
Mild to Moderate Sleep Restriction Does Not Affect the Cortisol Awakening Response in Healthy Adult Males


Abstract
:1. Introduction
2. Results
2.1. Sleep
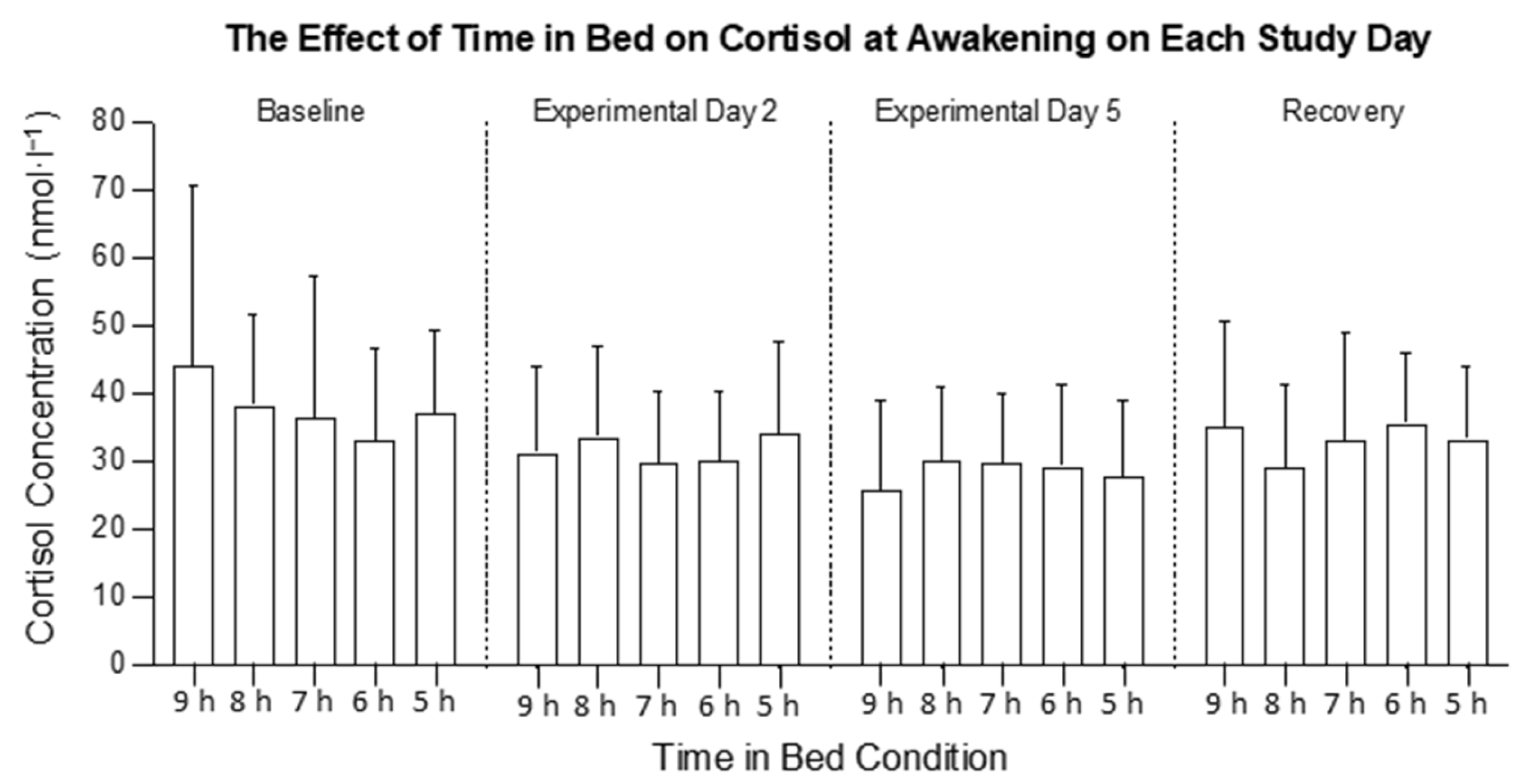
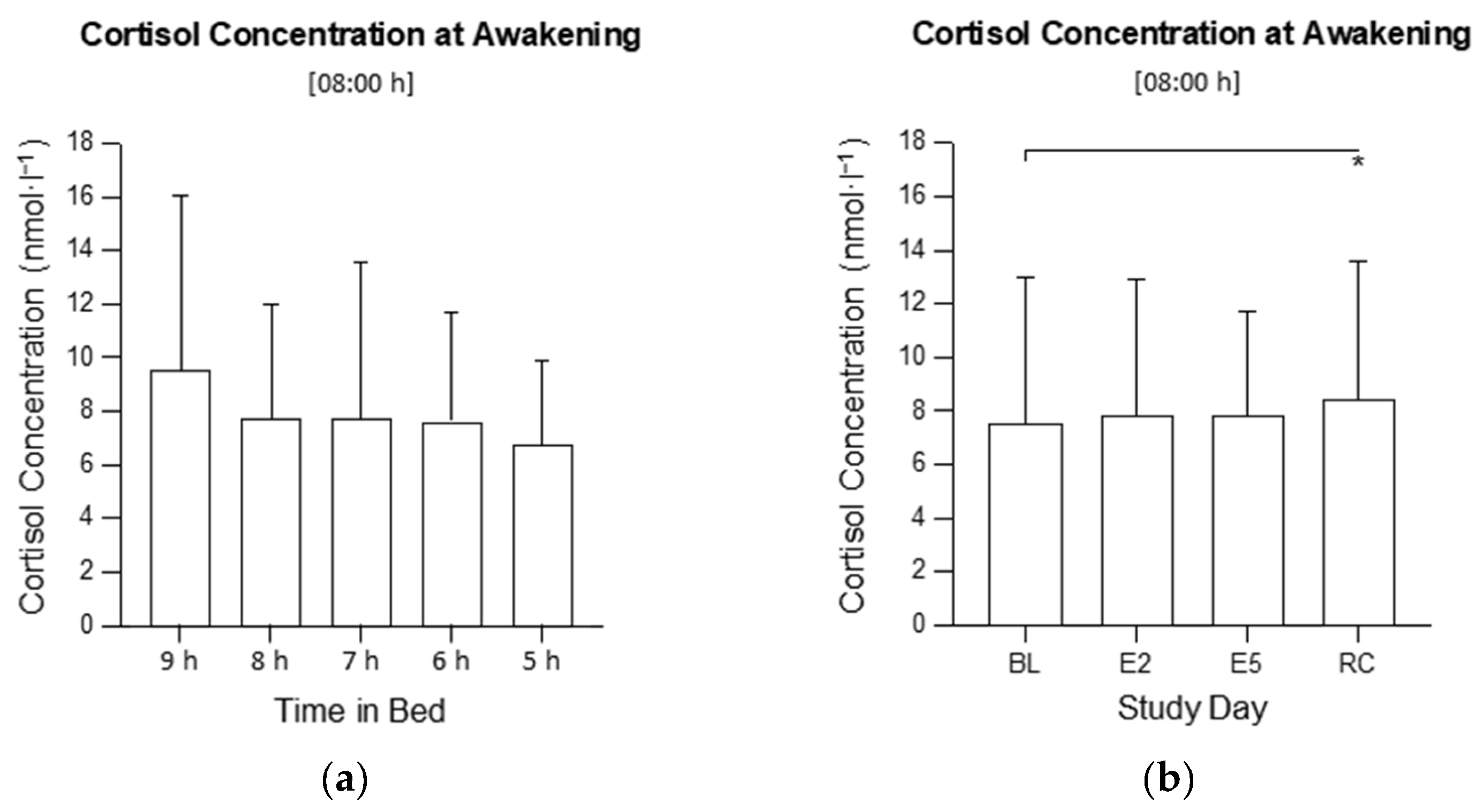
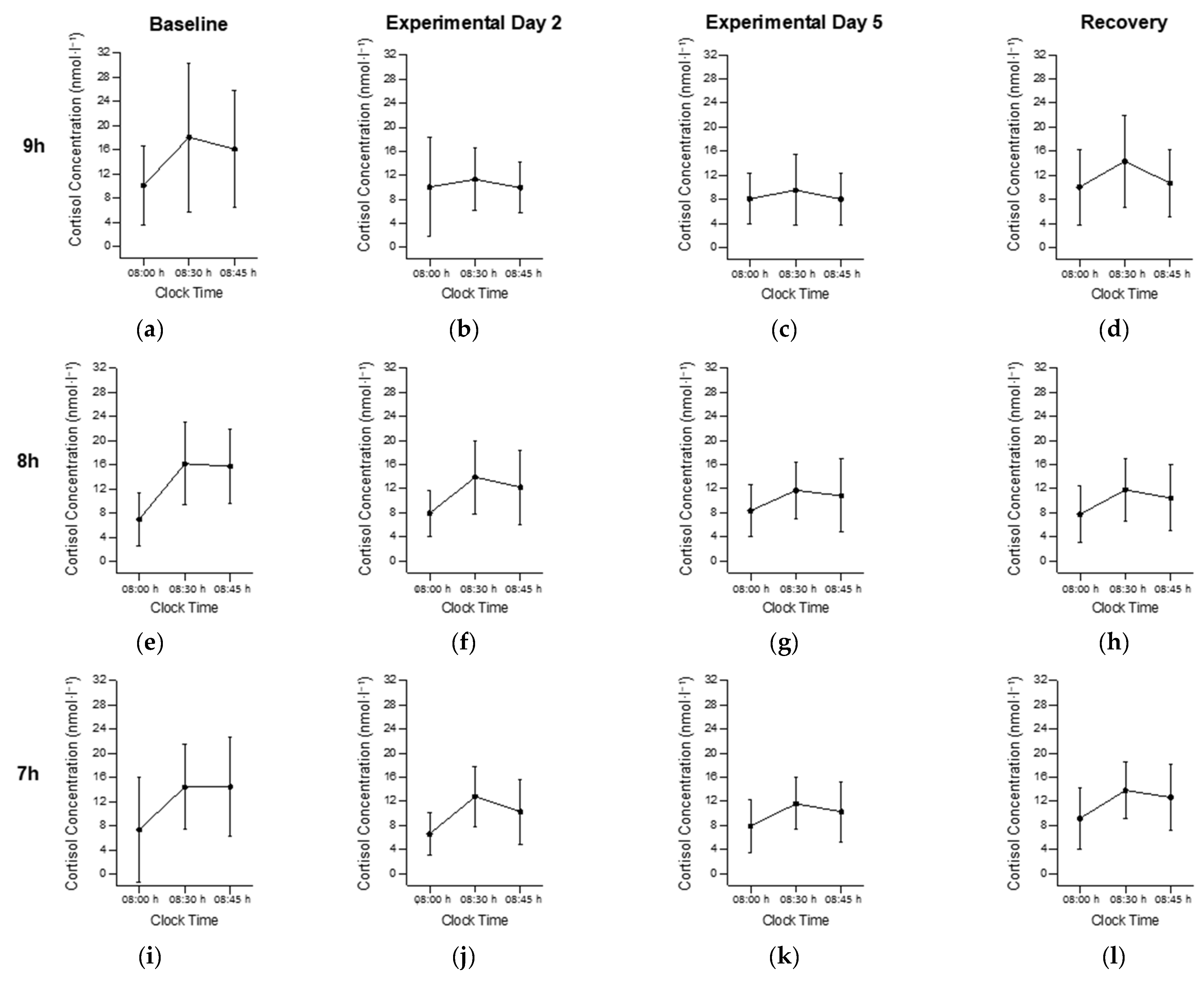
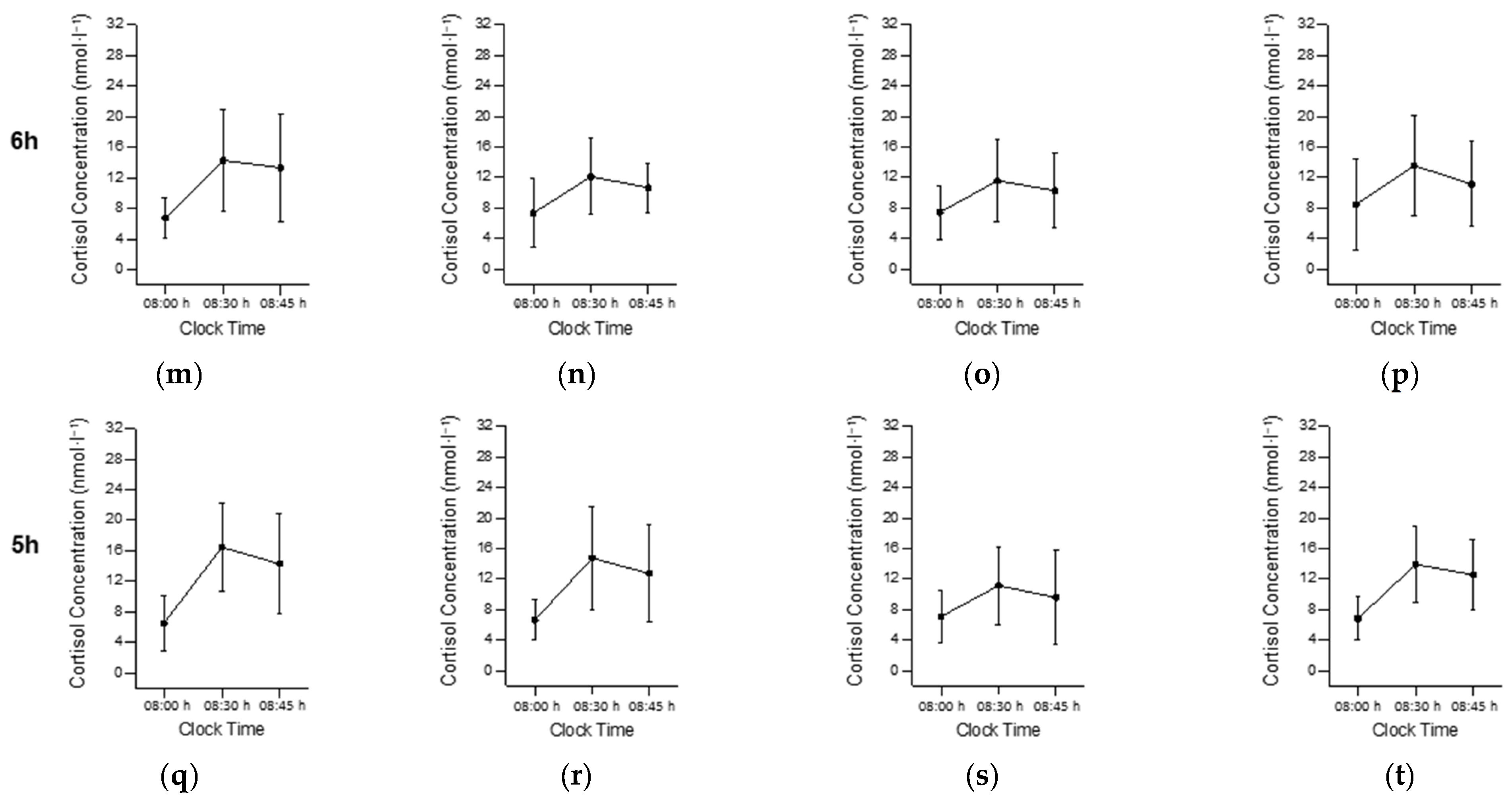
2.2. Cortisol at Awakening (08:00 h)
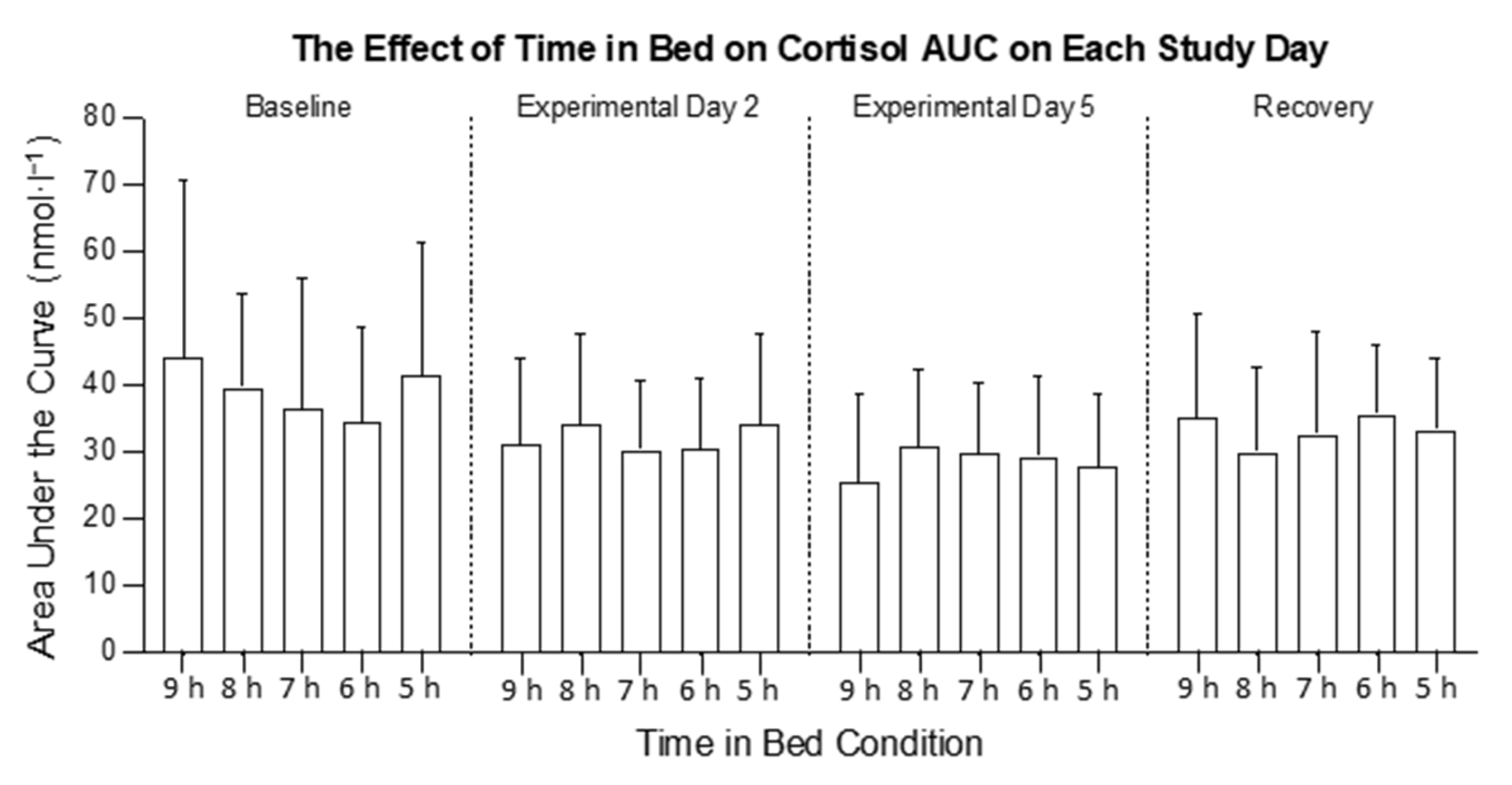
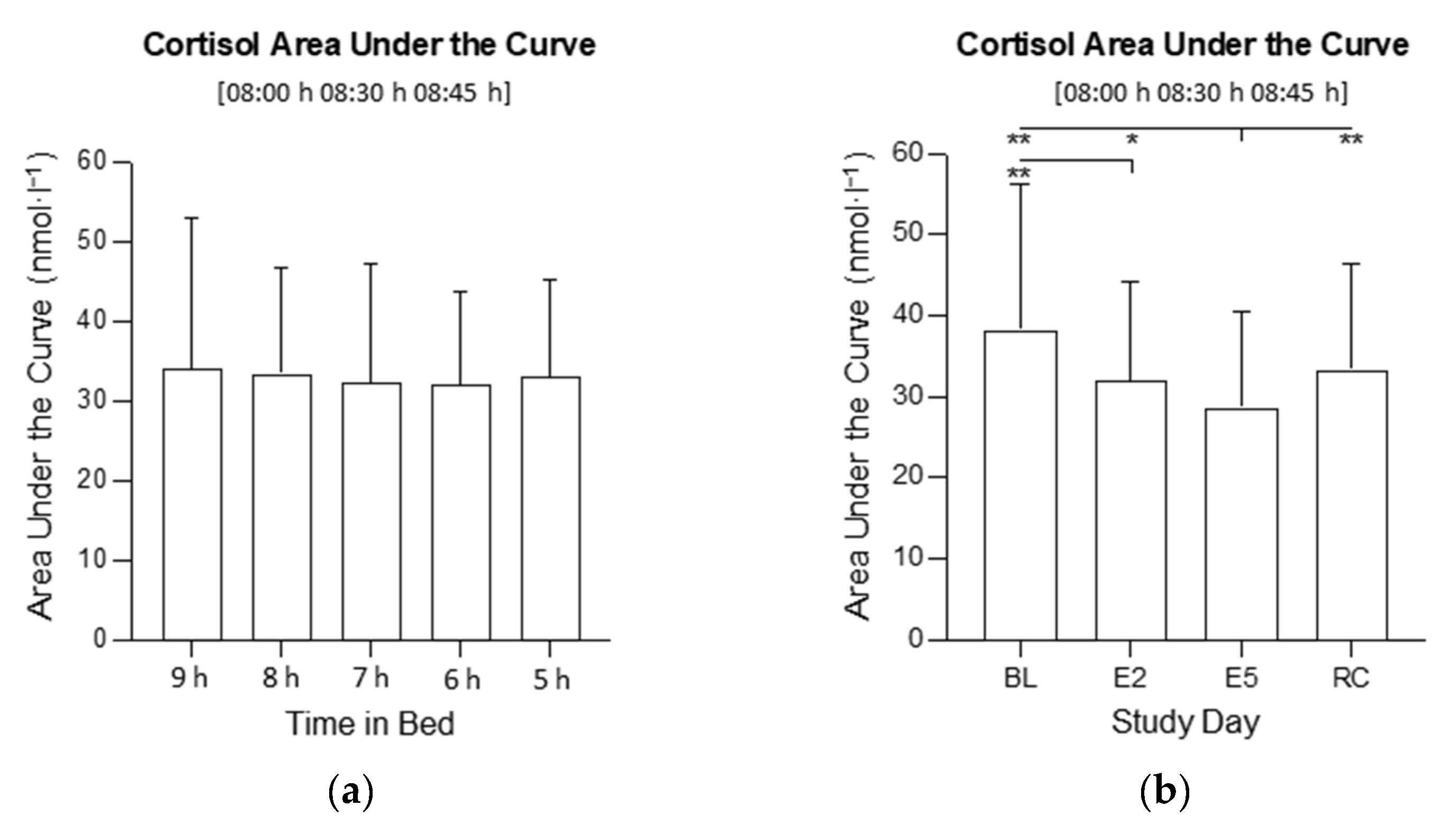
2.3. Cortisol Area under the Curve (AUC)
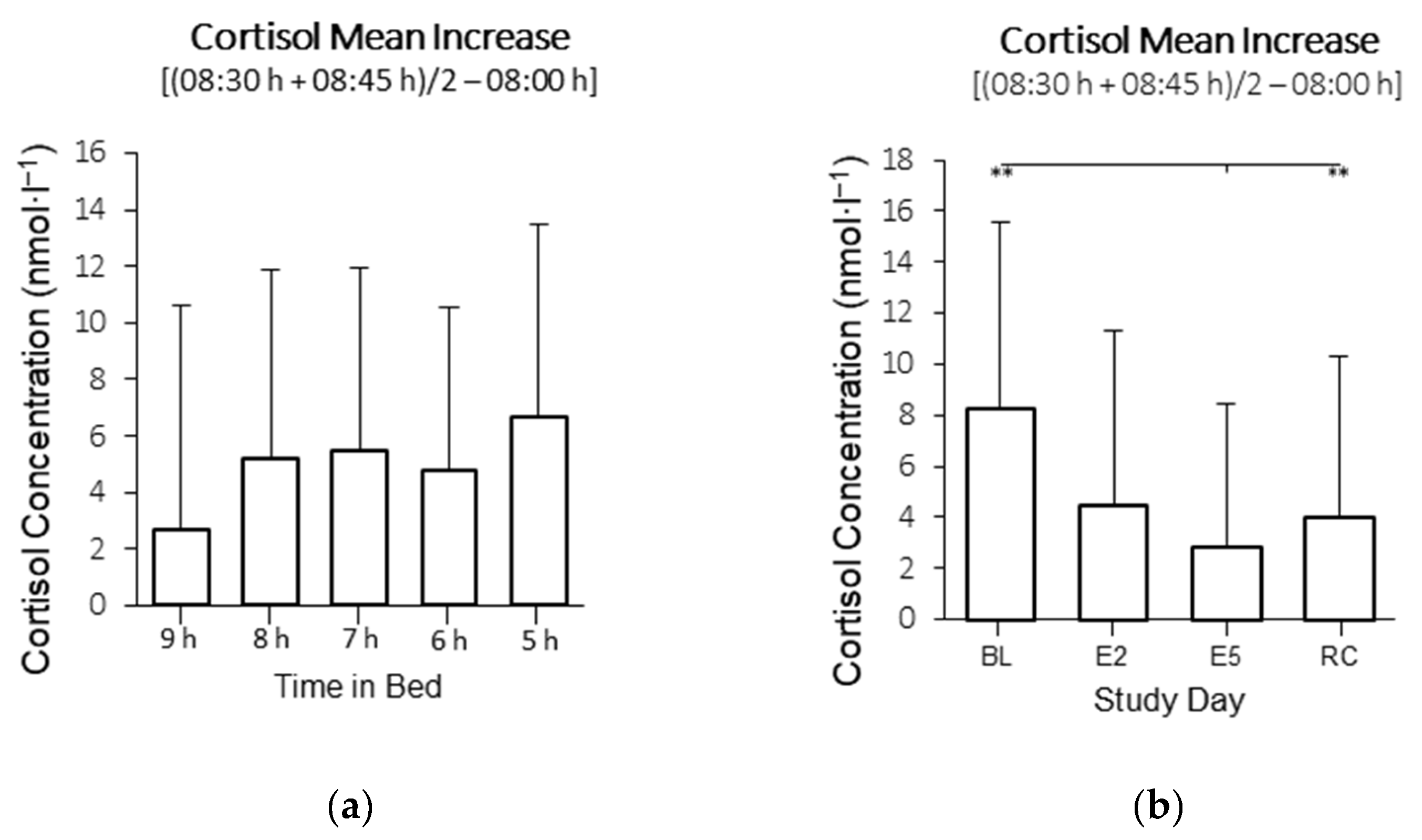
2.4. Cortisol Mean Increase (MnInc)
3. Discussion
4. Materials and Methods
4.1. Participants
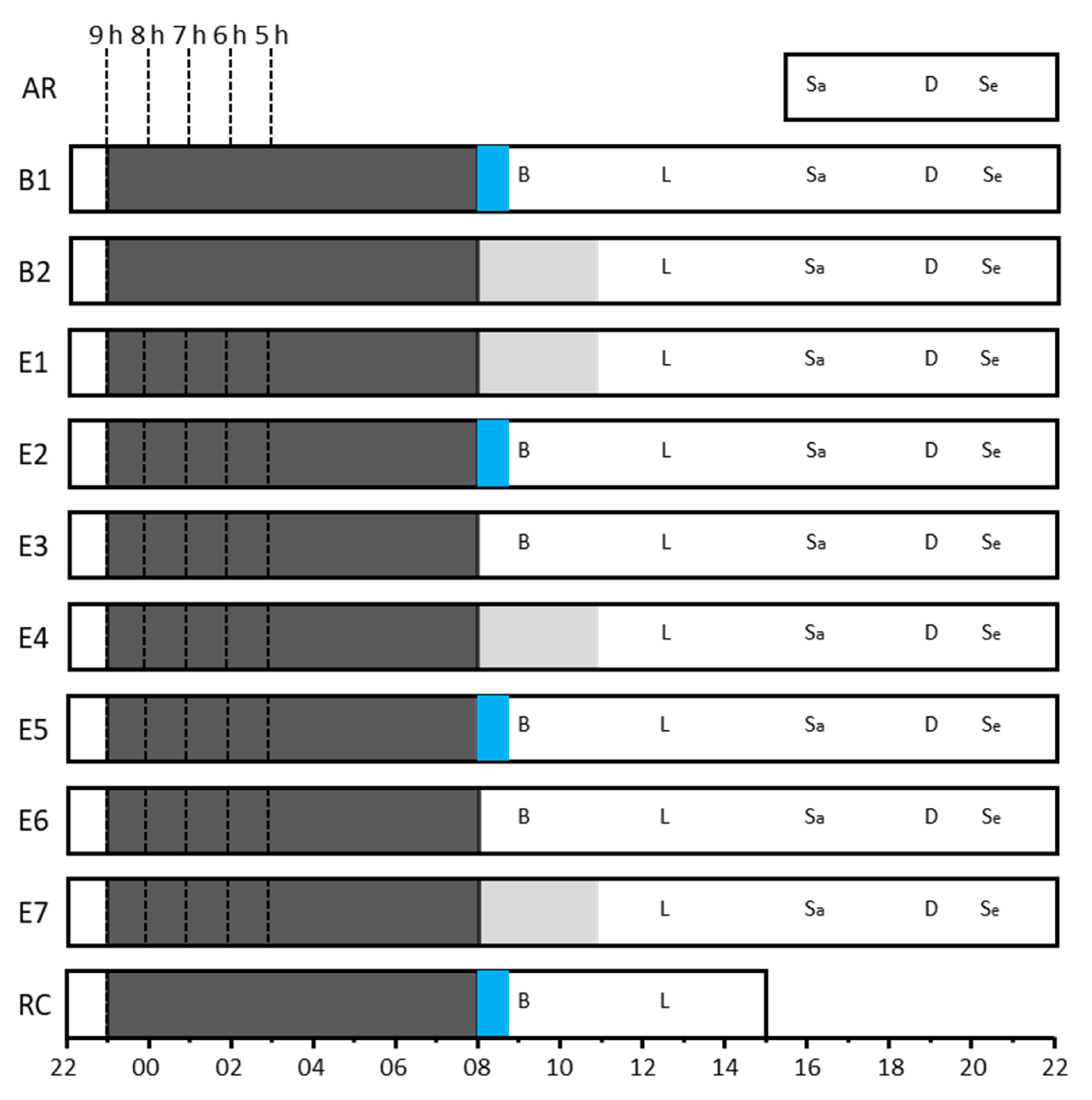
4.2. Experimental Design
4.3. Laboratory Setting
4.4. Protocol
4.5. Measures
4.6. Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smyth, N.; Thorn, L.; Hucklebridge, F.; Evans, P.; Clow, A. Detailed time course of the cortisol awakening response in healthy participants. Psychoneuroendocrinology 2015, 62, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Pruessner, J.; Wolf, O.; Hellhammer, D.; Buske-Kirschbaum, A.; von Auer, K.; Jobst, S.; Kaspers, F.; Kirschbaum, C. Free cortisol levels after awakening: A reliable biological marker for the assessment of adrenocortical activity. Life Sci. 1997, 61, 2539–2549. [Google Scholar] [CrossRef] [PubMed]
- Clow, A.; Thorn, L.; Evans, P.; Hucklebridge, F. The awakening cortisol response: Methodological issues and significance. Stress 2004, 7, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, I.; Born, J.; Kudielka, B.M.; Schlotz, W.; Wust, S. Is the cortisol awakening rise a response to awakening? Psychoneuroendocrinology 2007, 32, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Wust, S.; Federenko, I.; Hellhammer, D.H.; Kirschbaum, C. Genetic factors, perceived chronic stress, and the free cortisol response to awakening. Psychoneuroendocrinology 2000, 25, 707–720. [Google Scholar] [CrossRef]
