
Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature

 , , ,
, , , 
 ,
,  and
and
Abstract
:1. Introduction
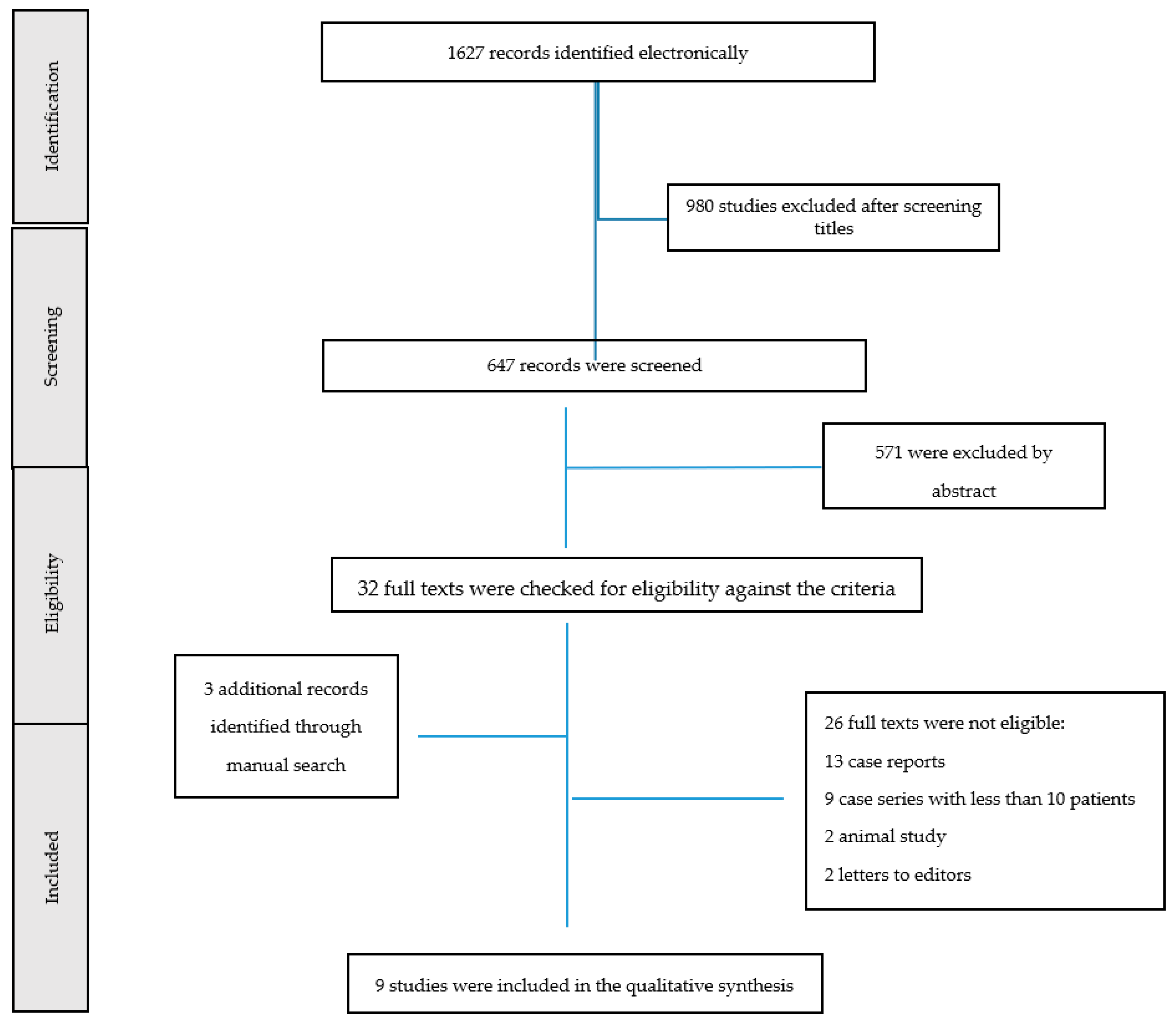
2. Materials and Methods
3. Results
3.1. Prosthodontic Treatment in Patients Affected by TMDs
3.2. Prosthodontic Treatment in Patients Affected by Bruxism
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TMD | Temporomandibular disorder |
| TMJ | Temporomandibular joint |
| EMG | Electromyography |
| MRI | Magnetic resonance imaging |
| VDO | Vertical dimension of occlusion |
| DC/TMD | Diagnostic Criteria for Temporomandibular Disorders |
| FDPs | Fixed dental prostheses |
References
- Manfredini, D.; Lombardo, L.; Siciliani, G. Temporomandibular disorders and dental occlusion. A systematic review of association studies: End of an era? J. Oral Rehabil. 2017, 44, 908–923. [Google Scholar] [CrossRef]
- Racich, M.J. Occlusion, temporomandibular disorders, and orofacial pain: An evidence-based overview and update with recommendations. J. Prosthet. Dent. 2018, 120, 678–685. [Google Scholar] [CrossRef]
- Moccia, S.; Nucci, L.; Spagnuolo, C.; d’Apuzzo, F.; Grazia, M.; Minervini, G. Polyphenols as potential agents in the management of temporomandibular disorders. Appl. Sci. 2020, 10, 5305. [Google Scholar] [CrossRef]
- Ingawalé, S.; Goswami, T. Temporomandibular joint: Disorders, treatments, and biomechanics. Ann. Biomed. Eng. 2009, 37, 976–996. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, J.; Wang, L.; Wang, K.; Svensson, P. Effect of transcutaneous electrical nerve stimulation on jaw movement-evoked pain in patients with TMJ disc displacement without reduction and healthy controls. Acta Odontol. Scand. 2020, 78, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Tiirp, J.C.; Dent, M.; Strub, J.R.; Dentb, M. Prosthetic rehabilitation in patients with temporomandibular disorders. J. Prosthet. Dent. 1996, 76, 418–423. [Google Scholar] [CrossRef]
- Minervini, G.; Nucci, L.; Lanza, A.; Femiano, F.; Contaldo, M.; Grassia, V. Temporomandibular disc displacement with reduction treated with anterior repositioning splint: A 2-year clinical and magnetic resonance imaging (MRI) follow-up. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. 1), 151–160. [Google Scholar] [PubMed]
