
Motion Sickness during Roll Motion: VR HMD View versus Monitor View

1
Human Factors Research Unit, Institute of Sound and Vibration Research, University of Southampton, Southampton SO17 1BJ, UK
2
Industrial Engineering Department, College of Engineering, Jazan University, Jazan 45142, Saudi Arabia
*
Author to whom correspondence should be addressed.
Vibration 2023, 6(1), 45-56; https://doi.org/10.3390/vibration6010004
Submission received: 12 November 2022
/
Revised: 16 December 2022
/
Accepted: 3 January 2023
/
Published: 6 January 2023
Abstract
:The purpose of this study was to investigate the effect of two views on motion sickness caused by low-frequency roll motion in the laboratory. Fifteen healthy male subjects participated in the study and were exposed to 30 min of 0.25 Hz roll oscillation at an angle of rotation (±5°). Subjects sat on a rigid seat with one of two visual scenes each session: (i) viewing 360° videos through virtual reality (VR) head-mounted display (HMD) device and (ii) reading articles on a monitor in a closed cabin. Ratings of motion sickness were obtained at 1 min intervals. The mean illness ratings of subjects for all visual conditions increased over the 30 min exposure to motion. There was significantly less sickness in the HMD condition than in the monitor condition. The findings suggest a beneficial effect of the HMD view on the severity of sickness. However, the HMD view had no effect on the sickness experienced by those vulnerable to sickness caused by exposure to motion or use of VR. It was concluded that the visual activity had a significant influence on motion sickness induced by 0.25 Hz roll oscillation with an angle of rotation (±5°), and the applications of VR could be implemented to further reduce motion sickness.
1. Introduction
Motion sickness is a major issue that impacts the comfort of passengers in all transport forms. All modes of transport can cause rotational motions in all axes, including roll, pitch and yaw. In land transport, exposure to roll oscillation can occur in road transport (during cornering) and in tilting trains. Roll oscillation has often been found to provoke motion sickness in isolation or in combination with translational or rotational oscillation [1,2,3,4,5]. The visual scene has been found to significantly modify the severity of sickness induced by different motion directions, such as lateral oscillation [6,7,8,9,10] or fore-and-aft oscillation [11] or combined fore-and-aft and pitch oscillation [12]. In addition, a recent international survey on the incidence of sickness in road transport found that 46% of subjects experienced motion sickness and that visual activity was one of the main factors in modifying the severity of sickness [13]. The use of VR has recently increased in education, research and entertainment, with continues development in its applications. However, some users may experience sickness known as VR sickness with symptoms related to nausea, oculomotor issues and disorientation.
Previous studies investigating the effect of roll motion on motion sickness have showed consistent findings that motion sickness can be caused due to exposure to roll motion. Roll oscillation at frequencies ranging from 0.025 to 0.4 Hz could produce motion sickness [1]. There was a significant difference in motion sickness triggered by roll oscillation, with magnitudes between 61.83° and 63.66° and between 61.83° and 67.32° [3]. Joseph and Griffin concluded that sickness induced by 0.2 Hz roll oscillation is dependent on the oscillation magnitude (illness ratings increase with increasing magnitude). At frequencies greater than 0.4 Hz, with magnitudes between 0.063 and 0.63 ms−2, acceleration caused by roll oscillation generated higher discomfort compared to the same acceleration caused by lateral acceleration [2]. With seven frequencies ranging from 0.25 to 1.0 Hz at magnitudes between 0.08 and 0.40 ms−2 r.m.s., similar discomfort produced by lateral acceleration or roll acceleration at frequencies less than 0.4 Hz and a higher discomfort caused by roll oscillation than that induced by lateral oscillation at frequencies ranges from 0.4 to 1.0 Hz [5].
The role of visual scene in the occurrence of motion sickness was investigated during exposure to different rotational motions with various visual conditions. These motions included rotational velocities increasing from 1 to 6 rpm in a clockwise direction [14], clockwise yaw oscillation [15], a constant counterclockwise acceleration of 20°/s2 until the device reached an angular velocity of 120°/s [16] and 0.025 and 0.1 Hz roll and pitch oscillation at an amplitude of 10° [17]. The results of these studies consistently indicated that the visual activity had a significant effect on the development of motion sickness.
Studies of visually induced motion sickness (VIMS) have contributed to the investigation of the influence of visual activity on motion sickness during rotational motions. Less sickness is induced by spiral motion relative to two conditions with single-axis motion, including roll oscillation and fore-and-aft oscillation [18]. In a study with three simulated rollercoaster rides moving in the fore-and-aft axis and rotating in three rotational motions ((i) pitch only; (ii) pitch and roll axes or in pitch, roll and yaw axes) 15 min videos were presented on a large projection screen to all subjects [19]. Their results showed that dual-axis rotation (pitch and roll) is significantly more nausea inducing than single-axis (pitch).
The investigation of the effect of using a VR HMD device during exposure to motion has received little attention. Previous studies have examined the influence of using a VR HMD device during exposure to motion (lateral motion) in car [20] and in the laboratory [10]. The study conducted in the car found no significant differences among all VR (different optical presentations of a real vehicle motion) with motion conditions. The laboratory study showed that VR HMD view resulted in slightly less sickness than the condition of watching a video on a monitor in a closed cabin and greater sickness than the blindfold condition. Recent studies investigated the effect of providing visual motion cues through a VR HMD device to reduce sensory conflict between vestibular and visual systems to enable the use of VR HMD in vehicles [21,22]. Consistent findings showed a beneficial effect of applying visual motion cues on the severity of motion sickness.
However, the effect of visual activities on motion sickness induced by low-frequency roll motion in isolation is not clear. In addition, the influence of using a VR HMD device on the development of motion sickness during exposure to roll motion is unknown. Despite VR sickness, the current focus of research is to further enable the use of VR applications as both a transport and simulation platform.
The aim of this study was to compare the effect of two visual scenes (viewing 360° videos through VR HMD device and reading articles on a monitor in a closed cabin) on the severity of motion sickness induced by low-frequency roll oscillation. It was hypothesized that a view with a VR HMD device would result in less sickness.
2. Methods
2.1. Subjects
First, 15 healthy male subjects aged between 21 and 40 years (mean 29.5, SD 7.25) participated in the study. The mean stature and mean body weight were 175.63 cm (SD 4.00) and 71.63 kg (SD 13.26). All subjects were either staff or students at the University of Southampton. Subjects were asked to complete a consent form before participating in the experiment, which was approved by the Human Experimentation Safety and Ethics Committee at the University of Southampton (ERGO/FEPS/64986). They were screened using a health questionnaire to exclude those with visual and balance issues. Each subject was required to respond to five questions: (1) do you have visual issues? (2) can you read articles on a monitor clearly? (3) can you see a visual content through a VR HMD device clearly? (4) do you have balance issues? and (5) can you maintain a postural stability?
