The Association between Sleep Duration and Quality with Readmissions: An Exploratory Pilot-Study among Cardiology Inpatients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
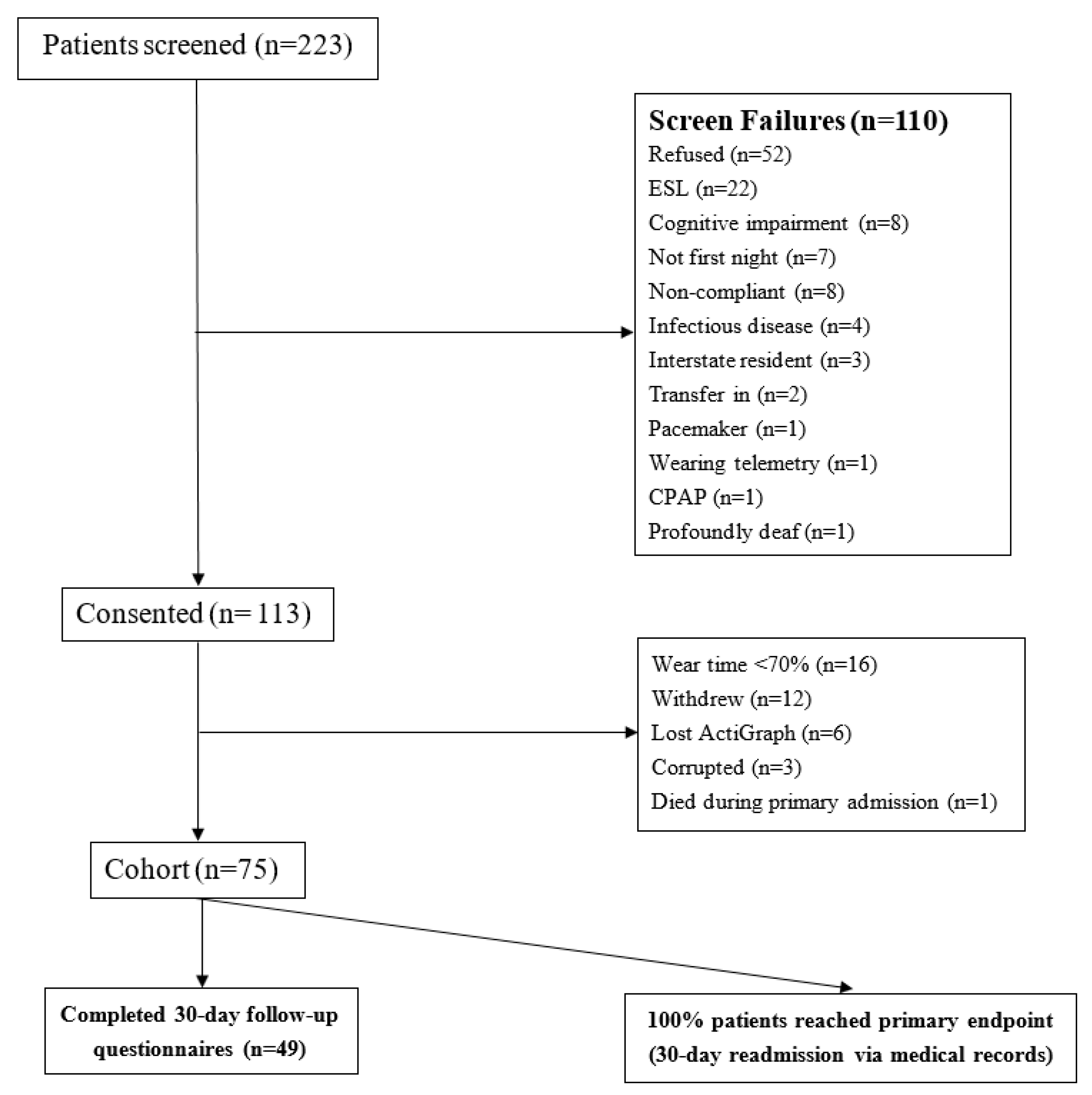
2.1. Patient Demographics
2.2. Readmission Timing and Causes
2.3. Objective Sleep Measures
2.4. Self-Reported Measures
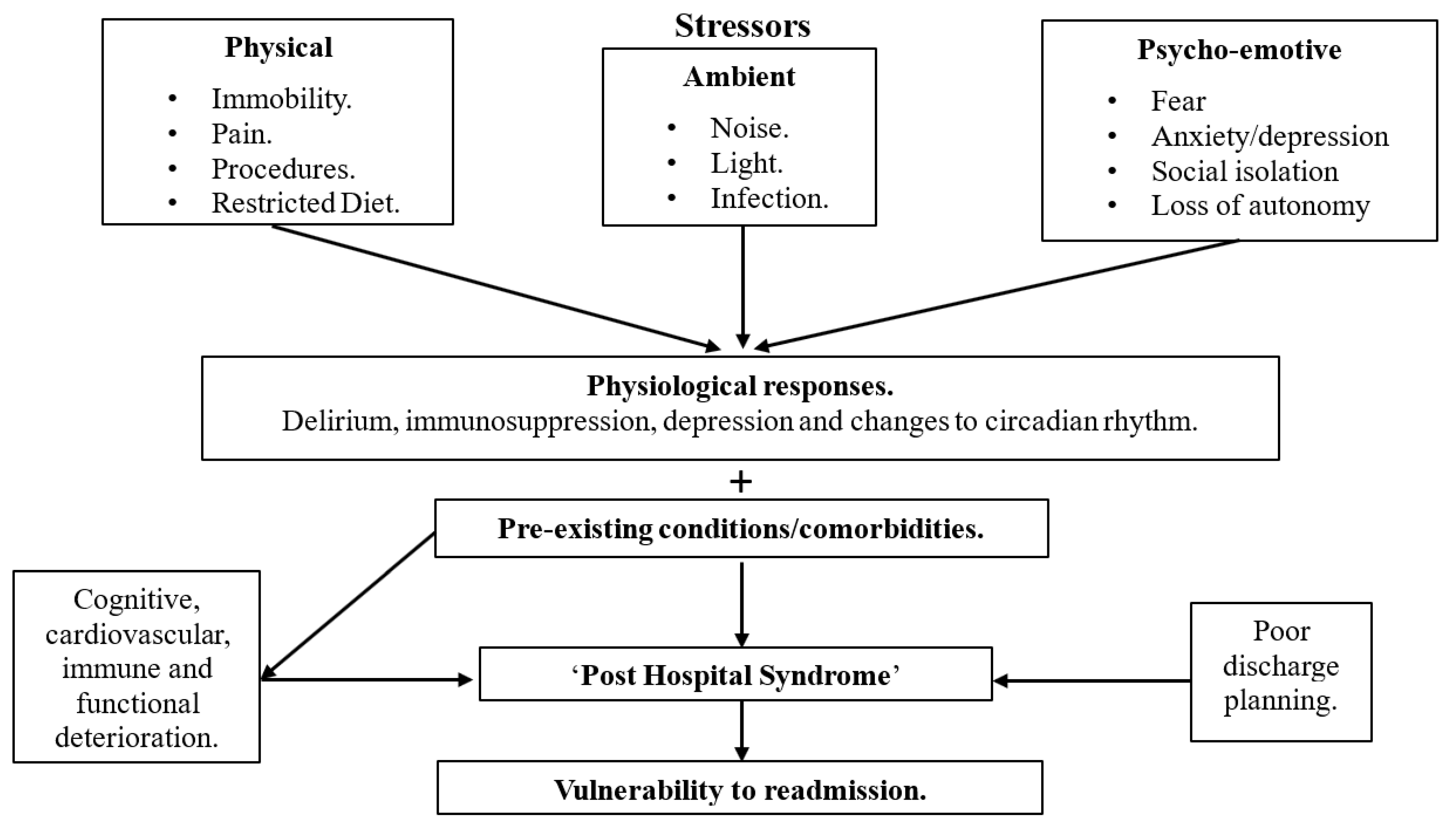
3. Discussion
3.1. Sleep in the Inpatient Environment
3.2. Sleep and Readmissions
3.3. Limitations
4. Methods and Materials
4.1. Study Patients
4.2. Study Protocol
4.3. 30-Day All-Cause Unplanned Readmission
4.4. Follow-Up
4.5. Sleep Parameters
4.5.1. Actigraphy
4.5.2. Pittsburgh Sleep Quality Index (PSQI)
4.5.3. Epworth Sleepiness Scale (ESS)
4.5.4. STOP BANG
4.5.5. EuroQoL-5 Dimensions- 3 Levels (EQ-5D-3L)
4.6. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Validity of ActiGraph Wear Time

{kind=link}
{kind=link}
| Average Time Worn (%) | Number of Patients | % of Patients |
|---|---|---|
| 0 | 1 | 1.09 |
| 4.4 | 1 | 1.09 |
| 41.1 | 1 | 1.09 |
| 42.8 | 1 | 1.09 |
| 44 | 1 | 1.09 |
| 44.7 | 1 | 1.09 |
| 44.9 | 1 | 1.09 |
| 46.3 | 1 | 1.09 |
| 51.8 | 1 | 1.09 |
| 59.5 | 1 | 1.09 |
| 67 | 3 | 3.26 |
| 67.8 | 1 | 1.09 |
| 70.3 | 1 | 1.09 |
| 74 | 2 | 2.17 |
| 74.3 | 1 | 1.09 |
| 74.4 | 1 | 1.09 |
| 75 | 1 | 1.09 |
| 75.5 | 1 | 1.09 |
| 77 | 1 | 1.09 |
| 77.4 | 1 | 1.09 |
| 78.4 | 1 | 1.09 |
| 78.8 | 1 | 1.09 |
| 79.3 | 1 | 1.09 |
| 80 | 2 | 2.17 |
| 80.4 | 1 | 1.09 |
| 81.6 | 1 | 1.09 |
| 82 | 2 | 2.17 |
| 83.5 | 1 | 1.09 |
| 84.3 | 1 | 1.09 |
| 84.3 | 1 | 1.09 |
| 84.5 | 1 | 1.09 |
| 84.7 | 1 | 1.09 |
| 85.4 | 1 | 1.09 |
| 85.5 | 1 | 1.09 |
| 86 | 1 | 1.09 |
| 86.5 | 1 | 1.09 |
| 86.6 | 1 | 1.09 |
| 87 | 1 | 1.09 |
| 87.4 | 1 | 1.09 |
| 88.3 | 1 | 1.09 |
| 88.7 | 1 | 1.09 |
| 88.8 | 1 | 1.09 |
| 89 | 1 | 1.09 |
| 89.5 | 1 | 1.09 |
| 90 | 1 | 1.09 |
| 91.3 | 1 | 1.09 |
| 91.4 | 1 | 1.09 |
| 91.6 | 1 | 1.09 |
| 91.9 | 1 | 1.09 |
| 92 | 4 | 4.35 |
| 93.2 | 1 | 1.09 |
| 94.6 | 1 | 1.09 |
| 94.8 | 1 | 1.09 |
| 96.3 | 1 | 1.09 |
| 96.5 | 1 | 1.09 |
| 96.8 | 1 | 1.09 |
| 97.4 | 1 | 1.09 |
| 97.7 | 1 | 1.09 |
| 97.9 | 1 | 1.09 |
| 98 | 1 | 1.09 |
| 98.6 | 1 | 1.09 |
| 98.8 | 1 | 1.09 |
| 98.95 | 1 | 1.09 |
| NA | 3 | 3.26 |
| 100 | 18 | 19.6 |
| Total | 92 |
| (a) | |||
| Average Time Worn (%) | Number of Patients | % of Patients | |
| 80 | 2 | 2.2 | |
| 80.4 | 1 | 1.1 | |
| 81.6 | 1 | 1.1 | |
| 82 | 2 | 2.2 | |
| 83.5 | 1 | 1.1 | |
| 84.3 | 1 | 1.1 | |
| 84.3 | 1 | 1.1 | |
| 84.5 | 1 | 1.1 | |
| 84.7 | 1 | 1.1 | |
| 85.4 | 1 | 1.1 | |
| 85.5 | 1 | 1.1 | |
| 86 | 1 | 1.1 | |
| 86.5 | 1 | 1.1 | |
| 86.6 | 1 | 1.1 | |
| 87 | 1 | 1.1 | |
| 87.4 | 1 | 1.1 | |
| 88.3 | 1 | 1.1 | |
| 88.7 | 1 | 1.1 | |
| 88.8 | 1 | 1.1 | |
| 89 | 1 | 1.1 | |
| 89.5 | 1 | 1.1 | |
| 90 | 1 | 1.1 | |
| 91.3 | 1 | 1.1 | |
| 91.4 | 1 | 1.1 | |
| 91.6 | 1 | 1.1 | |
| 91.9 | 1 | 1.1 | |
| 92 | 4 | 4.4 | |
| 93.2 | 1 | 1.1 | |
| 94.6 | 1 | 1.09 | |
| 94.8 | 1 | 1.09 | |
| 96.3 | 1 | 1.09 | |
| 96.5 | 1 | 1.09 | |
| 96.8 | 1 | 1.09 | |
| 97.4 | 1 | 1.09 | |
| 97.7 | 1 | 1.09 | |
| 97.9 | 1 | 1.09 | |
| 98 | 1 | 1.09 | |
| 98.6 | 1 | 1.09 | |
| 98.8 | 1 | 1.09 | |
| 98.95 | 1 | 1.09 | |
| 100 | 18 | 19.6 | |
| Total | 63 | ||
| (b) | |||
| Wear Time (%) | |||
| <80% (n = 29) | 80% (n = 63) | p | |
| Age | 71±12.1 | 66.5±13.3 | 0.1246 |
| Female | 11/29 = | 15/63 = | 0.162 |
| ESS baseline | 6.7±4.2 | 6.1±4.7 | 0.5964 |
| EQ5D baseline | 58.8±26.5 | 58.9±28.4 | 0.9789 |
| PSQI baseline | 5.2±3.1 | 7.1±4.2 | 0.0371 |
| STOP BANG baseline | 4.1±1.4 | 4.1±1.5 | 0.9415 |
