
Excellence in Heart Failure: A Multidisciplinary Program on Heart Failure Management for Improved Patient Outcome

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Participants
2.3. Data Collection and Outcomes
2.4. Statistical Analysis
2.5. Ethics
3. Results
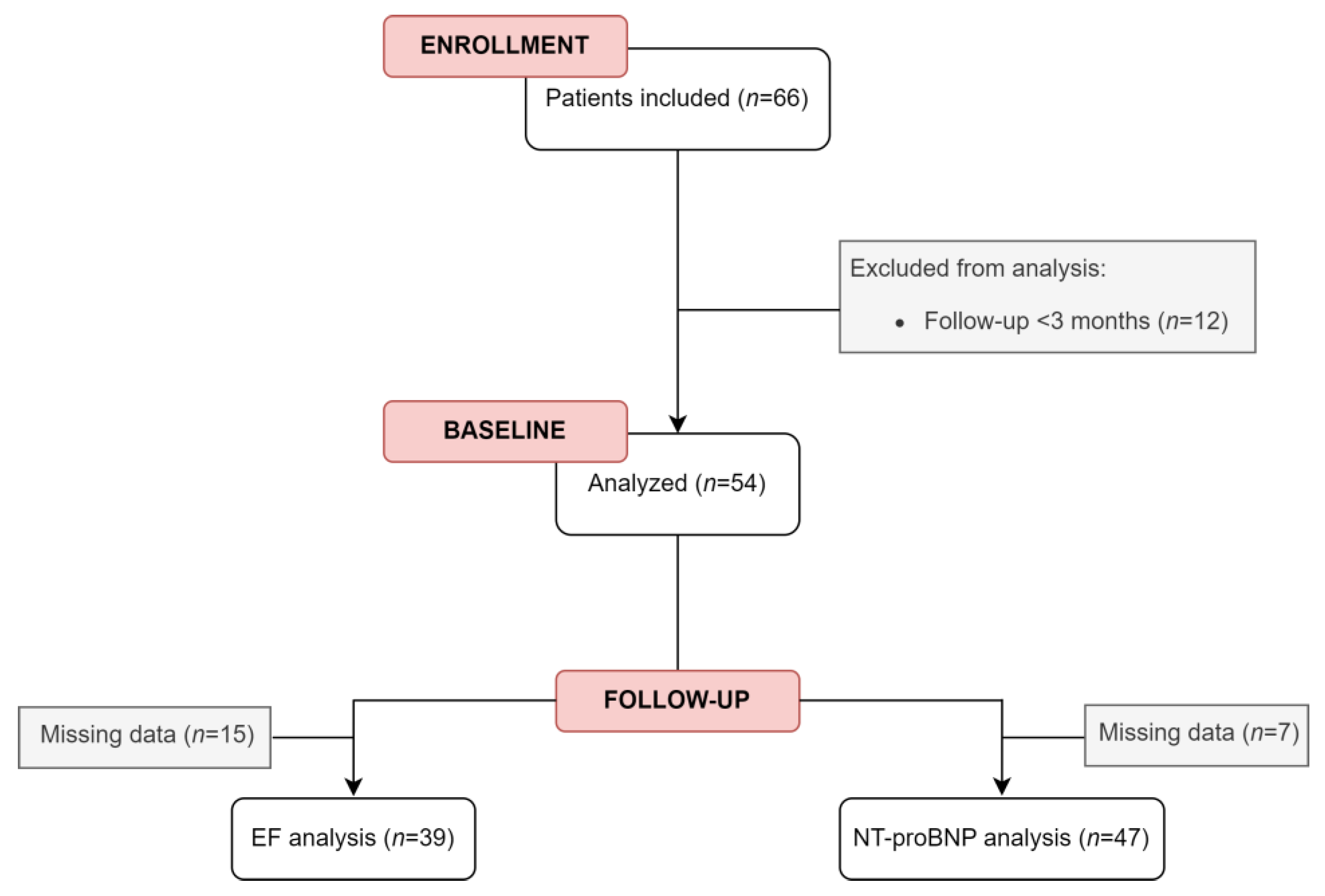
3.1. Study Sample
3.2. Patient Characteristics at Baseline
3.3. HF-Related Events: Hospitalizations, ER Visits, and Mortality Rates
3.4. Treatment Profile during Follow-Up
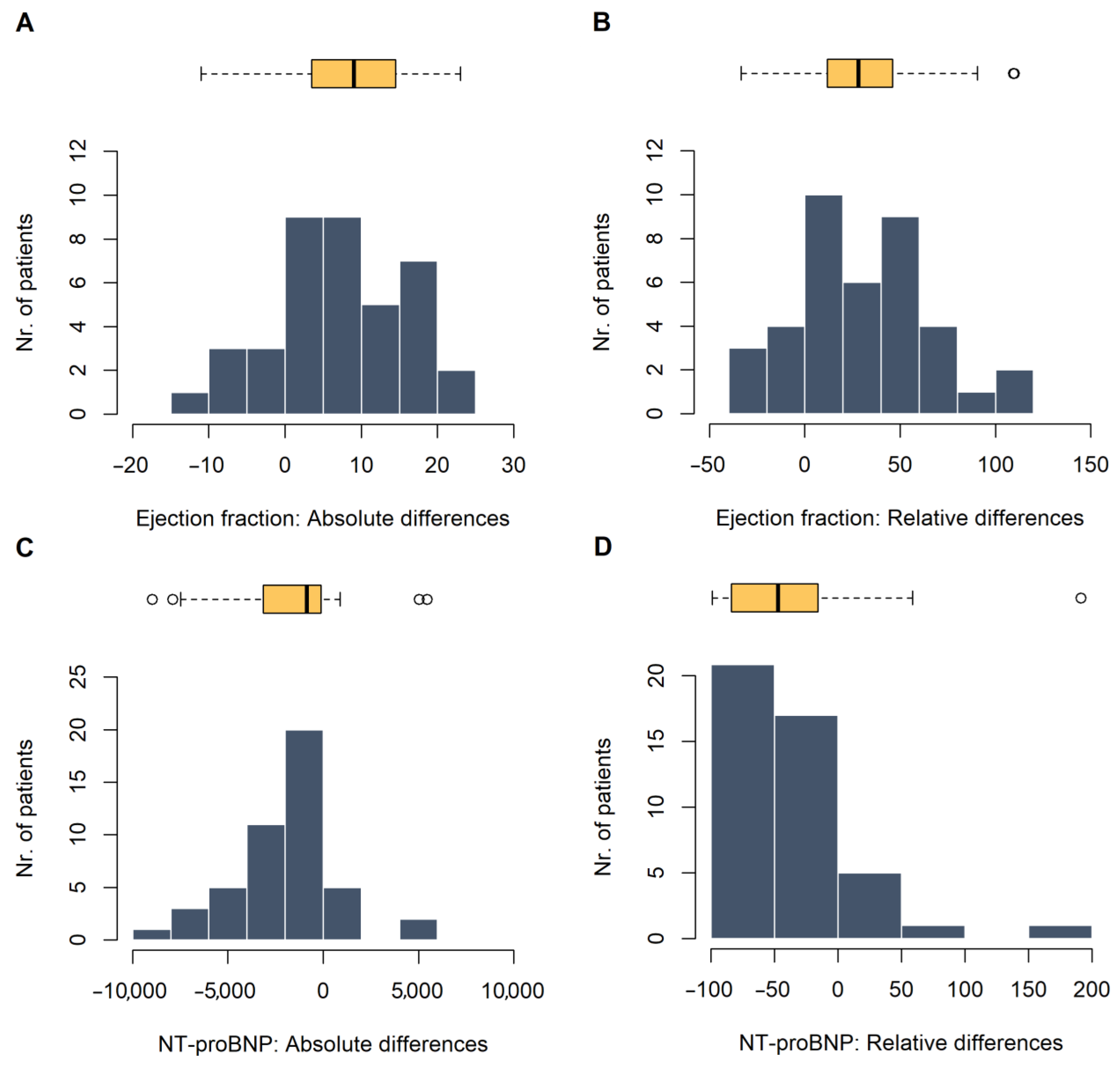
3.5. Cardiac Function at Follow-Up
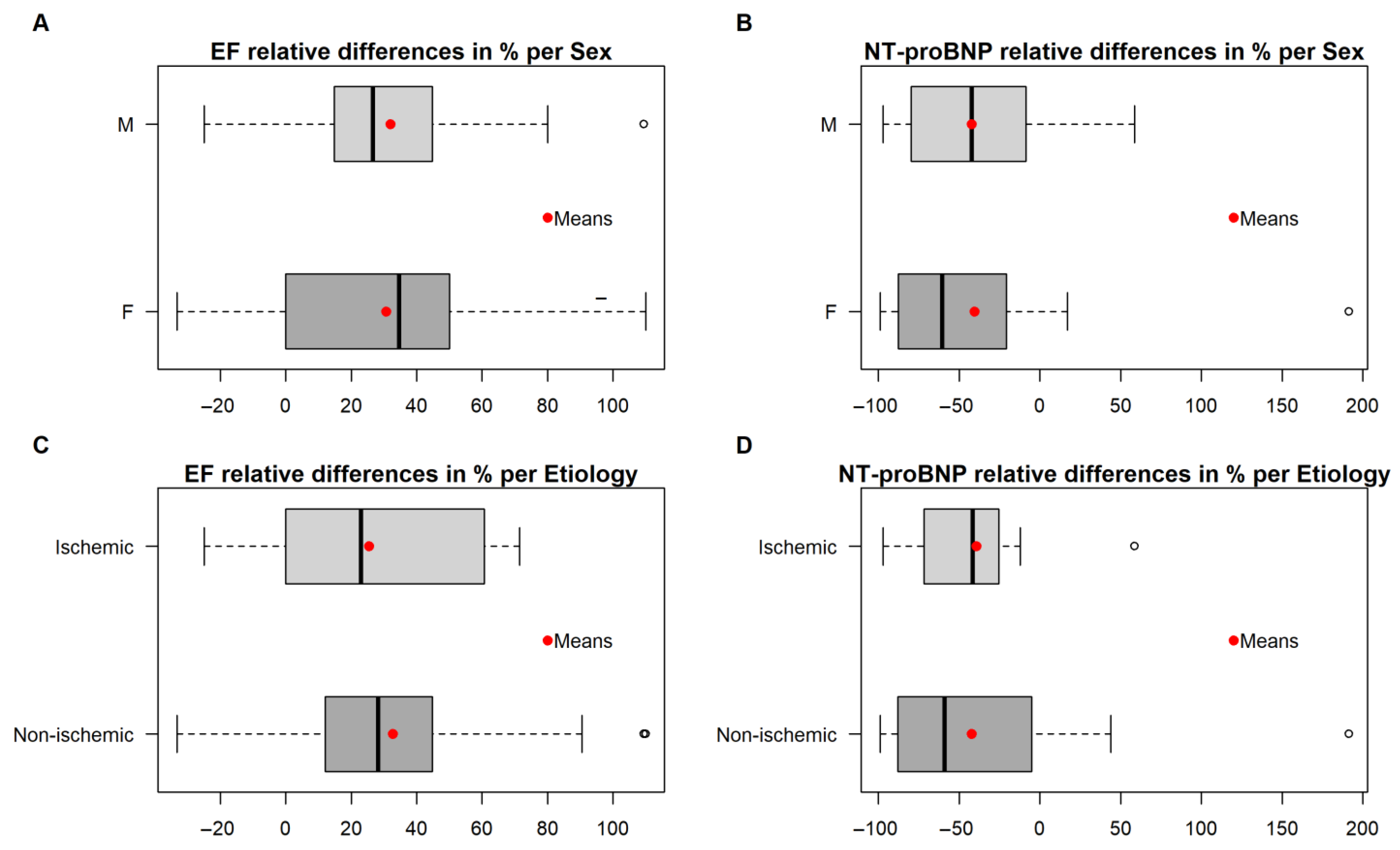
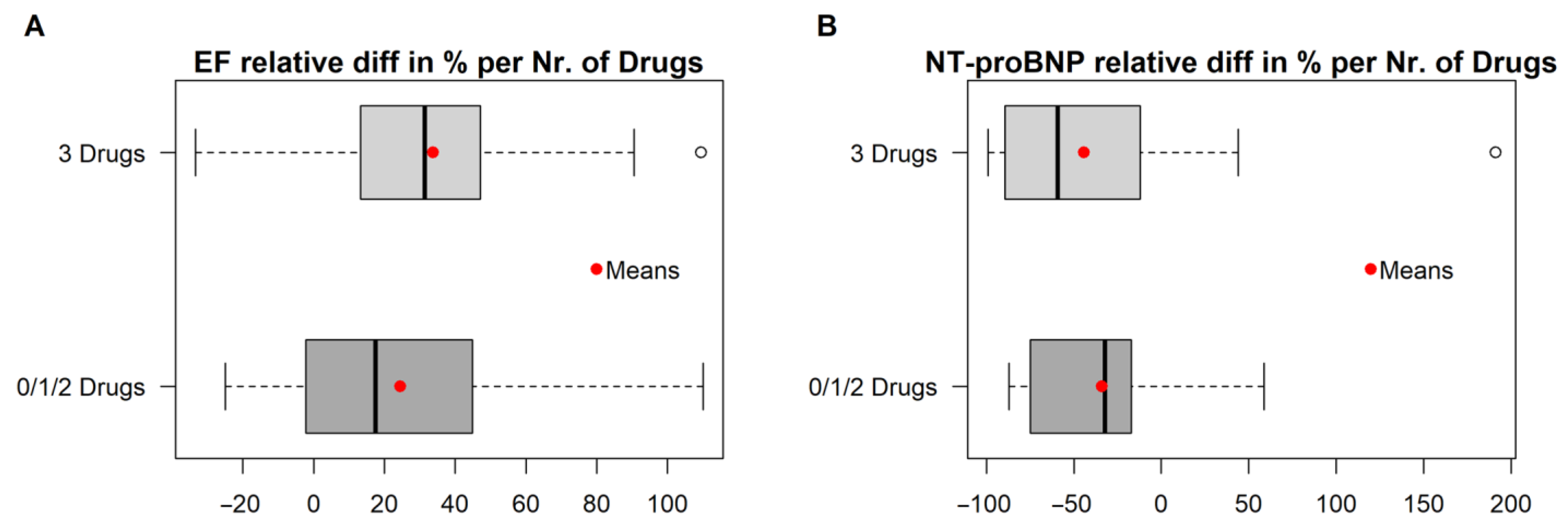
3.6. Factors Associated with Improved Cardiac Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- Farmakis, D.; Stafylas, P.; Giamouzis, G.; Maniadakis, N.; Parissis, J. The medical and socioeconomic burden of heart failure: A comparative delineation with cancer. Int. J. Cardiol. 2016, 203, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, M.; Ascencao, R.; Fiorentino, F.; Costa, J.; Caldeira, D.; Broeiro-Goncalves, P.; Fonseca, C.; Borges, M. The current and future burden of heart failure in Portugal. ESC Heart Fail. 2019, 6, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, C.; Bras, D.; Araujo, I.; Ceia, F. Heart failure in numbers: Estimates for the 21st century in Portugal. Rev. Port. Cardiol. Engl. Ed. 2018, 37, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Rethy, L.; McCabe, M.; Pool, L.R.; Vu, T.T.; Kershaw, K.N.; Yancy, C.; Vupputuri, S.; Feinglass, J.; Khan, S.S. Contemporary Rates of Hospitalization for Heart Failure in Young and Middle-Aged Adults in a Diverse US State. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e007014. [Google Scholar] [CrossRef] [PubMed]