- Elder, G.J.; Barclay, N.L.; Wetherell, M.A.; Ellis, J.G. Anticipated next-day demand affects the magnitude of the cortisol awakening response, but not subjective or objective sleep. J. Sleep Res. 2018, 27, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Violanti, J.M.; Fekedulegn, D.; Andrew, M.E.; Hartley, T.A.; Charles, L.E.; Miller, D.B.; Burchfiel, C.M. The impact of perceived intensity and frequency of police work occupational stressors on the cortisol awakening response (CAR): Findings from the BCOPS study. Psychoneuroendocrinology 2017, 75, 124–131. [Google Scholar] [CrossRef] [Green Version]
- Duan, H.; Yuan, Y.; Zhang, L.; Qin, S.; Zhang, K.; Buchanan, T.W.; Wu, J. Chronic stress exposure decreases the cortisol awakening response in healthy young men. Stress 2013, 16, 630–637. [Google Scholar] [CrossRef]
- Wessa, M.; Rohleder, N.; Kirschbaum, C.; Flor, H. Altered cortisol awakening response in posttraumatic stress disorder. Psychoneuroendocrinology 2006, 31, 209–215. [Google Scholar] [CrossRef]
- Bruehl, H.; Wolf, O.T.; Convit, A. A blunted cortisol awakening response and hippocampal atrophy in type 2 diabetes mellitus. Psychoneuroendocrinology 2009, 34, 815–821. [Google Scholar] [CrossRef]
- Champaneri, S.; Xu, X.; Carnethon, M.R.; Bertoni, A.G.; Seeman, T.; Roux, A.D.; Golden, S.H. Diurnal salivary cortisol and urinary catecholamines are associated with diabetes mellitus: The Multi-Ethnic Study of Atherosclerosis. Metab. Clin. Exp. 2012, 61, 986–995. [Google Scholar] [CrossRef] [Green Version]
