
A Review on Risk Management of Coronavirus Disease 19 (COVID-19) Infection in Dental Practice: Focus on Prosthodontics and All-Ceramic Materials

 ,
,  , ,
, ,
Abstract
:1. Introduction
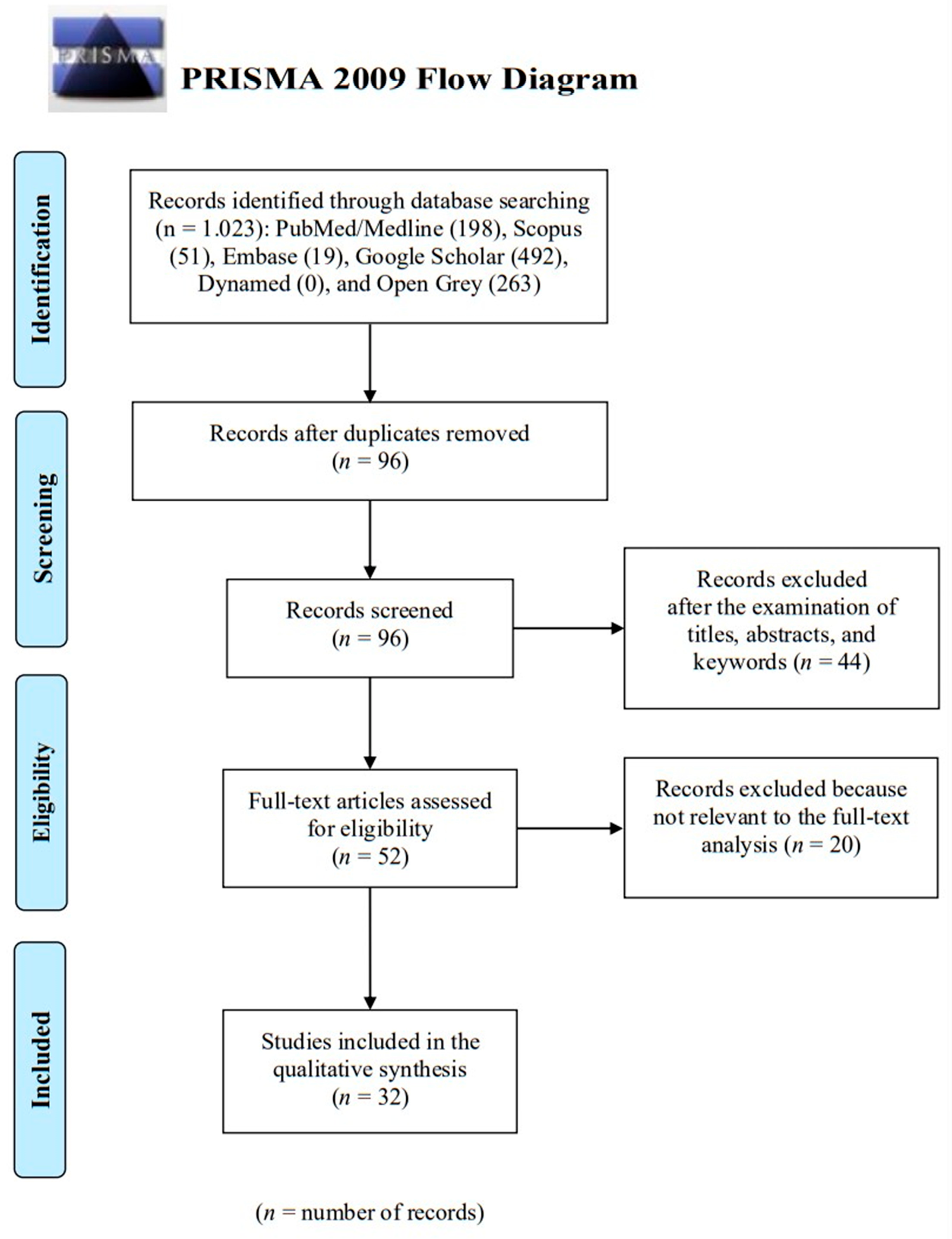
2. Methods
2.1. Search Strategy
- COVID-19;
- SARS-CoV-2;
- Coronavirus;
- Contaminated surface;
- Cross-infection;
- Prosthodontics;
- Dental ceramic;
- Glass-ceramic.