- Timmis, A.; Townsend, N.; Gale, C.; Grobbee, R.; Maniadakis, N.; Flather, M.; Wilkins, E.; Wright, L.; Vos, R.; Bax, J.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2017. Eur. Heart J. 2018, 39, 508–579. [Google Scholar] [CrossRef] [PubMed]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N.; et al. The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, L.W.E.; Wickramasinghe, K.; Bhatnagar, P.; Leal, J.; Luengo-Fernandez, R.; Burns, R.; Rayner, M.; Townsend, N. European Cardiovascular Disease Statistics 2017; European Heart Network, Ed.; European Heart Network: Brussels, Belgium, 2017. [Google Scholar]
- Vedel, I.; Khanassov, V. Transitional Care for Patients with Congestive Heart Failure: A Systematic Review and Meta-Analysis. Ann. Fam. Med. 2015, 13, 562–571. [Google Scholar] [CrossRef]
- Chou, A.; Euloth, T.; Matcho, B.; Pastva, A.M.; Bilderback, A.; Freburger, J.K. Is Discordance between Recommended and Actual Postacute Discharge Setting a Risk Factor for Readmission in Patients with Congestive Heart Failure? J. Am. Heart Assoc. 2021, 10, e020425. [Google Scholar] [CrossRef]
- Retrum, J.H.; Boggs, J.; Hersh, A.; Wright, L.; Main, D.S.; Magid, D.J.; Allen, L.A. Patient-identified factors related to heart failure readmissions. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 171–177. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, C. A Heart Failure Clinic. Eur. Heart J. 2018, 39, 826–828. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Blue, L.; Lang, E.; McMurray, J.J.; Davie, A.P.; McDonagh, T.A.; Murdoch, D.R.; Petrie, M.C.; Connolly, E.; Norrie, J.; Round, C.E.; et al. Randomised controlled trial of specialist nurse intervention in heart failure. BMJ 2001, 323, 715–718. