

Screwed Monolithic Zirconia Crowns for Mono-Implant Posterior Rehabilitation: A Prospective Clinical Study on 41 Patients with a 7-Year Follow-Up

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Sampling
2.2. Inclusion Criteria
- Patients with monolithic zirconia single crowns in posterior sectors;
- Crowns screwed on the implant abutment;
- Good oral hygiene;
- No temporomandibular disorders;
- Absence of systemic diseases that contraindicate minor oral surgery.
2.3. Exclusion Criteria
- Poor oral hygiene;
- Severe periodontal disease;
- Parafunctions;
- Presence of temporomandibular disorder;
- Systemic disease that contraindicates the surgical placement of implant;
- Patients who do not complete the follow-up period.
2.4. Operative Protocol
- Initial evaluation: anamnesis, panoramic radiograph, and eventual targeted intraoral radiograms, and when necessary, CT or CBCT; preliminary impression by irreversible hydrocolloid impression material (Alginate—Kromopan LASCOD, Sesto Fiorentino, Italy) and analysis of the study models.
- Surgical procedure: after local anesthesia, a full-thickness flap was elevated, and the implant (Neoss-ProActive Straight, Neoss-ProActive Tapered, Milano, Italy) was inserted according to the actual guidelines about operating protocol and direct closure of the implant site with cover screw application.
- Exposure of the cover screw and substitution with the healing abutment after 4 months.
- After 7 days, polyether impression of the implant fixture with individual tray (Impregum™, Saint Paul, MN, USA).
- The temporary crown of acrylic resin (PMMA) is applied and screwed onto the fixture with a temporary titanium abutment.
- Positioning of the second PMMA prototype for an appropriate functional and aesthetic evaluation of the emergence profile, with articulation paper use (8-μm aluminum Shimstock, Coltène, Altstätten, Switzerland) to detect premature contacts and interference during centric and eccentric mandibular movements. Aesthetic evaluation in regard to morphology and color using the Easyshade® Compact (VITA® North America, Yorba Linda, CA, USA) spectrophotometer.
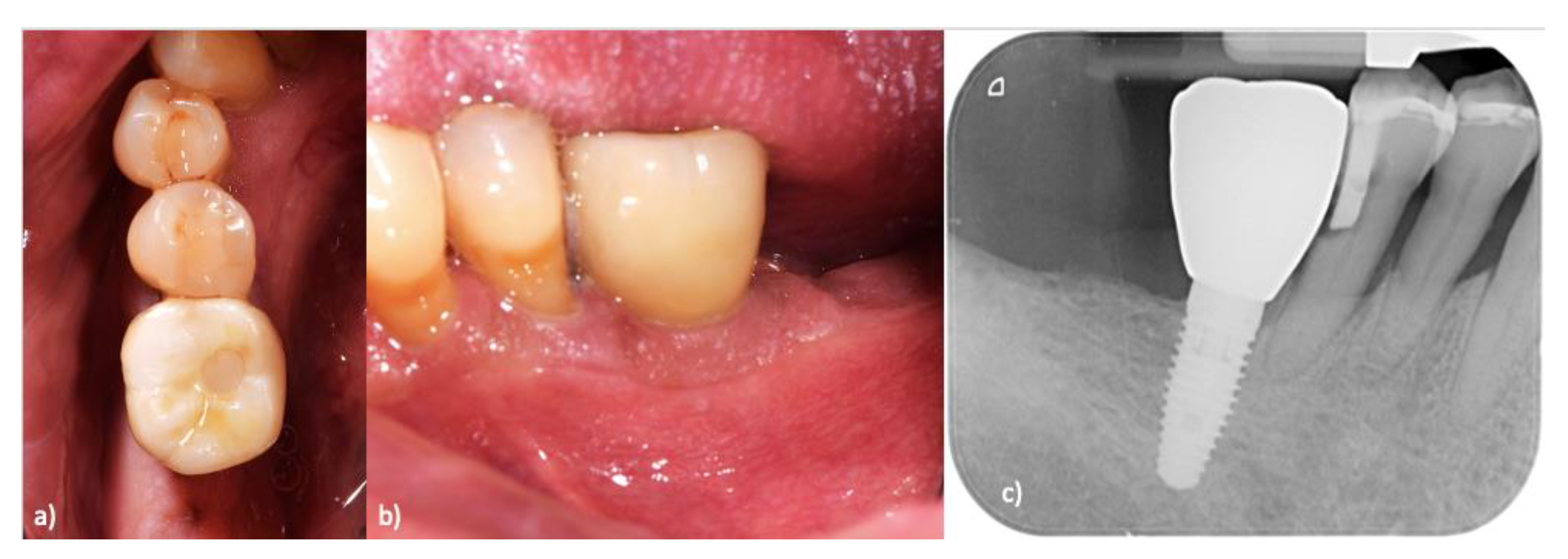
- Positioning the “raw” prosthetic product in 5Y-PSZ Zirconia Biodynamic Zirconium Multilayer 1200/600 Mpa Progressive (Biodynamic, Correggio, Italy) assessing morphological checks and functional adaptation.