2.2. Motion Stimuli
Subjects were exposed to sinusoidal low-frequency roll oscillation at 0.25 Hz with an angle of rotation (±5°). This motion is suitable for investigating motion sickness based on international standards for exposure to whole-body vibration, such as [23,24]. Motions were produced using an Institute of Sound and Vibration Research simulator (Six-Axis Motion Simulator). The simulator was maximumly capable of displacement of 1000 mm and 500 mm in vertical and horizontal directions, respectively, with about 20° in roll and pitch and about 10° in yaw as the maximum angle of rotation. The simulator was controlled using the ServoTest Pulsar software (Institute of Sound and Vibration Research, University of Southampton, Southampton, UK).
2.3. Visual Stimuli
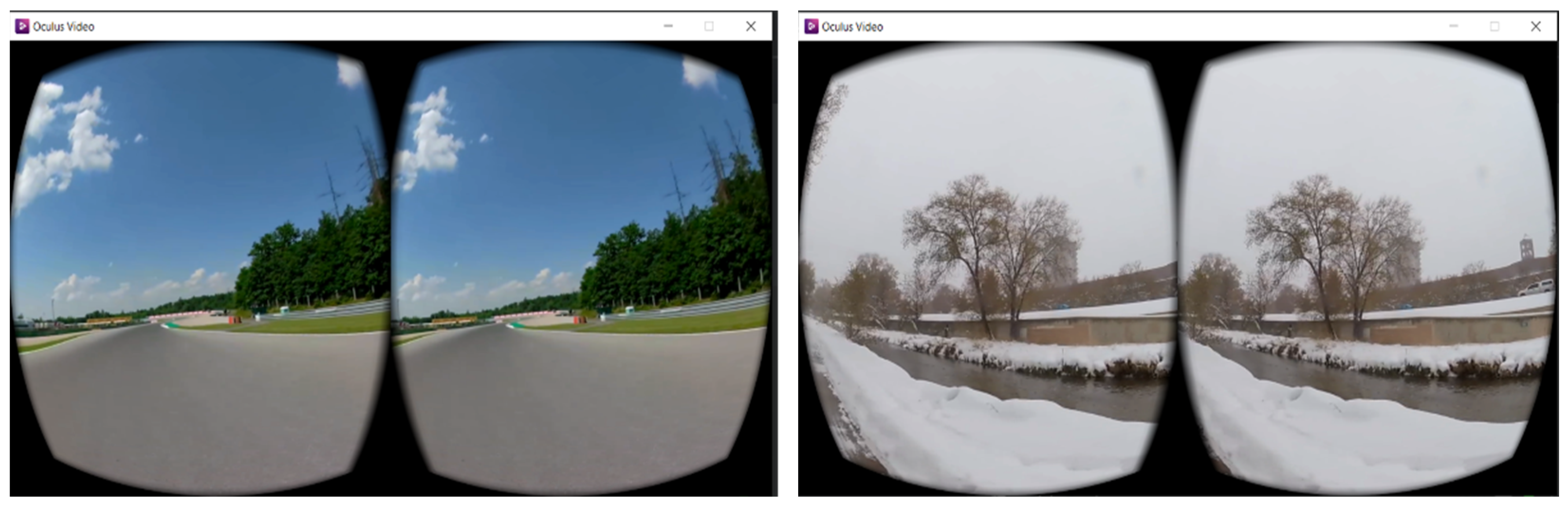
Visual conditions included in the study: (i) viewing 360° videos through VR HMD device and (ii) reading articles on a monitor in a closed cabin. The content used in the first condition was a combination of 360° videos with different motions from a car. Examples of these videos are shown in Figure 1. Subjects were instructed to skip any video causing discomfort. This enabled them to control the content they were experiencing while wearing the HMD device. The second condition, for instance, is similar to being in a vehicle without access to an outside view. Subjects were asked to read articles on the BBC news website in this condition. Table 1 highlights the differences between the contents of both visual conditions. The HMD device used in the current study was the Oculus Rift CV1 Headset device with 2160 × 1200 resolution (1080 × 1200 per eye) at 90 Hz refresh rate and the field of view (FOV) was 98.07°.
2.4. Cabin Environment and Seating
Subjects sat on a rigid seat, which was positioned at the centre of the simulator platform. The seat height was 430 mm above the floor with a rigid vertical backrest, which was 680 mm above the seat surface. Subjects were instructed to maintain upright posture, ensuring full contact with the seat backrest. For safety, subjects were asked to wear a loose lap belt. Subjects were also asked to wear Headphones (Sennheiser HD202), which produced white noise to mask the simulator noise at 55 ± 3 dB during exposure to motion, generated by the Human Factors Research Unit (HFRU) Deluxe Noise System. The experimenter communicated with subjects using a microphone by interrupting the white noise.
2.5. Experimental Design and Procedure
The study design was a within-subject design (repeated groups). The repeated-groups design was selected over the between-subject design because motion sickness varies considerably among individuals, which results in an increase in the inter-subject variability and difficulty in comparing different experimental groups. Subjects were asked to attend two sessions, with each session less than one hour. During the session, subjects were exposed to low-frequency roll oscillation for 30 min with a different visual condition each session at a one-week interval. Half of the subjects started with the first condition and another half started with the second condition.
Prior to motion exposure, subjects were asked to complete a motion sickness susceptibility questionnaire. The motion sickness susceptibility questionnaire [25] was designed to determine how susceptible a person is to motion sickness and what types of motion are most effective in causing that sickness (i.e., nausea, vomiting, etc.) in both land and non-land transport. Subjects were then given instructions on the objective of the experiment, the illness rating scale and the symptom checklist.
During the experiment, subjects were asked every minute to rate their sickness using a number based on an illness rating scale. The illness rating scale (adapted from [26]) was used to measure the motion sickness of subjects on a seven-point scale from 0 to 6 during motion exposure (0: no symptoms; 1: any symptoms, however slight; 2: mild symptoms; 3: mild nausea; 4: mild to moderate nausea; 5: moderate nausea but can continue; 6: moderate nausea and want to stop).
After exposure to motion, subjects were asked to fill in the symptom checklist to summarise the symptoms (i.e., general discomfort, warmth sensation, dizziness, nausea, etc.) experienced during the session.
2.6. Statistical Analysis
Data analysis was conducted using the software package SPSS (version 27.0). Since the data were not normally distributed, nonparametric tests were used for analysing the data. The Wilcoxon signed ranks test was used to quantify differences between the two groups (differences between the two visual conditions). The Spearman rank correlation coefficient was used to quantify associations between mean illness ratings and a total number of symptoms for each visual condition. The statistical significance was at p-value < 0.05.
3. Results
3.1. Subject Susceptibility to Motion Sickness
The motion sickness susceptibility questionnaire completed by subjects prior to the exposure to motion indicated that there were significant differences between the subjects in two measures of motion sickness susceptibility: illness susceptibility in the last year, Isusc(yr) (p = 0.001), and vomiting susceptibility in the last year, Vsusc(yr) (p = 0.001), and there were no significant differences between the subjects in four measures of motion sickness susceptibility: total susceptibility to vomiting, Vtotal (p = 0.119); total susceptibility to motion sickness in all types of transport, Mtotal (p = 0.997); susceptibility to motion sickness in land transport, Mland (p = 0.999); and susceptibility to motion sickness in non-land transport, Mnon-land (p = 0.185). These measures are defined and explained in [25].