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Blue, L.; Clark, A.L.; Dahlstrom, U.; Ekman, I.; Lainscak, M.; McDonald, K.; Ryder, M.; Stromberg, A.; Jaarsma, T.; et al. European Society of Cardiology Heart Failure Association Standards for delivering heart failure care. Eur. J. Heart Fail. 2011, 13, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Bhat, S.; Kansal, M.; Kondos, G.T.; Groo, V. Outcomes of a Pharmacist-Managed Heart Failure Medication Titration Assistance Clinic. Ann. Pharmacother. 2018, 52, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Keeney, T.; Lee, M.K.; Basford, J.R.; Cheville, A. Association of Function, Symptoms, and Social Support Reported in Standardized Outpatient Clinic Questionnaires with Subsequent Hospital Discharge Disposition and 30-Day Readmissions. Arch. Phys. Med. Rehabil. 2022, 103, 2383–2390. [Google Scholar] [CrossRef] [PubMed]
- Dorsch, M.P.; Farris, K.B.; Rowell, B.E.; Hummel, S.L.; Koelling, T.M. The Effects of the ManageHF4Life Mobile App on Patients with Chronic Heart Failure: Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e26185. [Google Scholar] [CrossRef]
- Liu, S.; Xiong, X.Y.; Chen, H.; Liu, M.D.; Wang, Y.; Yang, Y.; Zhang, M.J.; Xiang, Q. Transitional Care in Patients with Heart Failure: A Concept Analysis Using Rogers’ Evolutionary Approach. Risk Manag. Healthc. Policy 2023, 16, 2063–2076. [Google Scholar] [CrossRef]
- Lecoeur, E.; Domeng, O.; Fayol, A.; Jannot, A.S.; Hulot, J.S. Epidemiology of heart failure in young adults: A French nationwide cohort study. Eur. Heart J. 2023, 44, 383–392. [Google Scholar] [CrossRef]
