 3
I’ve had, let’s say, a bad experience with psychological support. I was forced to engage with it in 2019, due to some difficulties with my son. [...] My wife and I were sent to see a family psychologist once a week, and this never really sat right with me. [...] I felt helped a bit, but then this woman would dig up my past every time, and I always felt I had to open up too much. [...] And in 2021, when I received my diagnosis, I was advised to see a psychologist. But I’ll be honest, I did not do it. I did not follow that advice, coming from my previous experience.—Patient 1
Receiving some psychological support is always good, so I would accept it if it was offered to me. But my wife? I don’t know, she is a bit peculiar about this. […] Because she rejects the disease at times. She doesn’t want to feel ill, let’s say.—Caregiver 5
My husband denies it, but we were only married three months when we found out [about HD]. And I married a cheerful guy who turned into another person overnight. Always serious and withdrawn. […] All these years, he has kept telling himself this fairy tale that he has not changed. […] A defence mechanism, isn’t it? […] And I keep telling him: ‘You need to get some help!’—Caregiver 1
3.4. Theme 3—‘I Would Speak with My HD Organisation First’: Enablers to Accessing Psychological Support
The HD organisation’s staff gave me the contact details of a fantastic psychologist.—Patient 7
The organisation’s staff recommended this psychologist, in case I wanted to receive some support, because they knew her. So, I went to see her.—Patient 6
The psychologist was private, […] but we agreed a discounted fee.—Patient 6
The psychologist gave me a special treatment. The regular fee was 70 euros per session, I only paid 45. It was a fantastic deal.—Patient 7
If I need it, I’ll certainly seek some support. […] But I would speak with my HD organisation first, about seeing a psychologist.—Patient 2
If my HD organisation has the contact details of someone in my area, someone they know, who knows HD… then this person would already know what I’m talking about.—Caregiver 4
First of all, I need to be able to choose the person to do therapy with. They can’t be someone random, because rapport is essential in therapy, the empathy between the patient and the clinician.—Patient 5
Someone who knows HD, is welcoming, and understands our difficulties. […] I’ll go where I need to. If it has to be a private one, then I’ll see a private one.—Patient 4
I was really lucky to find the perfect psychologist for me from day one. Love at first sight, you know. And that helped me massively.—Caregiver 1
You know what matters the most to me? Trust. If I trust a person, I’ll be happy to see them even online.—Patient 2
I saw a psychologist previously, but for different reasons. […] a friend of mine died by suicide, and I felt like giving everything up. So, I told myself: ‘I need some help’. And I started seeing a psychologist every week. […] It was the best choice I could ever make.—Caregiver 1
I went to see a psychologist for other problems, some problems I had with my daughter. […] It helped me increase my self-esteem.—Patient 2
When I got the news [diagnosis], I reconnected with the psychologist I saw for a long time when I was at university. I went to see him only once. […] One session was enough for me, to ‘reset my mind’.—Patient 5
3.5. Theme 4—‘We Should Just Be Able to Call’: Future Development of Public Psychological Provision in HD
A toll-free number to support patients and caregivers at different life stages. When they are having acute difficulties, because these can happen, but also during moments of apparent calm.—Caregiver 5
We should just be able to call… ring a person who would be able to see how things are going, what patients need.—Caregiver 6
They should create ad-hoc centres. […] Listening or counselling centres. There may not be enough resources for ones dedicated to Huntington’s disease, because it’s a rare condition, but they could create some regional centres for rare neurodegenerative diseases where patients can access psychological support.—Caregiver 5
It needs to be easy to access. Being public, it needs to be a service where if you ask for a session today, they don’t tell you: ‘Come the day before Christmas’. Because that’s how public services work right now.—Caregiver 2
It should be free! [laughs]—Patient 4