3.2. Illness Ratings
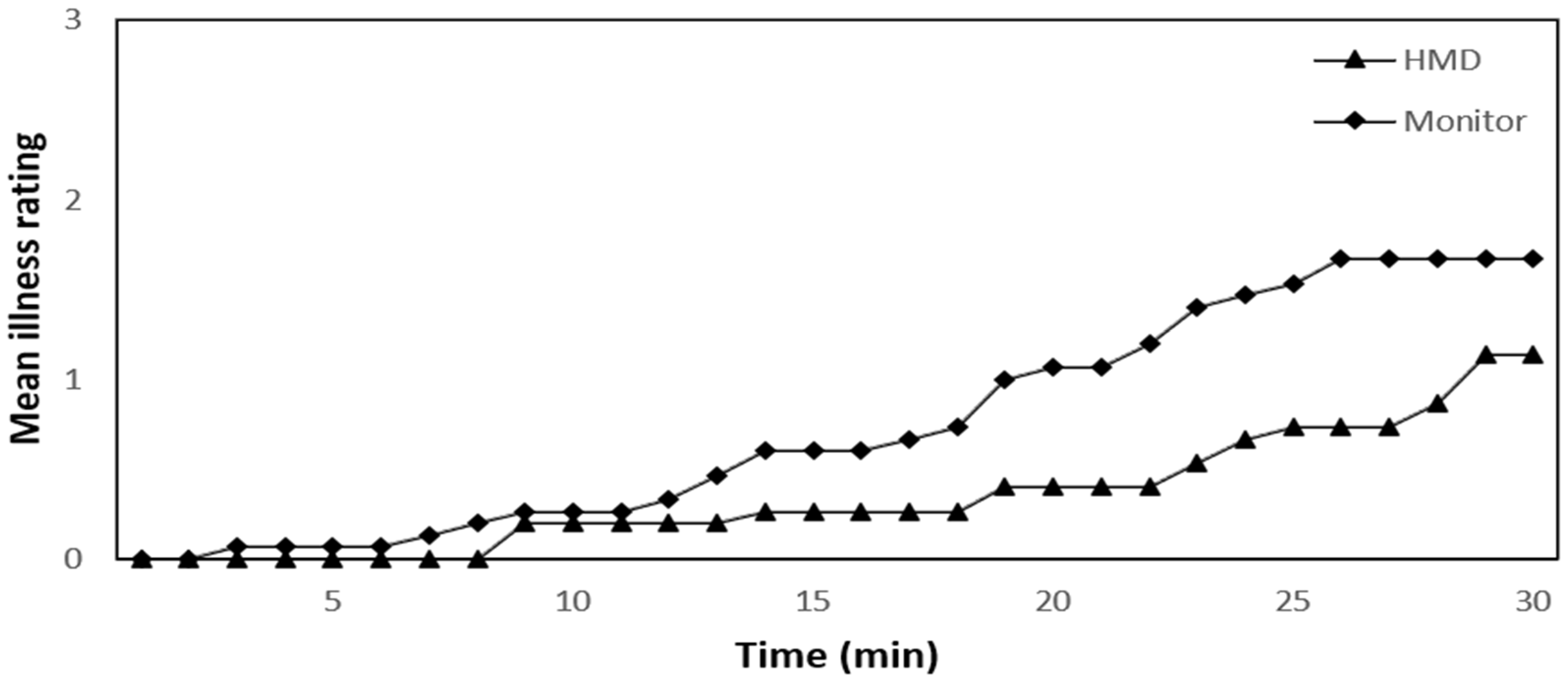
Based on the mean illness ratings at every minute of the 30 min exposure, there was a significant difference (Wilcoxon: p = 0.001) between the mean illness ratings reported by the subjects in the two visual conditions. The HMD condition significantly reduced sickness compared to the monitor condition. The mean illness ratings were taken every minute during the 30 min exposure to motion (Figure 2). The data in Figure 2 indicate that the mean illness ratings of subjects for all visual conditions increased over the 30 min exposure to motion. The maximum difference observed between the two visual conditions in the mean illness ratings is 100% at the 22nd minute, with a decrease of more than 66% in the mean illness ratings of the HMD condition relative to that of the monitor condition.
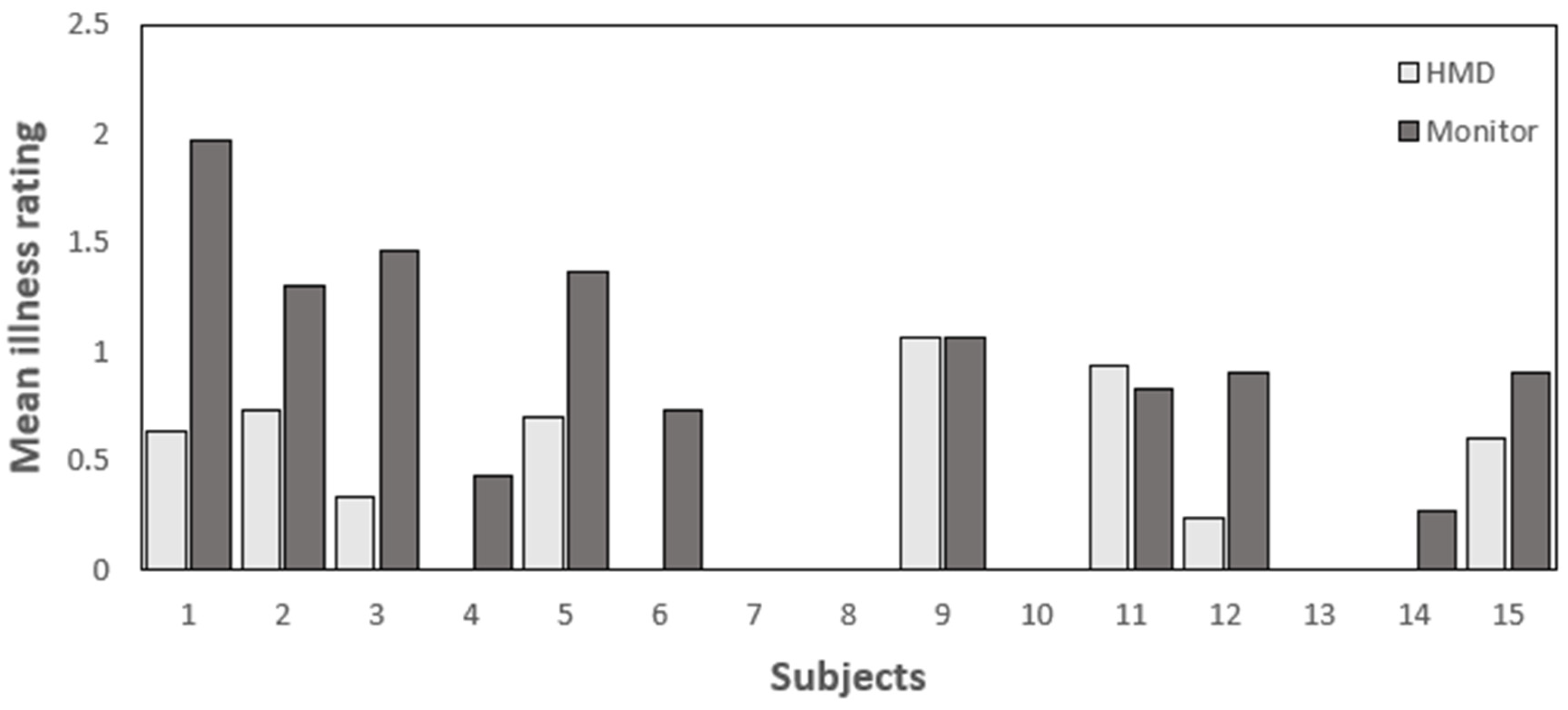
Based on the mean illness ratings for each subject over the 30 min motion exposure, there was a significant difference between the subjects’ mean illness ratings in the two visual conditions. The HMD condition resulted in less sickness than the monitor-view condition (Wilcoxon: p = 0.007). Figure 3 shows the mean illness ratings for each subject during 30 min exposure to roll oscillation in the two visual conditions. Based on the data in Figure 3, most subjects experienced the greatest motion sickness during exposure to motion with the monitor condition compared to the HMD condition. Three subjects reported no illness during the 30 min motion exposure in both conditions. The maximum individual difference observed between the two visual conditions is more than 103%, with the first subject having a decrease of more than 68% in the mean illness ratings of the HMD condition relative to that of the monitor condition.