- Marques, I.; Abreu, S.; Bertao, M.V.; Ferreira, B.; Ramos, R.L.; Lopes, J.; Nunes, S.; Mendonca, D.; Teixeira, L. Characteristics and outcomes of heart failure hospitalization before implementation of a heart failure clinic: The PRECIC study. Rev. Port. Cardiol. 2017, 36, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Daubert, M.A.; Adams, K.; Yow, E.; Barnhart, H.X.; Douglas, P.S.; Rimmer, S.; Norris, C.; Cooper, L.; Leifer, E.; Desvigne-Nickens, P.; et al. NT-proBNP Goal Achievement Is Associated with Significant Reverse Remodeling and Improved Clinical Outcomes in HFrEF. JACC Heart Fail. 2019, 7, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Savarese, G.; Hage, C.; Orsini, N.; Dahlstrom, U.; Perrone-Filardi, P.; Rosano, G.M.; Lund, L.H. Reductions in N-Terminal Pro-Brain Natriuretic Peptide Levels Are Associated with Lower Mortality and Heart Failure Hospitalization Rates in Patients with Heart Failure with Mid-Range and Preserved Ejection Fraction. Circ. Heart Fail. 2016, 9, e003105. [Google Scholar] [CrossRef] [PubMed]
- Kewcharoen, J.; Trongtorsak, A.; Thangjui, S.; Kanitsoraphan, C.; Prasitlumkum, N. Female Gender Is Associated with an Increased Left Ventricular Ejection Fraction Recovery in Patients with Heart Failure with Reduced Ejection Fraction. Med. Sci. 2022, 10, 21. [Google Scholar] [CrossRef]
- Chung, A.K.; Das, S.R.; Leonard, D.; Peshock, R.M.; Kazi, F.; Abdullah, S.M.; Canham, R.M.; Levine, B.D.; Drazner, M.H. Women have higher left ventricular ejection fractions than men independent of differences in left ventricular volume: The Dallas Heart Study. Circulation 2006, 113, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Ghali, J.K.; Krause-Steinrauf, H.J.; Adams, K.F.; Khan, S.S.; Rosenberg, Y.D.; Yancy, C.W.; Young, J.B.; Goldman, S.; Peberdy, M.A.; Lindenfeld, J. Gender differences in advanced heart failure: Insights from the BEST study. J. Am. Coll. Cardiol. 