- Pubmed (Medline) = (“COVID-19” or “SARS-CoV-2” or “coronavirus” or “contaminated surface” or “cross-infection”) and (“prosthodontics” or “dental ceramic” or “glass-ceramic”);
- Google Scholar = title, abstract, keywords: “COVID-19” or “SARS-CoV-2” or “coronavirus” or “contaminated surface” or “cross-infection” and (prosthodontics or dental ceramic or glass-ceramic);
- Open Grey = (COVID-19) or (SARS-CoV-2) or (Coronavirus) or (contaminated surface) or (cross-infection) and (Prosthodontics or dental ceramic or glass-ceramic);
- Dynamed = (COVID-19; SARS-CoV-2; coronavirus) and/or (contaminated surface) and/or (cross-infection) and/or (prosthodontics or dental ceramic or glass-ceramic);
- Scopus = (TITLE-ABS-KEY ((COVID-19)) or TITLE-ABS-KEY ((SARS-CoV-2)) or TITLE-ABS-KEY ((coronavirus)) or TITLE-ABS-KEY ((contaminated and surface)) or TITLE-ABS-KEY ((cross-infection)) and TITLE-ABS-KEY ((prosthodontics or dental and ceramic or glass-ceramic)));
- Embase = (‘COVID-19’:ti,ab,kw or ‘SARS-CoV-2’:ti,ab,kw or coronavirus:ti,ab,kw or ‘contaminated surface’:ti,ab,kw or ‘cross infection’:ti,ab,kw) and (prosthodontics:ti,ab,kw or ‘dental ceramic’:ti,ab,kw or ‘glass ceramic’:ti,ab,kw).
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Calibration Process
3. Results
4. Discussion
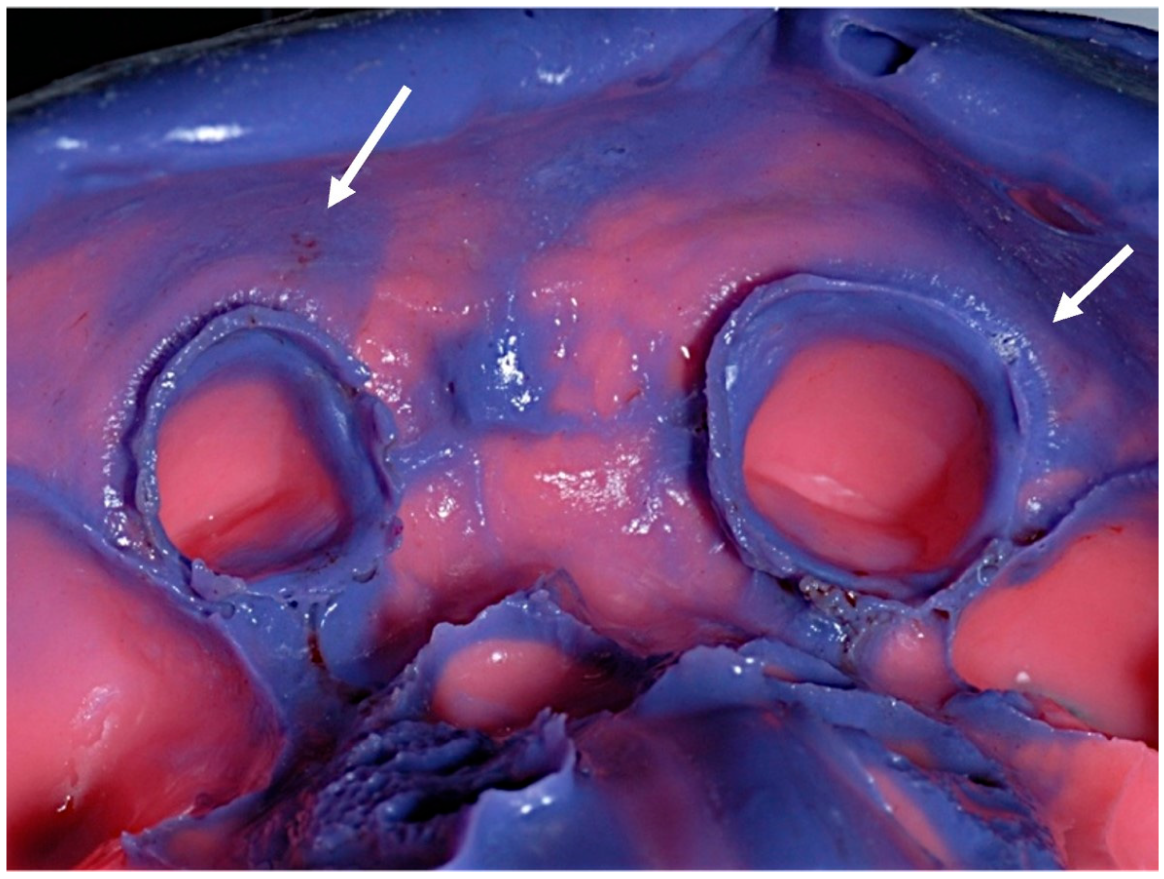
4.1. Dental Impression
4.2. Prosthodontics Aids
4.3. Metal–Ceramic Materials
4.4. All-Ceramic Materials
4.5. Pre-Check Triages
4.6. Limitations of the Search Methodology
4.7. Future Perspective
4.8. Summary of Risk Management of COVID-19
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of Public Health Interventions with the Epidemiology of the COVID-19 Outbreak in Wuhan, China. JAMA 2020, 323, 1915–1923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Centre for Disease Prevention and Control. An agency of the European Union. Available online: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed on 5 January 2022).
- Kakodkar, P.; Kaka, N.; Baig, M. A comprehensive literature review on the clinical presentation, and management of the pandemic coronavirus disease 2019 (COVID-19). Cureus 2020, 12, e7560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, Z.W.; Yuan, S.; Yuen, K.S.; Fung, S.Y.; Chan, C.P.; Jin, D.Y. Zoonotic origins of human coronaviruses. Int. J. Biol. Sci. 2020, 16, 1686–1697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araf, Y.; Akter, F.; Tang, Y.D.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 And Novel Therapeutics against Coronavirus (COVID-19). In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2021. [Google Scholar]
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 20 June 2022).
- Torjesen, I. COVID-19: Omicron may be more transmissible than other variants and partly resistant to existing vaccines, scientists fear. BMJ 2021, 375, n2943. [Google Scholar] [CrossRef]
- Coronavirus Disease 2019 (COVID-19) Situation Report–30. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200219-sitrep-30-covid-19.pdf?sfvrsn=3346b04f_2 (accessed on 31 December 2021).
