
Recurrent Falls as the Only Clinical Sign of Cortical–Subcortical Myoclonus: A Case Report
 , , , , and
, , , , and 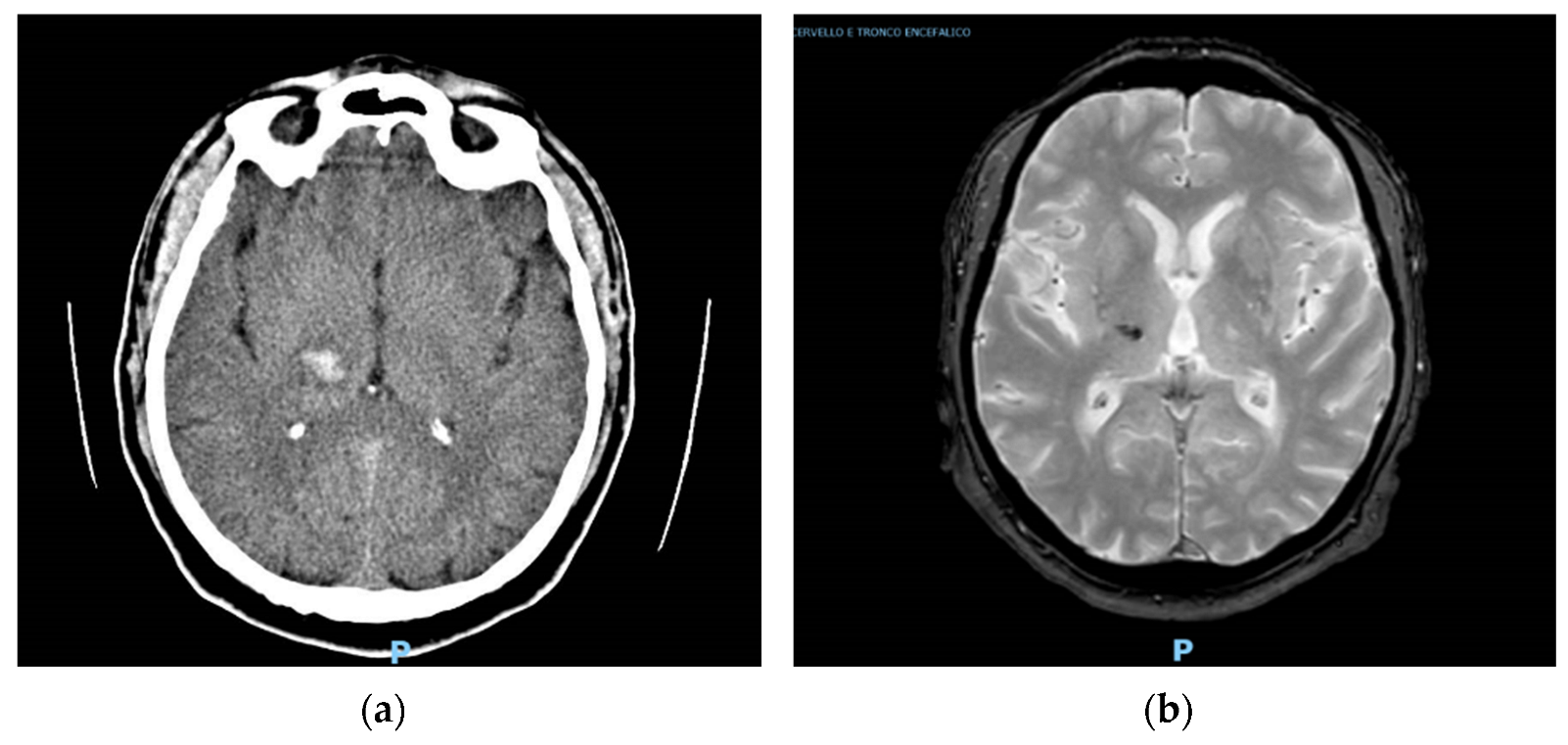{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
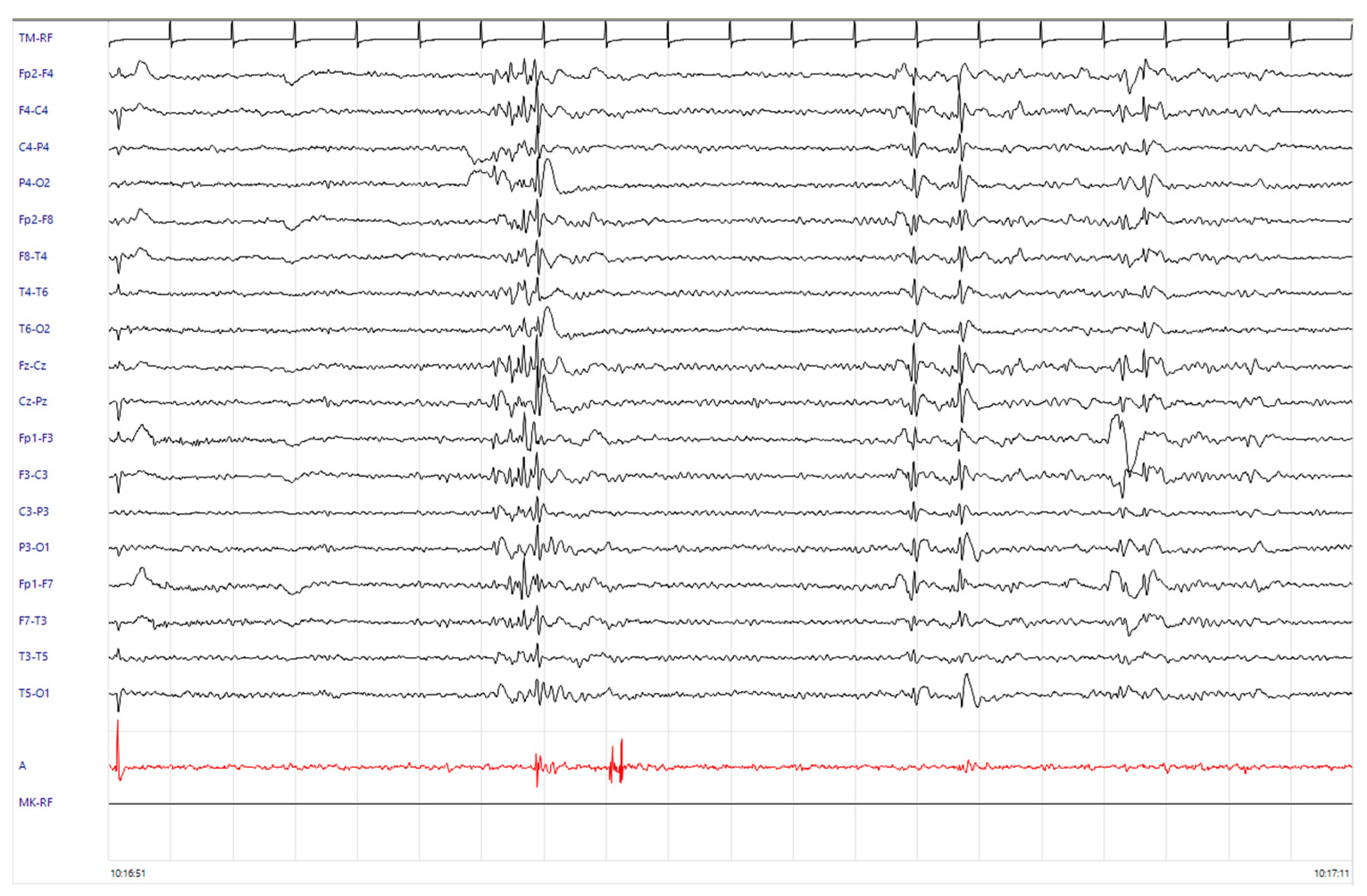
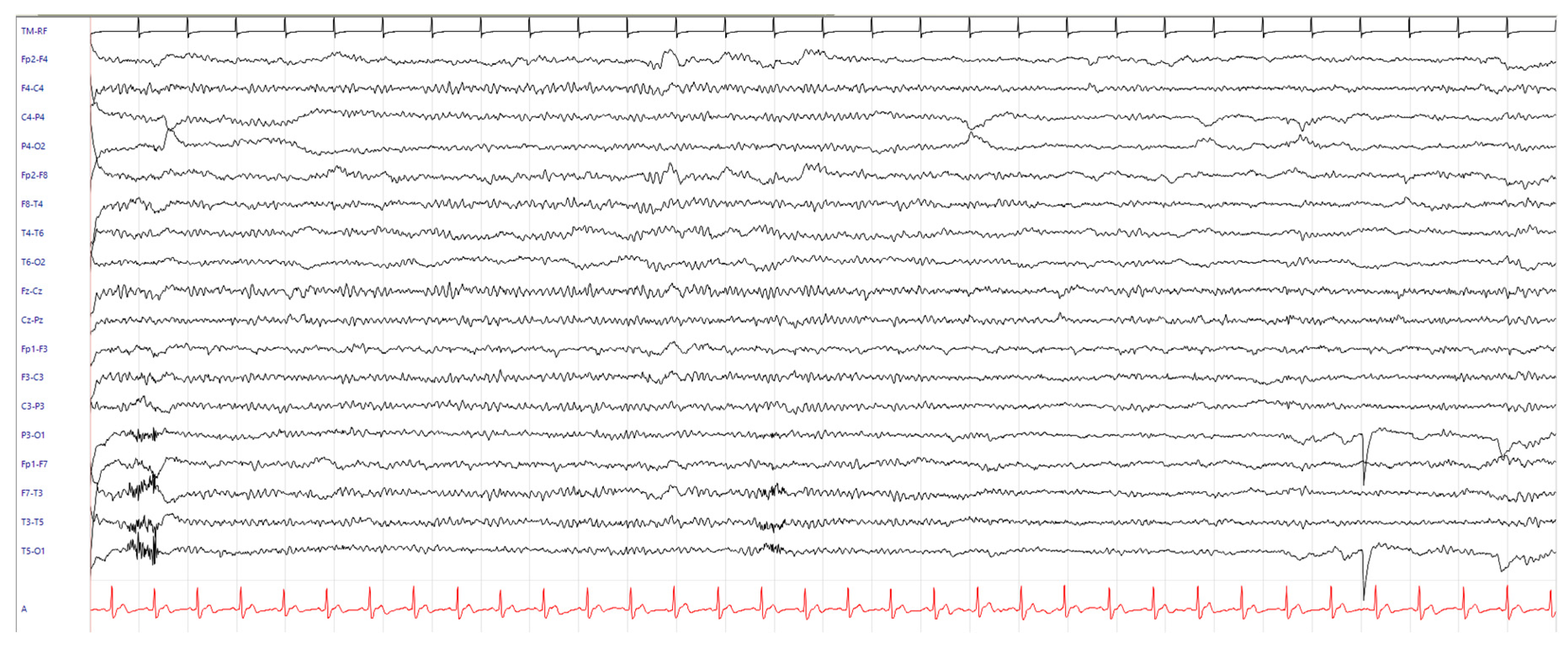
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caviness, J.N. Myoclonus. Contin. Lifelong Learn. Neurol. 2019, 25, 1055–1080. [Google Scholar] [CrossRef] [PubMed]
- Pranzatelli, M.R. Infantile spasms versus myoclonus: Is there a connection? Int. Rev. Neurobiol. 2002, 49, 285–314. [Google Scholar] [CrossRef] [PubMed]
- Caviness, J.N. Pathophysiology and treatment of myoclonus. Neurol. Clin. 2009, 27, 757–777. [Google Scholar] [CrossRef] [PubMed]
- Caviness, J.N.; Truong, D.D. Myoclonus. Handb. Clin. Neurol. 2011, 100, 399–420. [Google Scholar] [CrossRef] [PubMed]
- Stahl, C.M.; Frucht, S.J. An Update on Myoclonus Management. Expert Rev. Neurother. 2019, 19, 325–331. [Google Scholar] [CrossRef]
- Chandarana, M.; Saraf, U.; Divya, K.; Krishnan, S.; Kishore, A. Myoclonus—A Review. Ann. Indian Acad. Neurol. 2021, 24, 327. [Google Scholar] [CrossRef] [PubMed]
- Cassim, F.; Houdayer, E. Neurophysiology of myoclonus. Neurophysiol. Clin. 2006, 36, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Shibasaki, H.; Hallett, M. Electrophysiological studies of myoclonus. Muscle Nerve 2005, 31, 157–174. [Google Scholar] [CrossRef]
