1. Introduction
In the healthcare industry, employees are often occupied with caring for a large number of patients [
1]. These individuals depend on healthcare providers to address their needs when they experience health-related problems. There are instances where patients may be unable to request immediate assistance, such as those in the ICU dealing with delirium, which is a prevalent complication that impairs their ability to seek help [
2]. Additionally, relying solely on direct observations by staff members for patient monitoring can result in operational vulnerabilities [
3]. Consequently, it is crucial to establish a system that can assist individuals without the need for human intervention. One potential solution involves utilizing sensor-equipped devices capable of automatically detecting changes or movements made by immobile patients. This technology would allow healthcare providers to swiftly monitor and respond through automatic notifications in emergency situations, such as patients falling off their beds while asleep or disconnecting from medical equipment due to excessive movement during sleep. Implementing this innovative approach would guarantee prompt responses and improve the quality of care provided, leading to positive outcomes for both caregivers and patients.
Similar to physiological monitoring devices, the aforementioned technologies employ a comparable approach. They constantly keep track of crucial signs like heart rate, blood pressure, respiratory rate, and oxygen saturation. Even minor fluctuations in these vital signs can indicate the presence of a life-threatening event when they occur within 24 h prior [
4]. As a result, these devices can be programmed to produce alarms or notifications when certain thresholds are surpassed or specific patterns are identified. This has the potential to enable early detection of patient deterioration during hospitalization so that healthcare professionals can intervene promptly [
5]. Along with patient-operated devices and physiological monitors, centralized alert systems are also available. These systems gather information from multiple sources, including monitoring devices and electronic health records, to create comprehensive alerts. By utilizing algorithms and rules, they analyze the data and detect critical events or unusual patterns. The identified issues are then communicated to relevant healthcare personnel for prompt action.
Different alert systems have been studied before, including alarms that notify caregivers when a patient tries to get out of bed without help [
6]. These alarms are effective but need to be part of a larger plan for preventing falls. However, thanks to technological advancements, there are now more advanced options available, such as wearable devices and smart sensors placed discreetly on or near patients, for real-time monitoring while causing minimal disruption or interference.
As anticipated, there is currently a lack of sensor-based smart systems that notify healthcare staff about the activity levels of bed-ridden patients. Existing systems primarily focus on alerting staff when patients become disconnected from monitoring machines. Therefore, in this ‘technical note’, we present the possibility of using affordable sensors to monitor common movements experienced by hospital-bed-bound patients and assess their feasibility.
A unique approach that utilizes sensors to track a patient’s body positions and movements while they are in bed can serve as an effective solution. This technology not only allows for quick responses but also ensures the safety and well-being of patients without disrupting their sleep, thereby improving the overall quality of care provided. Additionally, implementing alerts based on patient movement can greatly enhance efficiency in healthcare settings by reducing unnecessary check-ins and allowing staff to focus on areas where attention is most needed. Integrating such an alert system represents a valuable investment for healthcare facilities looking to prioritize patient comfort, safety, and care while simultaneously enhancing staff productivity through real-time information delivery, faster response times, and increased operational efficiency.
2. Methods
The methods section is split into multiple subsections, which cover the concept and processing of Euler angles using Procrustes analysis. Additionally, the last subsection describes how various body movements are differentiated based on a series of comparative analyses.
2.1. Euler Angles