| Body Mass Index | 28.1±5.6 | 30.1±5.4 | 0.1138 |
| Neck circumference | 39.4±2.5 | 39.2±4.1 | 0.8496 |
| Length of stay | 3.2±2.7 | 3.0±1.5 | 0.6345 |
| (a) | |||
| Average Time Worn (%) | Number of Patients | % of Patients | |
| 75 | 1 | 1.09 | |
| 75.5 | 1 | 1.09 | |
| 77 | 1 | 1.09 | |
| 77.4 | 1 | 1.09 | |
| 78.4 | 1 | 1.09 | |
| 78.8 | 1 | 1.09 | |
| 79.3 | 1 | 1.09 | |
| 80 | 2 | 2.17 | |
| 80.4 | 1 | 1.09 | |
| 81.6 | 1 | 1.09 | |
| 82 | 2 | 2.17 | |
| 83.5 | 1 | 1.09 | |
| 84.3 | 1 | 1.09 | |
| 84.3 | 1 | 1.09 | |
| 84.5 | 1 | 1.09 | |
| 84.7 | 1 | 1.09 | |
| 85.4 | 1 | 1.09 | |
| 85.5 | 1 | 1.09 | |
| 86 | 1 | 1.09 | |
| 86.5 | 1 | 1.09 | |
| 86.6 | 1 | 1.09 | |
| 87 | 1 | 1.09 | |
| 87.4 | 1 | 1.09 | |
| 88.3 | 1 | 1.09 | |
| 88.7 | 1 | 1.09 | |
| 88.8 | 1 | 1.09 | |
| 89 | 1 | 1.09 | |
| 89.5 | 1 | 1.09 | |
| 90 | 1 | 1.09 | |
| 91.3 | 1 | 1.09 | |
| 91.4 | 1 | 1.09 | |
| 91.6 | 1 | 1.09 | |
| 91.9 | 1 | 1.09 | |
| 92 | 4 | 4.35 | |
| 93.2 | 1 | 1.09 | |
| 94.6 | 1 | 1.09 | |
| 94.8 | 1 | 1.09 | |
| 96.3 | 1 | 1.09 | |
| 96.5 | 1 | 1.09 | |
| 96.8 | 1 | 1.09 | |
| 97.4 | 1 | 1.09 | |
| 97.7 | 1 | 1.09 | |
| 97.9 | 1 | 1.09 | |
| 98 | 1 | 1.09 | |
| 98.6 | 1 | 1.09 | |
| 98.8 | 1 | 1.09 | |
| 98.95 | 1 | 1.09 | |
| 100 | 18 | 19.6 | |
| Total | 70 | ||
| (b) | |||
| Wear Time (%) | |||
| <75% (n = 22) | 75% (n = 70) | p | |
| Age | 71.3 ± 13.3 | 66.8 ± 12.9 | 0.1620 |
| Female | 10 | 16 | 0.040 |
| ESS baseline | 6.5 ± 4.2 | 6.2 ± 4.7 | 0.8401 |
| EQ5D baseline | 55.2 ± 29.1 | 60.0 ± 27.3 | 0.4955 |
| PSQI baseline | 4.6 ± 2.7 | 7.1 ± 4.2 | 0.0101 |
| STOP BANG baseline | 3.9 ± 1.4 | 4.1 ± 1.5 | 0.5125 |
| Body Mass Index | 28.8 ± 6.1 | 29.7 ± 5.3 | 0.4895 |
| Neck circumference | 39.5 ± 2.8 | 39.2 ± 3.9 | 0.7898 |
| Length of stay | 3.5 ± 3.1 | 3.0 ± 1.4 | 0.3281 |
| (a) | |||
| Average Time Worn (%) | Number of Patients | % of Patients | |
| 70.3 | 1 | 1.09 | |
| 74 | 2 | 2.17 | |
| 74.3 | 1 | 1.09 | |
| 74.4 | 1 | 1.09 | |
| 75 | 1 | 1.09 | |
| 75.5 | 1 | 1.09 | |
| 77 | 1 | 1.09 | |
| 77.4 | 1 | 1.09 | |
| 78.4 | 1 | 1.09 | |
| 78.8 | 1 | 1.09 | |
| 79.3 | 1 | 1.09 | |
| 80 | 2 | 2.17 | |
| 80.4 | 1 | 1.09 | |
| 81.6 | 1 | 1.09 | |
| 82 | 2 | 2.17 | |
| 83.5 | 1 | 1.09 | |
| 84.3 | 1 | 1.09 | |
| 84.3 | 1 | 1.09 | |
| 84.5 | 1 | 1.09 | |
| 84.7 | 1 | 1.09 | |
| 85.4 | 1 | 1.09 | |
| 85.5 | 1 | 1.09 | |
| 86 | 1 | 1.09 | |
| 86.5 | 1 | 1.09 | |
| 86.6 | 1 | 1.09 | |
| 87 | 1 | 1.09 | |
| 87.4 | 1 | 1.09 | |
| 88.3 | 1 | 1.09 | |
| 88.7 | 1 | 1.09 | |
| 88.8 | 1 | 1.09 | |
| 89 | 1 | 1.09 | |
| 89.5 | 1 | 1.09 | |
| 90 | 1 | 1.09 | |
| 91.3 | 1 | 1.09 | |
| 91.4 | 1 | 1.09 | |
| 91.6 | 1 | 1.09 | |
| 91.9 | 1 | 1.09 | |
| 92 | 4 | 4.35 | |
| 93.2 | 1 | 1.09 | |
| 94.6 | 1 | 1.09 | |
| 94.8 | 1 | 1.09 | |
| 96.3 | 1 | 1.09 | |
| 96.5 | 1 | 1.09 | |
| 96.8 | 1 | 1.09 | |
| 97.4 | 1 | 1.09 | |
| 97.7 | 1 | 1.09 | |
| 97.9 | 1 | 1.09 | |
| 98 | 1 | 1.09 | |
| 98.6 | 1 | 1.09 | |
| 98.8 | 1 | 1.09 | |
| 98.95 | 1 | 1.09 | |
| 100 | 18 | 19.6 | |
| Total | 75 | ||
| (b) | |||
| Wear Time (%) | |||
| <70% (n = 17) | 70% (n = 75) | p | |
| Age | 71.8 ± 13.5 | 67.0 ± 12.9 | 0.1727 |
| Female | 8 | 18 | 0.057 |
| ESS baseline | 6.1 ± 4.2 | 6.3 ± 4.7 | 0.8694 |
| EQ5D baseline | 49.1 ± 28.6 | 61.1 ± 27.1 | 0.1069 |
| PSQI baseline | 3.9 ± 2.0 | 7.1 ± 4.0 | 0.0031 |
| STOP BANG baseline | 3.7 ± 1.4 | 4.2 ± 1.5 | 0.2321 |
| Body Mass Index | 28.3 ± 6.7 | 29.8 ± 5.2 | 0.3420 |
| Neck circumference | 38.9 ± 2.8 | 39.3 ± 3.8 | 0.6807 |
| Length of stay | 3.8 ± 3.5 | 2.9 ± 1.4 | 0.0894 |
Appendix B
| Diagnosis Category | n | % |