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Euro Surveill 2020, 25, 2000062. [Google Scholar] [CrossRef] [Green Version]
- Kolifarhood, G.; Aghaali, M.; Mozafar Saadati, H.; Taherpour, N.; Rahimi, S.; Izadi, N.; Hashemi Nazari, S.S. Epidemiological and clinical aspects of COVID-19; a narrative review. Arch. Acad. Emerg. Med. 2020, 8, e41. [Google Scholar]
- Soler, Z.M.; Patel, Z.M.; Turner, J.H.; Holbrook, E.H. A primer on viral-associated olfactory loss in the era of COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 814–820. [Google Scholar] [CrossRef]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-reported olfactory and taste disorders in SARS-CoV-2 patients: A cross-sectional study. Clin. Infect. Dis. 2020, 71, 889–890. [Google Scholar] [CrossRef] [Green Version]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef]
- Gabutti, G.; D’Anchera, E.; Sandri, F.; Savio, M.; Stefanati, A. Coronavirus: Update Related to the Current Outbreak of COVID-19. Infect. Dis. Ther. 2020, 9, 241–253. [Google Scholar] [CrossRef]
- Chih-Cheng, L.; Tzu-Ping, S.; Wen-Chien, K.; Hung-Jen, T.; Po-Ren, H. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar]
- Yang, C.; Ma, Q.Y.; Zheng, Y.H.; Yang, Y.X. Transmission routes of 2019-novel coronavirus (2019-nCoV). Zhonghua Yu Fang Yi Xue Za Zhi 2020, 54, 374–377. [Google Scholar]
- Dietz, L.; Horve, P.; Coil, D.A.; Fretz, M.; Eisen, J.A.; Van Den Wymelenberg, K. 2019 Novel Coronavirus (COVID-19) pandemic: Built environment considerations to reduce transmission. mSystems 2020, 5, e00245-20. [Google Scholar] [CrossRef] [Green Version]
- To, K.K.; Tsang, O.T.; Yip, C.C.; Chan, K.H.; Wu, T.C.; Chan, J.M.; Leung, W.S.; Chik, T.S.; Choi, C.Y.; Kandamby, D.H.; et al. Consistent Detection of 2019 Novel Coronavirus in Saliva. Clin. Infect. Dis. 2020, 71, 841–843. [Google Scholar] [CrossRef] [Green Version]
- Ong, S.W.X.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.T.; Wong, M.S.Y.; Marimuthu, K. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA 2020, 323, 1610–1612. [Google Scholar] [CrossRef] [Green Version]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and future challenges for dental and oral medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Dropulic, L.K.; Lederman, H.M. Overview of infections in the immunocompromised host. Microbiol. Spectr. 2016, 4, 1–50. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Meo, S.A.; Alhowikan, A.M.; Al-Khlaiwi, T.; Meo, I.M.; Halepoto, D.M.; Iqbal, M.; Usmani, A.M.; Hajjar, W.; Ahmed, N. Novel coronavirus 2019-nCoV: Prevalence, biological and clinical characteristics comparison with SARS-CoV and MERS-CoV. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2012–2019. [Google Scholar]
- Barenghi, L.; Barenghi, A.; Cadeo, C.; Di Blasio, A. Innovation by Computer-Aided Design/Computer-Aided Manufacturing technology: A look at infection prevention in dental settings. Biomed. Res. Int. 2019, 2019, 6092018. [Google Scholar] [CrossRef]