One common method for representing an object’s orientation in three-dimensional space is by measuring Euler angles relative to a fixed coordinate system. They offer a convenient way to describe an object’s rotation along its longitudinal, lateral, and vertical axes, i.e., Euler angles involve rotations around each of the three coordinate axes; thus, they are extensively utilized in aerospace engineering, robotics, and computer graphics. For example, video game programming utilizes Euler angles to animate 3D characters and objects.
This study utilizes Euler angles to assess the body posture of patients in bed and monitor their movements over a specific time frame. We examine the changes in Euler angles that occur during common movements performed by patients while lying down. Our goal is to identify distinct patterns in these angle variations that are indicative of these movements. The selection of Euler angles is suitable for this investigation as they offer a straightforward and concise method for representing the orientation of the human body in three-dimensional space. Previous research studies have also made use of Euler angles in their investigations into human body movements [
7]. Euler angles provide a reliable method for healthcare professionals to assess body posture and motion accurately. This enables accurate monitoring of patient conditions and allows for necessary adjustments to improve their comfort and overall well-being.
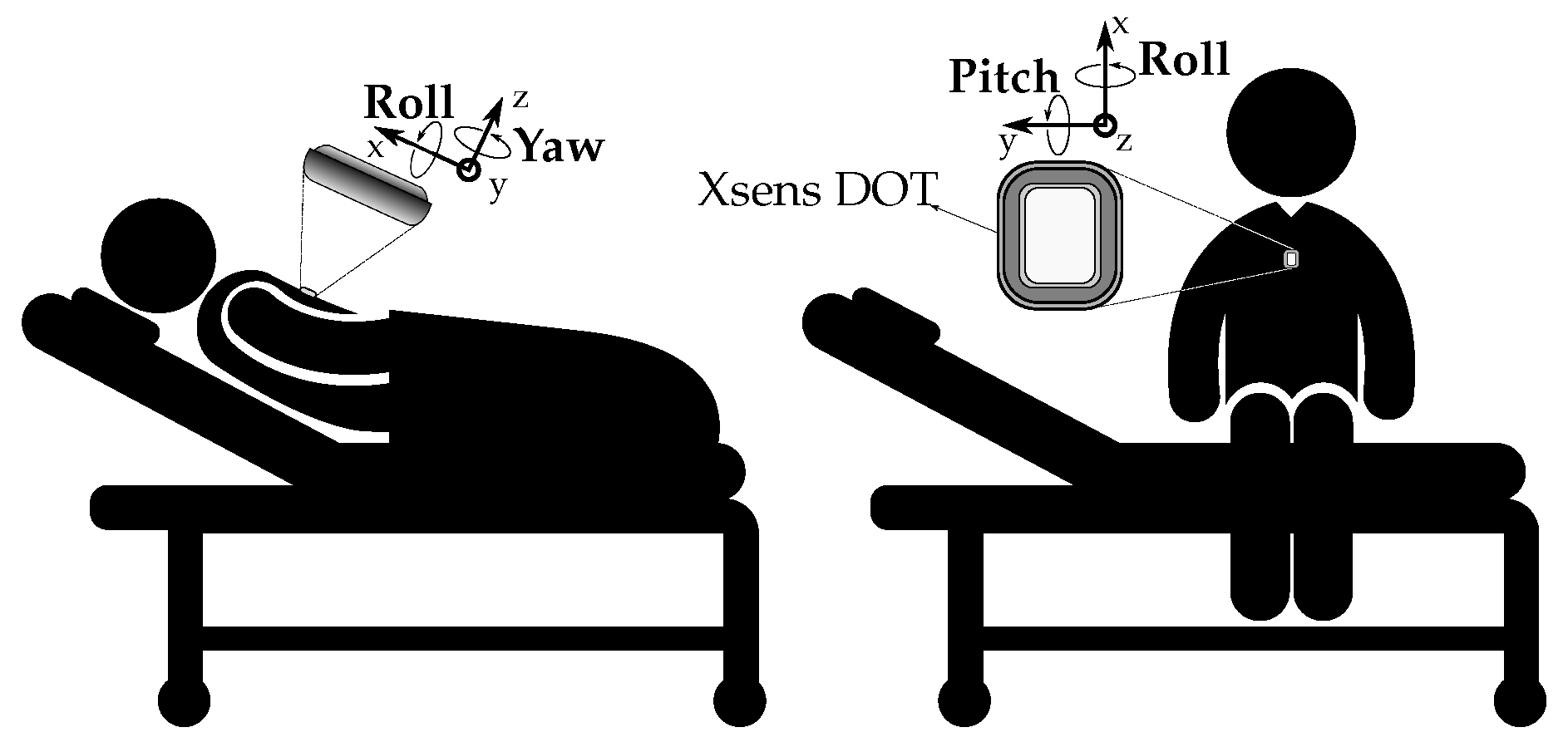
For our research purposes, we utilize Xsens DOT sensors (Movella, Inc., Henderson, NV, USA), which include a gyroscope for determining 3D angular velocity, an accelerometer for measuring 3D acceleration, and a magnetometer to detect the earth’s magnetic field in three dimensions. The fusion algorithms used by Xsens improve the accuracy of orientation measurements while also enabling detection of free acceleration. Furthermore, Bluetooth technology allows for the precise wireless tracking of human body movements, making it a valuable tool in our study.
The orientation provided by Xsens DOT pertains to the alignment of the sensor coordinate system in relation to the local earth coordinate system. An output option available through Xsens DOT is a north-referenced yaw or heading. The default orientation output is presented in an east–north–up (ENU) configuration where the roll, pitch, and yaw are set at 0 degrees, where the x-axis aligns with east, the y-axis with north, and the z-axis upward. In this frame of reference, positive values for x signify magnetic east; positive values for y indicate magnetic north; while Z corresponds to the upwards direction. The system is derived from the rotational movements of aircraft during flight, which are defined by three axes: pitch, roll, and yaw. Pitch refers to the upward or downward movement of an airplane’s nose with respect to a horizontal axis running between its wings. Roll entails the side-to-side rotation around an axis extending from the tail to nose of the airplane, enabling it to rock back and forth laterally. Yaw involves rotating around a vertical axis so that the plane’s nose moves sideways in either direction horizontally. Refer to
Figure 1 for an illustration of pitch, roll, and yaw relative to a patient in both supine and sitting positions.
Real-time analysis of a patient’s bodily movements can be determined by the specific sequence of rotational actions. For instance, in
Figure 1, when a patient tries to sit up from a supine position, pitch is identified first followed by roll. The system has the capability to notify healthcare professionals if assistance may be needed for the patient. Conversely, an immediate intervention is required when pitch immediately follows after both roll and pitch, indicating that the individual fell forward while trying to stand up after sitting upright. To put it concisely, the specific sequence of rotational movements mentioned above has corresponding effects on a patient’s bodily stance and motion. Specifically, pitch–roll pertains to rising from a prone position into sitting posture, while pitch–roll–pitch indicates that the patient rose to sit but subsequently fell forward off of their bed.
2.2. Procrustes Analysis
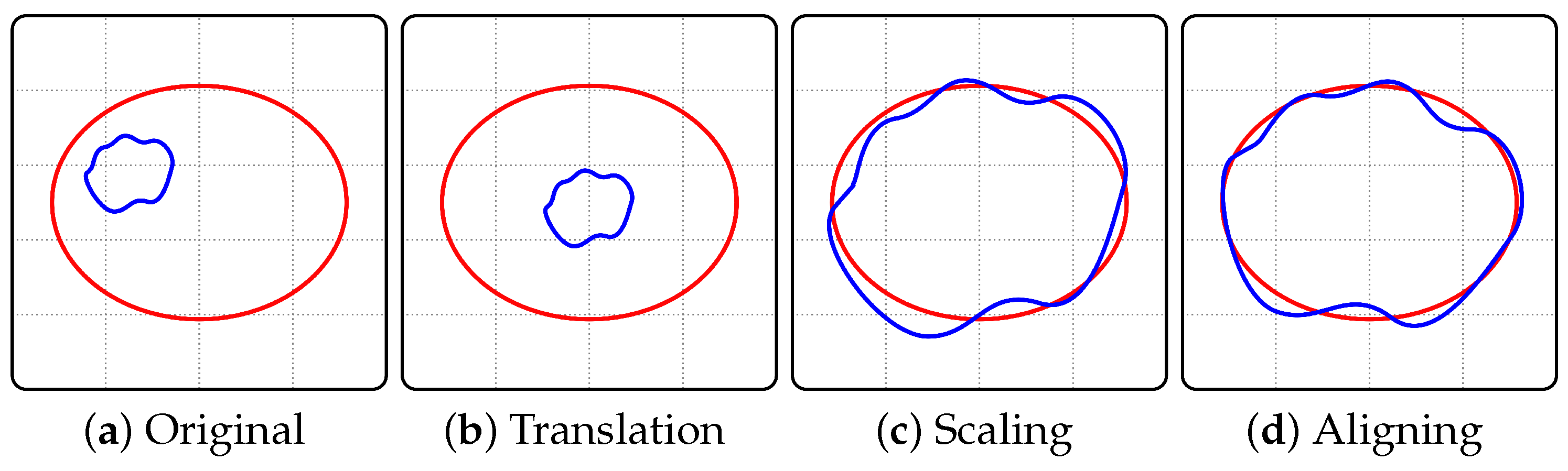
To differentiate the aforementioned measurements, it is essential to perform a comparative analysis of these measured curves. Hence, they first need to be aligned in an optimal manner prior to any comparison process. This can be achieved through Procrustes superimposition, which entails finding the optimal translation, rotation, and uniform scaling for each object (
Figure 2). In essence, this involves adjusting both the spatial placement and dimensions such that similarities in size and arrangement can be attained while minimizing shape differences quantified by calculating the Procrustes distance separating said curves.