|---|---|---|
| Elective procedures | 22 | 33 |
| Acute coronary syndromes | 18 | 27 |
| Arrhythmias | 8 | 12 |
| Heart failure | 7 | 11 |
| Other | 11 | 17 |
Appendix C
| Wore ActiGraph Post-Discharge | Did Not Wear ActiGraph Post-Discharge | p | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Demographics and Comorbidities | |||||
| n | 37 | - | 38 | - | - |
| Age (years) | 67.4 | 14.4 | 66.4 | 12.0 | 0.75 |
| Sex (% Females) | 37.8 | - | 18.4 | - | 0.06 |
| Length of Stay (days) | 2.9 | 1.4 | 3.0 | 1.6 | 0.93 |
| Private insurance (%) | 37.8 | - | 42.1 | - | 0.71 |
| Atrial Fibrillation (%) | 37.8 | - | 26.3 | - | 0.29 |
| Heart Failure (%) | 13.5 | - | 23.7 | - | 0.26 |
| Dyslipidemia (%) | 70.3 | - | 65.8 | - | 0.68 |
| Hypertension (%) | 70.3 | - | 73.7 | - | 0.74 |
| Prior Stroke (%) | 16.2 | - | 10.5 | - | 0.47 |
| Prior Diabetes (%) | 32.4 | - | 26.3 | - | 0.56 |
| Prior Angina (%) | 40.5 | - | 55.3 | - | 0.20 |
| Prior Myocardial Infarction (%) | 16.2 | - | 26.3 | - | 0.26 |
| Prior Percutaneous Coronary Intervention (%) | 24.3 | - | 15.8 | - | 0.36 |
| Current Smoker (%) | 21.6 | - | 23.7 | - | 0.28 |
| Ischemic Heart Disease (%) | 40.5 | - | 44.7 | - | 0.71 |
| Chronic Obstructive Pulmonary Disease (%) | 10.8 | - | 18.4 | - | 0.35 |
Appendix D
| Cardiovascular-Related Readmission | Non-Cardiovascular-Related Readmission |
|---|---|
| ST-elevated myocardial infarction | Return to Emergency Department for unknown reason (x2) |
| Exacerbation of heart failure | Gynaecological pain |
| Coronary spasm | Haematoma on the arm |
| Chest pain (x3) | Itchy skin rash |
| Atrial fibrillation | Accidental overdose |
| Atypical angina | |
| Unstable angina |
References
- Ashton, C.M.; Kiukendall, D.H.; Johnson, M.L.; Wray, N.P.; Wu, L. The association between the quality of inpatient care and early readmission. Ann. Intern. Med. 1995, 122, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Milne, R.; Clarke, A. Can readmission rates be used as an outcome indicator? BMJ 1990, 301, 1139–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fein, I.A. Readmissions as a Quality Metric: Ready for Prime Time? Crit. Care Med. 2018, 46, 821–823. [Google Scholar] [CrossRef] [PubMed]
- Keenan, P.S.; Normand, S.L.; Lin, Z.; Drye, E.E.; Bhat, K.R.; Ross, J.S.; Schuur, J.D.; Stauffer, B.D.; Berheim, S.M.; Epstein, A.J.; et al. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circ. Cardiovasc. Qual. Outcomes 2008, 1, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dharmarajan, K.; Hsieh, A.F.; Lin, Z.; Bueno, H.; Ross, J.S.; Horwitz, L.I.; Barreto-Filho, J.A.; Kim, N.; Bernheim, S.M.; Suter, L.G.; et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA 2013, 309, 355–363. [Google Scholar] [CrossRef]
- Mirkin, K.A.; Enomoto, L.M.; Caputo, G.M.; Hollenbeak, C.S. Risk factors for 30-day readmission in patients with congestive heart failure. Heart Lung 2017, 46, 357–362. [Google Scholar] [CrossRef]
- Vogel, T.R.; Smith, J.B.; Kruse, R.L. Risk factors for thirty-day readmissions after lower extremity amputation in patients with vascular disease. PM R 2018, 10, 1321–1329. [Google Scholar] [CrossRef]
- Rodriguez, J.B.C.; Acharya, P.; Olso, E.; Cler, L. Risk factors for 30-day readmissions after acute myocardial infarction. Int. Cardiovasc. Forum J. 2015, 4, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Kansagara, D.; Englander, H.; Salanitro, A.; Kagen, D.; Theobald, C.; Freeman, M.; Kripalani, S. Risk prediction models for hospital readmission: A systematic review. JAMA 2011, 306, 1688–1698. [Google Scholar] [CrossRef] [Green Version]