- Bonding on the definitive prosthetic abutment.
- Final decontamination of the fixture and application of the crown with 40 N of screwing force.
- Closure of the access hole with Teflon and flow composite resin (Versite Flow Composite, Kerr Dental, Orange, CA, USA).
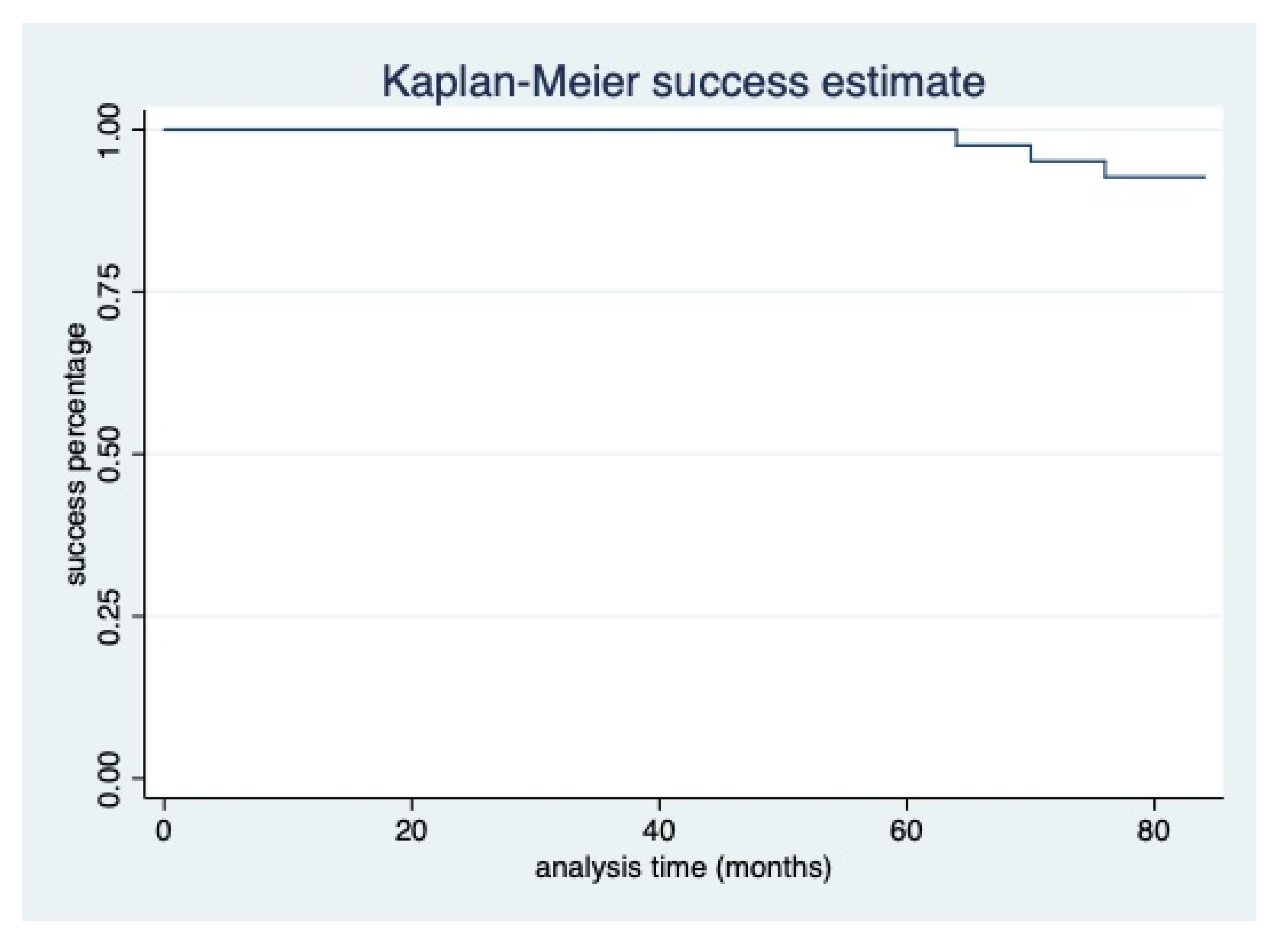
- Clinical follow-up visits at 1, 3, 6, and 12 months, and annual check-ups were performed for the following 6 years.