- Klumpers, U.M.; Veltman, D.J.; van Tol, M.J.; Kloet, R.W.; Boellaard, R.; Lammertsma, A.A.; Hoogendijk, W.J. Neurophysiological effects of sleep deprivation in healthy adults, a pilot study. PLoS ONE 2015, 10, e0116906. [Google Scholar] [CrossRef] [Green Version]
- Vargas, I.; Lopez-Duran, N. The cortisol awakening response after sleep deprivation: Is the cortisol awakening response a “response” to awakening or a circadian process? J. Health Psychol. 2017, 25, 900–912. [Google Scholar] [CrossRef]
- Kumari, M.; Badrick, E.; Ferrie, J.; Perski, A.; Marmot, M.; Chandola, T. Self-reported sleep duration and sleep disturbance are independently associated with cortisol secretion in the Whitehall II study. J. Clin. Endocrinol. Metab. 2009, 94, 4801–4809. [Google Scholar] [CrossRef] [Green Version]
- Vargas, I.; Lopez-Duran, N. Dissecting the impact of sleep and stress on the cortisol awakening response in young adults. Psychoneuroendocrinology 2013, 40, 10–16. [Google Scholar] [CrossRef]
- Law, R.; Hucklebridge, F.; Thorn, L.; Evans, P.; Clow, A. State variation in the cortisol awakening response. Stress 2013, 16, 483–492. [Google Scholar] [CrossRef]
- Kudielka, B.M.; Broderick, J.E.; Kirschbaum, C. Compliance with saliva sampling protocols: Electronic monitoring reveals invalid cortisol daytime profiles in noncompliant subjects. Psychosom. Med. 2003, 65, 313–319. [Google Scholar] [CrossRef]
- Smyth, N.; Clow, A.; Thorn, L.; Hucklebridge, F.; Evans, P. Delays of 5-15 min between awakening and the start of saliva sampling matter in assessment of the cortisol awakening response. Psychoneuroendocrinology 2013, 38, 1476–1483. [Google Scholar] [CrossRef]