- Sofou, A.; Larsen, T.; Fiehn, N.E.; Owall, B. Contamination level of alginate impressions arriving at a dental laboratory. Clin. Oral Investig. 2002, 6, 161–165. [Google Scholar] [CrossRef]
- Al Shikh, A.; Milosevic, A. Effectiveness of alcohol and aldehyde spray disinfectants on dental impressions. Clin. Cosmet. Investig. Dent. 2020, 12, 25–30. [Google Scholar] [CrossRef] [Green Version]
- British Dental Association. Health Technical Memorandum 01-05: Decontamination in Primary Care Dental Practices. London: Department of Health. Available online: https://www.england.nhs.uk/wp-content/uploads/2021/05/HTM_01-05_2013.pdf (accessed on 31 December 2021).
- Kotsiomiti, E.; Tzialla, A.; Hatjivasiliou, K. Accuracy and stability of impression materials subjected to chemical disinfection—A literature review. J. Oral Rehabil. 2008, 35, 291–299. [Google Scholar] [CrossRef]
- Fathizadeh, H.; Maroufi, P.; Momen-Heravi, M.; Dao, S.; Köse, Ş.; Ganbarov, K.; Pagliano, P.; Esposito, S.; Kafil, H.S. Protection and disinfection policies against SARS-CoV-2 (COVID-19). Infez. Med. 2020, 28, 185–191. [Google Scholar]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmannb, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [Green Version]
- Prabu, P.; Kattak, S.A.K.; Prabu, N.; Beenu, V.; Nair, S.J.; Sreeleksmi, M.S. Asepsis in prosthodontics. J. Prosthet. Implant Dent. 2021, 4, 67–71. [Google Scholar]
- Punj, A.; Bompolaki, D.; Garaicoa, J. Dental impression materials and techniques. Dent. Clin. North Am. 2017, 61, 779–796. [Google Scholar] [CrossRef]
- Markarian, R.A.; da Silva, R.L.B.; Burgoa, S.; Pinhata-Baptista, O.H.; No-Cortes, J.; Cortes, A.R.G. Clinical relevance of Digital Dentistry during COVID-19 outbreak: A scoped review. Braz. J. Oral Sci. 2020, 19, e200201. [Google Scholar] [CrossRef]
- Naylor, W.P. Prosthodontic items of interest. Int. J. Prosthodont. 1992, 5, 188–189. [Google Scholar]
- Rampal, N.; Pawah, S.; Kaushik, P. Infection Control in Prosthodontics. J. Oral Health Comm. Dent. 2010, 4, 7–11. [Google Scholar] [CrossRef]
- ADA Council on Scientific Affairs; ADA Council on Dental Practice. Infection control recommendations for the dental and the dental laboratory. J. Am. Dent. Assoc. 1996, 127, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Sumanth, K.S.; Poovani, S.; Shetty, G.; Kumar, N.S.B.; Sudhakar, S.K. Infection Control Protocol in Prosthodontic—A Review. Int. J. Scien. Res. 2019, 8, 75–78. [Google Scholar]
- Council on dental materials. Infection control recommendation for a dental office and dental laboratory by the council of dental materials. J. Am. Dent. Assoc. 1988, 116, 241–248. [Google Scholar] [CrossRef]
- Sarangi, D. Infection Control in Prosthodontics: A Review. Indian J. Forensic Med. Toxicol. 2020, 14, 8180–8183. [Google Scholar]
- Bhat, V.S.; Shetty, M.S.; Shenoy, K.K. Infection control in the prosthodontic laboratory. J. Indian Prosthodont. Soc. 2007, 7, 62–65. [Google Scholar] [CrossRef]