Procrustes shape analysis is a statistical technique used to compare and analyze shapes. The goal of Procrustes shape analysis is to remove the effects of translation, rotation, and scaling from shapes, allowing for meaningful comparisons. The analysis begins with a set of shapes represented by landmark points. The first step is to align the shapes by removing the effects of translation, rotation, and scaling. This is achieved by minimizing the sum of squared differences between corresponding landmarks across all shapes. The result is a set of aligned shapes that are scaled, rotated, and translated to best fit each other. Next, the aligned shapes are subjected to Procrustes superimposition, where further adjustments are made to remove the effects of size and orientation. This is performed by finding a consensus shape, known as the Procrustes mean, which represents the average shape of the aligned set. Each aligned shape is then individually transformed to match the Procrustes mean by scaling, rotating, and translating. After alignment and superimposition, statistical analyses can be performed on the shape data.
Procrustes shape analysis is a useful tool for the quantification and comparison of shape dissimilarities between individuals or groups, and is commonly used in biomedical studies [
8]. This technique has been employed in diverse fields, such as biology, anthropology, paleontology, and computer vision. There are various potential uses for this tool, including its application in the assessment of classification systems that categorize designs according to shape data sets [
9]. Hence, in this study, it is employed to differentiate patients’ movement patterns while in bed based on Euler angle time series curves.
2.3. Comparative Analysis
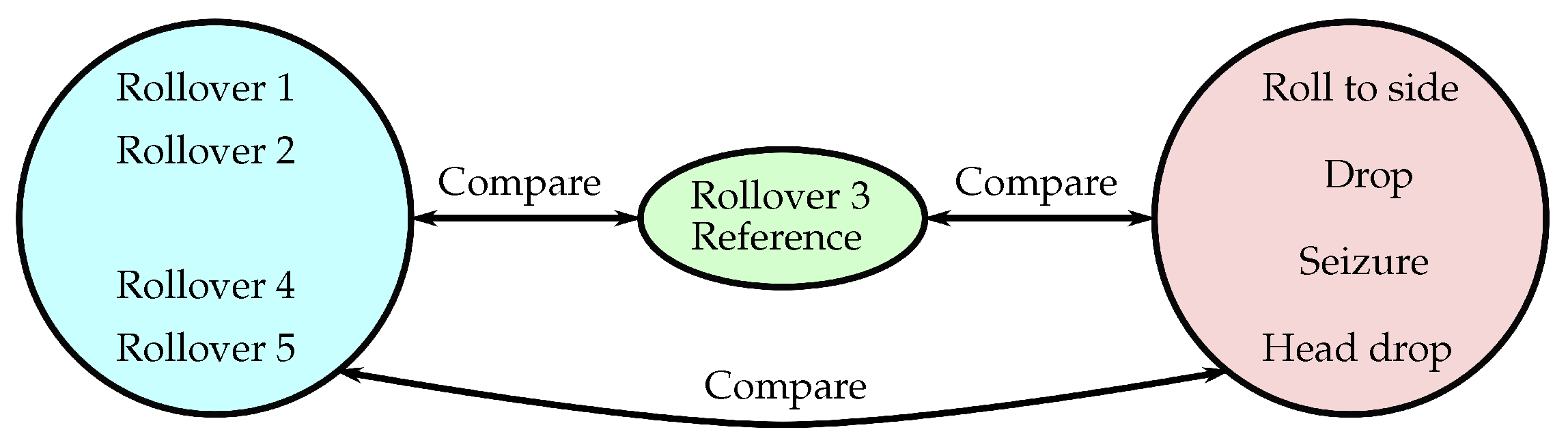
By placing the sensors on advanced medical mannequins, Euler angles were measured while executing several typical supine body movements. These maneuvers include a range of postural transitions, such as rolling from the back to the stomach, slipping from the bed surface onto the floor below, turning towards one’s side, experiencing a seizure, and succumbing to head droopiness. By performing a Procrustes shape analysis, dissimilarity values are obtained and utilized to distinguish between various movements by comparing them with reference shape data sets. In case an individual executes multiple rollovers (i.e., transitioning from a back to a stomach position), then the dissimilarity values for such transitions (compared with reference shape data set) must be significantly different in comparison to rolling over towards either side, so as to accurately differentiate among these distinct maneuvers.
To compare different movement types, it is expected that we will find low dissimilarity values when each movement type is compared to another of its own kind. Conversely, higher dissimilarity values should emerge through comparisons between a reference data set (e.g., Rollover 3) and other kinds of bodily movements. Therefore, in analyzing a specific movement’s curve shape data set, it is juxtaposed with standard sets of body motion data (
Figure 3); this comparison allows for finding the smallest dissimilarity value—significantly lower than others—which then represents the given action associated with that reference motion. Hence, the body movement is identified.
To summarize, sensors placed on advanced medical mannequins were used to measure the Euler angles during various bodily movements. These measurements were then compared using a Procrustes shape analysis to obtain dissimilarity values. These values are pivotal in differentiating between various movements when compared with a reference shape data set. For instance, if a patient performs multiple rollovers (e.g., transitioning from a back to a stomach position), the dissimilarity values for such transitions (compared with a reference shape data set) must be significantly lower in comparison to rolling over towards either side. This will help accurately differentiate among these different maneuvers. It is anticipated that one can identify body movements by comparing a specific movement’s curve shape data set against standard sets of body motion data. This comparison aims to identify the dissimilarity value that distinctly represents the given action associated with that reference motion, thereby identifying the body movement.