- Labrosciano, C.; Air, T.; Tavella, R.; Beltrame, J.F.; Ranasinghe, I. Readmissions following hospitalisations for cardiovascular disease: A scoping review of the Australian literature. Aust. Health Rev. 2019, 44, 93–103. [Google Scholar] [CrossRef]
- Labrosciano, C.; Air, T.; Tavella, R.; Beltrame, J.; Zeitz, C.; Horton, D.; Ranasinghe, I. Rates of 30-Day readmission and mortality after heart failure hospitalisation in Australia and New Zealand: A population study. Heart Lung Circ. 2017, 26, S145–S146. [Google Scholar] [CrossRef] [Green Version]
- Labrosciano, C.; Tavella, R.; Air, T.; Zetiz, C.; Worthley, M.; Beltrame, J. Using the LACE index to predict 30-day all-cause unplanned readmission and mortality in acute myocardial infarction patients: Insights from the CADOSA registry. Heart Lung Circ. 2019, 28, S328. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, A.C.; Banks, S. Total sleep deprivation, chronic sleep restriction and sleep disruption. Prog. Brain Res. 2010, 185, 91–103. [Google Scholar] [PubMed]
- Zhang, L.; Sha, Y.S.; Kong, Q.Q.; Woo, J.A.; Miller, A.R.; Li, H.W.; Zhou, L.X.; Zhou, L.X.; Wang, C.L. Factors that affect sleep quality: Perceptions made by patients in the intensive care unit after thoracic surgery. Support. Care Cancer 2013, 21, 2091–2096. [Google Scholar] [CrossRef]
- Oswald, I. Sleep, the great restorer. New Sci. 1970, 46, 170–172. [Google Scholar]
- Cappuccio, F.P.; Cooper, D.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration predicts cardiovascular outcomes: A systematic review and meta-analysis of prospective studies. Eur. Heart, J. 2011, 32, 1484–1492. [Google Scholar] [CrossRef] [Green Version]
- Grandner, M.A.; Sands-Lincoln, M.R.; Pak, V.M.; Garland, S.N. Sleep duration, cardiovascular disease, and proinflammatory biomarkers. Nat. Sci. Sleep 2013, 5, 93–107. [Google Scholar] [CrossRef] [Green Version]
- Arora, V.M.; Chang, K.L.; Fazal, A.Z.; Staisiunas, P.G.; Meltzer, D.O.; Zee, P.C.; Knutson, K.L.; Van Cauter, E. Objective sleep duration and quality in hospitalized older adults: Associations with blood pressure and mood. J. Am. Geriatr. Soc. 2011, 59, 2185–2186. [Google Scholar] [CrossRef]
- Kessler, R.; Knutson, K.L.; Mokhiesi, B.; Anderson, S.L.; Shah, M.; Meltzer, D.O.; Arora, V.M. Sleep and activity patterns in older patients discharged from the hospital. Sleep 2019, 42. [Google Scholar] [CrossRef]
- Elliott, R.; Rai, T.; McKinley, S. Factors affecting sleep in the critically ill: An observational study. J. Crit. Care 2014, 29, 859–863. [Google Scholar] [CrossRef]
- DuBose, J.R.; Hadi, K. Improving inpatient environments to support patient sleep. Int. J. Qual. Health Care 2016, 28, 540–553. [Google Scholar] [CrossRef] [PubMed]
- Giménez, M.C.; Geerdinck, L.M.; Versteylen, M.; Leffers, P.; Meekes, G.J.; Herremans, H.; de Ruyter, B.; Schlangen, L.J. Light and sleep within hospital settings. Sleep-Wake Research in The Netherlands. Annu. Proc. Dutch Soc. Sleep Wake Res. NSWO 2011, 22, 56–59. [Google Scholar]
- Bihari, S.; Doug McEvoy, R.; Matheson, E.; Kim, S.; Woodman, R.J.; Bersten, A.D. Factors affecting sleep quality of patients in intensive care unit. J. Clin. Sleep Med. 2012, 8, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Krumholz, H.M. Post-hospital syndrome--an acquired, transient condition of generalized risk. N. Engl. J. Med. 2013, 368, 100–102. [Google Scholar] [CrossRef] [Green Version]