2.5. Clinical Evaluation
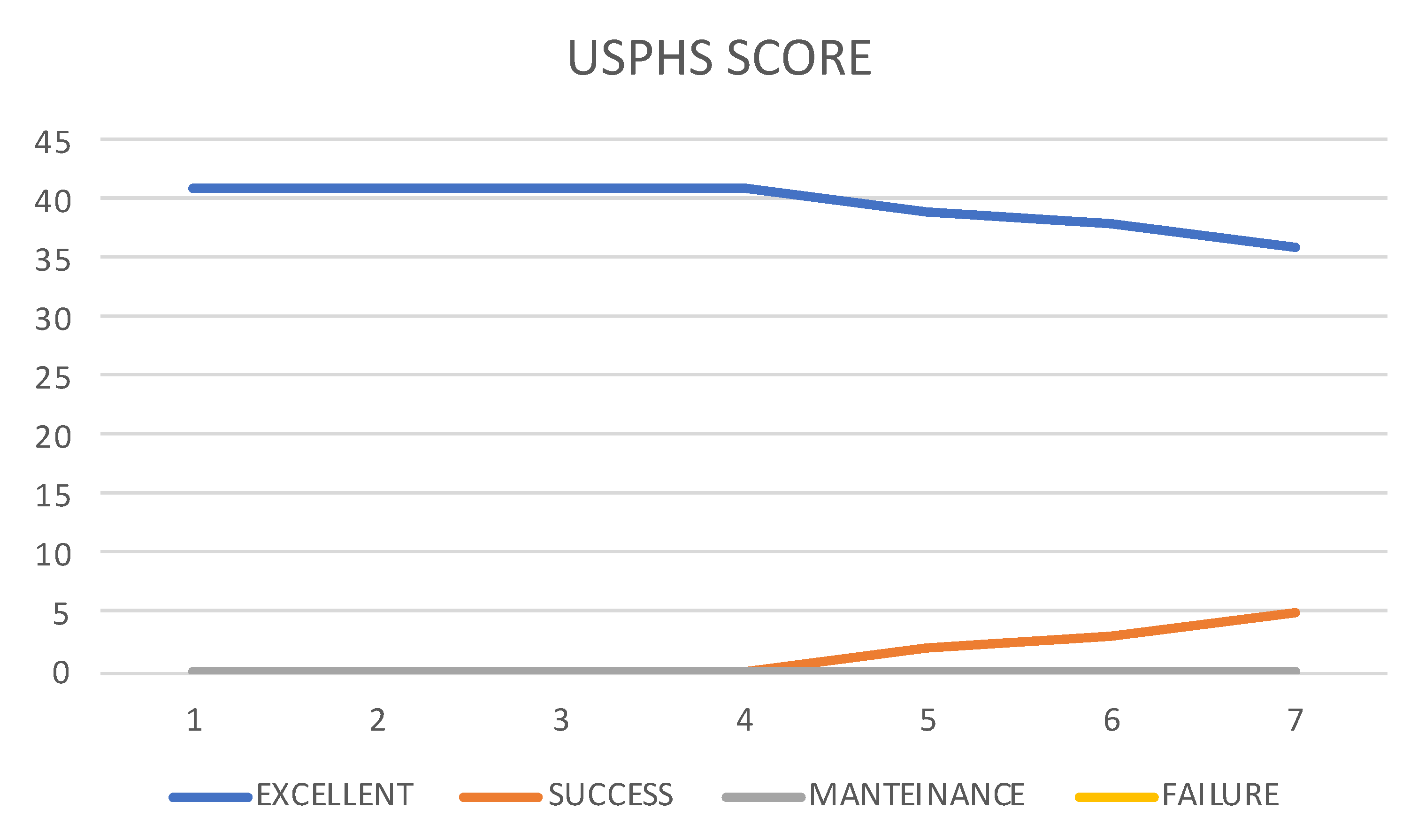
- “EXCELLENT” if the restoration has only “a” score;
- “SUCCESS” if the restoration has at least a “b” score;
- “MAINTENANCE” if the restoration has at least a “c” score;
- “FAILURE” if the restoration has at least a “d” score or the presence of non-correctable adversity.