- Charles, L.E.; Slaven, J.E.; Mnatsakanova, A.; Ma, C.; Violanti, J.M.; Fekedulegn, D.; Andrew, M.E.; Vila, B.J.; Burchfiel, C.M. Association of perceived stress with sleep duration and sleep quality in police officers. Int. J. Emerg. Ment. Health 2011, 13, 229–241. [Google Scholar]
- Dahlgren, A.; Kecklund, G.; Åkerstedt, T. Different levels of work-related stress and the effects on sleep, fatigue and cortisol. Scand. J. Work. Environ. Health 2005, 31, 277–285. [Google Scholar] [CrossRef] [Green Version]
- Omisade, A.; Buxton, O.M.; Rusak, B. Impact of acute sleep restriction on cortisol and leptin levels in young women. Physiol. Behav. 2010, 99, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Zoumakis, E.; Bixler, E.O.; Lin, H.M.; Follett, H.; Kales, A.; Chrousos, G.P. Adverse effects of modest sleep restriction on sleepiness, performance, and inflammatory cytokines. J. Clin. Endocrinol. Metab. 2004, 89, 2119–2126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegel, K.; Leproult, R.; L’Hermite-Baleriaux, M.; Copinschi, G.; Penev, P.D.; Van Cauter, E. Leptin levels are dependent on sleep duration: Relationships with sympathovagal balance, carbohydrate regulation, cortisol, and thyrotropin. J. Clin. Endocrinol. Metab. 2004, 89, 5762–5771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyon, A.; Balbo, M.; Morselli, L.L.; Tasali, E.; Leproult, R.; L’Hermite-Balériaux, M.; Van Cauter, E.; Spiegel, K. Adverse effects of two nights of sleep restriction on the hypothalamic-pituitary-adrenal axis in healthy men. J. Clin. Endocrinol. Metab. 2014, 99, 2861–2868. [Google Scholar] [CrossRef] [PubMed]