3. Results
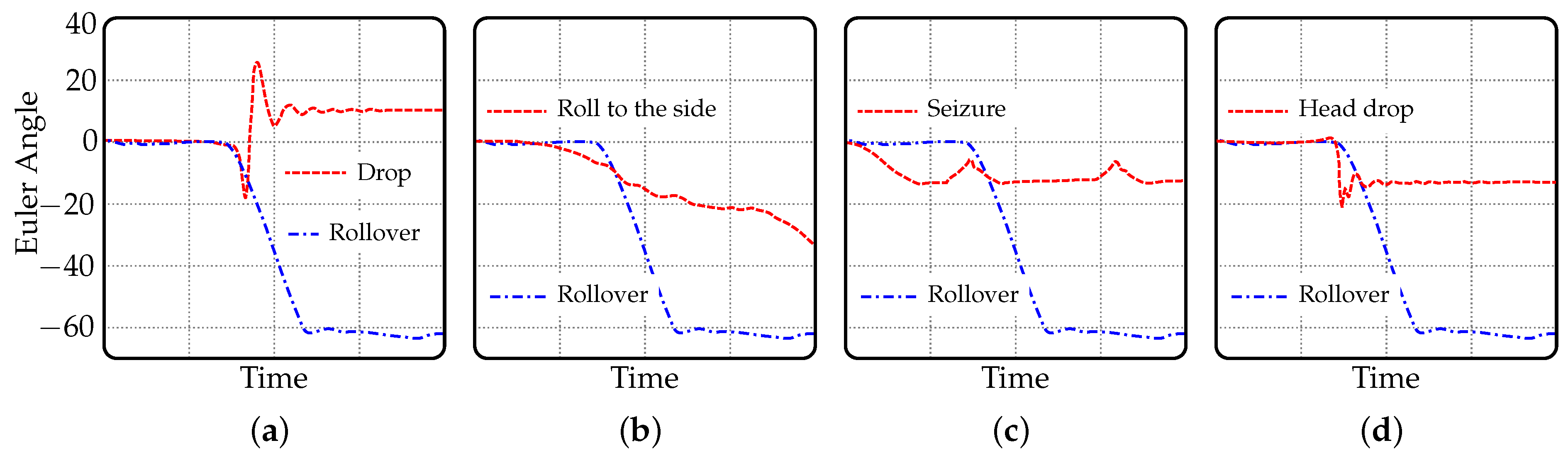
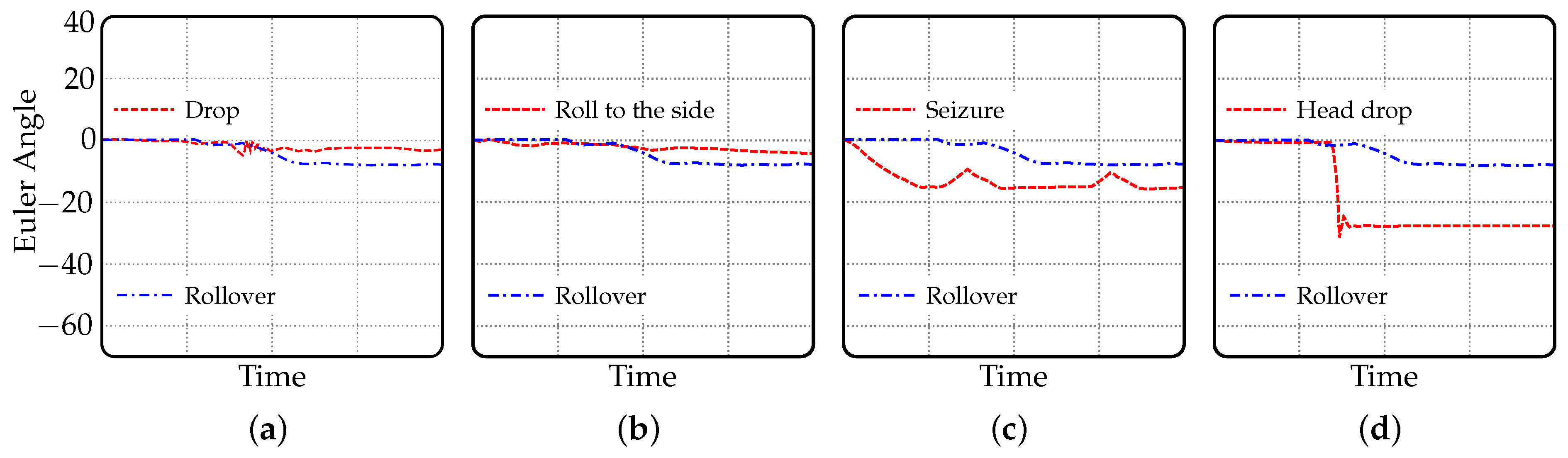
The graphs in
Figure 4 display the Euler angles revolving around the x-axis, namely the roll (refer to illustration in
Figure 1). They exhibit rotational movement angles linked to various bodily motions performed on a bed in comparison to rolling over—which is deemed the most common of them. While pitch and yaw also constitute rotational movements, they are not as apparent as roll; however, it can be expected that pitch will surpass yaw’s level of prominence. On similar grounds,
Figure 5 illustrates Euler angles relevant to identical bodily activities executed while pitching (i.e., rotating about y-axis). Both illustrations (
Figure 4 and
Figure 5) retain an equivalent value range for comparative purposes. As a result of its minimal association with physical movements tested, yaw does not manifest itself.
In other words,
Figure 4 and
Figure 5 display graphs of Euler angles representing rotational movements performed by a patient lying on a bed. These rotational movements can be interpreted as different types of movements or actions performed by the patient.
Figure 4 demonstrates Euler angles that are revolving around the x-axis, also referred to as the roll. Each chart in the figure reflects the roll value during different physical movements, such as rolling over, dropping, rolling to the side, having a seizure, and a head drop. The blue dot-dashed line in each of these plots represents the standard motion of rolling over, which appears to be a common reference motion against which other types of movements are compared.
Figure 5, on the other hand, illustrates Euler angles which correspond to the y-axis, denoted as pitch. These figures show the pitch-related values during the same types of bodily activities. This is similar to
Figure 4, but here, the rotation is based on a different axis, changing the impact and detectability of specific movements. Again, the blue dot-dashed line represents the standard motion of rolling over. Each of the types of movements is matched with the standard of rolling over to give a visual representation of how these movements differ from the norm. This identification helps in discerning one type of movement from another, potentially assisting in patient monitoring applications.