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Limones, A.; Molinero-Mourelle, P.; Azevedo, L.; Romeo-Rubio, M.; Correia, A.; Gómez-Polo, M. Zirconia-Ceramic versus Metal-Ceramic Posterior Multiunit Tooth-Supported Fixed Dental Prostheses. J. Am. Dent. Assoc. 2020, 151, 230–238.e7. [Google Scholar] [CrossRef]
- Zhang, Y.; Lawn, B.R. Novel Zirconia Materials in Dentistry. J. Dent. Res. 2018, 97, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Stawarczyk, B.; Emslander, A.; Roos, M.; Sener, B.; Noack, F.; Keul, C. Zirconia Ceramics, Their Contrast Ratio and Grain Size Depending on Sintering Parameters. Dent. Mater. J. 2014, 33, 591–598. [Google Scholar] [CrossRef]
- Ban, S. Chemical Durability of High Translucent Dental Zirconia. Dent. Mater. J. 2020, 39, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Kuwajima, H.; Masaki, T. Phase Change and Mechanical Properties of ZrO2-Y2O3 Solid Electrolyte after Ageing. Solid. State Ion. 1981, 3–4, 489–493. [Google Scholar] [CrossRef]
- De Angelis, P.; Gasparini, G.; Rella, E.; De Angelis, S.; Grippaudo, C.; D’Addona, A.; Manicone, P.F. Patient Satisfaction with Implant-Supported Monolithic and Partially Veneered Zirconia Restorations. BioMed Res. Int. 2021, 2021, 6692939. [Google Scholar] [CrossRef]
- Tabatabaian, F. Color Aspect of Monolithic Zirconia Restorations: A Review of the Literature. J. Prosthodont. 2019, 28, 276–287. [Google Scholar] [CrossRef]
- Kim, W.; Li, X.C.; Bidra, A.S. Clinical Outcomes of Implant-Supported Monolithic Zirconia Crowns and Fixed Partial Dentures: A Systematic Review. J. Prosthodont. 2023, 32, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Nardi, D.; Gianluca, S.; Piattelli, A. The Conometric Concept: A 5-Year Follow-up of Fixed Partial Monolithic Zirconia Restorations Supported by Cone-in-Cone Abutments. Int. J. Periodontics Restor. Dent. 2018, 38, 363–371. [Google Scholar] [CrossRef]
- Diéguez-Pereira, M.; Chávarri-Prado, D.; Estrada-Martínez, A.; Pérez-Pevida, E.; Brizuela-Velasco, A. Monolithic and Minimally Veneered Zirconia Complications as Implant-Supported Restorative Material: A Retrospective Clinical Study up to 5 Years. BioMed Res. Int. 2020, 2020, 8821068. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Valente, N.A.; Strasding, M.; Zwahlen, M.; Liu, S.; Sailer, I. A Systematic Review of the Survival and Complication Rates of Zirconia-Ceramic and Metal-Ceramic Single Crowns. Clin. Oral Implant. Res. 2018, 29, 199–214. [Google Scholar] [CrossRef] [PubMed]