- Jain, S.; Yadav, B.; Phogat, S.; Madan, R. Disinfection in prosthodontics. Int. J. Dent. Health Sci. 2014, 1, 779–787. [Google Scholar]
- Zidan, O.; Ferguson, G.C. The retention of complete crowns prepared with three different tapers and luted with four different cements. J. Prosthet. Dent. 2003, 89, 565–571. [Google Scholar] [CrossRef]
- Gönüldaş, F.; Öztürk, C.; Atalay, P.; Öztaş, D. Influence of different surface finishing techniques on machinable feldspathic and leucite-reinforced ceramics. Dent. Mater. J. 2019, 38, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Maroulakos, G.; Thompson, G.A.; Kontogiorgos, E.D. Effect of cement type on the clinical performance and complications of zirconia and lithium disilicate tooth-supported crowns: A systematic review. Report of the Committee on Research in Fixed Prosthodontics of the American Academy of Fixed Prosthodontics. J. Prosthet. Dent. 2019, 121, 754–765. [Google Scholar] [CrossRef]
- Kim, M.J.; Kim, K.H.; Kim, Y.K.; Kwon, T.Y. Degree of conversion of two dual-cured resin cements light-irradiated through zirconia ceramic disks. J. Adv. Prosthodont. 2013, 5, 464–470. [Google Scholar] [CrossRef]
- Kern, M. Bonding to oxide ceramics-laboratory testing versus clinical outcome. Dent. Mater. 2015, 31, 8–14. [Google Scholar] [CrossRef]
- Özcan, M.; Bernasconi, M. Adhesion to zirconia used for dental restorations: A systematic review and meta-analysis. J. Adhes. Dent. 2015, 17, 7–26. [Google Scholar]
- Zemouri, C.; de Soet, H.; Crielaard, W.; Laheij, A. A scoping review on bio-aerosols in healthcare and the dental environment. PLoS ONE 2017, 12, e0178007. [Google Scholar] [CrossRef]
- Akin, H.; Karabay, O.; Toptan, H.; Furuncuoglu, H.; Kaya, G.; Akin, E.G.; Koroglu, M. Investigation of the Presence of SARS-CoV-2 in Aerosol After Dental Treatment. Int. Dent. J. 2022, 72, 211–215. [Google Scholar] [CrossRef]
- Sa, Y.; Lin, W.S.; Morton, D.; Huang, C. Coronavirus disease 2019 (COVID-19): Experiences and protocols from the Department of Prosthodontics at the Wuhan University. J. Prosthet. Dent. 2021, 126, 41–50. [Google Scholar] [CrossRef]
- Batista, A.U.D.; Silva, P.L.P.D.; Melo, L.A.; Carreiro, A.D.F.P. Prosthodontic practice during the COVID-19 pandemic: Prevention and implications. Braz. Oral Res. 2021, 35, e049. [Google Scholar] [CrossRef]
- COVIDental Collaboration Group. The COVID-19 pandemic and its global effects on dental practice. An international survey. J. Dent. 2021, 114, 103749. [Google Scholar] [CrossRef]
- Abdelrahman, H.; Atteya, S.; Ihab, M.; Nyan, M.; Maharani, D.A.; Rahardjo, A.; Shaath, M.; Aboalshamat, K.; Butool, S.; Shamala, A.; et al. Dental practice closure during the first wave of COVID-19 and associated professional, practice and structural determinants: A multi-country survey. BMC Oral Health 2021, 21, 243. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection when Novel Coronavirus (2019-nCoV) Infection is Suspected: Interim Guidance. 28 January 2020. Available online: https://apps.who.int/iris/handle/10665/330893 (accessed on 10 December 2021).