- Manfredini, D.; Ahlberg, J.; Aarab, G.; Bracci, A.; Durham, J.; Ettlin, D.; Gallo, L.M.; Koutris, M.; Wetselaar, P.; Svensson, P.; et al. Towards a Standardized Tool for the Assessment of Bruxism (STAB)—Overview and general remarks of a multidimensional bruxism evaluation system. J. Oral Rehabil. 2020, 47, 549–556. [Google Scholar] [CrossRef]
- Al-Jabrah, O.A.; Al-Shumailan, Y.R. Prevalence of temporomandibular disorder signs in patients with complete versus partial dentures. Clin. Oral Investig. 2006, 10, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Minervini, A.L.G.; Romano, A.; Petruzzi, M.; Maio, C.; Serpico, R.; di Stasio, D. Oral-Facial-Digital Syndrome (OFD): 31-Year follow-up management and monitoring. J. Biol. Regul. Homeost. Agents 2018, 32, 127–130. [Google Scholar]
- Johansson, A.; Omar, R.; Carlsson, G.E. Bruxism and prosthetic treatment: A critical review. J. Prosthodont. Res. 2011, 55, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Minervini, G.; Lucchese, A.; Perillo, L.; Serpico, R.; Minervini, G. Unilateral superior condylar neck fracture with dislocation in a child treated with an acrylic splint in the upper arch for functional repositioning of the mandible. Cranio-J. Craniomandib. Pract. 2017, 35, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, G.E. Some dogmas related to prosthodontics, temporomandibular disorders and occlusion. Acta Odontol. Scand. 2010, 68, 313–322. [Google Scholar] [CrossRef]
- Bousema, E.J.; Koops, E.A.; van Dijk, P.; Dijkstra, P.U. Association between Subjective Tinnitus and Cervical Spine or Temporomandibular Disorders: A Systematic Review. Trends Hear. 2018, 22, 2331216518800640. [Google Scholar] [CrossRef] [PubMed]
- Deregibus, A.; Ferrillo, M.; Piancin, M.G.; Domini, M.C.; de Sire, A.; Castroflorio, T. Are occlusal splints effective in reducing myofascial pain in patients with muscle-related temporomandibular disorders? A randomized-controlled trial. Turk. J. Phys. Med. Rehabil. 2021, 67, 32–40. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Marotta, N.; Ferrillo, M.; Agostini, F.; Sconza, C.; Lippi, L.; Respizzi, S.; Giudice, A.; Invernizzi, M.; Ammendolia, A. Oxygen-Ozone Therapy for Reducing Pro-Inflammatory Cytokines Serum Levels in Musculoskeletal and Temporomandibular Disorders: A Comprehensive Review. Int. J. Mol. Sci. 2022, 23, 2528. [Google Scholar] [CrossRef]