- Koenig, V.; Wulfman, C.; Bekaert, S.; Dupont, N.; Le Goff, S.; Eldafrawy, M.; Vanheusden, A.; Mainjot, A. Clinical Behavior of Second-Generation Zirconia Monolithic Posterior Restorations: Two-Year Results of a Prospective Study with Ex Vivo Analyses Including Patients with Clinical Signs of Bruxism. J. Dent. 2019, 91, 103229. [Google Scholar] [CrossRef] [PubMed]
- Laumbacher, H.; Strasser, T.; Knüttel, H.; Rosentritt, M. Long-Term Clinical Performance and Complications of Zirconia-Based Tooth- and Implant-Supported Fixed Prosthodontic Restorations: A Summary of Systematic Reviews. J. Dent. 2021, 111, 103723. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.H.; Guo, D.N.; Zhou, Y.S.; Pan, S.X. Clinical outcome of single posterior implant-supported monolithic zirconia crowns fabricated using full digital workflow and conventional workflow: A 3-year follow-up. Zhonghua Kou Qiang Yi Xue Za Zhi 2022, 57, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Hardan, L.; Mancino, D.; Bourgi, R.; Cuevas-Suárez, C.E.; Lukomska-Szymanska, M.; Zarow, M.; Jakubowicz, N.; Zamarripa-Calderón, J.E.; Kafa, L.; Etienne, O.; et al. Treatment of Tooth Wear Using Direct or Indirect Restorations: A Systematic Review of Clinical Studies. Bioengineering 2022, 9, 346. [Google Scholar] [CrossRef]
- Zarone, F.; Di Mauro, M.I.; Spagnuolo, G.; Gherlone, E.; Sorrentino, R. Fourteen-Year Evaluation of Posterior Zirconia-Based Three-Unit Fixed Dental Prostheses: A Prospective Clinical Study of All Ceramic Prosthesis. J. Dent. 2020, 101, 103419. [Google Scholar] [CrossRef]
- Monaco, C.; Caldari, M.; Scotti, R.; AIOP (Italian Academy of Prosthetic Dentistry). Clinical Research Group Clinical Evaluation of Zirconia-Based Restorations on Implants: A Retrospective Cohort Study from the AIOP Clinical Research Group. Int. J. Prosthodont. 2015, 28, 239–242. [Google Scholar] [CrossRef]
- Weigl, P.; Saarepera, K.; Hinrikus, K.; Wu, Y.; Trimpou, G.; Lorenz, J. Screw-Retained Monolithic Zirconia vs. Cemented Porcelain-Fused-to-Metal Implant Crowns: A Prospective Randomized Clinical Trial in Split-Mouth Design. Clin. Oral. Invest. 2019, 23, 1067–1075. [Google Scholar] [CrossRef]
- Kraus, R.D.; Epprecht, A.; Hämmerle, C.H.F.; Sailer, I.; Thoma, D.S. Cemented vs Screw-Retained Zirconia-Based Single Implant Reconstructions: A 3-Year Prospective Randomized Controlled Clinical Trial. Clin. Implant. Dent. Relat. Res. 2019, 21, 578–585. [Google Scholar] [CrossRef]
- Spies, B.C.; Witkowski, S.; Vach, K.; Kohal, R.-J. Clinical and Patient-Reported Outcomes of Zirconia-Based Implant Fixed Dental Prostheses: Results of a Prospective Case Series 5 Years after Implant Placement. Clin. Oral. Implant. Res. 2018, 29, 91–99. [Google Scholar] [CrossRef]