To have a support… that is public and doesn’t break the bank. That’d be helpful.—Patient 6
It should be free, or with a fee based on income. […] So that those who can’t afford it don’t need to pay.—Caregiver 5
For someone like my dad, who has trouble getting out of the house, it should be possible to do it online or to have a home visit. It should be tailored around a person’s needs.—Patient 5
If it’s public, it also needs to be accessible from home without having to travel here and there. That can also be a problem, you know. [...] My wife currently goes on her own [to therapy], but if we both need to start traveling there then it can become a problem.—Caregiver 2
We need psychological support from someone who knows the condition, who knows other cases. Someone experienced.—Caregiver 3
It would take someone who knows the disease and, most importantly, has had some experience dealing with a patient with Huntington’s.—Patient 3
When the time comes to tell the children [about HD]. Then, yes, a psychologist would be helpful, maybe even a developmental psychologist.—Caregiver 4
Maybe a psychologist would be better than me at dealing with these things, they are able to connect with the kids, use the right words.—Patient 4
I don’t know if due to the disease or what else, but we are living through a time of enormous change. […] The girls are growing up and I thought that my role as a parent, you know, I didn’t think it would end exactly when they turn 18, but I thought it would get at least a bit lighter. Instead, I feel a great pressure to continue supporting my daughters.—Patient 5
We need clinicians who are qualified to work psychologically with patients as well as partners and relatives […] because at times they may struggle to understand that issues such as irritability and aggressiveness are due to the disease.—Patient 3
They [psychologists] would be needed to help caregivers understand that life isn’t over. I see my father-in-law and my heart bleeds. […] There should be some support for family members too.—Patient 5
It needs to be available before taking the test. When you go and do the test you must be sure, psychologically, that you want to do it. Because otherwise you risk being hit by a brick.—Patient 1
It’d be certainly very important in the beginning, when it’s diagnosed. It’s life-changing, so a psychologist would be needed for sure.—Caregiver 4
Psychological support would also be needed halfway through… after someone gets to know, because then you get the thought… personally, I’ve never had the idea of taking my own life, because I never thought about it. But there are people who may.—Patient 6
Perhaps it would be good to get some help during the final stage, when maybe you start realising you are about to go and you need support.—Patient 4
I would ask for psychological help according to my needs, and I believe needs increase over time. So, maybe now I need it less than I will in one, five, or ten years.—Caregiver 7
It has to be a type of support that evolves along with the disease, because each different situation needs a different type of intervention.—Caregiver 2
4. Discussion
4.1. Summary of Main Findings
4.2. Clinical Implications
4.3. Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghosh, R.; Tabrizi, S.J. Huntington Disease. Handb. Clin. Neurol. 2018, 147, 255–278. [Google Scholar] [CrossRef]
- Walker, F.O.O. Huntington’s Disease. Lancet 2007, 27, 143–150. [Google Scholar] [CrossRef]
- Ghosh, R.; Tabrizi, S.J. Clinical Aspects of Huntington’s Disease; Springer: Berlin/Heidelberg, Germany, 2013; pp. 3–31. [Google Scholar]
- Zarotti, N.; Simpson, J.; Fletcher, I.; Squitieri, F.; Migliore, S. Exploring Emotion Regulation and Emotion Recognition in People with Presymptomatic Huntington’s Disease: The Role of Emotional Awareness. Neuropsychologia 2018, 112, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zarotti, N.; Fletcher, I.; Simpson, J. New Perspectives on Emotional Processing in People with Symptomatic Huntington’s Disease: Impaired Emotion Regulation and Recognition of Emotional Body Language. Arch. Clin. Neuropsychol. 2019, 34, 610–624. [Google Scholar] [CrossRef] [PubMed]
- Dumas, E.E.M.; van den Bogaard, S.J.A.; Middelkoop, H.A.M.; Roos, R.A.C. A Review of Cognition in Huntington’s Disease. Front. Biosci. (Schol. Ed.) 2013, 5, 1–18. [Google Scholar]