- Goldwater, D.S.; Dharmarajan, K.; McEwan, B.S.; Krumholz, H.M. Is posthospital syndrome a result of hospitalization-induced allostatic overload? J. Hosp. Med. 2018, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesquita, E.T.; Cruz, L.N.; Mariano, B.M.; Jorge, A.J. Post-Hospital syndrome: A new challenge in cardiovascular practice. Arq. Bras. Cardiol. 2015, 105, 540–544. [Google Scholar] [CrossRef]
- Topf, M.; Thompson, S. Interactive relationships between hospital patients’ noise-induced stress and other stress with sleep. Heart Lung J. Acute Crit. Care 2001, 30, 237–243. [Google Scholar] [CrossRef]
- Marin, J.M.; Carrizo, S.J.; Vicente, E.; Agusti, A.G. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: An observational study. Lancet 2005, 365, 1046–1053. [Google Scholar] [CrossRef]
- Loke, Y.K.; Brown, J.W.; Kwok, C.S.; Niruban, A.; Myint, P.K. Association of obstructive sleep apnea with risk of serious cardiovascular events: A systematic review and meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 720–728. [Google Scholar] [CrossRef] [Green Version]
- Bikov, A.; Kolossvary, M.; Jermendy, A.L.; Drobni, Z.D.; Tarnoki, A.D.; Tarnoki, D.L.; Forgo, B.; Kovacs, D.T.; Losonczy, G.; Kunos, L.; et al. Comprehensive coronary plaque assessment in patients with obstructive sleep apnea. J. Sleep Res. 2019, 28, e12828. [Google Scholar] [CrossRef]
- Scalzitti, N.J.; O’Connor, P.D.; Nielsen, S.W.; Aden, J.K.; Brock, M.S.; Taylor, D.M.; Mysliwiec, V.; Dion, G.R. Obstructive sleep apnea is an independent risk factor for hospital readmission. J. Clin. Sleep Med. 2018, 14, 753–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kauta, S.R.; Kennan, B.T.; Goldberg, L.; Schwab, R.J. Diagnosis and treatment of sleep disordered breathing in hospitalized cardiac patients: A reduction in 30-day hospital readmission rates. J. Clin. Sleep Med. 2014, 10, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Wesselius, H.M.; van den Ende, E.S.; Alsma, J.; Ter Maaten, J.C.; Schuit, S.C.E.; Stassen, P.M.; de Vries, O.J.; Kaasjager, K.; Haak, H.R.; van Doormaal, F.F.; et al. Quality and quantity of sleep and factors associated with sleep disturbance in hospitalized patients. JAMA Intern. Med. 2018, 178, 1201–1208. [Google Scholar] [CrossRef]
- Delaney, L.J.; Currie, M.J.; Huang, H.C.; Lopez, V.; Van Haren, F. “They can rest at home”: An observational study of patients’ quality of sleep in an Australian hospital. BMC Health Serv. Res. 2018, 18, 524. [Google Scholar] [CrossRef] [Green Version]
- Martin, J.L.; Hakim, A.D. Wrist actigraphy. Chest 2011, 139, 1514–1527. [Google Scholar] [CrossRef]
- van der Kooi, A.W.; Tulen, J.H.; van Elijk, M.M.; de Weerd, A.W.; van Uitert, M.J.; van Munster, B.C.; Slooter, A.J. Sleep monitoring by actigraphy in short-stay ICU patients. Crit. Care Nurs. Q. 2013, 36, 169–173. [Google Scholar] [CrossRef] [Green Version]
- Ancoli-Israel, S.; Cole, R.; Alessi, C.; Chambers, M.; Moorcroft, W.; Pollak, C.P. The role of actigraphy in the study of sleep and circadian rhythms. Sleep 2003, 26, 342–392. [Google Scholar] [CrossRef] [Green Version]
- Schwab, K.E.; Ronish, B.; Needham, D.M.; To, A.Q.; Martin, J.L.; Kamdar, B.B. Actigraphy to evaluate sleep in the intensive care unit. A systematic review. Ann. Am. Thorac. Soc. 2018, 15, 1075–1082. [Google Scholar] [CrossRef]