- Leproult, R.; Copinschi, G.; Buxton, O.; Van Cauter, E. Sleep loss results in an elevation of cortisol levels the next evening. Sleep 1997, 20, 865–870. [Google Scholar]
- Buxton, O.M.; Pavlova, M.; Reid, E.W.; Wang, W.; Simonson, D.C.; Adler, G.K. Sleep restriction for 1 week reduces insulin sensitivity in healthy men. Diabetes 2010, 59, 2126–2133. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, R.M.; Labad, J.; Strachan, M.W.J.; Braun, A.; Fowkes, F.G.R.; Lee, A.J.; Frier, B.M.; Seckl, J.R.; Walker, B.R.; Price, J.F.; et al. Elevated fasting plasma cortisol is associated with ischemic heart disease and its risk factors in people with type 2 diabetes: The Edinburgh type 2 diabetes study. J. Clin. Endocrinol. Metab. 2010, 95, 1602–1608. [Google Scholar] [CrossRef] [Green Version]
- Schmid, S.M.; Hallschmid, M.; Jauch-Chara, K.; Wilms, B.; Lehnert, H.; Born, J.; Schultes, B. Disturbed glucoregulatory response to food intake after moderate sleep restriction. Sleep 2011, 34, 371–377. [Google Scholar] [CrossRef] [Green Version]
- van Leeuwen, W.M.A.; Sallinen, M.; Virkkala, J.; Lindholm, H.; Hirvonen, A.; Hublin, C.; Porkka-Heiskanen, T.; Härmä, M. Physiological and autonomic stress responses after prolonged sleep restriction and subsequent recovery sleep in healthy young men. Sleep Biol. Rhythm. 2018, 16, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Voderholzer, U.; Piosczyk, H.; Holz, J.; Feige, B.; Loessl, B.; Kopasz, M.; Riemann, D.; Nissen, C. The impact of increasing sleep restriction on cortisol and daytime sleepiness in adolescents. Neurosci. Lett. 2012, 507, 161–166. [Google Scholar] [CrossRef]