- Medina, A.; Mahjoub, Y.; Shaver, L.; Pringsheim, T. Prevalence and Incidence of Huntington’s Disease: An Updated Systematic Review and Meta-Analysis. Mov. Disord. 2022, 37, 2327–2335. [Google Scholar] [CrossRef] [PubMed]
- Huntington’s Disease Collaborative Research Group A Novel Gene Containing a Trinucleotide Repeat That Is Expanded and Unstable on Huntington’s Disease Chromosomes. Cell 1993, 72, 971–983. [CrossRef]
- Fusilli, C.; Migliore, S.; Mazza, T.; Consoli, F.; De Luca, A.; Barbagallo, G.; Ciammola, A.; Gatto, E.M.; Cesarini, M.; Etcheverry, J.L.; et al. Biological and Clinical Manifestations of Juvenile Huntington’s Disease: A Retrospective Analysis. Lancet Neurol. 2018, 17, 986–993. [Google Scholar] [CrossRef]
- Folstein, S. Huntington’s Disease: A Disorder of Families; The Johns Hopkins University Press: Baltimore, MD, USA, 1989. [Google Scholar]
- Rodrigues, F.B.; Abreu, D.; Dam, J.; Goncalves, N.; Correia-Guedes, L.; Coelho, M.; Ferreira, J.J. Survival, Mortality, Causes and Places of Death in a European Huntington’s Disease Prospective Cohort CLINICAL PRACTICE. Mov. Disord Clin. Pract. 2017, 4, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Shoulson, I.; Fahn, S. Huntington Disease: Clinical Care and Evaluation. Neurology 1979, 29, 1–3. [Google Scholar] [CrossRef]
- Zarotti, N.; Dale, M.; Eccles, F.; Simpson, J. Psychological Interventions for People with Huntington’s Disease: A Call to Arms. J. Huntingt. Dis. 2020, 9, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Dale, M.; van Duijn, E. Anxiety in Huntington’s Disease. J. Neuropsychiatry Clin. Neurosci. 2015, 27, 262–271. [Google Scholar] [CrossRef] [PubMed]
- van Duijn, E.; Craufurd, D.; Hubers, A.A.M.; Giltay, E.J.; Bonelli, R.; Rickards, H.; Anderson, K.E.; Van Walsem, M.R.; Van Der Mast, R.C.; Orth, M.; et al. Neuropsychiatric Symptoms in a European Huntington’s Disease Cohort (REGISTRY). J. Neurol. Neurosurg. Psychiatry 2014, 85, 1411–1418. [Google Scholar] [CrossRef] [PubMed]
- Roos, R.A.C. Huntington’s Disease: A Clinical Review. Orphanet J. Rare Dis. 2010, 5, 40. [Google Scholar] [CrossRef]
- Hubers, A.A.M.; Reedeker, N.; Giltay, E.J.; Roos, R.A.C.; van Duijn, E.; van der Mast, R.C. Suicidality in Huntington’s Disease. J. Affect. Disord. 2012, 136, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Banaszkiewicz, K.; Sitek, E.J.; Rudzińska, M.; Sołtan, W.; Sławek, J.; Szczudlik, A. Huntington’s Disease from the Patient, Caregiver and Physician’s Perspectives: Three Sides of the Same Coin? J. Neural Transm. 2012, 119, 1361–1365. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.; Hocaoglu, M. Impact of Huntington’s across the Entire Disease Spectrum: The Phases and Stages of Disease from the Patient Perspective. Clin. Genet 2011, 80, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Underwood, M.; Bonas, S.; Dale, M. Huntington’s Disease: Prevalence and Psychological Indicators of Pain. Mov. Disord Clin. Pract. 2017, 4, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Crozier, S.; Robertson, N.; Dale, M. The Psychological Impact of Predictive Genetic Testing for Huntington′s Disease: A Systematic Review of the Literature. J. Genet. Couns. 2014, 24, 29–39. [Google Scholar] [CrossRef]
- Wahlin, T.-B.R. To Know or Not to Know: A Review of Behaviour and Suicidal Ideation in Preclinical Huntington’s Disease. Patient Educ. Couns. 2007, 65, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, L.; Timman, R.; Trijsburg, W.; Duisterhof, M.; Erdman, R.; Van Elderen, T.; Tibben, A. Attachment in Families with Huntington’s Disease. A Paradigm in Clinical Genetics. Patient Educ. Couns. 2006, 63, 246–254. [Google Scholar] [CrossRef]
- Forrest Keenan, K.; van Teijlingen, E.; McKee, L.; Miedzybrodzka, Z.; Simpson, S.A.; Keenan, K.F.; van Teijlingen, E.; McKee, L.; Miedzybrodzka, Z.; Simpson, S.A. How Young People Find out about Their Family History of Huntington’s Disease. Soc. Sci. Med. 2009, 68, 1892–1900. [Google Scholar] [CrossRef] [PubMed]
- Zarotti, N.; Dale, M.; Eccles, F.J.R.; Simpson, J. More than Just a Brain Disorder: A Five-Point Manifesto for Psychological Care for People with Huntington’s Disease. J. Pers. Med. 2022, 12, 64. [Google Scholar] [CrossRef] [PubMed]
- Simpson, J.; Eccles, F.J.; Zarotti, N. Extended Evidence-Based Guidance on Psychological Interventions for Psychological Difficulties in Individuals with Huntington’s Disease, Parkinson’s Disease, Motor Neurone Disease, and Multiple Sclerosis; Lancaster University: Lancaster, UK, 2021. [Google Scholar] [CrossRef]
