
Effects of Customized 3D-Printed Insoles in Patients with Foot-Related Musculoskeletal Ailments—A Survey-Based Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Requirement
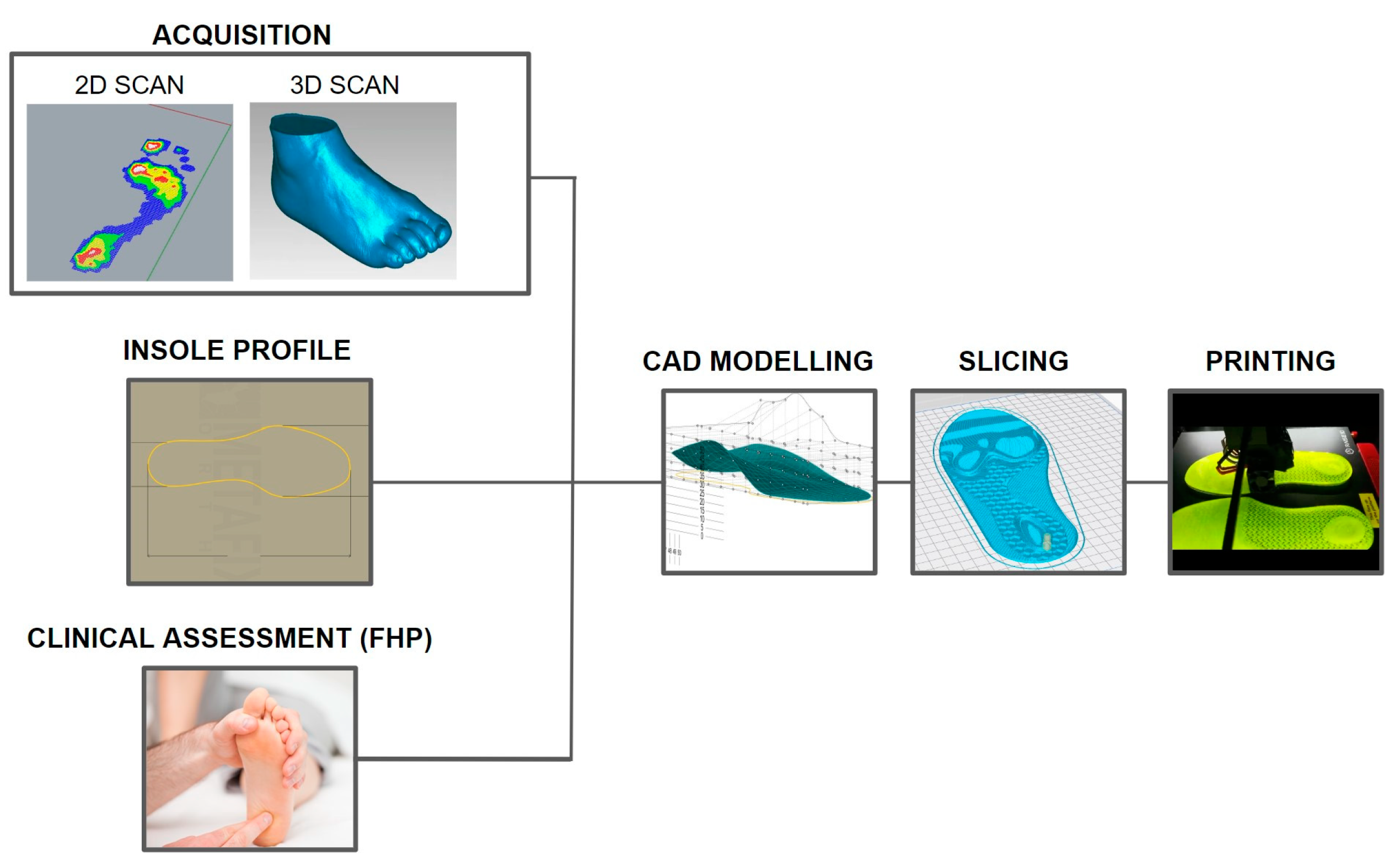
2.2. Insole Design and Development
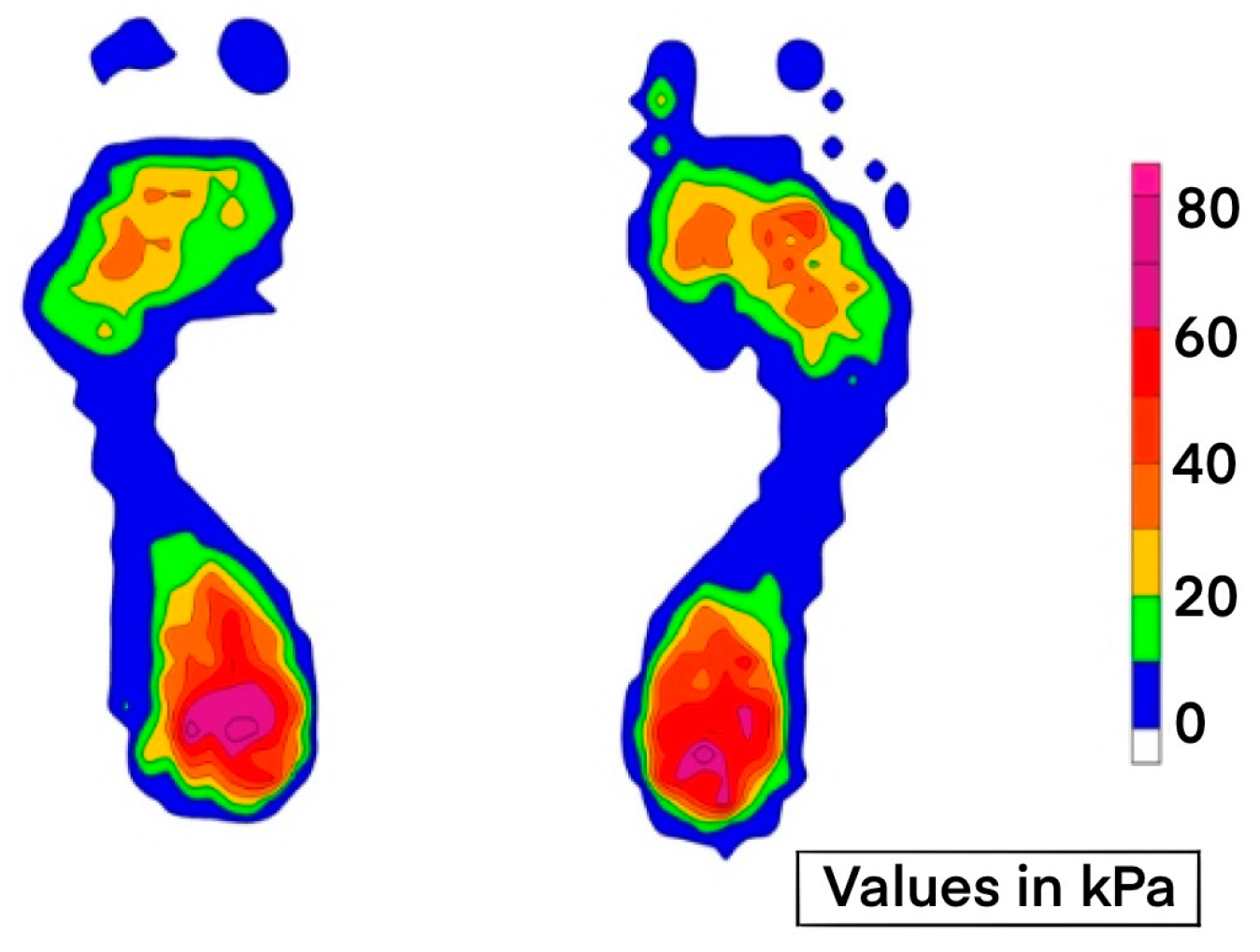
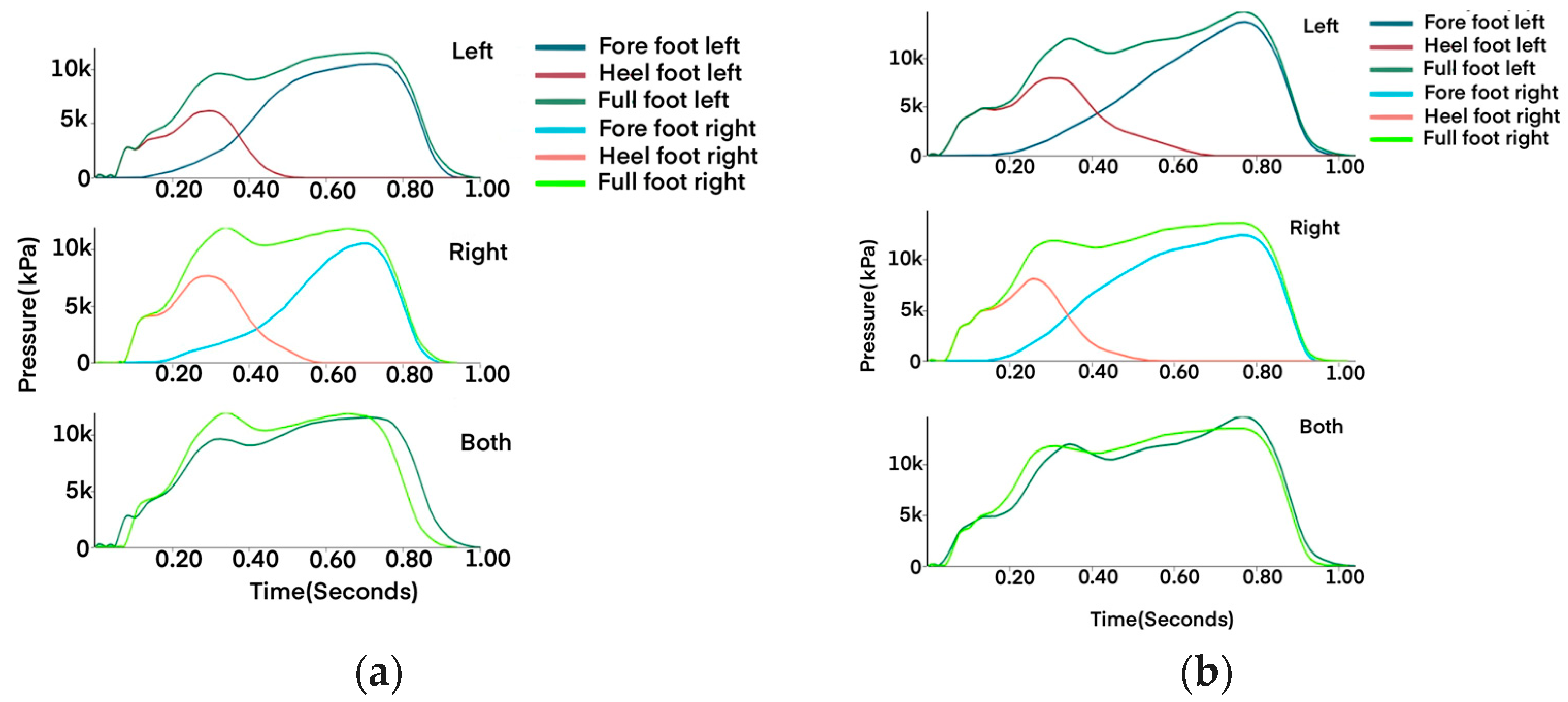
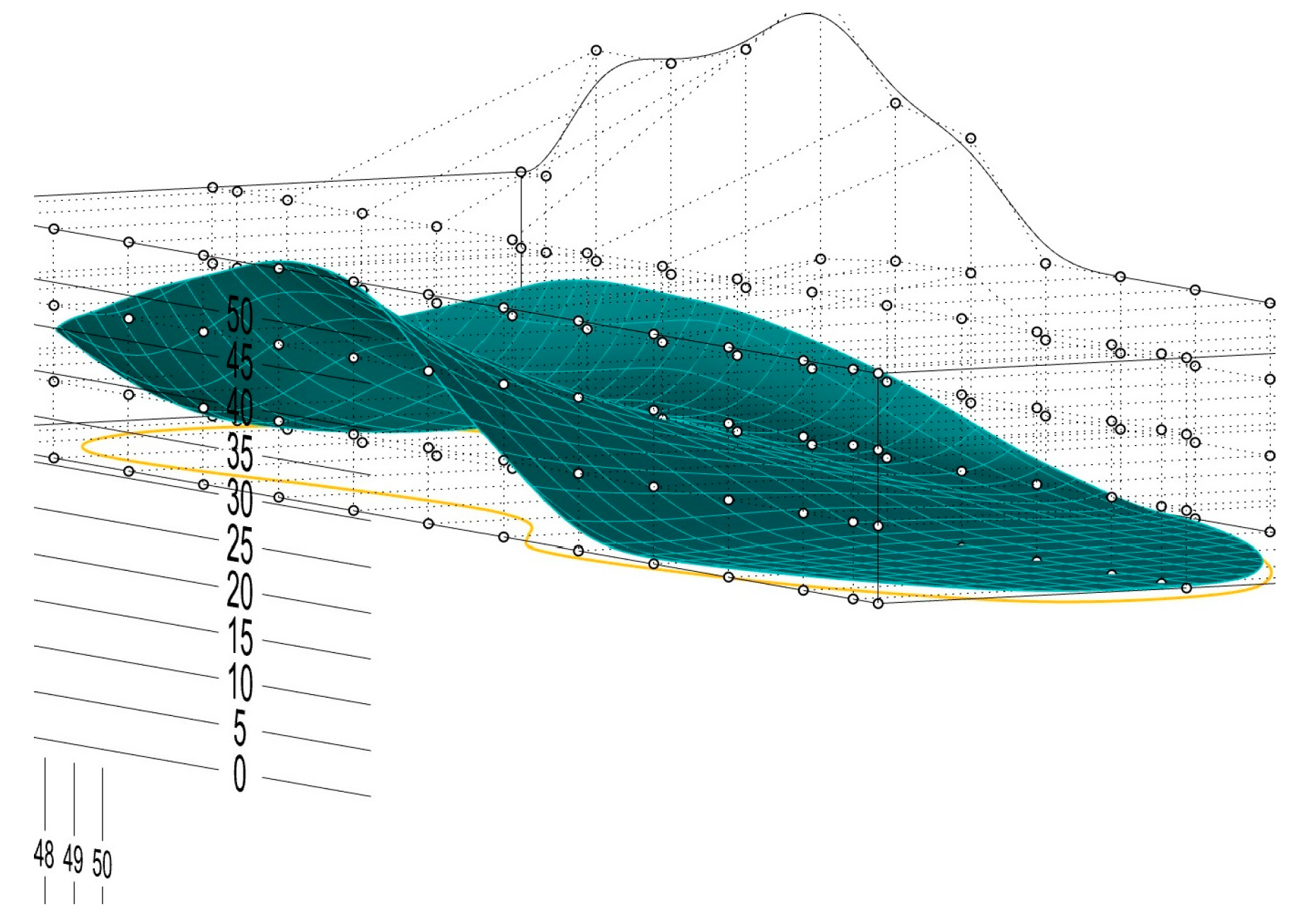
2.2.1. Foot Scan and Acquisition
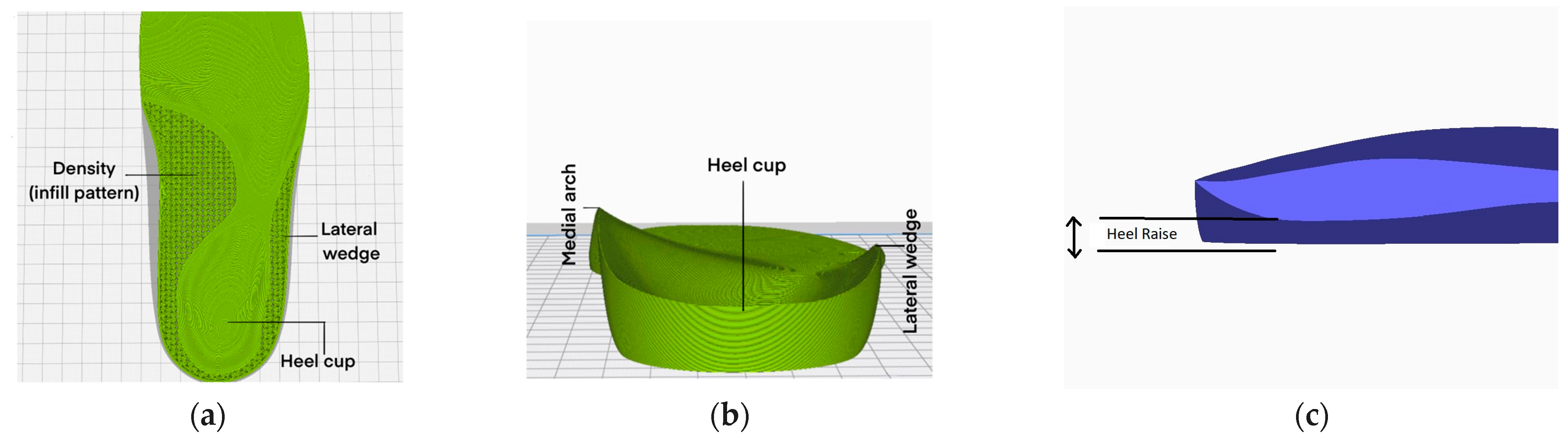
2.2.2. Insole Design
2.2.3. Slicing
2.2.4. Three-Dimensional Printing and Post-Processing
2.3. Tools and Procedure
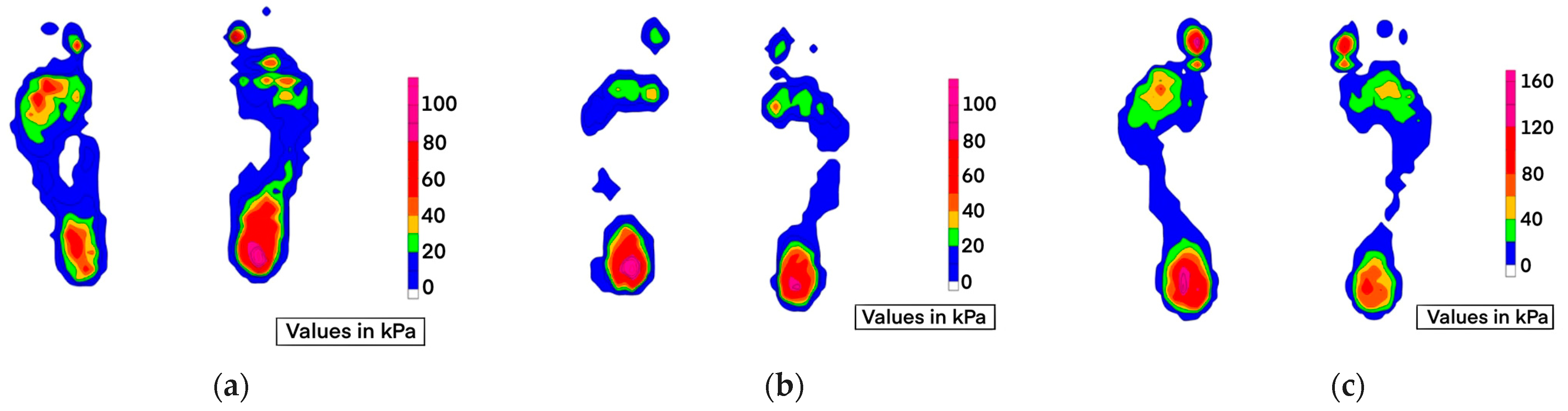
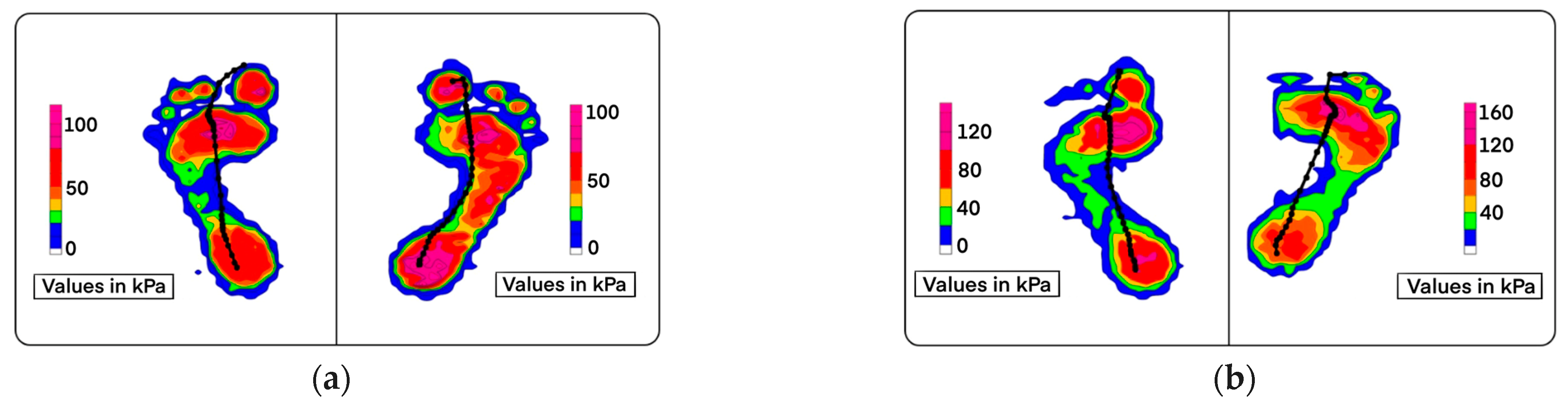
3. Results
3.1. Flat Foot, High Arch
3.2. Diabetic/Neuropathic Foot
3.3. Patients with Joint Pain
4. Discussion
4.1. Limitations
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bonanno, D.; Landorf, K.B.; Munteanu, S.; Murley, G.S.; Menz, H. Effectiveness of foot orthoses and shock-absorbing insoles for the prevention of injury: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, S.; Sumer, E.; Zengin, H.Y.; Bek, N. Intensive