2003, 42, 2128–2134. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Packer, M. How Should We Sequence the Treatments for Heart Failure and a Reduced Ejection Fraction? A Redefinition of Evidence-Based Medicine. Circulation 2021, 143, 875–877. [Google Scholar] [CrossRef] [PubMed]
- Straw, S.; McGinlay, M.; Witte, K.K. Four pillars of heart failure: Contemporary pharmacological therapy for heart failure with reduced ejection fraction. Open Heart 2021, 8, e001585. [Google Scholar] [CrossRef]
- Brennan, E.J. Chronic heart failure nursing: Integrated multidisciplinary care. Br. J. Nurs. 2018, 27, 681–688. [Google Scholar] [CrossRef]
- Pant, B.P.; Satheesh, S.; Pillai, A.A.; Anantharaj, A.; Ramamoorthy, L.; Selvaraj, R. Outcomes with heart failure management in a multidisciplinary clinic—A randomized controlled trial. Indian Heart J. 2022, 74, 327–331. [Google Scholar] [CrossRef]
- Peri-Okonny, P.A.; Mi, X.; Khariton, Y.; Patel, K.K.; Thomas, L.; Fonarow, G.C.; Sharma, P.P.; Duffy, C.I.; Albert, N.M.; Butler, J.; et al. Target Doses of Heart Failure Medical Therapy and Blood Pressure: Insights From the CHAMP-HF Registry. JACC Heart Fail. 2019, 7, 350–358. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | n = 54 |
|---|---|
| Sex, n (%) | |
| Female | 16 (29.6%) |
| Male | 38 (70.4%) |
| Age (years), median (P25; P75) | 62 (51; 71) |
| EF (%), median (IQR) | 28 (23; 34) |
| ≤40%, n (%) | 52 (96.3%) |
| 41–49%, n (%) | 2 (3.7%) |
| NT-proBNP (pg/mL), median (P25; P75) | 2552 (895; 29,726) |
| Patient origin, n (%) | |
| Hospitalization | 24 (44.4%) |
| Cardiology outpatient consultation | 20 (37.0%) |
| Emergency department | 10 (18.5%) |
| Etiology, n (%) | |