- Minervini, G.; Russo, D.; Herford, A.S.; Gorassini, F.; Meto, A.; D’Amico, C.; Cervino, G.; Cicciù, M.; Fiorillo, L. Teledentistry in the Management of Patients with Dental and Temporomandibular Disorders. BioMed Res. Int. 2022, 2022, 7091153. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Castroflorio, T.; Perinetti, G.; Guarda-Nardini, L. Dental occlusion, body posture and temporomandibular disorders: Where we are now and where we are heading for. J. Oral Rehabil. 2012, 39, 463–471. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- di Francesco, F.; de Marco, G.; Capcha, E.B.; Lanza, A.; Cristache, C.M.; Vernal, R.; Cafferata, E.A. Patient satisfaction and survival of maxillary overdentures supported by four or six splinted implants: A systematic review with meta-analysis. BMC Oral Health 2021, 21, 247. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Poggio, C.E. Prosthodontic planning in patients with temporomandibular disorders and/or bruxism: A systematic review. J. Prosthet. Dent. 2017, 117, 606–613. [Google Scholar] [CrossRef]
- Sessle, B.J. Mechanisms of oral somatosensory and motor functions and their clinical correlates. J. Oral Rehabil. 2006, 33, 243–261. [Google Scholar] [CrossRef]
- Carlsson, G.E. Dental occlusion: Modern concepts and their application in implant prosthodontics. Odontology 2009, 97, 8–17. [Google Scholar] [CrossRef]
- Levartovsky, S.; Pilo, R.; Shadur, A.; Matalon, S.; Winocur, E. Complete rehabilitation of patients with bruxism by veneered and non-veneered zirconia restorations with an increased vertical dimension of occlusion: An observational case-series study. J. Prosthodont. Res. 2019, 63, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Chatzopoulos, G.S.; Wolff, L.F. Symptoms of temporomandibular disorder, self-reported bruxism, and the risk of implant failure: A retrospective analysis. Cranio-J. Craniomandib. Pract. 2020, 38, 50–57. [Google Scholar] [CrossRef]
- di Francesco, F.; de Marco, G.; Sommella, A.; Lanza, A. Splinting vs Not Splinting Four Implants Supporting a Maxillary Overdenture: A Systematic Review. Int. J. Prosthodont. 2019, 32, 509–518. [Google Scholar] [CrossRef]
- di Francesco, F.; de Marco, G.; Carnevale, U.A.G.; Lanza, M.; Lanza, A. The number of implants required to support a maxillary overdenture: A systematic review and meta-analysis. J. Prosthodont. Res. 2019, 63, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2019. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 February 2022).