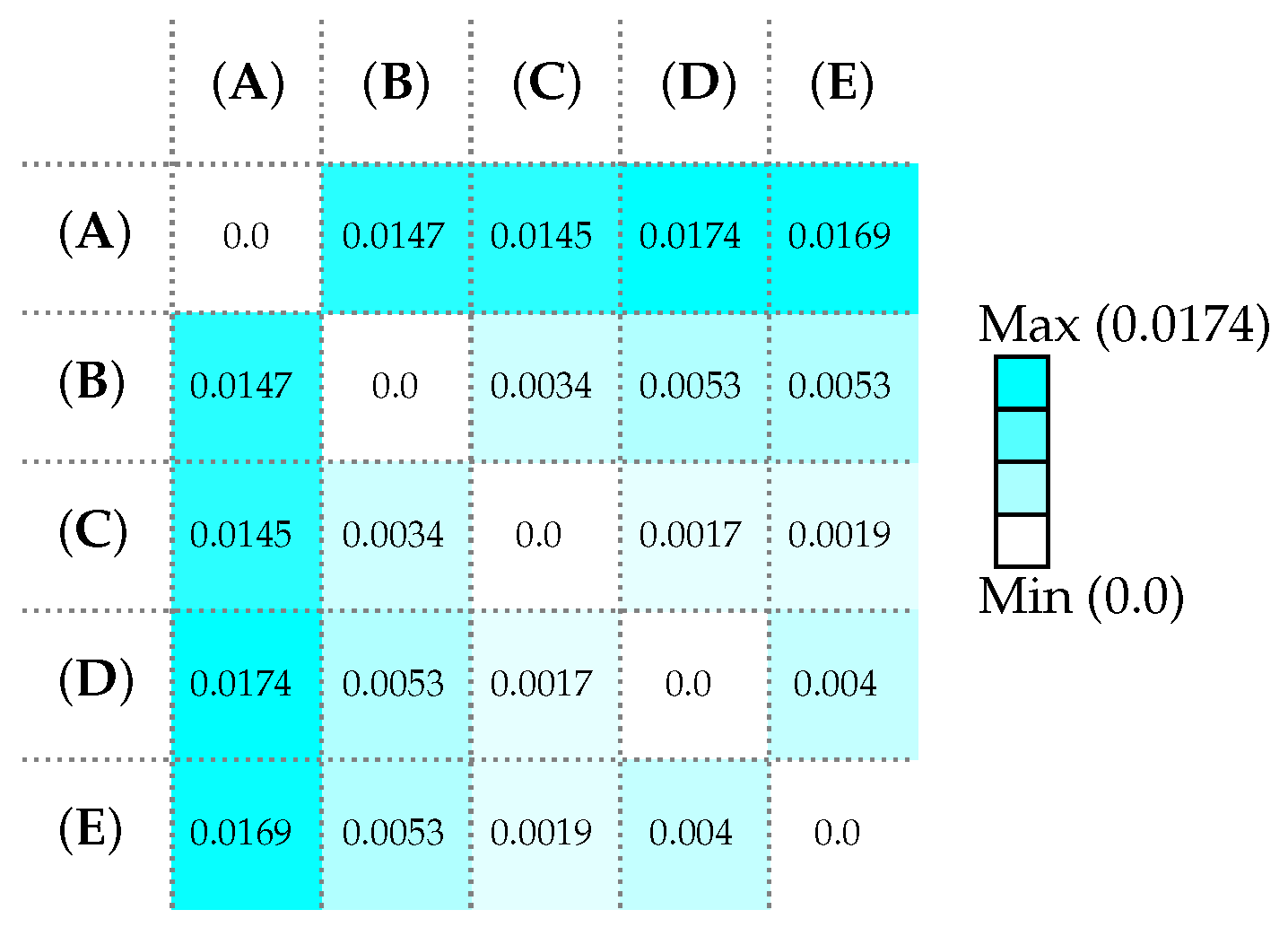
Figure 6 provides a summary of the dissimilarity values resulting from comparing each body movement with other movements. When two identical shapes are compared, inevitably their dissimilarity value is zero. The analysis indicates that the rollover movement generates higher dissimilarity values when paired with different types of motion in comparison to others. The inquiry persists as to whether there will be a noteworthy reduction in the dissimilarity values when comparing a specific motion with analogous motions. Each of the aforementioned movements are juxtaposed against motions with corresponding characteristics, and the variances in resemblance (i.e., dissimilarity values) are delineated in
Figure 7. Upon observing the values, it can be inferred that dissimilarity values have a relatively low magnitude when comparing similar data sets of shape and a larger magnitude when compared with different types of movement.
Specifically,
Figure 6 and
Figure 7 provide information regarding the dissimilarity values resulting from comparing different body movements.
Figure 6 presents a matrix of dissimilarity values comparing five different types of movements: rolling over from the back to the stomach (A), dropping from bed (B), rolling to the side (C), experiencing a seizure (D), and head drops (E). The dissimilarity value is zero when two identical movements are compared. The analysis indicates that the rollover movement generates higher dissimilarity values when paired with different types of motion in comparison to others.