For the option of changing the visual content through the VR HMD device, only two out of fifteen subjects changed the content during exposure to motion. The two subjects changed the content multiple times after they started feeling nauseous. However, from the data analysis, there is no suggestion of these two subjects having lower motion sickness relative to other subjects.
For the effect of habituation to motion, order effects were examined by comparing the mean illness ratings reported by subjects in the first and second sessions. There was no significant difference in the mean illness ratings reported by subjects in the first and second sessions (p = 0.878; Wilcoxon).
The accumulated illness ratings during exposure to motion with the HMD condition were positively correlated with five measures of self-rated susceptibility to motion sickness provided by the subjects prior to motion exposure: vomiting susceptibility in the last year (Spearman: rs = 0.615, p = 0.015); total susceptibility to vomiting (Spearman: rs = 0.535, p = 0.04); total susceptibility to motion sickness in all types of transport (Spearman: rs = 0.699, p = 0.004); susceptibility to motion sickness in land transport (Spearman: rs = 0.623, p = 0.013); and susceptibility to motion sickness in non-land transport (Spearman: rs = 0.652, p = 0.008). The accumulated illness ratings during exposure to motion in the monitor condition were positively correlated with one measure of self-rated susceptibility to motion sickness: illness susceptibility in the last year (Spearman: rs = 0.576, p = 0.025).
3.3. Symptoms
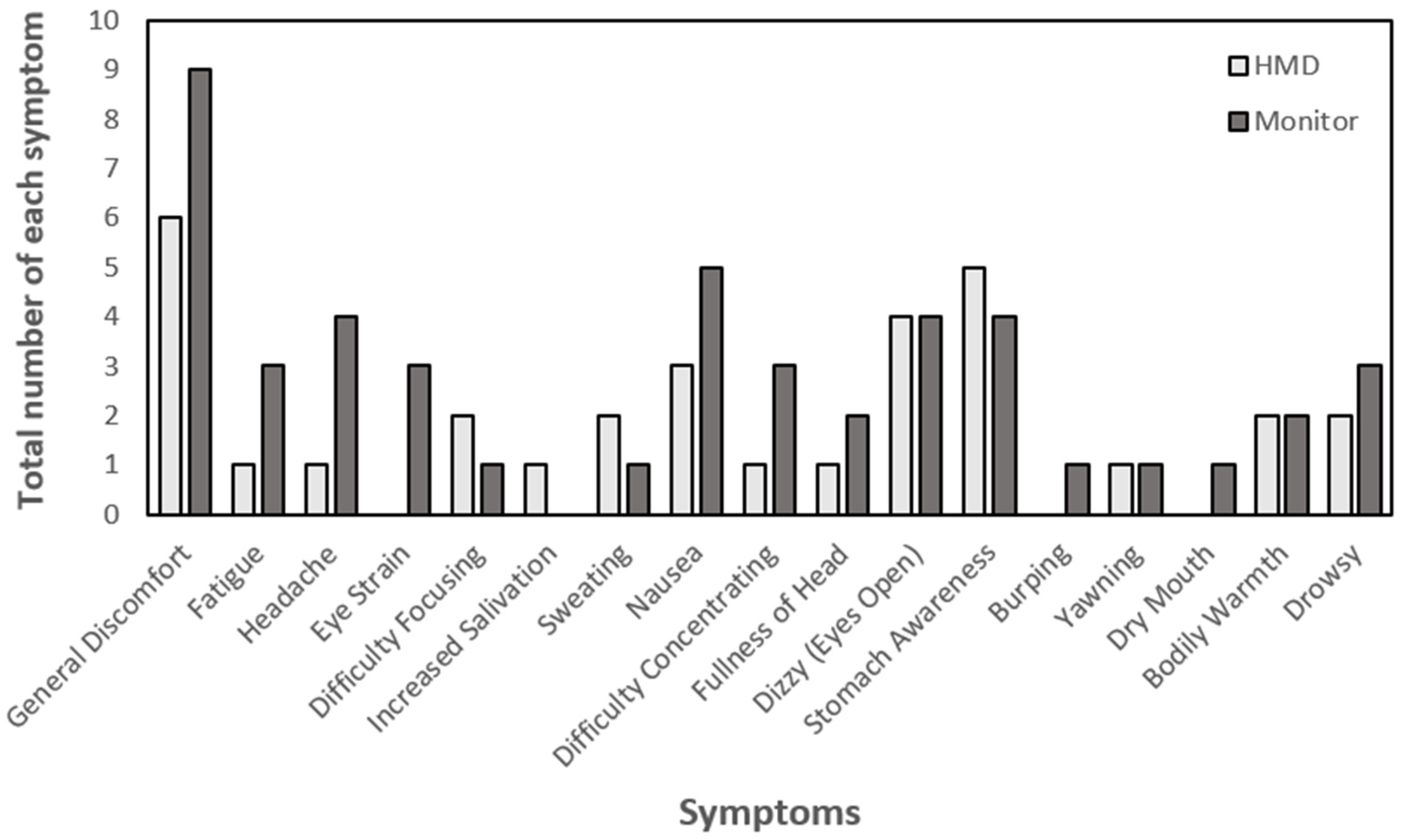
There was a significant difference between the two visual conditions in the total number of symptoms reported by subjects (Wilcoxon: p = 0.024). Similar to the illness ratings, fewer symptoms were reported by subjects after the exposure to motion in the HMD condition than in the monitor condition. Figure 4 shows the total number of each symptom reported by subjects after exposure to motion with the two visual conditions. From Figure 4, the highest symptom reported by subjects in each visual condition was general discomfort and nausea (n = 7 and 5, respectively, in monitor condition) and general discomfort and stomach awareness (n = 6 and 5, respectively, in HMD condition). The total number of symptoms reported by subjects was positively correlated with their accumulated illness ratings over the 30 min exposures to roll oscillation in both visual conditions (Spearman: rs = 0.869, p = 0.001 and Spearman: rs = 0.920, p = 0.001, respectively).
