
Effectiveness of Different Irrigation Techniques on Post Space Smear Layer Removal: SEM Evaluation


 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
Root Canal Preparation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gillen, B.M.; Looney, S.W.; Gu, L.-S.; Loushine, B.A.; Weller, R.N.; Loushine, R.J.; Pashley, D.H.; Tay, F.R. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: A systematic review and meta-analysis. J. Endod. 2011, 37, 895–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroeder, A.A.; Ford, N.L.; Coil, J.M. Micro-computed tomography analysis of post space preparation in root canals filled with carrier-based thermoplasticized gutta-percha. Int. Endod. J. 2016, 50, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Özkurt-Kayahan, Z.; Barut, G.; Ulusoy, Z.; Oruçoğlu, H.; Kayahan, M.B.; Kazazoğlu, E.; Haznedaroğlu, F. Influence of post space preparation on the apical leakage of calamus, single-cone and cold lateral condensation obturation techniques: A computerized fluid filtration study. J. Prosthodont. 2019, 28, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Asmussen, E.; Peutzfeldt, A.; Heitmann, T. Stiffness, elastic limit, and strength of newer types of endodontic posts. J. Dent. 1999, 27, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Perdigão, J.; Geraldeli, S.; Lee, I.K. Push-out bond strengths of tooth-colored posts bonded with different adhesive systems. Am. J. Dent. 2004, 17, 422–426. [Google Scholar] [PubMed]
- Hayashi, M.; Takahashi, Y.; Hirai, M.; Iwami, Y.; Imazato, S.; Ebisu, S. Effect of endodontic irrigation on bonding of resin cement to radicular dentin. Eur. J. Oral Sci. 2005, 113, 70–76. [Google Scholar] [CrossRef]
- Zhang, L.; Huang, L.; Xiong, Y.; Fang, M.; Chen, J.H.; Ferrari, M. Effect of post-space treatment on retention of fiber posts in differen root regions using two self-etching systems. Eur. J. Oral Sci. 2008, 116, 280–286. [Google Scholar] [CrossRef]
- Caputo, A.A.; Standlee, J.P. Pins and posts—Why, when and how. Dent. Clin. N. Am. 1976, 20, 299–311. [Google Scholar] [CrossRef]
- Kremeier, K.; Fasen, L.; Klaiber, B.; Hofmann, N. Influence of endodontic post type (glass fiber, quartz fiber or gold) and luting material on push-out bond strength to dentin in vitro. Dent. Mater. 2008, 24, 660–666. [Google Scholar] [CrossRef]
- Akgungor, G.; Akkayan, B. Influence of dentin bonding agents and polymerization modes on the bond strength between translucent fiber posts and three dentin regions within a post space. J. Prosthet. Dent. 2006, 95, 368–378. [Google Scholar] [CrossRef]