- Worni, A.; Katsoulis, J.; Kolgeci, L.; Worni, M.; Mericske-Stern, R. Monolithic Zirconia Reconstructions Supported by Teeth and Implants: 1- to 3-Year Results of a Case Series. Quintessence Int. 2017, 48, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Korsch, M.; Walther, W. Retrospective Analysis of Loosening of Cement-Retained vs Screw-Retained Fixed Implant-Supported Reconstructions. Quintessence Int. 2015, 46, 583–589. [Google Scholar] [CrossRef]
- Lerner, H.; Mouhyi, J.; Admakin, O.; Mangano, F. Artificial Intelligence in Fixed Implant Prosthodontics: A Retrospective Study of 106 Implant-Supported Monolithic Zirconia Crowns Inserted in the Posterior Jaws of 90 Patients. BMC Oral. Health 2020, 20, 80. [Google Scholar] [CrossRef] [PubMed]
- Donker, V.J.J.; Raghoebar, G.M.; Jensen-Louwerse, C.; Vissink, A.; Meijer, H.J.A. Monolithic Zirconia Single Tooth Implant-Supported Restorations with CAD/CAM Titanium Abutments in the Posterior Region: A 1-Year Prospective Case Series Study. Clin. Implant. Dent. Relat. Res. 2022, 24, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, I.; Trikka, D.; Gasparatos, S.; Mitsias, M.E. Clinical Outcomes of Monolithic Zirconia Crowns with CAD/CAM Technology. A 1-Year Follow-Up Prospective Clinical Study of 65 Patients. Int. J. Environ. Res. Public. Health 2018, 15, 2523. [Google Scholar] [CrossRef]
- Pol, C.W.; Raghoebar, G.M.; Cune, M.S.; Meijer, H.J. Implant-Supported Three-Unit Fixed Dental Prosthesis Using Coded Healing Abutments and Fabricated Using a Digital Workflow: A 1-Year Prospective Case Series Study. Int. J. Prosthodont. 2020, 33, 609–619. [Google Scholar] [CrossRef]
- Kheur, M.; Lakha, T.; Shaikh, S.; Kheur, S.; Qamri, B.; Zhen, L.W.; Al-Haj Husain, N.; Özcan, M. A Comparative Study on Simulated Chairside Grinding and Polishing of Monolithic Zirconia. Materials 2022, 15, 2202. [Google Scholar] [CrossRef]
- Yang, H.; Xu, Y.-L.; Hong, G.; Yu, H. Effects of Low-Temperature Degradation on the Surface Roughness of Yttria-Stabilized Tetragonal Zirconia Polycrystal Ceramics: A Systematic Review and Meta-Analysis. J. Prosthet. Dent. 2021, 125, 222–230. [Google Scholar] [CrossRef]
- De Matteis, V.; Cascione, M.; Toma, C.C.; Albanese, G.; De Giorgi, M.L.; Corsalini, M.; Rinaldi, R. Silver Nanoparticles Addition in Poly(Methyl Methacrylate) Dental Matrix: Topographic and Antimycotic Studies. IJMS 2019, 20, 4691. [Google Scholar] [CrossRef]
- Dutra, D.; Pereira, G.; Kantorski, K.Z.; Exterkate, R.; Kleverlaan, C.J.; Valandro, L.F.; Zanatta, F.B. Grinding with Diamond Burs and Hydrothermal Aging of a Y-TZP Material: Effect on the Material Surface Characteristics and Bacterial Adhesion. Oper. Dent. 2017, 42, 669–678. [Google Scholar] [CrossRef]