physiotherapy versus home-based exercise and custom-made orthotic insoles in patients with plantar fasciitis: Pilot study. Foot 2022, 51, 101906. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Santos, A.; Preece, S.; Nester, C.J. Evaluation of orthotic insoles for people with diabetes who are at-risk of first ulceration. J. Foot Ankle Res. 2019, 12, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerrard, J.M.; Bonanno, D.R.; Whittaker, G.A.; Landorf, K.B. Effect of different orthotic materials on plantar pressures: A systematic review. J. Foot Ankle Res. 2020, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Davia-Aracil, M.; Hinojo-Pérez, J.J.; Jimeno-Morenilla, A.; Mora-Mora, H. 3D printing of functional anatomical insoles. Comput. Ind. 2018, 95, 38–53. [Google Scholar] [CrossRef] [Green Version]
- Ma, Z.; Lin, J.; Xu, X.; Ma, Z.; Tang, L.; Sun, C.; Li, D.; Liu, C.; Zhong, Y.; Wang, L. Design and 3D printing of adjustable modulus porous structures for customized diabetic foot insoles. Int. J. Lightweight Mater. Manuf. 2019, 2, 57–63. [Google Scholar] [CrossRef]
- Jin, H.; Xu, R.; Wang, S.; Wang, J. Use of 3D-Printed Heel Support Insoles Based on Arch Lift Improves Foot Pressure Distribution in Healthy People. Experiment 2019, 25, 7175–7181. [Google Scholar] [CrossRef] [PubMed]
- Yarwindran, M.; Sa’aban, N.A.; Ibrahim, M.; Periyasamy, R. Thermoplastic elastomer infill pattern impact on mechanical properties 3D printed customized orthotic insole. ARPN J. Eng. Appl. Sci. 2016, 11, 6519–6524. [Google Scholar]
- Leal-Junior, A.G.; Díaz, C.R.; Marques, C.; Pontes, M.J.; Frizera, A. 3D-printed POF insole: Development and applications of a low-cost, highly customizable device for plantar pressure and ground reaction forces monitoring. Opt. Laser Technol. 2019, 116, 256–264. [Google Scholar] [CrossRef]
- Zuñiga, J.; Moscoso, M.; Padilla-Huamantinco, P.G.; Lazo-Porras, M.; Tenorio-Mucha, J.; Padilla-Huamantinco, W.; Tincopa, J.P. Development of 3D-Printed Orthopedic Insoles for Patients with Diabetes and Evaluation with Electronic Pressure Sensors. Designs 2022, 6, 95. [Google Scholar] [CrossRef]