- van Leeuwen, W.M.; Hublin, C.; Sallinen, M.; Harma, M.; Hirvonen, A.; Porkka-Heiskanen, T. Prolonged sleep restriction affects glucose metabolism in healthy young men. Int. J. Endocrinol. 2010, 2010, 108641. [Google Scholar] [CrossRef]
- Stalder, T.; Kirschbaum, C.; Kudielka, B.M.; Adam, E.K.; Pruessner, J.C.; Wüst, S.; Miller, R.; Wetherell, M.A.; Lupien, S.J.; Clow, A.; et al. Assessment of the cortisol awakening response: Expert consensus guidelines. Psychoneuroendocrinology 2016, 63, 414–432. [Google Scholar] [CrossRef]
- Abercrombie, H.C.; Giese-Davis, J.; Sephton, S.; Epel, E.S.; Turner-Cobb, J.M.; Spiegel, D. Flattened cortisol rhythms in metastatic breast cancer patients. Psychoneuroendocrinology 2004, 29, 1082–1092. [Google Scholar] [CrossRef]
- Abell, J.G.; Shipley, M.J.; Ferrie, J.E.; Kivimaki, M.; Kumari, M. Recurrent short sleep, chronic insomnia symptoms and salivary cortisol: A 10-year follow-up in the Whitehall II study. Psychoneuroendocrinology 2016, 68, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Scarinci, F.; Patacchioli, F.R.; Ghiciuc, C.M.; Pasquali, V.; Bercea, R.M.; Cozma, S.; Parravano, M. Psychological Profile and Distinct Salivary Cortisol Awake Response (CAR) in Two Different Study Populations with Obstructive Sleep Apnea (OSA) and Central Serous Chorioretinopathy (CSC). J. Clin. Med. 2020, 9, 2490. [Google Scholar] [CrossRef]
- Silva, G.E.; Goodwin, J.L.; Sherrill, D.L.; Arnold, J.L.; Bootzin, R.R.; Smith, T.; Walsleben, J.A.; Baldwin, C.M.; Quan, S.F. Relationship between reported and measured sleep times: The sleep heart health study (SHHS). J. Clin. Sleep Med. 2007, 3, 622–630. [Google Scholar] [CrossRef] [Green Version]