- Eccles, F.J.R.; Craufurd, D.; Smith, A.; Davies, R.; Glenny, K.; Homberger, M.; Rose, L.; Theed, R.; Peeren, S.; Rogers, D.; et al. Experiences of Mindfulness-Based Cognitive Therapy for Premanifest Huntington’s Disease. J. Huntingt. Dis. 2021, 10, 277–291. [Google Scholar] [CrossRef] [PubMed]
- A’Campo, L.E.I.; Spliethoff-Kamminga, N.G.A.; Roos, R.A.C. The Patient Education Program for Huntington’s Disease (PEP-HD). J. Huntingt. Dis. 2012, 1, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Eccles, F.J.R.; Craufurd, D.; Smith, A.; Davies, R.; Glenny, K.; Homberger, M.; Peeren, S.; Rogers, D.; Rose, L.; Skitt, Z.; et al. A Feasibility Investigation of Mindfulness-Based Cognitive Therapy for People with Huntington’s Disease. Pilot Feasibility Stud. 2020, 6, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.A.; Brown, A. Sensory Modulation Intervention and Behaviour Support Modification for the Treatment of Severe Aggression in Huntington’s Disease. A Single Case Experimental Design. Neuropsychol. Rehabil. 2017, 27, 891–903. [Google Scholar] [CrossRef] [PubMed]
- British Psychological Society. Psychological Interventions for People with Huntington’s Disease, Parkinson’s Disease, Motor Neurone Disease, and Multiple Sclerosis: Evidence-Based Guidance; British Psychological Society: Leicester, UK, 2021. [Google Scholar] [CrossRef]
- Cresswell, J. Qualitative Inquiry and Research Design: Choosing among Five Approaches, 2nd ed.; SAGE: London, UK, 2007. [Google Scholar]
- Harper, D. Choosing a Qualitative Research Method; Wiley Blackwell: Hoboken, NJ, USA, 2011; ISBN 0470663731. [Google Scholar]
- Hartelius, L.; Jonsson, M.; Rickeberg, A.; Laakso, K. Communication and Huntington’s Disease: Qualitative Interviews and Focus Groups with Persons with Huntington’s Disease, Family Members, and Carers. Int. J. Lang. Commun. Disord./R. Coll. Speech Lang. Ther. 2010, 45, 381–393. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. APA Handbook of Research Methods in Psychology, Vol 2: Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological; Cooper, H., Camic, P.M., Long, D.L., Panter, A.T., Rindskopf, D., Sher, K.J., Eds.; American Psychological Association: Washington, DC, USA, 2012; Volume 2, ISBN 1-4338-1005-0. [Google Scholar]
- Braun, V.; Clarke, V. Is Thematic Analysis Used Well in Health Psychology? A Critical Review of Published Research, with Recommendations for Quality Practice and Reporting. Health Psychol. Rev. 2023, 17, 695–718. [Google Scholar] [CrossRef] [PubMed]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Sayer, A. Realism and Social Science; Routledge: London, UK, 2000. [Google Scholar]
- France, G.; Taroni, F.; Donatini, A. The Italian Health-Care System. Health Econ. 2005, 14, S187–S202. [Google Scholar] [CrossRef] [PubMed]
- Priebe, S.; Wright, D. The Provision of Psychotherapy: An International Comparison. J. Public Ment. Health 2006, 5, 12–22. [Google Scholar] [CrossRef]
- Soltysiak, B.; Gardiner, P.; Skirton, H. Exploring Supportive Care for Individuals Affected by Huntington Disease and Their Family Caregivers in a Community Setting. J. Clin. Nurs. 2008, 17, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Lee, O.; Porteous, M. Genetic Testing and Reproductive Choice in Neurological Disorders. Pract. Neurol. 2017, 17, 275–281. [Google Scholar] [CrossRef]
- Saita, E.; Zuliani, C.; Tramontano, M.; Bonanno, G.A. Trust or Distrust Toward Healthcare Services: Breast Screening in the North and South of Italy. World Futures 2016, 72, 254–265. [Google Scholar] [CrossRef]
- Mohr, D.C.; Ho, J.; Duffecy, J.; Baron, K.G.; Lehman, K.A.; Jin, L.; Reifler, D. Perceived Barriers to Psychological Treatments and Their Relationship to Depression. J. Clin. Psychol. 2010, 66, 394–409. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S. Accessing Psychological Therapies: Homeless Young People’s Views on Barriers and Facilitators. Couns. Psychother. Res. (CPR) 2016, 16, 54–63. [Google Scholar] [CrossRef]
- Schaffler, Y.; Probst, T.; Jesser, A.; Humer, E.; Pieh, C.; Stippl, P.; Haid, B.; Schigl, B. Perceived Barriers and Facilitators to Psychotherapy Utilisation and How They Relate to Patient’s Psychotherapeutic Goals. Healthcare 2022, 10, 2228. [Google Scholar] [CrossRef] [PubMed]