- Singh, S.; Mali, H.S. 3D printed orthotic insoles for foot rehabilitation. In 3D Printing in Podiatric Medicine, 1st ed.; Sandhu, K., Singh, S., Eds.; Academic Press: Cambridge, MA, USA, 2023; pp. 211–219. [Google Scholar] [CrossRef]
- Daryabor, A.; Kobayashi, T.; Saeedi, H.; Lyons, S.M.; Maeda, N.; Naimi, S.S. Effect of 3D printed insoles for people with flatfeet: A systematic review. Assist. Technol. 2022, 35, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Xu, R.; Wang, J. The Effects of Short-Term Wearing of Customized 3D Printed Single-Sided Lateral Wedge Insoles on Lower Limbs in Healthy Males: A Randomized Controlled Trial. Experiment 2019, 25, 7720–7727. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jiang, W.; Gan, Y.; Yu, Y.; Dai, K. Clinical Observation of 3D Printing Technology in Insoles for Flexible Flatfoot Patients. J. Shanghai Jiaotong Univ. Sci. 2021, 26, 398–403. [Google Scholar] [CrossRef]
- Jandova, S.; Mendricky, R. Benefits of 3D Printed and Customized Anatomical Footwear Insoles for Plantar Pressure Distribution. 3D Print. Addit. Manuf. 2022, 9, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Wang, C.S.; Lin, K.W.; Chien, M.J.; Wei, S.H.; Chen, C.S. Biomechanical Analysis of the FlatFoot with Different 3D-Printed Insoles on the Lower Extremities. Bioengineering 2022, 9, 563. [Google Scholar] [CrossRef] [PubMed]
- Geiger, F.; Kebbach, M.; Vogel, D.; Weissmann, V.; Bader, R. Efficient Computer-Based Method for Adjusting the Stiffness of Subject-Specific 3D-Printed Insoles during Walking. Appl. Sci. 2023, 13, 3854. [Google Scholar] [CrossRef]
- Gupta, S.; Jayaraman, R.; Sidhu, S.S.; Malviya, A.; Chatterjee, S.; Chhikara, K.; Singh, G.; Chanda, A. Diabot: Development of a Diabetic Foot Pressure Tracking Device. J 2023, 6, 32–47. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Number | Score | |||
|---|---|---|---|---|---|
| A (>90) | B (75–90) | C (50–75) | D (<50) | ||