- Aksornmuang, J.; Nakajima, M.; Foxton, R.M.; Panyayong, W.; Tagami, J. Regional bond strengths and failure analysis of fiber posts bonded to root canal dentin. Oper. Dent. 2008, 33, 636–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teoh, Y.Y.; Walsh, L.J. Residual Endodontic Filling Material after Post Space Preparation: A Confocal Microscopic Study. Materials 2017, 10, 1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannocli, F.; Innocenti, M.; Ferrari, M.; Watson, T.F. Confocal and scanning electron microscopic study of teeth restored with fiber posts, metal posts, and composite resins. J. Endod. 1999, 25, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Perdigão, J.; Gomes, G.; Augusto, V. The effect of dowel space on the bond strengths of fiber posts. J. Prosthodont. 2007, 16, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Seballos, V.G.; Barreto, M.S.; Rosa, R.A.D.; Machado, E.; Valandro, L.F.; Kaizer, O.B. Effect of Post-Space Irrigation with NaOCl and CaOCl at Different Concentrations on the Bond Strength of Posts Cemented with a Self-Adhesive Resin Cement. Braz. Dent. J. 2018, 29, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.D.; Lee, K.W.; Agee, K.A.; Bouillaguet, S.; Pashely, D.H. Effects of sodium hypoclorite and RC-prep on bond strengths of resin cement to endodontic surfaces. J. Endod. 2001, 27, 753–757. [Google Scholar] [CrossRef]
- Ferreira, M.B.d.C.; Carlini Júnior, B.; Galafassi, D.; Gobbi, D.L. Calcium hypochlorite as a dentin deproteinization agent: Microleakage, scanning electron microscopy and elemental analysis. Microsc. Res. Tech. 2015, 78, 676–681. [Google Scholar] [CrossRef]
- Dutta, A.; Saunders, W.P. Comparative evaluation of calcium hypochlorite and sodium hypochlorite on soft-tissue dissolution. J. Endod. 2012, 38, 1395–1398. [Google Scholar] [CrossRef]
- Görduysus, M.; Küçükkaya, S.; Bayramgil, N.P.; Görduysus, M.Ö. Evaluation of the effects of two novel irrigants on intraradicular dentine erosion, debris and smear layer removal. Restor. Dent. Endod. 2015, 40, 216–222. [Google Scholar] [CrossRef]
- Macário, T.R.L.; de Carvalho, R.F.; Domingues, P.B.A.; Maia, B.d.G.O.; Marinho, C.C.; Barcellos, A.S.d.P.; Junqueira, R.B. Evaluation of the cleaning protocol of post space on bond strength of glass fiber posts. Int. J. Odontostomatol. 2021, 15, 427–433. [Google Scholar] [CrossRef]
- Iandolo, A.; Simeone, M.; Orefice, S.; Rengo, S. 3D cleaning, a perfected technique: Thermal profile assessment of heated NaOCl. G. Ital. Di Endod. 2017, 31, 58–61. [Google Scholar] [CrossRef]
- Schneider, S.W. A Comparison of Canal Preparations in Straight and Curved Root Canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Rajamanickam, K.; Teja, K.V.; Ramesh, S.; AbuMelha, A.S.; Alkahtany, M.F.; Almadi, K.H.; Bahammam, S.A.; Janani, K.; Choudhari, S.; Jose, J.; et al. Comparative Study Assessing the Canal Cleanliness Using Automated Device and Conventional Syringe Needle for Root Canal Irrigation-An Ex-Vivo Study. Materials 2022, 15, 6184. [Google Scholar] [CrossRef] [PubMed]