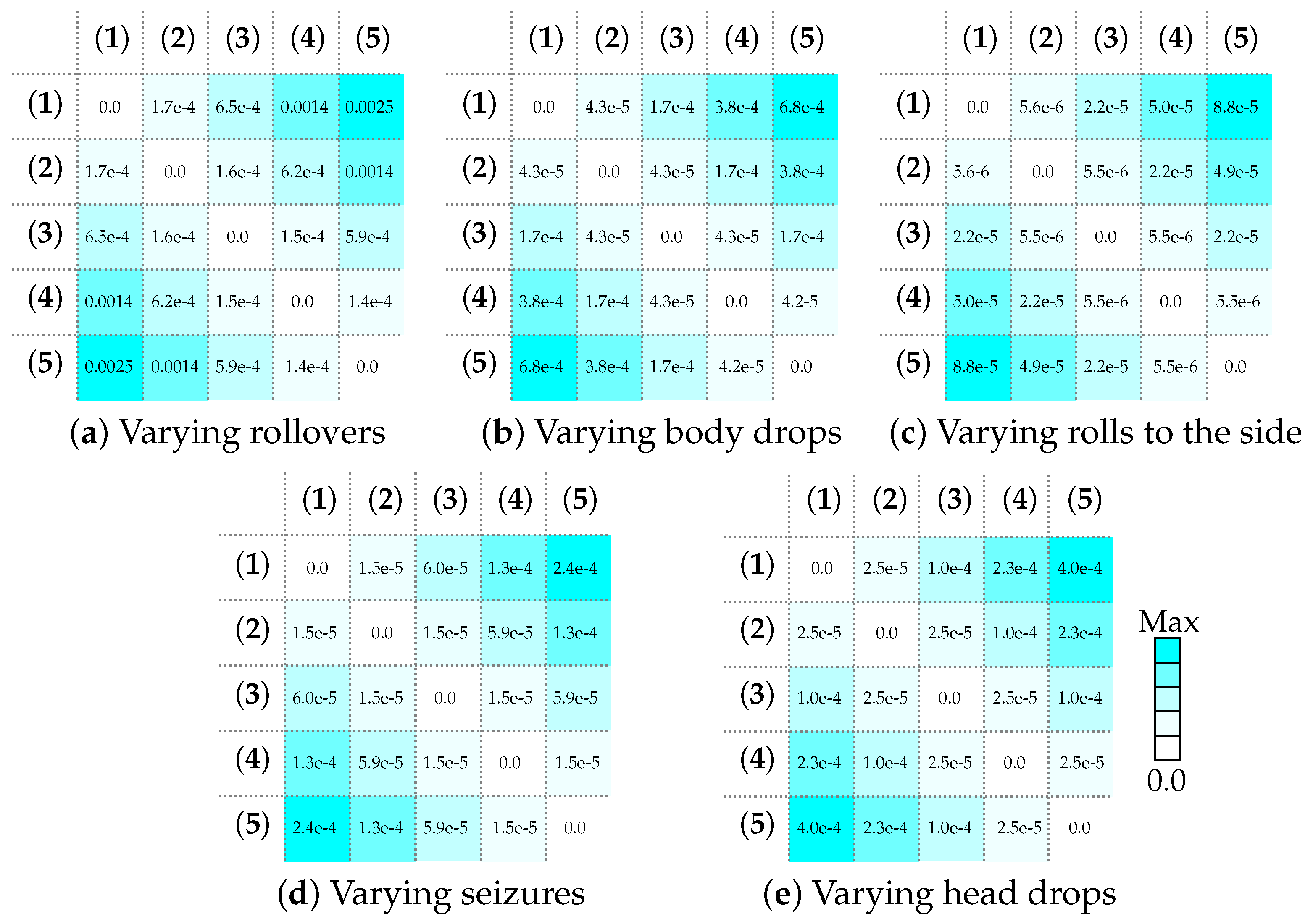
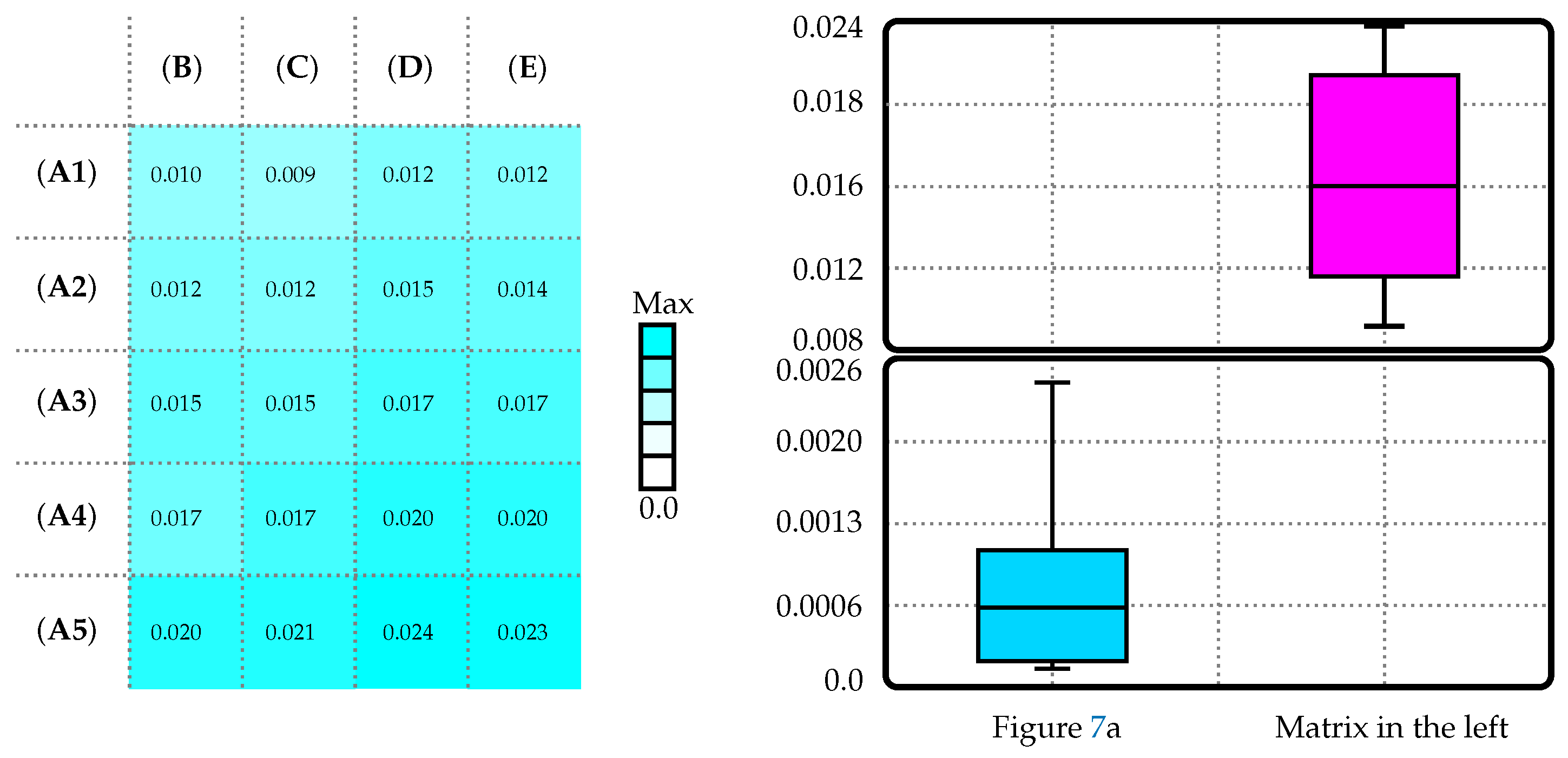
Figure 7, on the other hand, illustrates the dissimilarity values of varying types of the same body movements when compared against each other. It includes separate dissimilarity matrices for varying rollovers, body drops, rolls to the side, seizures, and head drops. For example, in
Figure 7a, the first row represents the varying dissimilarity values when rollover measurement #1 is compared to four other rollover measurements. The purpose of this is to evaluate if similar types of movements show lower dissimilarity values compared to dissimilar types of movements. In other words, it is testing if the dissimilarity values can help distinguish between different movements. The results show relatively low dissimilarity values when comparing similar data sets of shape (same type of movements) and a larger magnitude when compared with different types of movement. In combination,
Figure 6 and
Figure 7 offer a statistical representation of the variability and differences in movements as detected by their respective Euler angles, suggesting that these differences could be used to identify and categorize different types of patient movements.