- den Hartog, L.; Slater, J.J.R.H.; Vissink, A.; Meijer, H.J.A.; Raghoebar, G.M. Treatment outcome of immediate, early and conventional single-tooth implants in the aesthetic zone: A systematic review to survival, bone level, soft-tissue, aesthetics and patient satisfaction. J. Clin. Periodontol. 2008, 35, 1073–1086. [Google Scholar] [CrossRef] [PubMed]
- Calamita, M.; Coachman, C.; Sesma, N.; Kois, J. Occlusal vertical dimension: Treatment planning decisions and management considerations. Int. J. Esthet. Dent. 2019, 14, 166–181. [Google Scholar]
- Fabbri, G.; Sorrentino, R.; Cannistraro, G.; Mintrone, F.; Bacherini, L.; Turrini, R.; Bombardelli, T.; Nieri, M.; Fradeani, M. Increasing the Vertical Dimension of Occlusion: A Multicenter Retrospective Clinical Comparative Study on 100 Patients with Fixed Tooth-Supported, Mixed, and Implant-Supported Full-Arch Rehabilitations. Int. J. Periodontics Restor. Dent. 2018, 38, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Alhajj, M.N.; Khalifa, N.; Abduo, J.; Amran, A.G.; Ismail, I.A. Determination of occlusal vertical dimension for complete dentures patients: An updated review. J. Oral Rehabil. 2017, 44, 896–907. [Google Scholar] [CrossRef]
- Moreno-Hay, I.; Okeson, J.P. Does altering the occlusal vertical dimension produce temporomandibular disorders? A literature review. J. Oral Rehabil. 2015, 42, 875–882. [Google Scholar] [CrossRef]
- Abduo, J. Safety of increasing vertical dimension of occlusion: A systematic review. Quintessence Int. 2012, 43, 369–380. [Google Scholar] [PubMed]
- Vailati, F.; Carciofo, S. Treatment planning of adhesive additive rehabilitations: The progressive wax-up of the three-step technique. Int. J. Esthet. Dent. 2016, 11, 356–377. [Google Scholar]
- Bourdiol, P.; Hennequin, M.; Peyron, M.-A.; Woda, A. Masticatory Adaptation to Occlusal Changes. Front. Physiol. 2020, 11, 263. [Google Scholar] [CrossRef] [Green Version]
- Johansson, A.; Johansson, A.-K.; Omar, R.; Carlsson, G.E. Rehabilitation of the worn dentition. J. Oral Rehabil. 2008, 35, 548–566. [Google Scholar] [CrossRef]
- Abdelnabi, M.H.; Swelem, A.A. Influence of defective complete dentures renewal on TMD; An MRI and clinical controlled prospective study. Gerodontology 2015, 32, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Poštić, S.D. Specific occlusal scheme for partially edentulous patients with TMD signs-preliminary report. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 337–347. [Google Scholar] [CrossRef]
- Fiorillo, L.; D’Amico, C.; Turkina, A.Y.; Nicita, F.; Amoroso, G.; Risitano, G. Endo and Exoskeleton: New Technologies on Composite Materials. Prosthesis 2020, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Sreekumar, S.; Janakiram, C.; Mathew, A. Effects of Prosthetic Rehabilitation on Temporomandibular Disorders: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2021, 10, e33104. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, C.; Bocchieri, S.; Sambataro, S.; Surace, G.; Stumpo, C.; Fiorillo, L. Occlusal Load Considerations in Implant-Supported Fixed Restorations. Prosthesis 2020, 2, 252–265. [Google Scholar] [CrossRef]
- Ribeiro, J.A.M.; de Resende, C.M.B.M.; Lopes, A.L.C.; Farias-Neto, A.; Carreiro, A.D.F.P. Association between prosthetic factors and temporomandibular disorders in complete denture wearers. Gerodontology 2014, 31, 308–313. [Google Scholar] [CrossRef]
- Muts, E.J.; van Pelt, H.; Edelhoff, D.; Krejci, I.; Cune, M. Tooth wear: A systematic review of treatment options. J. Prosthet. Dent. 2014, 112, 752–759. [Google Scholar] [CrossRef]