| Flexible Flat Foot | 96 | 3 | 62 | 29 | 2 |
| Rigid Flat Foot | 29 | 1 | 13 | 8 | 7 |
| Overpronated | 41 | 6 | 20 | 6 | 9 |
| High Arch | 16 | 2 | 8 | 3 | 3 |
| Diabetic (with corn/ulcers) | 12 | 0 | 5 | 6 | 1 |
| Diabetic (without ulcers) | 6 | 1 | 3 | 2 | 0 |
| Total | 200 | 13 | 111 | 54 | 22 |
| Type | Number | Score | |||
|---|---|---|---|---|---|
| A (>90) | B (75–90) | C (50–75) | D (<50) | ||
| Flexible Flat Foot | 96 | 69 | 20 | 7 | 0 |
| Rigid Flat Foot | 29 | 17 | 8 | 2 | 2 |
| Overpronated | 41 | 28 | 11 | 1 | 1 |
| High Arch | 16 | 9 | 7 | 0 | 0 |
| Diabetic (with corn/ulcers) | 12 | 6 | 4 | 1 | 1 |
| Diabetic (without ulcers) | 6 | 3 | 3 | 0 | 0 |
| Total | 200 | 132 | 53 | 11 | 4 |
| Type | Number | Score | |||
|---|---|---|---|---|---|
| A (>90) | B (75–90) | C (50–75) | D (<50) | ||
| Midfoot Pain | 48 | 10 | 26 | 11 | 1 |
| Ankle Pain | 36 | 6 | 13 | 14 | 3 |
| Knee Pain | 32 | 3 | 8 | 20 | 1 |
| Hip and Lower Back Pain | 10 | 0 | 6 | 2 | 2 |
| Total | 126 | 19 | 53 | 47 | 7 |
| Type | Number | Score | |||