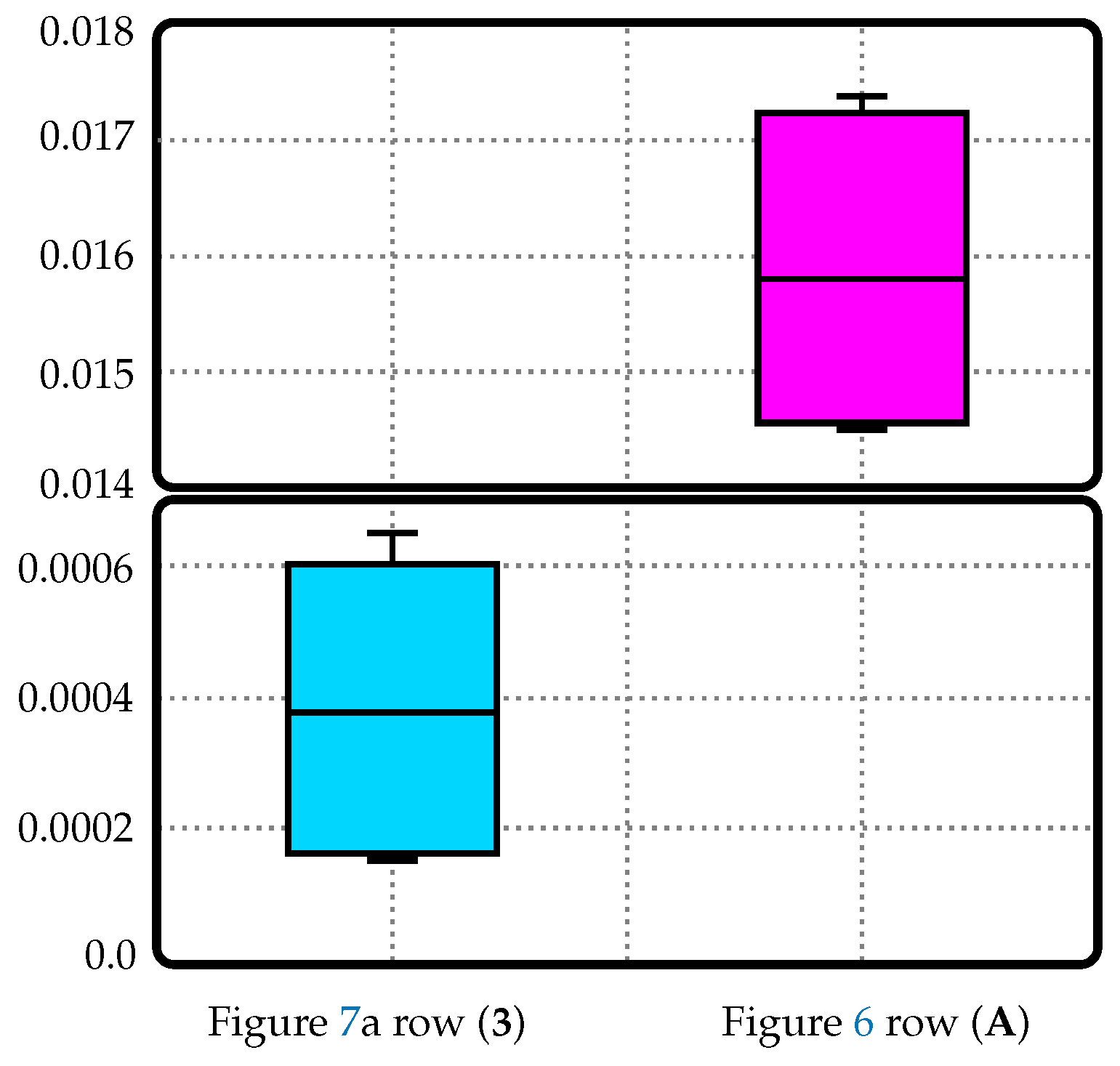
An example of small dissimilarity values being used as a data set identifier is shown in
Figure 8. For instance, when a patient switches from their back to their stomach (known as a rollover), such rollovers have maximal dissimilarity values of 5.9 × 10
−4 in comparison with other rollover types; on the contrary, its dissimilarity value for the less similar movement samples has been identified to be at least 0.0145. There is an almost twenty-five-fold difference between these two metrics and this thereby highlights the reliability placed upon these dissimilarity values as markers or defining characteristics that help identify data sets analogous to and consistent with the reference set being utilized for analysis purposes.
Nevertheless, the information depicted in
Figure 8 only presents a comparison of one rollover movement. In order to ascertain its applicability for various types of rollovers, each distinct movement was assessed against all forms of rollovers, illustrated in
Figure 9. The dissimilarity value reaches a maximum of 0.0025 when comparing all rollovers to each other, while the minimum value is 0.01 for all body movements compared with every measured rollover (now just rollover 3 as in
Figure 8). This represents a stark four-fold contrast in values that can effectively serve as an identifying factor for movement classification based on dissimilarity values alone.
To reiterate,
Figure 8 and
Figure 9 further delve into the comparison of dissimilarity values when distinguishing body movements based on Euler angles. In
Figure 8, the reference bodily motion chosen is rollover 3. The figure displays the dissimilarity values obtained from comparing this reference data set to other similar rollovers, contrasted against dissimilar body movements. For example, when rollover 3 is compared to other rollover types, the maximum dissimilarity value is 5.9 × 10
−4. However, the dissimilarity value significantly increases to at least 0.0145 when it is contrasted with less similar movements or diverse body movements. The difference in these dissimilarity values helps in identifying and grouping similar and dissimilar types of movements.
Figure 9 expands on this approach by comparing the movements in bed and the dissimilarity values obtained from Euler angles associated with different rollovers versus other bodily movements. The dissimilarity value reaches a maximum of 0.0025 when comparing all rollovers to each other. When all body movements are compared with every measured rollover, the minimum value is 0.01. This four-fold contrast in values suggests that these dissimilarity values can effectively serve as an identifying factor for movement classification. Thus,
Figure 8 and
Figure 9 both demonstrate how these relatively significant differences in dissimilarity values can serve as potential markers for detecting specific forms of movement within a bed environment.
4. Discussion
A notification signal system that identifies patient positions and movements in their bed has the capacity to substantially enhance comprehensive patient care within a hospital environment, as outlined below, with various critical factors that could result in enhanced healthcare outcomes if put into practice. Improved Fall Prevention: Falls are a significant concern in healthcare facilities, especially among elderly or physically compromised patients. Not only do falls lead to possible physical injuries, they can also lead to psychological sequelae such as an increased fear of falling which will ultimately delay patient recovery [
10]. Pressure Ulcer Prevention: Prolonged immobility or incorrect positioning can lead to the development of pressure ulcers, which are a major concern for bed-ridden or immobilized patients. Developing a pressure ulcer can cause unnecessary pain, increase the length of stay at the hospital, and can even contribute to the rapid mortality of certain patients [
11]. Early Detection of Respiratory Distress: Changes in patient posture and movements can provide valuable insights into their respiratory status. For example, sudden changes in respiratory patterns or increased restlessness may indicate respiratory distress. Additionally, for patients who suffer from acute respiratory distress syndrome, a change in movement, specifically being placed in the prone position, could help in lowering their respiratory rate and improve oxygenation [
12]. The aforementioned categories share a common theme of an abnormal change in body position. By utilizing a trigger alert system that monitors patient postures and movements in bed, healthcare providers can receive real-time notifications when a patient is in distress, which will ultimately allow for timely interventions. This also serves as an add on to enhance patient monitoring and patient-specific care. Due to the uniqueness of every patient, the additional monitoring of patient postures and movements can provide a more comprehensive understanding of the patient’s condition and the recognition of specific patient trends in movement so that a tailored care plan can be implemented to enhance patient satisfaction, comfort, and overall care quality.