- Watson, P.L. Measuring sleep in critically ill patients: Beware the pitfalls. Crit. Care 2007, 11, 159. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- The EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawada, T. Validation study of STOP-Bang score for screening sleep-disordered breathing. Sleep Breath. 2016, 20, 1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baandrup, L.; Jennum, P.J. A validation of wrist actigraphy against polysomnography in patients with schizophrenia or bipolar disorder. Neuropsychiatr. Dis. Treat. 2015, 11, 2271–2277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullaney, D.J.; Kripke, D.F.; Messin, S. Wrist-actigraphic estimation of sleep time. Sleep 1980, 3, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Cellini, N.; McDevitt, E.A.; Mednick, S.C.; Buman, M.P. Free-living cross-comparison of two wearable monitors for sleep and physical activity in healthy young adults. Physiol. Behav. 2016, 157, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Cellini, N.; Buman, M.P.; McDevitt, E.A.; Ricker, A.A.; Mednick, S.C. Direct comparison of two actigraphy devices with polysomnographically recorded naps in healthy young adults. Chronobiol. Int. 2013, 30, 691–698. [Google Scholar] [CrossRef]
- Rosenberger, M.E.; Buman, M.P.; Haskell, W.L.; McConnell, M.V.; Carstensen, L.L. Twenty-four Hours of Sleep, Sedentary Behavior, and Physical Activity with Nine Wearable Devices. Med. Sci. Sports Exerc. 2016, 48, 457–465. [Google Scholar] [CrossRef] [Green Version]
- Zinkhan, M.; Berger, K.; Hense, S.; Nagel, M.; Obst, A.; Koch, B.; Penzel, T.; Fietze, I.; Ahrens, W.; Young, P.; et al. Agreement of different methods for assessing sleep characteristics: A comparison of two actigraphs, wrist and hip placement, and self-report with polysomnography. Sleep Med. 2014, 15, 1107–1114. [Google Scholar] [CrossRef]
- Slater, J.A.; Botsis, T.; Walsh, J.; King, S.; Straker, L.M.; Eastwood, P.R. Assessing sleep using hip and wrist actigraphy. Sleep Biol. Rhythm. 2015, 13, 172–180. [Google Scholar] [CrossRef] [Green Version]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Cole, R.J.; Kripke, D.F.; Gruen, W.; Mullaney, D.J.; Gillin, J.C. Automatic sleep/wake identification from wrist activity. Sleep 1992, 15, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Carskadon, M.A.; Dement, W.C. Normal human sleep: An overview. Princ. Pract. Sleep Med. 2005, 4, 13–23. [Google Scholar]
- Devine, E.B.; Hakim, Z.; Green, J. A systematic review of patient-reported outcome instruments measuring sleep dysfunction in adults. Pharmacoeconomics 2005, 23, 889–912. [Google Scholar] [CrossRef]
- Johns, M.W. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep 1992, 15, 376–381. [Google Scholar] [CrossRef] [Green Version]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S.A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C.M. STOP questionnaire: A tool to screen patients for obstructive sleep apnea. Anesthesiology 2008, 108, 812–821. [Google Scholar] [CrossRef] [Green Version]
- Brazier, J.; Jones, N.; Kind, P. Testing the validity of the Euroqol and comparing it with the SF-36 health survey questionnaire. Qual. Life Res. 1993, 2, 169–180. [Google Scholar] [CrossRef]
- Dorman, P.; Slattery, J.; Farrell, B.; Dennis, M.; Sandercock, P. Qualitative comparison of the reliability of health status assessments with the EuroQol and SF-36 questionnaires after stroke. United Kingdom Collaborators in the International Stroke Trial. Stroke 1998, 29, 63–68. [Google Scholar] [CrossRef]
- Stone, K.L.; Ewing, S.K.; Ancoli-Israel, S.; Ensrud, K.E.; Redline, S.; Bauer, D.C.; Cauley, J.A.; Hillier, T.A.; Cummings, S.R. Self-reported sleep and nap habits and risk of mortality in a large cohort of older women. J. Am. Geriatr. Soc. 2009, 57, 604–611. [Google Scholar] [CrossRef] [Green Version]