Like the illness ratings, the total number of symptoms reported by subjects with the monitor condition was positively correlated with one measure of self-rated susceptibility to motion sickness: illness susceptibility in the last year (Spearman: rs = 0.542, p = 0.037). The total number of symptoms reported by subjects in the HMD condition was positively correlated with five measures of self-rated susceptibility to motion sickness: illness susceptibility in the last year (Spearman: rs = 0.644, p = 0.01); vomiting susceptibility in the last year (Spearman: rs = 0.728, p = 0.002); total susceptibility to motion sickness in all types of transport (Spearman: rs = 0.695, p = 0.004); susceptibility to motion sickness in land transport (Spearman: rs = 0.650, p = 0.009); and susceptibility to motion sickness in non-land transport (Spearman: rs = 0.604, p = 0.017).
4. Discussion
The illness ratings and the symptom scores indicated that motion sickness was influenced by the visual activity during exposure to roll oscillation. The HMD condition resulted in significantly less sickness than the monitor condition.
4.1. Effect of Visual Scene
For the beneficial effect of the HMD condition on the development of motion sickness induced by roll oscillation, only one study compared the effect of monitor view and HMD view on motion sickness induced by either translational or rotational oscillation. The previous study indicated that the HMD visual condition produced slightly less motion sickness than the monitor [10]. The difference in the findings between the two studies may be explained by the content experienced by subjects while wearing the HMD device. The previous study used a 2D video of forward view of the simulator, which was recorded, stabilizing the camera on the simulator during motion. The current study used a combination of 360° videos, and each subject was instructed to skip any video causing discomfort. In addition, some of the subjects who participated in the present study were more familiar to the use of the HMD device and less susceptible to the sickness triggered by VR. This suggests that familiarity to VR use while watching suitable 360° visual content may help the subjects engage and not concentrate on the motion during exposure. The suitability of visual content through the HMD device may depend on the preferences of individuals and their susceptibility to VR sickness.
Other studies have investigated the influence of having an internal view in a closed cabin (similar to the monitor condition) on motion sickness caused by either translational oscillation, rotational oscillation or combined translational and rotational oscillation. Consistent findings indicated that exposure to motion with an internal view of a moving cabin resulted in the greatest sickness when compared to other visual conditions, including external view and eye closure/blindfold [6,11,12,15,26,27]. The internal view may include a visual task (i.e., reading articles, as in the current study), which may cause more motion sickness than having a static visual view. In a laboratory study with low-frequency translational oscillation, the visual search task triggered motion sickness more than keeping the eyes closed [26]. During exposure to linear accelerations in a car with three visual conditions ((i) eyes open (visual control of car motion); (ii) eyes closed; and (iii) eyes open (reading a map)), the highest sickness was produced when subjects read a map relative to the other two visual conditions [11]. A possible explanation for the increase in the severity of motion sickness with the monitor condition is that the increase in the vestibulo-ocular reflex (VOR) during reading articles with head movement results in greater eye movements, which may increase the severity of motion sickness experienced by subjects with this condition [11,28,29,30].
From Figure 3, although the HMD condition reduced the severity of sickness experienced by the subjects in this study, some subjects reported similar great sickness in both visual conditions. This suggests that having different visual contents through the VR HMD device with the option of controlling the content being experienced has no beneficial effect for all subjects, in particular, those who are unfamiliar with the use of the VR HMD device and susceptible to motion sickness. The positive effect of the HMD view on the severity of sickness may depend on various factors, such as individual differences (i.e., susceptibility to sickness), familiarity to the use of VR, content and specifications of display [31,32,33,34].
Sensitivity of individuals to 3D motion may depend on motion sensitivity cues, such as monocular, binocular and motion parallax. Subjects were exposed to four cue conditions (monocular, binocular, combined (both monocular and binocular cues) and full VR (combined condition and motion parallax cues)) to investigate the individual differences [35]. The findings showed that cue sensitivity varied with and across individuals and conflicts related to motion parallax may be the main source of sickness in VR. In addition, the level of susceptibility to motion sickness may have a major effect on the severity of VR sickness. Individuals with high levels of susceptibility to motion sickness experienced greater VR sickness [31,36]. This is the reason why adaptation to VR 3D motion is a key factor in the severity of motion sickness.
One of the main display specifications of a VR system is its latency (display lag). The poor latency in a VR system can lead to a time difference between expected and actual view, which can cause VR sickness [37]. The Oculus Rift CV1 HMD device (the device used in this study) has a very low baseline display delay of about 5.3 ms [38] and its motion to photon latency at the start (Sudden) and middle (Continuous) of the movement was 20.6 ms and 1.5 ms, respectively [39]. The results of comparing four conditions of time delay (67 ms, 167 ms, 267 ms and 367 ms) indicated that there was an increase in the severity of VR sickness with increasing time delay [40]. In addition, the increase in head-to-display delay up to 212 ms decreased the presence and vection in the Oculus Rift CV1 Headset [38]. Inconsistent findings showed no difference found in the severity of VR sickness between three conditions of time delay, including 48 ms, 125 ms and 250 ms [41]. Draper et al. suggested that the user can habituate to a fixed time delay during exposure to VR content. However, this may not occur with a variable time delay, which can result in an increased VR sickness. It can be concluded that it is difficult to provide an acceptable delay time because individuals respond differently to latency [42].
4.2. Effect of Duration
Figure 2 shows that the mean illness ratings of subjects for both visual conditions increased over the 30 min exposure to roll oscillation at 0.25 Hz with an angle of rotation (±5°). This was different from previous studies [11,27,43]; however, the findings of this study were consistent with several previous studies. These studies indicated that an increase in motion sickness was found with increasing duration of exposure to vertical oscillation [44], lateral or fore-and-aft oscillation [6,45,46,47,48,49], roll or pitch oscillation [1,3], combined fore-and-aft and pitch oscillation [12] and combined lateral and roll oscillation [4,50,51,52]. The increase in the duration of exposure to translational oscillation, rotational oscillation or combined translational and rotational oscillation can produce an increased magnitude of sensed and expected signals from the vestibular system. This causes an increase in conflict between signals, resulting in an increase in the amount of motion sickness.