| Ischemic disease | 12 (22.2%) |
| Non-ischemic disease | 42 (77.8%) |
| Consultations (number), median (P25; P75) | 4 (3; 5) |
| Follow-up time (months), median (P25; P75) | 7 (4; 10) |
| Medication for HF Management | n = 54 |
|---|---|
| BB, n (%) | 50 (92.6%) |
| Reached the target dose | 4 (7.4%) |
| MRA, n (%) | 44 (81.5%) |
| Reached the target dose | 8 (14.8%) |
| ACEi/ARB, n (%) | 28 (51.9%) |
| Reached the target dose | 8 (14.8%) |
| ARNI, n (%) | 21 (38.9%) |
| Reached the target dose | 10 (18.5%) |
| EF at Follow-Up (n, %) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| ≤40% | 41–49% | ≥50% | Total | ||||||
| EF at baseline (n, %) | ≤40% | 23 | 59.0% | 11 | 28.2% | 4 | 10.3% | 38 | 97.4% |
| 41–49% | 0 | 0% | 1 | 2.6% | 0 | 0% | 1 | 2.6% | |
| Total | 23 | 59.0% | 12 | 30.8% | 4 | 10.3% | 39 | 100% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousa, O.; Ponte, M.; Caeiro, D.; Pereira, E.; Silva, M.; Pestana, S.; Braga, P.; Fontes-Carvalho, R. Excellence in Heart Failure: A Multidisciplinary Program on Heart Failure Management for Improved Patient Outcome. Hearts 2024, 5, 1-13. https://doi.org/10.3390/hearts5010001
Sousa O, Ponte M, Caeiro D, Pereira E, Silva M, Pestana S, Braga P, Fontes-Carvalho R. Excellence in Heart Failure: A Multidisciplinary Program on Heart Failure Management for Improved Patient Outcome. Hearts. 2024; 5(1):1-13. https://doi.org/10.3390/hearts5010001
Chicago/Turabian StyleSousa, Olga, Marta Ponte, Daniel Caeiro, Eulália Pereira, Marisa Silva, Sandra Pestana, Pedro Braga, and Ricardo Fontes-Carvalho. 2024. "Excellence in Heart Failure: A Multidisciplinary Program on Heart Failure Management for Improved Patient Outcome" Hearts 5, no. 1: 1-13. https://doi.org/10.3390/hearts5010001