- Yılmaz, D.; Kamburoğlu, K. Comparison of the effectiveness of high resolution ultrasound with MRi in patients with temporomandibular joint dısorders. Dentomaxillofac. Radiol. 2019, 48, 20180349. [Google Scholar] [CrossRef]
- de Boever, J.A.; Carlsson, G.E.; Klineberg, I.J. Need for occlusal therapy and prosthodontic treatment in the management of temporomandibular disorders. Part II. Tooth loss and prosthodontic treatment. J. Oral Rehabil. 2000, 27, 647–659. [Google Scholar] [CrossRef]
- Granell-Ruíz, M.; Agustín-Panadero, R.; Fons-Font, A.; Román-Rodríguez, J.L.; Solá-Ruíz, M.F. Influence of bruxism on survival of porcelain laminate veneers. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e426–e432. [Google Scholar] [CrossRef] [PubMed]
- Lobbezoo, F.; Ahlberg, J.; Manfredini, D.; Winocur, E. Are bruxism and the bite causally related? J. Oral Rehabil. 2012, 39, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Botelho, J.; Machado, V.; Proença, L.; Rua, J.; Martins, L.; Alves, R.; Cavacas, M.A.; Manfredini, D.; Mendes, J.J. Relationship between self-reported bruxism and periodontal status: Findings from a cross-sectional study. J. Periodontol. 2020, 91, 1049–1056. [Google Scholar] [CrossRef] [PubMed]
- Huhtela, O.; Näpänkangas, R.; Joensuu, T.; Raustia, A.; Kunttu, K.; Sipilä, K. Self-Reported Bruxism and Symptoms of Temporomandibular Disorders in Finnish University Students. J. Oral Facial Pain Headache 2016, 30, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Koenig, V.; Wulfman, C.; Bekaert, S.; Dupont, N.; le Goff, S.; Eldafrawy, M.; Vanheusden, A.; Mainjot, A. Clinical behavior of second-generation zirconia monolithic posterior restorations: Two-year results of a prospective study with Ex vivo analyses including patients with clinical signs of bruxism. J. Dent. 2019, 91, 103229. [Google Scholar] [CrossRef] [PubMed]
- Brignardello-Petersen, R. There are probably similar outcomes between a glass-hybrid restorative and a nanoceramic composite resin after 2 years of restoring noncarious cervical lesions in patients with bruxism. J. Am. Dent. Assoc. 2020, 151, e6. [Google Scholar] [CrossRef]
- Contaldo, M.; Serpico, R.; Lucchese, A. In vivo imaging of enamel by reflectance confocal microscopy (RCM): Non-invasive analysis of dental surface. Odontology 2014, 102, 325–329. [Google Scholar] [CrossRef]
- Gentile, E.; di Stasio, D.; Santoro, R.; Contaldo, M.; Salerno, C.; Serpico, R.; Lucchese, A. In Vivo Microstructural Analysis of Enamel in Permanent and Deciduous Teeth. Ultrastruct. Pathol. 2015, 39, 131–134. [Google Scholar] [CrossRef] [Green Version]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Bruxism and dental implants: A meta-analysis. Implant. Dent. 2015, 24, 505–516. [Google Scholar] [CrossRef]
- Faus-Matoses, V.; Ruiz-Bell, E.; Faus-Matoses, I.; Özcan, M.; Salvatore, S.; Faus-Llácer, V.J. An 8-year prospective clinical investigation on the survival rate of feldspathic veneers: Influence of occlusal splint in patients with bruxism. J. Dent. 2020, 99, 103352. [Google Scholar] [CrossRef]
- Cicciù, M.; Cervino, G.; Terranova, A.; Risitano, G.; Raffaele, M.; Cucinotta, F.; Santonocito, D.; Fiorillo, L. Prosthetic and Mechanical Parameters of the Facial Bone under the Load of Different Dental Implant Shapes: A Parametric Study. Prosthesis 2019, 1, 41–53. [Google Scholar] [CrossRef] [Green Version]
- Manfredini, D.; Poggio, C.E.; Lobbezoo, F. Is Bruxism a Risk Factor for Dental Implants? A Systematic Review of the Literature. Clin. Implant. Dent. Relat. Res. 2014, 16, 460–469. [Google Scholar] [CrossRef]
- Manfredini, D.; Ahlberg, J.; Mura, R.; Lobbezoo, F. Bruxism is unlikely to cause damage to the periodontium: Findings from a systematic literature assessment. J. Periodontol. 2015, 86, 546–555. [Google Scholar] [CrossRef]