- Brown, P.; Day, B.L.; Rothwell, J.C.; Thompson, P.D.; Marsden, C.D. Intrahemispheric and interhemispheric spread of cerebral cortical myoclonic activity and its relevance to epilepsy. Brain 1991, 114, 2333–2351. [Google Scholar] [CrossRef]
- Caviness, J.N. Treatment of Myoclonus. Neurotherapeutics 2014, 11, 188. [Google Scholar] [CrossRef]
- Merchant, S.H.I.; Vial-Undurraga, F.; Leodori, G.; van Gerpen, J.A.; Hallett, M. Myoclonus: An Electrophysiological Diagnosis. Mov. Disord. Clin. Pract. 2020, 7, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Deppe, M.; Kellinghaus, C.; Duning, T.; Möddel, G.; Mohammadi, S.; Deppe, K.; Schiffbauer, H.; Kugel, H.; Keller, S.S.; Ringelstein, E.B.; et al. Nerve fiber impairment of anterior thalamocortical circuitry in juvenile myoclonic epilepsy. Neurology 2008, 71, 1981–1985. [Google Scholar] [CrossRef] [PubMed]
- Snead, O.C. Basic mechanisms of generalized absence seizures. Ann. Neurol. 1995, 37, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.; Rothwell, J.C.; Thompson, P.D.; Marsden, C.D. Propriospinal myoclonus: Evidence for spinal “pattern” generators in humans. Mov. Disord. 1994, 9, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, O.; Topka, H. Myoclonic Disorders. Brain Sci. 2017, 7, 103. [Google Scholar] [CrossRef] [PubMed]