- Mühlemann, S.; Lakha, T.; Jung, R.E.; Hämmerle, C.H.F.; Benic, G.I. Prosthetic Outcomes and Clinical Performance of CAD-CAM Monolithic Zirconia versus Porcelain-fused-to-metal Implant Crowns in the Molar Region: 1-year Results of a RCT. Clin. Oral. Impl Res. 2020, 31, 856–864. [Google Scholar] [CrossRef]
- Herpel, C.; Rammelsberg, P.; Rues, S.; Zenthöfer, A.; Seceleanu, I.; Corcodel, N. Color Stability of Individually Stained Monolithic Zirconia Following Occlusal Adjustment. J. Esthet. Restor. Dent. 2021, 33, 387–393. [Google Scholar] [CrossRef]
- Pieralli, S.; Kohal, R.J.; Jung, R.E.; Vach, K.; Spies, B.C. Clinical Outcomes of Zirconia Dental Implants: A Systematic Review. J. Dent. Res. 2017, 96, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Kolgeci, L.; Mericske, E.; Worni, A.; Walker, P.; Katsoulis, J.; Mericske-Stern, R. Technical Complications and Failures of Zirconia-Based Prostheses Supported by Implants Followed Up to 7 Years: A Case Series. Int. J. Prosthodont. 2014, 27, 544–552. [Google Scholar] [CrossRef]
- Moscovitch, M. Consecutive Case Series of Monolithic and Minimally Veneered Zirconia Restorations on Teeth and Implants: Up to 68 Months. Int. J. Periodontics Restor. Dent. 2015, 35, 315–323. [Google Scholar] [CrossRef]
- Cascione, M.; De Matteis, V.; Pellegrino, P.; Albanese, G.; De Giorgi, M.L.; Paladini, F.; Corsalini, M.; Rinaldi, R. Improvement of PMMA Dental Matrix Performance by Addition of Titanium Dioxide Nanoparticles and Clay Nanotubes. Nanomaterials 2021, 11, 2027. [Google Scholar] [CrossRef] [PubMed]
- Assenza, B.; Artese, L.; Scarano, A.; Rubini, C.; Perrotti, V.; Piattelli, M.; Thams, U.; San Roman, F.; Piccirilli, M.; Piattelli, A. Screw vs Cement-Implant-Retained Restorations: An Experimental Study in the Beagle. Part 2. Immunohistochemical Evaluation of the Peri-Implant Tissues. J. Oral. Implantol. 2006, 32, 1–7. [Google Scholar] [CrossRef]
- Wittneben, J.-G.; Joda, T.; Weber, H.-P.; Brägger, U. Screw Retained vs. Cement Retained Implant-Supported Fixed Dental Prosthesis. Periodontol. 2000 2017, 73, 141–151. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| USPHS CRITERIA | ||||
|---|---|---|---|---|
| Alpha (A) | Bravo (B) | Charlie (C) | Delta (D) | |
| MARGINAL ADAPTION | No visible crack or penetration of the probe | Visible crack but no penetration of the probe | Visible crack and probe penetration | Restoration must be replaced |