- Mallon, L.; Broman, J.E.; Hetta, J. Sleep complaints predict coronary artery disease mortality in males: A 12-year follow-up study of a middle-aged Swedish population. J. Intern. Med. 2002, 251, 207–216. [Google Scholar] [PubMed]
- Tsubono, Y.; Fukao, A.; Hisamichi, S. Health practices and mortality in a rural Japanese population. Tohoku J. Exp. Med. 1993, 171, 339–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amagai, Y.; Ishikawa, S.; Gotoh, T.; Doi, Y.; Kayaba, K.; Nakamura, Y.; Kajii, E. Sleep duration and mortality in Japan: The Jichi medical school cohort study. J. Epidemiol. 2004, 14, 124–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrie, J.E.; Shipley, M.J.; Cappuccio, F.P.; Brunner, E.; Miller, M.A.; Kumari, M.; Marmot, M.G. A prospective study of change in sleep duration: Associations with mortality in the Whitehall II cohort. Sleep 2007, 30, 1659–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kripke, D.F.; Garfinkel, L.; Wingard, D.L.; Klauber, M.R.; Marler, M.R. Mortality associated with sleep duration and insomnia. Arch. Gen. Psychiatry 2002, 59, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, S.R.; Ayas, N.T.; Malhotra, M.R.; White, D.P.; Schernhammer, E.S.; Speizer, F.E.; Stampfer, M.J.; Hu, F.B. A prospective study of sleep duration and mortality risk in women. Sleep 2004, 27, 440–444. [Google Scholar] [CrossRef] [Green Version]
- Gangwisch, J.E.; Heymsfield, S.B.; Boden-Albala, B.; Buijs, R.M.; Kreier, F.; Pickering, T.G.; Rundle, A.G.; Zammit, G.K.; Malaspina, D. Sleep duration as a risk factor for diabetes incidence in a large U.S. sample. Sleep 2007, 30, 1667–1673. [Google Scholar] [CrossRef]
- Hublin, C.; Partinen, M.; Koskenvuo, M.; Kaprio, J. Sleep and mortality: A population-based 22-year follow-up study. Sleep 2007, 30, 1245–1253. [Google Scholar] [CrossRef] [Green Version]
- Ruigomez, A.; Alonso, J.; Anto, J.M. Relationship of health behaviours to five-year mortality in an elderly cohort. Age Ageing 1995, 24, 113–119. [Google Scholar] [CrossRef]
- Kojima, M.; Wakai, K.; Kawamura, T.; Tamakoshi, A.; Aoki, R.; Lin, Y.; Nakayama, T.; Horibe, H.; Aoki, N.; Ohno, Y. Sleep patterns and total mortality: A 12-year follow-up study in Japan. J. Epidemiol. 2000, 10, 87–93. [Google Scholar] [CrossRef]


| Readmitted | Not Readmitted | p | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Demographics and Comorbidities | |||||
| n | 15 | - | 60 | - | - |
| Age (years) | 64.5 | 18.7 | 67.5 | 11.5 | 0.43 |
| Sex (% Females) | 40 | - | 25 | - | 0.25 |
| Length of Stay (days) | 3.5 | 1.5 | 2.8 | 1.5 | 0.14 |
| Private insurance (%) | 47 | - | 38 | - | 0.57 |
| Single room (%) | 33 | - | 30 | - | 0.80 |
| Live alone (%) | 47 | - | 28 | - | 0.17 |
| Cardiovascular risk factors and comorbidities | |||||
| AF (%) | 33 | - | 32 | - | 0.90 |
| HF (%) | 33 | - | 15 | - | 0.10 |
| Dyslipidemia (%) | 67 | - | 68 | - | 0.90 |
| Hypertension (%) | 60 | - | 75 | - | 0.25 |
| Prior Stroke (%) | 20 | - | 12 | - | 0.40 |
| Prior Diabetes (%) | 20 | - | 32 | - | 0.38 |
| Prior Angina (%) | 73 | - | 25 | - | 0.03 |
| Prior MI (%) | 33 | - | 18 | - | 0.21 |
| Prior PCI (%) | 13 | - | 22 | - | 0.47 |
| Prior CABG (%) | 20 | - | 8 | - | 0.19 |
| PAD (%) | 13 | - | 3 | - | 0.13 |
| Current smoker (%) | 20 | - | 23 | - | 0.95 |
| Non-Cardiovascular risk factors or comorbidities | |||||
| COPD (%) | 20 | - | 13 | - | 0.51 |
| Arthritis (%) | 13 | - | 22 | - | 0.47 |
| Depression (%) | 20 | - | 10 | - | 0.29 |
| Anxiety (%) | 7 | - | 5 | - | 0.81 |
| No OSA (%) | 87 | - | 90 | - | 0.84 |
| OSA with CPAP (%) | 7 | - | 7 | - | |
| OSA w/o CPAP (%) | 7 | - | 3 | - | |
| Asthma (%) | 20 | - | 12 | - | 0.40 |