- Bäumler, D.; Kliegel, M.; Kirschbaum, C.; Miller, R.; Alexander, N.; Stalder, T. Effect of a naturalistic prospective memory-related task on the cortisol awakening response in young children. Biol. Psychol. 2014, 103, 24–26. [Google Scholar] [CrossRef]
- Elder, G.J.; Ellis, J.G.; Barclay, N.L.; Wetherell, M.A. Assessing the daily stability of the cortisol awakening response in a controlled environment. BMC Psychol. 2016, 4, 3. [Google Scholar] [CrossRef] [Green Version]
- Tamaki, M.; Nittono, H.; Hayashi, M.; Hori, T. Examination of the First-Night Effect during the Sleep-Onset Period. Sleep 2005, 28, 195–202. [Google Scholar] [CrossRef] [Green Version]
- Sprajcer, M.; Gupta, C.; Roach, G.; Sargent, C. Can we put the first night effect to bed? An analysis based on a large sample of healthy adults. Chronobiol. Int. 2022, 1–7. [Google Scholar] [CrossRef]
- Goerke, M.; Cohrs, S.; Rodenbeck, A.; Grittner, U.; Sommer, W.; Kunz, D. Declarative memory consolidation during the first night in a sleep lab: The role of REM sleep and cortisol. Psychoneuroendocrinology 2013, 38, 1102–1111. [Google Scholar] [CrossRef] [PubMed]
- Kontou, T.G.; Sargent, C.; Roach, G.D. Glucose Concentrations from Continuous Glucose Monitoring Devices Compared to those from Blood Plasma During an Oral Glucose Tolerance Test in Healthy Participants. Int. J. Environ. Res. Public Health 2021, 11, 12994. [Google Scholar] [CrossRef] [PubMed]
- Kontou, T.G.; Sargent, C.; Roach, G.D. A Week of Sleep Restriction Does Not Affect Nighttime Glucose Concentration in Healthy Adult Males When Slow-Wave Sleep Is Maintained. Sensors 2022, 22, 6962. [Google Scholar] [CrossRef] [PubMed]