- Metzger, Z.; Teperovich, E.; Cohen, R.; Zary, R.; Paqué, F.; Hülsmann, M. The self-adjusting file (SAF). Part 3: Removal of debris and smear layer—A scanning electron microscope study. J. Endod. 2010, 36, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Rödig, T.; Hülsmann, M.; Kahlmeier, C. Comparison of root canal preparation with two rotary NiTi instruments: ProFile. 04 and GT Rotary. Int. Endod. J. 2007, 40, 553–562. [Google Scholar] [CrossRef]
- Silva, N.R.D.; Rodrigues, M.D.P.; Bicalho, A.A.; De Deus, R.A.; Soares, P.B.F.; Soares, C.J. Effect of Magnification during Post Space Preparation on Root Cleanness and Fiber Post Bond Strength. Braz. Dent. J. 2019, 30, 491–497. [Google Scholar] [CrossRef]
- Van Meerbeek, B.; De Munck, J.; Yoshida, Y.; Inoue, S.; Vargas, M.; Vijay, P.; Van Landuyt, K.; Lambrechts, P.; Vanherle, G. Buonocore memorial lecture. Adhesion to enamel and dentin: Current status and future challenges. Oper. Dent. 2003, 28, 215–235. [Google Scholar]
- Boone, K.J.; Murchison, D.F.; Schindler, W.G.; Walker, W.A. Post retention: The effect of sequence of post-space preparation, cementation time, and different sealers. J. Endod. 2001, 27, 768–771. [Google Scholar] [CrossRef]
- Nakajima, M.; Kanemura, N.; Pereira, P.N.; Tagami, J.; Pashley, D.H. Comparative microtensile bond strenght and SEM analysis of bonding to wet and dry dentin. Am. J. Dent. 2000, 13, 324–328. [Google Scholar]
- Serper, A.; Çalt, S. The demineralizing effects of EDTA at different concentrations and pH. J. Endod. 2002, 28, 501–502. [Google Scholar] [CrossRef]
- Şen, B.H.; Wesselink, P.R.; Türkün, M. The smear layer: A phenomenon in root canal therapy. Int. Endod. J. 1995, 28, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Iandolo, A.; Amato, A.; Martina, S.; Latif, D.A.; Pantaleo, G. Management of severe curvatures in root canal treatment with the new generation of rotating files using a safe and predictable protocol. Open Dent. J. 2020, 14, 421–425. [Google Scholar] [CrossRef]
- Martina, S.; Pisano, M.; Amato, A.; Abdellatif, D.; Iandolo, A. Modern rotary files in minimally invasive endodontics: A case report. Front. Biosci. 2021, 13, 299–304. [Google Scholar]
- Abdellatif, D.; Amato, A.; Calapaj, M.; Pisano, M.; Iandolo, A. A novel modified obturation technique using biosealers: An ex vivo study. J. Conserv. Dent. 2021, 24, 369–373. [Google Scholar]
- Simeone, M.; Valletta, A.; Giudice, A.; Di Lorenzo, P.; Iandolo, A. The activation of irrigation solutions in Endodontics: A perfected technique. G. Ital. Di Endod. 2015, 29, 65–69. [Google Scholar] [CrossRef] [Green Version]
- Bohrer, T.C.; Fontana, P.E.; Rocha, R.O.; Kaizer, O.B. Post-Space Treatment Influences the Bond Strength in Endodontically Treated Teeth: A Systematic Review and Meta-Analysis of In Vitro Studies. Oper. Dent. 2021, 46, E132–E157. [Google Scholar] [CrossRef]