- Fiorillo, L.; Cervino, G.; Matarese, M.; D’Amico, C.; Surace, G.; Paduano, V.; Fiorillo, M.T.; Moschella, A.; Bruna, A.; Romano, G.L.; et al. COVID-19 Surface Persistence: A Recent Data Summary and Its Importance for Medical and Dental Settings. Int. J. Environ. Res. Public Health 2020, 17, 3132. [Google Scholar] [CrossRef]
- Eggers, M.; Koburger-Janssen, T.; Eickmann, M.; Zorn, J. In vitro bactericidal and virucidal efficacy of povidone-iodine gargle/mouthwash against respiratory and oral tract pathogens. Infect. Dis. Ther. 2018, 7, 249–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Bizzoca, M.E.; Campisi, G.; Lo Muzio, L. COVID-19 Pandemic: What Changes for Dentists and Oral Medicine Experts? A Narrative Review and Novel Approaches to Infection Containment. Int. J. Environ. Res. Public Health 2020, 17, 3793. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Y.; Guler, C. Evaluation of different sterilization and disinfection methods on commercially made preformed crowns. J. Indian Soc. Pedod. Prev. Dent. 2008, 26, 162. [Google Scholar] [CrossRef]
- Porto, V.C.; Balsalobre, R.; Pegoraro, L.F.; Valle, A.L. Surface roughness analysis of ceramic systems after disinfection and sterilization procedures. Braz. J. Oral Sci. 2006, 5, 963–966. [Google Scholar]
- Cervino, G.; Oteri, G. COVID-19 Pandemic and Telephone Triage before Attending Medical Office: Problem or Opportunity? Medicina 2020, 56, 250. [Google Scholar] [CrossRef]
- Basilicata, M.; Zarone, F.; Leone, R.; Guerriero, C.; Di Lauro, M.; Franco, R.; Bernardini, S.; Noce, A.; Bollero, P.; Sorrentino, R. Impact of SARS-CoV-2 on dentistry: A review of literature. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 3386–3398. [Google Scholar]
- Induri, S.N.R.; Chun, Y.C.; Chun, J.C.; Fleisher, K.E.; Glickman, R.S.; Xu, F.; Ioannidou, E.; Li, X.; Saxena, D. Protective Measures against COVID-19: Dental Practice and Infection Control. Healthcare 2021, 9, 679. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Telephonic triage |
| Date: Name: Surname: Reason for the visit: |
Have you had at least one of the following symptoms of respiratory illness in the last 14 days?
|
In the past 14 days, have you or your family member had:
|
| Did you take the test for SARS-CoV-2 and have an uncertain or positive result? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorrentino, R.; Basilicata, M.; Ruggiero, G.; Mauro, M.I.D.; Leone, R.; Bollero, P.; Zarone, F. A Review on Risk Management of Coronavirus Disease 19 (COVID-19) Infection in Dental Practice: Focus on Prosthodontics and All-Ceramic Materials. Prosthesis 2022, 4, 338-352. https://doi.org/10.3390/prosthesis4030028
Sorrentino R, Basilicata M, Ruggiero G, Mauro MID, Leone R, Bollero P, Zarone F. A Review on Risk Management of Coronavirus Disease 19 (COVID-19) Infection in Dental Practice: Focus on Prosthodontics and All-Ceramic Materials. Prosthesis. 2022; 4(3):338-352. https://doi.org/10.3390/prosthesis4030028
Chicago/Turabian StyleSorrentino, Roberto, Michele Basilicata, Gennaro Ruggiero, Maria Irene Di Mauro, Renato Leone, Patrizio Bollero, and Fernando Zarone. 2022. "A Review on Risk Management of Coronavirus Disease 19 (COVID-19) Infection in Dental Practice: Focus on Prosthodontics and All-Ceramic Materials" Prosthesis 4, no. 3: 338-352. https://doi.org/10.3390/prosthesis4030028