| SURFACE ROUGHNESS | Polished surface, no roughness | Slight roughness, not detectable with saliva film | Moderate roughness, detectable even with saliva film | Restoration must be replaced |
| COLOR MATCHING | No mismatch Perfect integration | Mismatch < 1 grade of Vita shades | Mismatch > 1 grade of Vita shades | Restoration must be replaced |
| ANATOMIC MORPHOLOGY | Natural and physiological anatomy | Unnatural anatomy | Loss of important anatomical structure | Restoration must be replaced |
| FRACTURE | No fracture | Minor fracture (polishable) | Major fracture (not polishable) | Restoration must be replaced |
| LOCALIZATION | |||
|---|---|---|---|
| REGION | Maxilla | Mandible | |
| TOOTH | Premolar | Molar | |
| SEX | Male | Female | |
| ANTAGONIST ELEMENT | Natural teeth | Prosthetic | Denture |
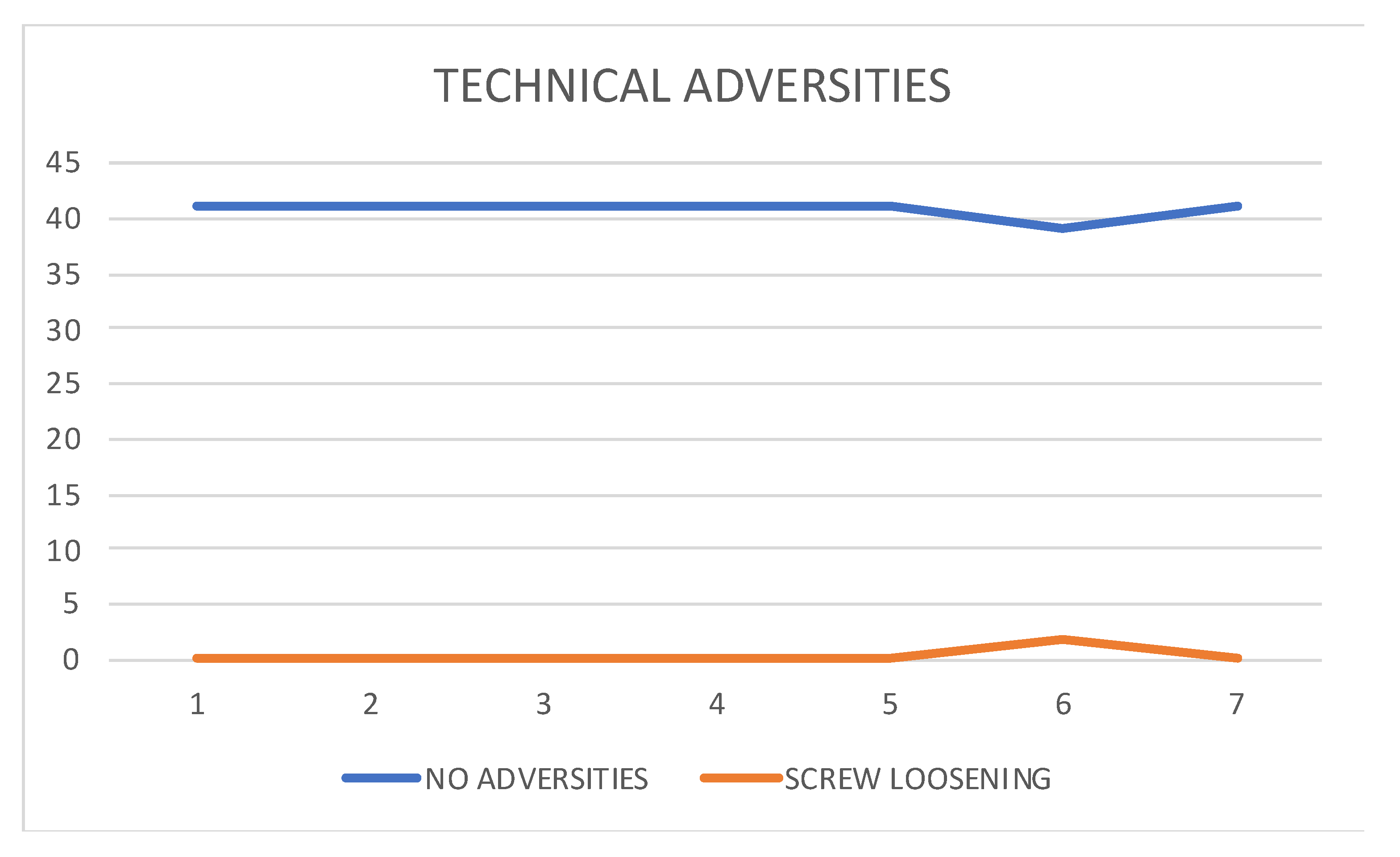
| TECHNICAL ADVERSITIES | Reparable | Irreparable |
|---|---|---|
| Debonding crown abutment | ||
| Screw loosening | ||
| Implant failure | ||
| Drop-out |
| USPHS Score Per Years | Marginal Adaption | Surface Roughness | Color Match | Anatomy | Fracture | Total |
|---|---|---|---|---|---|---|
| 1 Year | ||||||
| A | 41 | 41 | 41 | 41 | 41 | 41 |
| B | 0 | |||||
| 2 Year | ||||||
| A | 41 | 41 | 41 | 41 | 41 | 41 |
| B | 0 | |||||
| 3 Year | ||||||
| A | 41 | 41 | 41 | 41 | 41 | 41 |
| B | 0 | |||||
| 4 Year | ||||||
| A | 41 | 41 | 41 | 41 | 41 | 41 |
| B | 0 | |||||
| 5 Year | ||||||
| A | 41 | 39 | 41 | 41 | 41 | 39 |
| B | 2 | 2 | ||||
| 6 Year | ||||||
| A | 41 | 38 | 41 | 41 | 41 | 38 |
| B | 3 | 3 | ||||
| 7 Year | ||||||
| A | 41 | 37 | 40 | 41 | 41 | 36 |
| B | 4 | 1 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barile, G.; Capodiferro, S.; De Rosa, G.; Muci, G.; Vanzanelli, A.; Corsalini, M. Screwed Monolithic Zirconia Crowns for Mono-Implant Posterior Rehabilitation: A Prospective Clinical Study on 41 Patients with a 7-Year Follow-Up. Prosthesis 2023, 5, 1037-1048. https://doi.org/10.3390/prosthesis5040072
Barile G, Capodiferro S, De Rosa G, Muci G, Vanzanelli A, Corsalini M. Screwed Monolithic Zirconia Crowns for Mono-Implant Posterior Rehabilitation: A Prospective Clinical Study on 41 Patients with a 7-Year Follow-Up. Prosthesis. 2023; 5(4):1037-1048. https://doi.org/10.3390/prosthesis5040072
Chicago/Turabian StyleBarile, Giuseppe, Saverio Capodiferro, Giovanni De Rosa, Giovannino Muci, Alessandro Vanzanelli, and Massimo Corsalini. 2023. "Screwed Monolithic Zirconia Crowns for Mono-Implant Posterior Rehabilitation: A Prospective Clinical Study on 41 Patients with a 7-Year Follow-Up" Prosthesis 5, no. 4: 1037-1048. https://doi.org/10.3390/prosthesis5040072