- Dos Reis-Prado, A.H.; Abreu, L.G.; Tavares, W.L.F.; Peixoto, I.F.D.C.; Viana, A.C.D.; de Oliveira, E.M.C.; Bastos, J.V.; Ribeiro-Sobrinho, A.P.; Benetti, F. Comparison between immediate and delayed post space preparations: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 417–440. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
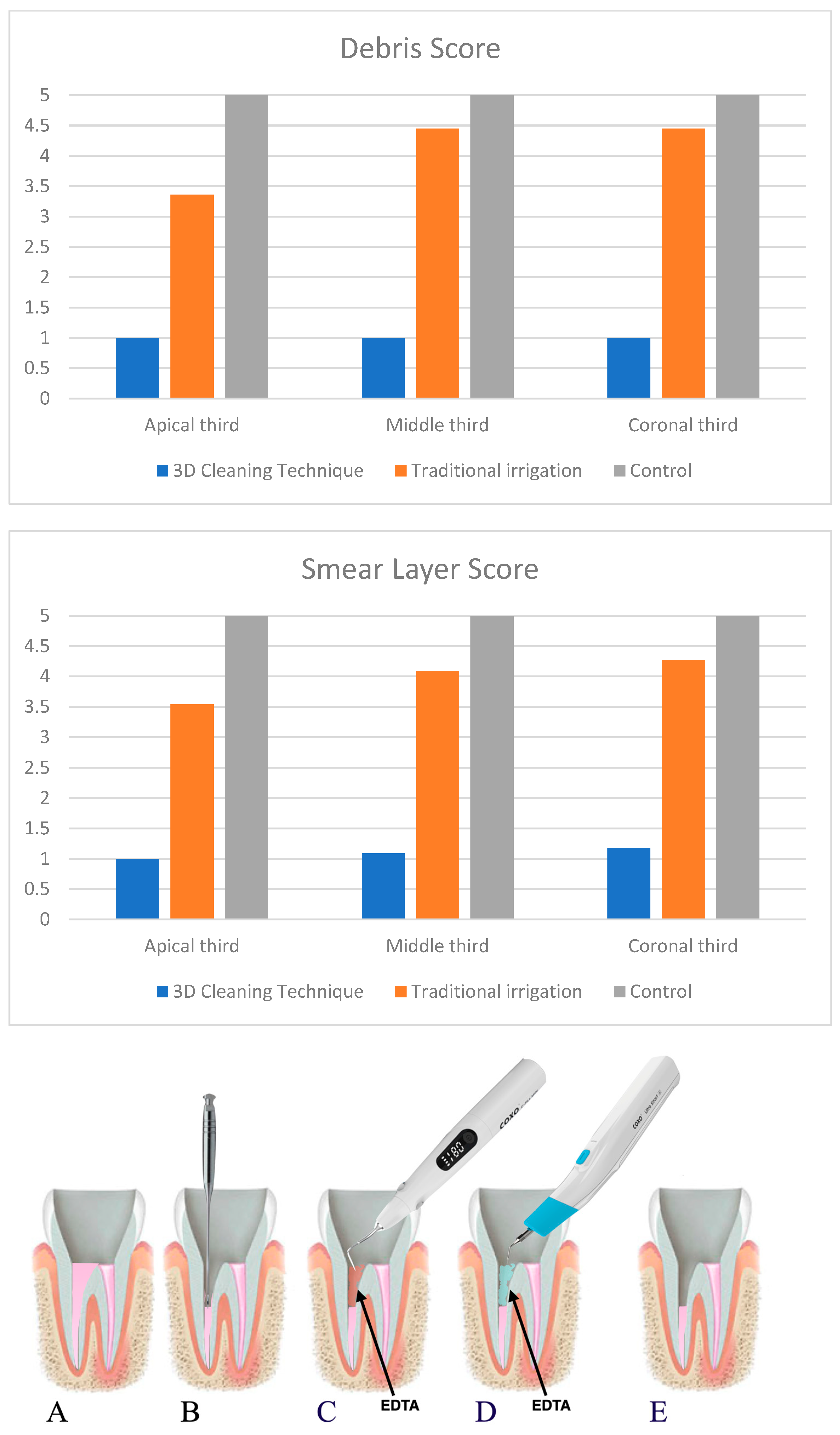
| Group | D Coronal | D Middle | D Apical | D Total | |
|---|---|---|---|---|---|
| 1 | Mean | 1 | 1 | 1 | 1.06 ± 0.24 |
| N | 11 | 11 | 11 | 33 | |
| Median 25 Percentile 75 Percentile | 1 1 1 | 1 1 1 | 1 1 1 | 1 1 1 | |
| 2 | Mean | 3.36 ± 0.67 | 4.45 ± 0.69 | 4.45 ± 0.69 | 4.06 ± 0.79 |
| N | 11 | 11 | 11 | 33 | |
| Median 25 Percentile 75 Percentile | 3 3 4 | 5 4 5 | 5 4 5 | 4 4 5 | |
| 3 | Mean | 5 | 5 | 5 | 5 |
| N | 11 | 11 | 11 | 33 | |
| Median 25 Percentile 75 Percentile | 5 5 5 | 5 5 5 | 5 5 5 | 5 5 5 | |
| Total | Mean | 3.12 ± 1.71 | 3.45 ± 1.8 | 3.54 ± 1.77 | |
| N | 33 | 33 | 33 | ||
| Median 25 Percentile 75 Percentile | 3 1 5 | 4 1 5 | 5 1 5 | ||
| Group | SL Coronal | SL Middle | SL Apical | SL Total | |
|---|---|---|---|---|---|
| 1 | Mean | 1 | 1.09 ± 0.3 | 1.18 ± 0.4 | 1.09 ± 0.29 |
| N | 11 | 11 | 11 | 33 | |
| Median 25 Percentile 75 Percentile | 1 1 1 | 1 1 1 | 1 1 1 | 1 1 1 | |
| 2 | Mean | 3.54 ± 0.82 | 4.09 ± 0.7 | 4.27 ± 0.9 | 3.96 ± 0.85 |
| N | 11 | 11 | 11 | 33 | |
| Median 25 Percentile 75 Percentile | 4 3 4 | 4 4 5 | 4 4 5 | 4 3.5 5 | |
| 3 | Mean | 5 | 5 | 5 | 5 |
| N | 11 | 11 | 11 | 33 | |
| Median 25 Percentile 75 Percentile | 5 5 5 | 5 5 5 | 5 5 5 | 5 5 5 | |
| Total | Mean | 3.18 ± 1.74 | 3.39 ± 1.75 | 3.48 ± 1.77 | |
| N | 33 | 33 | 33 | ||
| Median 25 Percentile 75 Percentile | 4 1 5 | 4 1 5 | 4 1 5 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iandolo, A.; Pisano, M.; Abdellatif, D.; Amato, A.; Giordano, F.; Buonavoglia, A.; Sangiovanni, G.; Caggiano, M. Effectiveness of Different Irrigation Techniques on Post Space Smear Layer Removal: SEM Evaluation. Prosthesis 2023, 5, 539-549. https://doi.org/10.3390/prosthesis5020037
Iandolo A, Pisano M, Abdellatif D, Amato A, Giordano F, Buonavoglia A, Sangiovanni G, Caggiano M. Effectiveness of Different Irrigation Techniques on Post Space Smear Layer Removal: SEM Evaluation. Prosthesis. 2023; 5(2):539-549. https://doi.org/10.3390/prosthesis5020037
Chicago/Turabian StyleIandolo, Alfredo, Massimo Pisano, Dina Abdellatif, Alessandra Amato, Francesco Giordano, Alessio Buonavoglia, Giuseppe Sangiovanni, and Mario Caggiano. 2023. "Effectiveness of Different Irrigation Techniques on Post Space Smear Layer Removal: SEM Evaluation" Prosthesis 5, no. 2: 539-549. https://doi.org/10.3390/prosthesis5020037