4.3. Effect of Habituation to Motion
Habituation to motion can occur with the repeated-measures (within-subject) design. The study’s findings showed no significant difference in the mean illness ratings reported by subjects in the first and second sessions (p = 0.878; Wilcoxon). This leads to the conclusion that habituation had no effect on the findings of this study. This was not identical to the results of two previous studies using a repeated-measures design, which claimed that habituation could occur if the exposure to the motion was at a weekly interval [4,50]. However, the findings of this study were consistent with many previous studies employing a within-subjects design, which concluded that habituation had no influence if subjects were tested at a weekly interval [10,26,53,54,55,56,57].
4.4. Self-Rating of Sickness Susceptibility
The positive correlation between the accumulated illness ratings during exposure to motion and the measures of self-rated susceptibility to motion sickness provided by the subjects prior to motion exposure suggests that the questionnaire responses indicate how subjects feel during exposure to roll motion in the laboratory. This was consistent with the findings of a previous laboratory study investigating the same motion direction [1].
4.5. Other Factors Influencing Severity of Motion Sickness
Correlated visual information with motion exposure during the use of a VR HMD device can reduce sensory conflict due to receiving congruent signals from the vestibular and visual sensory systems, resulting in decreased sickness. For instance, this is similar to being exposed to motion in any form of transport while having a clear outside view. Many previous studies showed a significant effect of having correlated visual information (a clear outside view) with motion exposure in the alleviation of motion sickness (i.e., [8,11,12]). In addition, providing visual motion cues through a VR HMD device to match the real (sensed) motion was found to reduce motion sickness in vehicles [21,22]. The current study focused on investigating the severity of sickness during exposure to roll motion with/without a VR HMD device. Further research should investigate the development of motion sickness while providing visual content through the VR HMD correlated with degree of roll motion.
The current study only considered male subjects; however, the literature did suggest that there is a difference between the responses of males and females. Females tend to have a higher susceptibility to motion sickness in environments with/without VR (i.e., [43,58,59,60,61,62]). Therefore, female subjects would be expected to have higher illness ratings if they were recorded. However, some previous studies found no significant differences between males and females in the vulnerability to motion sickness [35,63]. This suggests that although females have higher illness ratings, the trend would remain similar to males. In addition, it is still expected that females show lower illness ratings with the applications of VR through the HMD device; however, a large-scale study, including both female and male subjects, would be required to confirm this and to look at the overall effect as the next step of research.
5. Conclusions
This study investigated the effect of two visual conditions with/without a VR HMD device on the severity of motion sickness during exposure to low-frequency roll oscillation in the laboratory. There was a significant difference between the two visual scenes in the amount of motion sickness induced by 0.25 Hz pure roll oscillation with an angle of rotation (±5°). The HMD visual condition produced significantly less motion sickness relative to the monitor condition. The visual content through the HMD device used in this study was beneficial in reducing the motion sickness induced by roll oscillation. However, this view had no effect on the sickness experienced by those vulnerable to sickness caused by exposure to motion or sickness related to VR use. These findings add to the knowledge that the visual activity has a significant effect on the development of motion sickness caused by roll oscillation. Further investigation should consider the factors responsible for the variation in VR sickness to improve the VR experience during exposure to motion for all users.
Author Contributions
Conceptualization, Y.S. and Y.Y.; methodology, investigation and original draft preparation, Y.S.; supervision, review and editing, Y.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data are not publicly available due to privacy reasons.
Acknowledgments
We thank Gary Parker and Peter Russell for technical and instrumental support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Howarth, H.V.; Griffin, M.J. Effect of roll oscillation frequency on motion sickness. Aviat. Space Environ. Med. 2003, 74, 326–331. [Google Scholar] [PubMed]
- Wyllie, I.H.; Griffin, M.J. Discomfort from sinusoidal oscillation in the roll and lateral axes at frequencies between 0.2 and 1.6 Hz. J. Acoust. Soc. Am. 2007, 121, 2644–2654. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.A.; Griffin, M.J. Motion sickness: Effect of the magnitude of roll and pitch oscillation. Aviat. Space Environ. Med. 2008, 79, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.A.; Griffin, M.J. Motion sickness: Effect of changes in magnitude of combined lateral and roll oscillation. Aviat. Space Environ. Med. 2008, 79, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Beard, G.F.; Griffin, M.J. Discomfort caused by low-frequency lateral oscillation, roll oscillation and roll-compensated lateral oscillation. Ergonomics 2013, 56, 103–114. [Google Scholar] [CrossRef] [Green Version]
- Howarth, H.V.; Martino, M.M.; Griffin, M.J. Laboratory study of the effect of visual scene on motion sickness caused by lateral oscillation. In Proceedings of the 34th Meeting of the UK Group on Human Response to Vibration, Ford Motor Company, Essex, UK, 22–24 September 1999. [Google Scholar]
- Griffin, M.J.; Newman, M.M. An experimental study of low-frequency motion in cars. J. Automob. Eng. 2004, 218, 1231–1238. [Google Scholar] [CrossRef]
- Griffin, M.J.; Newman, M.M. Visual field effects on motion sickness in cars. Aviat. Space Environ. Med. 2004, 75, 739–748. [Google Scholar]
- Wada, T.; Yoshida, K. Effect of passengers’ active head tilt and opening/closure of eyes on motion sickness in lateral acceleration environment of cars. Ergonomics 2016, 59, 1050–1059. [Google Scholar] [CrossRef] [Green Version]
- Sumayli, Y.M.; Ye, Y. The effect of visual scene on motion sickness induced by lateral oscillation. In Proceedings of the 8th American Conference on Human Vibration, Organized by West Virginia University School of Medicine and Centres for Disease Control and Prevention, National Institute for Occupational Safety and Health, Morgantown, WV, USA, 23–25 June 2021. [Google Scholar]