- Apartis, E.; Vercueil, L. To jerk or not to jerk: A clinical pathophysiology of myoclonus. Rev. Neurol. 2016, 172, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Aghakhani, Y.; Bagshaw, A.P.; Bénar, C.G.; Hawco, C.; Andermann, F.; Dubeau, F.; Gotman, J. fMRI activation during spike and wave discharges in idiopathic generalized epilepsy. Brain 2004, 127, 1127–1144. [Google Scholar] [CrossRef] [PubMed]
- Moeller, F.; Siebner, H.R.; Wolff, S.; Muhle, H.; Boor, R.; Granert, O.; Jansen, O.; Stephani, U.; Siniatchkin, M. Changes in activity of striato–thalamo–cortical network precede generalized spike wave discharges. Neuroimage 2008, 39, 1839–1849. [Google Scholar] [CrossRef]
- Kim, J.H. Grey and White Matter Alterations in Juvenile Myoclonic Epilepsy: A Comprehensive Review. J. Epilepsy Res. 2017, 7, 77–88. [Google Scholar] [CrossRef]
- Kim, J.B.; Suh, S.I.; Seo, W.K.; Oh, K.; Koh, S.B.; Kim, J.H. Altered thalamocortical functional connectivity in idiopathic generalized epilepsy. Epilepsia 2014, 55, 592–600. [Google Scholar] [CrossRef]
- Hamandi, K.; Salek-Haddadi, A.; Laufs, H.; Liston, A.; Friston, K.; Fish, D.R.; Duncan, J.S.; Lemieux, L. EEG-fMRI of idiopathic and secondarily generalized epilepsies. Neuroimage 2006, 31, 1700–1710. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Li, Q.; Xia, Y.; Lei, X.; Xue, K.; Yao, Z.; Lai, Y.; Martínez-Montes, E.; Liao, W.; Zhou, D.; et al. Resting state basal ganglia network in idiopathic generalized epilepsy. Hum. Brain Mapp. 2012, 33, 1279–1294. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, J.B.; Suh, S.i.; Kim, D.W. Subcortical grey matter changes in juvenile myoclonic epilepsy. Neuroimage 2018, 17, 397. [Google Scholar] [CrossRef] [PubMed]
- Rossi, J.; Cavallieri, F.; Giovannini, G.; Benuzzi, F.; Ballotta, D.; Vaudano, A.E.; Ferrara, F.; Contardi, S.; Pietrangelo, A.; Corradini, E.; et al. Can Disruption of Basal Ganglia-Thalamocortical Circuit in Wilson Disease Be Associated with Juvenile Myoclonic Epilepsy Phenotype? Brain Sci. 2022, 12, 553. [Google Scholar] [CrossRef] [PubMed]
- Tater, P.; Pandey, S. Post-stroke Movement Disorders: Clinical Spectrum, Pathogenesis, and Management. Neurol. India 2021, 69, 272. [Google Scholar] [CrossRef] [PubMed]
- Suri, R.; Rodriguez-Porcel, F.; Donohue, K.; Jesse, E.; Lovera, L.; Dwivedi, A.K.; Espay, A.J. Post-stroke Movement Disorders: The Clinical, Neuroanatomic, and Demographic Portrait of 284 Published Cases. J. Stroke Cerebrovasc. Dis. 2018, 27, 2388–2397. [Google Scholar] [CrossRef]