| GORD (%) | 13 | - | 30 | - | 0.19 |
| Procedures and medications | |||||
| Angiography (%) | 27 | - | 47 | - | 0.15 |
| Aspirin (%) | 33 | - | 48 | - | 0.30 |
| Statin (%) | 40 | - | 50 | - | 0.49 |
| ARB / ACE inhibitor (%) | 40 | - | 42 | - | 0.91 |
| GTN (%) | 33 | - | 13 | - | 0.07 |
| Readmitted | Not Readmitted | p | Cohen’s d (95%CI) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| In hospital | ||||||
| Total sleep time (n) | 14 | - | 59 | - | - | - |
| In hours | 6.9 | 1.3 | 6.8 | 2.9 | 0.96 | 0.02 (−0.57–0.59) |
| 0 to 6 h (%) | 21 | - | 44 | - | 0.07 | - |
| 6 to <9 h (%) | 71 | - | 37 | - | - | - |
| ≥ 9 h (%) | 7 | - | 19 | - | - | - |
| Wake AfterSleep Onset (n) | 15 | - | 59 | - | - | - |
| In minutes | 84.5 | 85.3 | 61.9 | 51.3 | 0.14 | 0.43 (−0.14–1.00) |
| <30 min (%) | 0 | - | 12 | - | 0.16 | - |
| 30 to 60 min (%) | 33 | - | 46 | - | - | - |
| ≥ 60 min (%) | 67 | - | 42 | - | - | - |
| Number of awakenings (n) | 15 | - | 59 | - | - | - |
| 13.6 | 4.2 | 11.9 | 5.2 | 0.25 | 0.33 (−0.23–0.91) | |
| Average time awake (n) | 15 | - | 59 | - | - | - |
| In minutes | 4.7 | 1.6 | 5.4 | 2.4 | 0.29 | 0.30 (−0.26–0.87) |
| Post-discharge | ||||||
| Total sleep time (n) | 7 | - | 30 | - | - | - |
| Hours | 7.4 | 1.3 | 8.9 | 12.6 | 0.76 | 0.13 (−0.69–0.94) |
| 0 to 6 h (%) | 14.3 | - | 33 | - | 0.54 | - |
| 6 to <9 h (%) | 71.4 | - | 60 | - | - | - |
| ≥ 9 h (%) | 14.3 | - | 7 | - | - | - |
| Wake AfterSleep Onset (n) | 7 | - | 31 | - | - | - |
| In minutes | 43.4 | 15.6 | 46.2 | 14.6 | 0.65 | 0.19 (−0.63–1.01) |
| <30 min (%) | 14 | - | 16 | - | 0.78 | - |
| 30 to 60 min (%) | 72 | - | 58 | - | - | - |
| ≥ 60 min (%) | 14 | - | 26 | - | - | - |
| Number of awakenings (n) | 7 | - | 31 | - | - | - |
| 11.1 | 5.5 | 11.2 | 4.3 | 0.80 | 0.10 (−0.71–0.92) | |
| Average time awake (n) | 7 | - | 31 | - | - | - |
| In minutes | 5.6 | 2.8 | 4.9 | 1.7 | 0.47 | 0.31 (−0.51–1.13) |
| Readmitted | Not Readmitted | p | Cohen’s d (95%CI) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| In-hospital | ||||||
| n | 15 | - | 60 | - | - | - |
| ESS Mean Score | 5.9 | 5.3 | 6.3 | 4.6 | 0.73 | 0.09 (−0.47–0.66) |
| STOP BANG | 4.3 | 1.5 | 4.1 | 1.5 | 0.70 | 0.11 (−0.45–0.67) |
| PSQI | 9.13 | 3.6 | 6.4 | 4.1 | 0.02 | 0.70 (0.12–1.27) |
| n | 15 | - | 58 | - | - | - |
| EQ-5D VAS | 48.7 | 21.9 | 63.3 | 28.7 | 0.07 | 0.53 (−0.04–1.11) |
| Post-discharge | ||||||
| n | 7 | - | 40 | - | - | - |
| EQ-5D VAS | 74.3 | 15.1 | 76.5 | 22.3 | 0.80 | 0.10 (−0.70–0.91) |
| n | 8 | - | 41 | - | - | - |
| PSQI | 6.3 | 4.2 | 6.0 | 3.9 | 0.84 | 0.08 (−0.68–0.83) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labrosciano, C.; Tavella, R.; Reynolds, A.; Air, T.; Beltrame, J.F.; Ranasinghe, I.; Adams, R.J.T. The Association between Sleep Duration and Quality with Readmissions: An Exploratory Pilot-Study among Cardiology Inpatients. Clocks & Sleep 2020, 2, 120-142. https://doi.org/10.3390/clockssleep2020011
Labrosciano C, Tavella R, Reynolds A, Air T, Beltrame JF, Ranasinghe I, Adams RJT. The Association between Sleep Duration and Quality with Readmissions: An Exploratory Pilot-Study among Cardiology Inpatients. Clocks & Sleep. 2020; 2(2):120-142. https://doi.org/10.3390/clockssleep2020011
Chicago/Turabian StyleLabrosciano, Clementine, Rosanna Tavella, Amy Reynolds, Tracy Air, John F. Beltrame, Isuru Ranasinghe, and Robert J. T. Adams. 2020. "The Association between Sleep Duration and Quality with Readmissions: An Exploratory Pilot-Study among Cardiology Inpatients" Clocks & Sleep 2, no. 2: 120-142. https://doi.org/10.3390/clockssleep2020011