|---|---|---|---|---|---|
| A (>90) | B (75–90) | C (50–75) | D (<50) | ||
| Midfoot Pain | 48 | 30 | 18 | 0 | 0 |
| Ankle Pain | 36 | 25 | 8 | 1 | 2 |
| Knee Pain | 32 | 22 | 8 | 1 | 1 |
| Hip and Lower Back Pain | 10 | 6 | 3 | 1 | 0 |
| Total | 126 | 83 | 37 | 3 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaikh, S.; Jamdade, B.; Chanda, A. Effects of Customized 3D-Printed Insoles in Patients with Foot-Related Musculoskeletal Ailments—A Survey-Based Study. Prosthesis 2023, 5, 550-561. https://doi.org/10.3390/prosthesis5020038
Shaikh S, Jamdade B, Chanda A. Effects of Customized 3D-Printed Insoles in Patients with Foot-Related Musculoskeletal Ailments—A Survey-Based Study. Prosthesis. 2023; 5(2):550-561. https://doi.org/10.3390/prosthesis5020038
Chicago/Turabian StyleShaikh, Salman, Bhakti Jamdade, and Arnab Chanda. 2023. "Effects of Customized 3D-Printed Insoles in Patients with Foot-Related Musculoskeletal Ailments—A Survey-Based Study" Prosthesis 5, no. 2: 550-561. https://doi.org/10.3390/prosthesis5020038