- Gupta, N.; Pandey, S. Post-Thalamic Stroke Movement Disorders: A Systematic Review. Eur. Neurol. 2018, 79, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Hosp, J.A.; Luft, A.R. Cortical Plasticity during Motor Learning and Recovery after Ischemic Stroke. Neural Plast. 2011, 2011, 871296. [Google Scholar] [CrossRef]
- Fornito, A.; Zalesky, A.; Breakspear, M. The connectomics of brain disorders. Nat. Rev. Neurosci. 2015, 16, 159–172. [Google Scholar] [CrossRef]
- Scott, B.L.; Jankovic, J. Delayed-onset progressive movement disorders after static brain lesions. Neurology 1996, 46, 68–74. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Napoli, G.; Rossi, J.; Cavallieri, F.; Pugnaghi, M.; Rizzi, R.; Russo, M.; Assenza, F.; Di Rauso, G.; Valzania, F. Recurrent Falls as the Only Clinical Sign of Cortical–Subcortical Myoclonus: A Case Report. NeuroSci 2024, 5, 1-7. https://doi.org/10.3390/neurosci5010001
De Napoli G, Rossi J, Cavallieri F, Pugnaghi M, Rizzi R, Russo M, Assenza F, Di Rauso G, Valzania F. Recurrent Falls as the Only Clinical Sign of Cortical–Subcortical Myoclonus: A Case Report. NeuroSci. 2024; 5(1):1-7. https://doi.org/10.3390/neurosci5010001
Chicago/Turabian StyleDe Napoli, Giulia, Jessica Rossi, Francesco Cavallieri, Matteo Pugnaghi, Romana Rizzi, Marco Russo, Federica Assenza, Giulia Di Rauso, and Franco Valzania. 2024. "Recurrent Falls as the Only Clinical Sign of Cortical–Subcortical Myoclonus: A Case Report" NeuroSci 5, no. 1: 1-7. https://doi.org/10.3390/neurosci5010001