- Probst, T.; Krafczyk, S.; Büchele, W.; Brandt, T. Visuelle Prävention der Bewegungskrankheit im Auto [Visual prevention from motion sickness in cars]. Arch. Psychiatr. Nervenkr. 1982, 231, 409–421. (In German) [Google Scholar] [CrossRef]
- Butler, C.A.; Griffin, M.J. Motion sickness with combined fore-aft and pitch oscillation: Effect of phase and the visual scene. Aviat. Space Environ. Med. 2009, 80, 946–954. [Google Scholar] [CrossRef]
- Schmidt, E.A.; Kuiper, O.X.; Wolter, S.; Diels, C.; Bos, J.E. An international survey on the incidence and modulating factors of carsickness. Transp. Res. Part F-Traffic Psychol. Behav. 2020, 71, 76–87. [Google Scholar] [CrossRef]
- Reason, J.T.; Diaz, E.D. Effects of visual reference on adaptation to motion sickness and subjective responses evoked by graded cross-coupled angular accelerations. In Proceedings of the 5th Symposium on the Role of the Vestibular Organs in Space Exploration, NASA SP-314. Washington, DC, USA, 1–3 January 1973. [Google Scholar]
- Lackner, J.R.; Graybiel, A. Some influences of vision on susceptibility to motion sickness. Aviat. Space Environ. Med. 1979, 50, 1122–1125. [Google Scholar] [PubMed]
- Leger, A.; Money, K.E.; Landolt, J.P.; Cheung, B.S.; Rodden, B.E. Motion sickness caused by rotations about Earth-horizontal and Earth-vertical axes. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1981, 50, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Rolnick, A.; Bles, W. Performance and well-being under tilting conditions: The effects of visual reference and artificial horizon. Aviat. Space Environ. Med. 1989, 60, 779–785. [Google Scholar]
- Diels, C.; Howarth, P.A. Visually induced motion sickness: Single-versus dual-axis motion. Displays 2011, 32, 175–180. [Google Scholar] [CrossRef]
- Keshavarz, B.; Hecht, H. Axis rotation and visually induced motion sickness: The role of combined roll, pitch, and yaw motion. Aviat. Space Environ. Med. 2011, 82, 1023–1029. [Google Scholar] [CrossRef]
- McGill, M.; Alexander, N.G.; Brewster, S. I Am The Passenger: How Visual Motion Cues Can Influence Sickness For In-Car VR. In Proceedings of the CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017. [Google Scholar]
- Qiu, Z.; McGill, M.; Pöhlmann, K.M.T.; Brewster, S.A. Display Rotation for Reducing Motion Sickness Caused by Using VR in Vehicles. In Proceedings of the 14th International Conference on Automotive User Interfaces and Interactive Vehicular Applications, Seoul, Republic of Korea, 17–20 September 2022. [Google Scholar] [CrossRef]
- Pöhlmann, K.M.; Auf Der Heyde, M.S.; Li, G.; Verstraten, F.; Brewster, S.A.; McGill, M. Can Visual Motion Presented in a VR Headset Reduce Motion Sickness for Vehicle Passengers? In Proceedings of the 14th International Conference on Automotive User Interfaces and Interactive Vehicular Applications, Seoul, Republic of Korea, 17–20 September 2022. [Google Scholar] [CrossRef]
- BS 6841:1987; Measurement and Evaluation of Human Exposure to Whole-Body Mechanical Vibration and Repeated Shock. British Standard: Singapore. Available online: https://www.en-standard.eu/bs-6841-1987-guide-to-measurement-and-evaluation-of-human-exposure-to-whole-body-mechanical-vibration-and-repeated-shock/ (accessed on 10 November 2022).
- ISO 2631-1:1997; Mechanical Vibration and Shock—Evaluation of Human Exposure to Whole-Body Vibration—Part 1: General Requirements. International Standard: Geneva, Switzerland. Available online: https://www.iso.org/obp/ui/#iso:std:iso:2631:-1:ed-2:v2:en (accessed on 10 November 2022).
- Griffin, M.J.; Howarth, H.V. Motion Sickness History Questionnaire; Technical Report 283; Institute of Sound and Vibration Research, University of Southampton: Southampton, UK, 2000. [Google Scholar]
- Golding, J.F.; Kerguelen, M. A comparison of the nauseogenic potential of low-frequency vertical versus horizontal linear oscillation. Aviat. Space Environ. Med. 1992, 63, 491–497. [Google Scholar]
- Bos, J.E.; MacKinnon, S.N.; Patterson, A. Motion sickness symptoms in a ship motion simulator: Effects of inside, outside, and no view. Aviat. Space Environ. Med. 2005, 76, 1111–1118. [Google Scholar]
- Barr, C.C.; Schultheis, L.W.; Robinson, D.A. Voluntary, non-visual control of the human vestibulo-ocular reflex. Acta Otolaryngol. 1976, 81, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Weissman, B.M.; DiScenna, A.O.; Ekelman, B.L.; Leigh, R.J. Effect of eyelid closure and vocalization upon the vestibulo-ocular reflex during rotational testing. Ann Otol Rhinol Laryngol. 1989, 98, 548–550. [Google Scholar] [CrossRef]
- Ebenholtz, S.M.; Cohen, M.M.; Linder, B.J. The possible role of nystagmus in motion sickness: A hypothesis. Aviat. Space Environ. Med. 1994, 65, 1032–1035. [Google Scholar] [PubMed]
- Benzeroual, K.; Allison, R.S. Cyber (motion) sickness in active stereoscopic 3D gaming. In Proceedings of the International Conference on 3D Imaging, Liege, Belgium, 3–5 December 2013. [Google Scholar] [CrossRef]
- Keshavarz, B. Exploring Behavioral Methods to Reduce Visually Induced Motion Sickness in Virtual Environments. In Proceedings of the International Conference on Virtual, Augmented and Mixed Reality (VAMR), Toronto, ON, Canada, 17–22 July 2016. [Google Scholar]
- Davis, S.; Nesbitt, K.; Nalivaiko, E. Comparing the onset of cybersickness using the Oculus Rift and two virtual roller coasters. In Proceedings of the 11th Australasian Conference on Interactive Entertainment (IE), Sydney, Australia, 27–30 January 2015. [Google Scholar]
- Dennison, M.S.; Wisti, A.Z.; D’Zmura, M. Use of physiological signals to predict cybersickness. Displays 2016, 44, 42–52. [Google Scholar] [CrossRef]
- Fulvio, J.M.; Ji, M.; Rokers, B. Variations in visual sensitivity predict motion sickness in virtual reality. Entertain. Comput. 2021, 38, 1004–1023. [Google Scholar] [CrossRef]
- Llorach, G.; Evans, A.; Blat, J. Simulator sickness and presence using HMDs: Comparing use of a game controller and a position estimation system. In Proceedings of the 20th ACM Symposium on Virtual Reality Software and Technology, Edinburgh, Scotland, 11–13 November 2014. [Google Scholar] [CrossRef]
- Rebenitsch, L.; Owen, C. Review on cybersickness in applications and visual displays. Virtual Real. 2016, 20, 101–125. [Google Scholar] [CrossRef]
- Kim, J.; Charbel-Salloum, A.; Perry, S.; Palmisano, S. Effects of display lag on vection and presence in the Oculus Rift HMD. Virtual Real. 2022, 26, 425–436. [Google Scholar] [CrossRef]
- Warburton, M.; Mon-Williams, M.; Mushtaq, F.; Morehead, J.R. Measuring motion-to-photon latency for sensorimotor experiments with virtual reality systems. Behav. Res. Methods. 2022. [Google Scholar] [CrossRef]