- Domaradzki, J. The Impact of Huntington Disease on Family Carers: A Literature Overview. Psychiatr. Pol. 2015, 49, 931–944. [Google Scholar] [CrossRef] [PubMed]
- Skirton, H.; Williams, J.K.; Jackson Barnette, J.; Paulsen, J.S. Huntington Disease: Families’ Experiences of Healthcare Services. J. Adv. Nurs. 2010, 66, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.K.; Skirton, H.; Barnette, J.J.; Paulsen, J.S. Family Carer Personal Concerns in Huntington Disease. J. Adv. Nurs. 2012, 68, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Etchegary, H. Healthcare Experiences of Families Affected by Huntington Disease: Need for Improved Care. Chronic. Illn. 2011, 7, 225–238. [Google Scholar] [CrossRef] [PubMed]
- Lobban, T.C.A.; Camm, A.J. Patient Associations as Stakeholders: A Valuable Partner for Facilitating Access to Therapy. Europace 2011, 13, ii21-4. [Google Scholar] [CrossRef]
- Hélaine, A.; Podevin, M. The Role of Patients’ Associations. Bull. Cancer 2020, 107, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Pinto, C.; Geraghty, A.W.A.; McLoughlin, C.; Pagnini, F.; Yardley, L.; Dennison, L. Experiences of Psychological Interventions in Neurodegenerative Diseases: A Systematic Review and Thematic Synthesis. Health Psychol. Rev. 2023, 17, 416–438. [Google Scholar] [CrossRef]


{kind=link}
| Participant ID | Age | Gender | Area of Italy | Time Since Clinical Diagnosis |
|---|---|---|---|---|
| Patient 1 | 41 | Male | Centre | 1 year |
| Patient 2 | 61 | Female | North | 9 years |
| Patient 3 | 57 | Male | South | 1 year |
| Patient 4 | 38 | Female | Centre | 3 years |
| Patient 5 | 52 | Female | Centre | 4 years |
| Patient 6 | 51 | Female | South | 3 years |
| Patient 7 | 49 | Female | Centre | <1 year |
| Caregiver 1 | 42 | Female | Centre | |
| Caregiver 2 | 68 | Male | North | |
| Caregiver 3 | 57 | Female | South | |
| Caregiver 4 | 39 | Male | Centre | |
| Caregiver 5 | 53 | Male | Centre | |
| Caregiver 6 | 55 | Male | South | |
| Caregiver 7 | 52 | Male | Centre |
| Topic | Example Question |
|---|---|
| Introduction and preliminary clinical information | When were you/was your partner diagnosed with Huntington’s disease? |
| Psychological impact of HD | Have you ever received any information from healthcare professionals on the psychological impact of HD? |
| Psychological support for HD | Have you ever received any form of public/free psychological support for HD? |
| Closing remarks | Is there anything you would like to add that we did not have a chance to discuss? |
| Theme | Codes |
|---|---|
| ‘Unfortunately, that’s our country for you’: availability of psychological support in HD | Lack of public psychological provision No psychological support at testing Regional disparities in healthcare Support from organisations |
| ‘I’m afraid of seeing someone who doesn’t know HD’: barriers to accessing psychological support | Cost of private therapy Distrust in public healthcare Lack of knowledge about HD Preconceptions around therapy Illness denial |
| ‘I would speak with my HD organisation first’: enablers to accessing psychological support | Advice from organisations Special or discounted fees Finding the right person Seeking therapy for other reasons |
| ‘We should just be able to call’: Future development of public psychological provision in HD | Direct psychological pathways Free or basic fee therapy Tailored psychological provision Psychological support for family members Psychological provision across all stages |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarotti, N.; D’Alessio, B.; Scocchia, M.; Casella, M.; Squitieri, F. “I Wouldn’t Even Know What to Ask for”: Patients’ and Caregivers’ Experiences of Psychological Support for Huntington’s Disease in Italy. NeuroSci 2024, 5, 98-113. https://doi.org/10.3390/neurosci5020007
Zarotti N, D’Alessio B, Scocchia M, Casella M, Squitieri F. “I Wouldn’t Even Know What to Ask for”: Patients’ and Caregivers’ Experiences of Psychological Support for Huntington’s Disease in Italy. NeuroSci. 2024; 5(2):98-113. https://doi.org/10.3390/neurosci5020007
Chicago/Turabian StyleZarotti, Nicolò, Barbara D’Alessio, Marta Scocchia, Melissa Casella, and Ferdinando Squitieri. 2024. "“I Wouldn’t Even Know What to Ask for”: Patients’ and Caregivers’ Experiences of Psychological Support for Huntington’s Disease in Italy" NeuroSci 5, no. 2: 98-113. https://doi.org/10.3390/neurosci5020007