- Ortorp, A.; Kihl, M.L.; Carlsson, G.E. A 3-year retrospective and clinical follow-up study of zirconia single crowns performed in a private practice. J. Dent. 2009, 37, 731–736. [Google Scholar] [CrossRef]
- Koutayas, S.O.; Vagkopoulou, T.; Pelekanos, S.; Koidis, P.; Strub, J.R. Zirconia in dentistry: Part 2. Evidence-based clinical breakthrough. Eur. J. Esthet. Dent. 2009, 4, 348–380. [Google Scholar]
- Schley, J.-S.; Heussen, N.; Reich, S.; Fischer, J.; Haselhuhn, K.; Wolfart, S. Survival probability of zirconia-based fixed dental prostheses up to 5 yr: A systematic review of the literature. Eur. J. Oral Sci. 2010, 118, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Contaldo, M.; della Vella, F.; Raimondo, E.; Minervini, G.; Buljubasic, M.; Ogodescu, A.; Sinescu, C.; Serpico, R. Early Childhood Oral Health Impact Scale (ECOHIS): Literature review and Italian validation. Int J. Dent. Hyg. 2020, 18, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Bruxism and dental implant failures: A multilevel mixed effects parametric survival analysis approach. J. Oral Rehabil. 2016, 43, 813–823. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Year | Study Design | Topic |
|---|---|---|---|
| Levartovsky et al. | 2019 | Retrospective | TMD/Bruxism |
| Ribeiro et al. | 2014 | Retrospective | TMD |
| Yilmaz et al. | 2019 | Prospective | TMD |
| Al-Jabrah et al. | 2006 | Retrospective | TMD |
| Granell-Ruíz et al. | 2014 | Prospective | Bruxism |
| Koenig et al. | 2019 | Prospective | Bruxism |
| Brignardello et al. | 2020 | Retrospective | Bruxism |
| Faus-Matoses et al. | 2020 | Retrospective | TMD |
| Ortorp et al. | 2009 | Retrospective | Bruxism |
| Study | Selection **** | Comparability ** | Outcome *** | Score |
|---|---|---|---|---|
| Levartovsky et al. | **** | * | *** | 8 |
| Yilmaz et al. | **** | * | *** | 8 |
| Koenig et al. | **** | * | *** | 8 |
| Brignardello et al. | **** | * | ** | 7 |
| Faus-Matoses et al. | **** | ** | ** | 8 |
| Study | 1. Are the Characteristics of the Study Group Clearly Described? | 2. Is there a High Risk of Selection Bias? Are the Inclusion and Exclusion Criteria Clearly Described? | 3. Is the Intervention Clearly Described? Are all Patients Treated According to the Same Intervention? | 4. Are the Outcomes Clearly Described? Are Adequate Methods Used to Assess the Outcome? | 5. Is Blinding Used to Assess the Outcome? | 6. Is there a Sufficient Follow-Up? | 7. Can Selective Loss-to Follow-Up Sufficiently Be Excluded? | 8. Are the Most Important Confounders or Prognostic Factors Identified and Are these Taken into Consideration with Respect to the Study Design and Analysis? |
|---|---|---|---|---|---|---|---|---|
| Ribeiro et al. | + | + | + | + | + | + | + | − |
| Granell-Ruíz et al. | + | + | + | + | + | + | + | − |
| Ortorp et al. | + | + | + | + | ? | + | + | − |
| Al-Jabrah et al. | + | + | + | + | − | + | + | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Francesco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253-262. https://doi.org/10.3390/prosthesis4020025
Minervini G, Fiorillo L, Russo D, Lanza A, D’Amico C, Cervino G, Meto A, Di Francesco F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis. 2022; 4(2):253-262. https://doi.org/10.3390/prosthesis4020025
Chicago/Turabian StyleMinervini, Giuseppe, Luca Fiorillo, Diana Russo, Alessandro Lanza, Cesare D’Amico, Gabriele Cervino, Aida Meto, and Fabrizio Di Francesco. 2022. "Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature" Prosthesis 4, no. 2: 253-262. https://doi.org/10.3390/prosthesis4020025