- DiZio, P.; Lackner, J.R. Circumventing side effects of immersive virtual environments. In Proceedings of the 7th International Conference on Human-Computer Interaction, San Francisco, CA, USA, 24 August 1997. [Google Scholar]
- Draper, M.H.; Viirre, E.S.; Furness, T.A.; Gawron, V.J. Effects of image scale and system time delay on simulator sickness within head-coupled virtual environments. Hum. Factors 2001, 43, 129–146. [Google Scholar] [CrossRef]
- Jerald, J.J. Scene-Motion-and Latency-Perception Thresholds for Head-Mounted Displays. Doctoral Dissertation, The University of North Carolina at Chapel Hill, Chapel Hill, NG, USA, 2009. [Google Scholar]
- Turner, M.; Griffin, M.J. Motion sickness in public road transport: The relative importance of motion, vision and individual differences. Br. J. Psychol. 1999, 90, 519–530. [Google Scholar] [CrossRef]
- McCauley, M.E.; Royal, J.W.; Wylie, C.D.; O’hanlon, J.F.; Mackie, P.R. Motion Sickness Incidence: Exploratory Studies of Habituation, Pitch and Roll, and the Refinement of a Mathematical Model; Technical Report; Canyon Research Group Inc Goleta CA Human Factors Research Div.: Goleta, CA, USA, 1976. [Google Scholar]
- Howarth, H.V.; Griffin, M.J. Effect of foreground visual information on motion sickness caused by lateral oscillation. In Proceedings of the 35th UK Group Meeting on Human Response to Vibration, Southampton, UK, 12–14 September 2000. [Google Scholar]
- Howarth, H.V. A comparison of motion sickness with 2-dimensional and 3-dimensional visual scenes. In Proceedings of the 36th UK Group Conference on Human Response to Vibration, Farnborough, UK, 12–14 September 2001. [Google Scholar]
- Griffin, M.J.; Mills, K.L. Effect of magnitude and direction of horizontal oscillation on motion sickness. Aviat. Space Environ. Med. 2002, 73, 640–646. [Google Scholar]
- Donohew, B.E.; Griffin, M.J. Motion sickness: Effect of the frequency of lateral oscillation. Aviat. Space Environ. Med. 2004, 75, 649–656. [Google Scholar]
- Butler, C.A.; Griffin, M.J. Motion sickness during fore-and-aft oscillation: Effect of the visual scene. Aviat. Space Environ. Med. 2006, 77, 1236–1243. [Google Scholar] [PubMed]
- Joseph, J.A.; Griffin, M.J. Motion sickness from combined lateral and roll oscillation: Effect of varying phase relationships. Aviat. Space Environ. Med. 2007, 78, 944–950. [Google Scholar] [CrossRef]
- Donohew, B.E.; Griffin, M.J. Motion sickness with fully roll-compensated lateral oscillation: Effect of oscillation frequency. Aviat. Space Environ. Med. 2009, 80, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Donohew, B.E.; Griffin, M.J. Motion sickness with combined lateral and roll oscillation: Effect of percentage compensation. Aviat. Space Environ. Med. 2010, 81, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Golding, J.F.; Finch, M.I.; Stott, J.R. The effects of motion direction, body axis, and posture on motion sickness induced by low frequency linear oscillation. Aviat. Space Environ. Med. 1995, 66, 1046–1051. [Google Scholar]
- Golding, J.F.; Markey, H.M. Effect of frequency of horizontal linear oscillation on motion sickness and somatogravic illusion. Aviat. Space Environ. Med. 1996, 67, 121–126. [Google Scholar]
- Golding, J.F.; Finch, M.I.; Stott, J.R. Frequency effect of 0.35-1.0 Hz horizontal translational oscillation on motion sickness and the somatogravic illusion. Aviat. Space Environ. Med. 1997, 68, 396–402. [Google Scholar]
- Golding, J.F.; Mueller, A.G.; Gresty, M.A. A motion sickness maximum around the 0.2 Hz frequency range of horizontal translational oscillation. Aviat. Space Environ. Med. 2001, 72, 188–192. [Google Scholar]
- Golding, J.F.; Bles, W.; Bos, J.E.; Haynes, T.; Gresty, M.A. Motion sickness and tilts of the inertial force environment: Active suspension systems vs. active passengers. Aviat. Space Environ. Med. 2003, 74, 220–227. [Google Scholar]
- Lawther, A.; Griffin, M.J. A survey of the occurrence of motion sickness amongst passengers at sea. Aviat. Space Environ. Med. 1988, 59, 399–406. [Google Scholar]
- Turner, M.; Griffin, M.J.; Holland, I. Airsickness and aircraft motion during short-haul flights. Aviat. Space Environ. Med. 2000, 71, 1181–1189. [Google Scholar] [PubMed]
- Koslucher, F.; Munafo, J.; Stoffregen, T.A. Postural sway in men and women during nauseogenic motion of the illuminated environment. Exp. Brain Res. 2016, 234, 2709–2720. [Google Scholar] [CrossRef] [PubMed]
- Freitag, S.; Weyers, B.; Kuhlen, T.W. Examining rotation gain in CAVE-like virtual environments. IEEE Trans. Vis. Comput. Graph. 2016, 22, 1462–1471. [Google Scholar] [CrossRef] [PubMed]
- Munafo, J.; Diedrick, M.; Stoffregen, T.A. The virtual reality head-mounted display Oculus Rift induces motion sickness and is sexist in its effects. Exp. Brain Res. 2017, 235, 889–901. [Google Scholar] [CrossRef]
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.; Rizzo, A.; Loetscher, T. Factors associated with virtual reality sickness in head-mounted displays: A systematic review and meta-analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef]
Figure 1.
Examples of the 360° videos through the HMD device included in this study.

Figure 2.
Mean illness ratings during the 30 min exposure to roll oscillation in the two visual conditions.
Figure 2.
Mean illness ratings during the 30 min exposure to roll oscillation in the two visual conditions.

Figure 3.
Mean illness ratings for each subject during 30 min exposure to roll oscillation in the two visual conditions.
Figure 3.
Mean illness ratings for each subject during 30 min exposure to roll oscillation in the two visual conditions.

Figure 4.
The total number of each symptom reported by subjects after the exposure to motion with the two visual conditions.
Figure 4.
The total number of each symptom reported by subjects after the exposure to motion with the two visual conditions.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
The differences between the contents of both visual conditions.
| Visual Condition | Task | Device |
|---|---|---|
| Condition 1 | Watching 360° videos | HMD |
| Condition 2 | Reading articles on the BBC news website | Monitor |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sumayli, Y.; Ye, Y. Motion Sickness during Roll Motion: VR HMD View versus Monitor View. Vibration 2023, 6, 45-56. https://doi.org/10.3390/vibration6010004
AMA Style
Sumayli Y, Ye Y. Motion Sickness during Roll Motion: VR HMD View versus Monitor View. Vibration. 2023; 6(1):45-56. https://doi.org/10.3390/vibration6010004
Chicago/Turabian StyleSumayli, Yahya, and Ying Ye. 2023. "Motion Sickness during Roll Motion: VR HMD View versus Monitor View" Vibration 6, no. 1: 45-56. https://doi.org/10.3390/vibration6010004