- Boivin, D.B.; Duffy, J.F.; Kronauer, R.E.; Czeisler, C.A. Dose-response relationships for resetting of human circadian clock by light. Nature 1996, 379, 540–542. [Google Scholar] [CrossRef]
- Iber, C. The AASM Manual for the Scoring of Sleep and Associated Events: Rules. Terminology and Technical Specification. Darian (IL/USA): American Academy of Sleep Medicine. 2007. Available online: https://aasm.org/clinical-resources/scoring-manual/ (accessed on 15 November 2022).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | BL | E2 | E5 | RC |
|---|---|---|---|---|
| 9 h | 472.7 ± 53.5 | 481.0 ± 37.2 | 458.2 ± 48.8 | 462.5 ± 31.5 |
| 8 h | 483.6 ± 39.8 | 449.7 ± 9.9 | 444.0 ± 23.2 | 469.4 ± 39.5 |
| 7 h | 473.5 ± 45.1 | 400.8 ± 21.0 | 401.6 ± 20.5 | 479.7 ± 44.6 |
| 6 h | 462.8 ± 46.3 | 342.8 ± 13.3 | 345.1 ± 10.0 | 484.6 ± 59.6 |
| 5 h | 487.4 ± 42.7 | 288.7 ± 4.4 | 291.0 ± 6.1 | 512.1 ± 20.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kontou, T.G.; Roach, G.D.; Sargent, C. Mild to Moderate Sleep Restriction Does Not Affect the Cortisol Awakening Response in Healthy Adult Males. Clocks & Sleep 2022, 4, 722-734. https://doi.org/10.3390/clockssleep4040054
Kontou TG, Roach GD, Sargent C. Mild to Moderate Sleep Restriction Does Not Affect the Cortisol Awakening Response in Healthy Adult Males. Clocks & Sleep. 2022; 4(4):722-734. https://doi.org/10.3390/clockssleep4040054
Chicago/Turabian StyleKontou, Thomas G., Gregory D. Roach, and Charli Sargent. 2022. "Mild to Moderate Sleep Restriction Does Not Affect the Cortisol Awakening Response in Healthy Adult Males" Clocks & Sleep 4, no. 4: 722-734. https://doi.org/10.3390/clockssleep4040054