Euler angles, which represent an object’s orientation in three-dimensional space, have a significant importance in this study. They are utilized to assess and monitor patients’ body postures in bed over a specific time frame. The goal is to identify distinct patterns in these angle variations that are indicative of various movements. Euler angles are deemed suitable for analyzing body movements because they offer a straightforward and concise method for representing the orientation of the human body in three-dimensional space. With the help of sensors, changes in Euler angles that occur during common movements performed by patients can be examined. With proper consideration given to the differences between experimental and computational methods [
13], analyzing data using Euler angles can be a dependable approach for algorithms to effectively evaluate body position and movement. This enables accurate monitoring of patient conditions and allows for necessary adjustments to improve their comfort and overall well-being. Moreover, the study involves a comparison of dissimilarity values between various body movements by analyzing Euler angles, which could contribute to the development of a trigger alert system based on these values.
While the use of sensors to measure body posture can provide improved patient safety and response times, there are still several challenges that follow. One area that needs to be addressed is the occurrence of false alarms. False alarms can lead to alert fatigue among healthcare providers, where they become desensitized to the constant influx of alarms and may miss critical alerts. This can potentially jeopardize patient safety. To address this issue, advancements in artificial intelligence (AI) and machine learning could be explored. Currently, AI is implemented in several fields of medicine and assists in better identifying patients who need extra support and personalized protocols [
14,
15,
16]. By leveraging these technologies, it may be possible to develop algorithms that can better differentiate between true alarms and false alarms, reducing the number of unnecessary alerts. This is executed by making the statistical significance value within the algorithm more stringent so that false positives and negatives are minimized [
17]. AI algorithms could also learn from historical data, patient-specific information, and real-time contextual data to improve the accuracy of alert notifications, providing more reliable and actionable information to healthcare providers [
18]. Additionally, the algorithm must also recognize the patterns related to minor movements or temporary changes so that a false alarm is not triggered. Therefore, a potential future project would be to incorporate AI to continuously receive input data from the sensors and recognize what body postures and movements serve as a baseline and which movement patterns outside of the regular movements call for triggering an alarm. Other studies have also utilized Procrustes analyses in conjunction with machine learning models [
19]. Furthermore, evaluating diverse machine learning models on a consistent data set facilitates the identification of the most appropriate model for a particular application through the rigorous assessment of their respective performance, ultimately guiding model selection based on empirical evidence [
20]. By creating this iterative routine of data acquisition and statistical significance analysis, we should be able to determine if there is a noticeable change in the patient’s movement. If the algorithm can accurately recognize these patterns, its implementation through AI can serve as a promising tool to increase the safety of patients in the healthcare sector.
Overall, a trigger alert system based on patient posture and movements in bed has the potential to significantly benefit patient care in hospitals. By facilitating fall prevention, pressure ulcer prevention, early detection of respiratory distress, enhanced monitoring, and personalized care, this system can contribute to improved patient outcomes and safety. However, careful consideration of challenges, such as false alarms, is necessary during implementation. With that said, incorporating such a system into healthcare settings can enhance patient care, promote proactive interventions, and optimize resource allocation.
It is important to acknowledge that the current study is in its early stages and does not yet have sufficient significance for immediate practical application. This preliminary work involves a conceptual design, where basic principles were identified based on initial trunk posture data collected using mannequins as a temporary substitute. The next phase will involve testing with non-patient individuals followed by actual patients. These subsequent experiments will provide the necessary data to develop the desired classification algorithms. One of the main challenges in this area of research is that individuals, especially those with neurological impairments, may exhibit unique sequences of movements when adjusting their posture in bed or attempting to get out of bed. As a result, measuring the sequence of Euler angles for trunk movements (which can be performed relatively easily with modern sensors) is not as significant as developing a dependable classification algorithm that can work effectively across different patients.
Nevertheless, in healthcare, it is not uncommon for certain practices and procedures to become deeply ingrained in our routines, even when newer technologies and advancements are available. This can be attributed to a combination of factors, including familiarity, resistance to change, and a reliance on established protocols. Over time, healthcare professionals may become accustomed to the way things have always been done, leading to a reluctance to explore alternative approaches or embrace emerging technologies. This inertia can hinder progress and prevent the exploration of more efficient and effective solutions. It is essential for the healthcare community to foster a culture of continuous improvement, encouraging individuals to question established norms and seek out innovative ways to enhance patient care through the utilization of newer technologies and practices.
5. Conclusions
In the healthcare industry, medical professionals are often busy and have limited time to monitor patients. Currently, devices for monitoring physiological signs serve as a helpful tool in measuring vital indicators and alerting staff to significant changes. Call systems are also provided next to patients so they can request assistance when needed. However, some patients may be unable to use these systems due to their distress. Furthermore, patient posture and movement patterns are frequently overlooked despite their potential role in identifying possible complications. Using a sensor device to monitor patient movements shows promise as an effective solution. Our research indicates that data on different body postures and movements can be collected and distinguished from one another, making it possible to develop a trigger alert system based on such values. By collecting information on posture and movement patterns, medical staff can be notified of urgent situations caused by abnormal changes in movement. Implementing such a notification system would improve response times and ultimately enhance patient outcomes.
Using simple, affordable sensors to monitor bed-bound patients and their movements in hospitals can offer several advantages and disadvantages. Such sensors can be a valuable addition to patient care in hospitals, offering continuous monitoring and improved safety. However, their effectiveness depends on the careful selection, implementation, and integration of the sensors, along with ongoing training for healthcare providers to use the data effectively while addressing the potential disadvantages and privacy concerns.
One of the main challenges is that individuals, especially those with neurological impairments, may exhibit unique sequences of movements when adjusting their posture in bed. Hence, developing a reliable classification algorithm that can work effectively across different patients poses a challenge. Notably, false alarms could become a significant issue with such systems. The algorithm must recognize minor or temporary movements to ensure false alarms are not triggered. Another challenge pertains to the operational implementation of such systems.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








